
Disrupted Value-Directed Strategic Processing in Individuals with Mild Cognitive Impairment: Behavioral and Neural Correlates

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
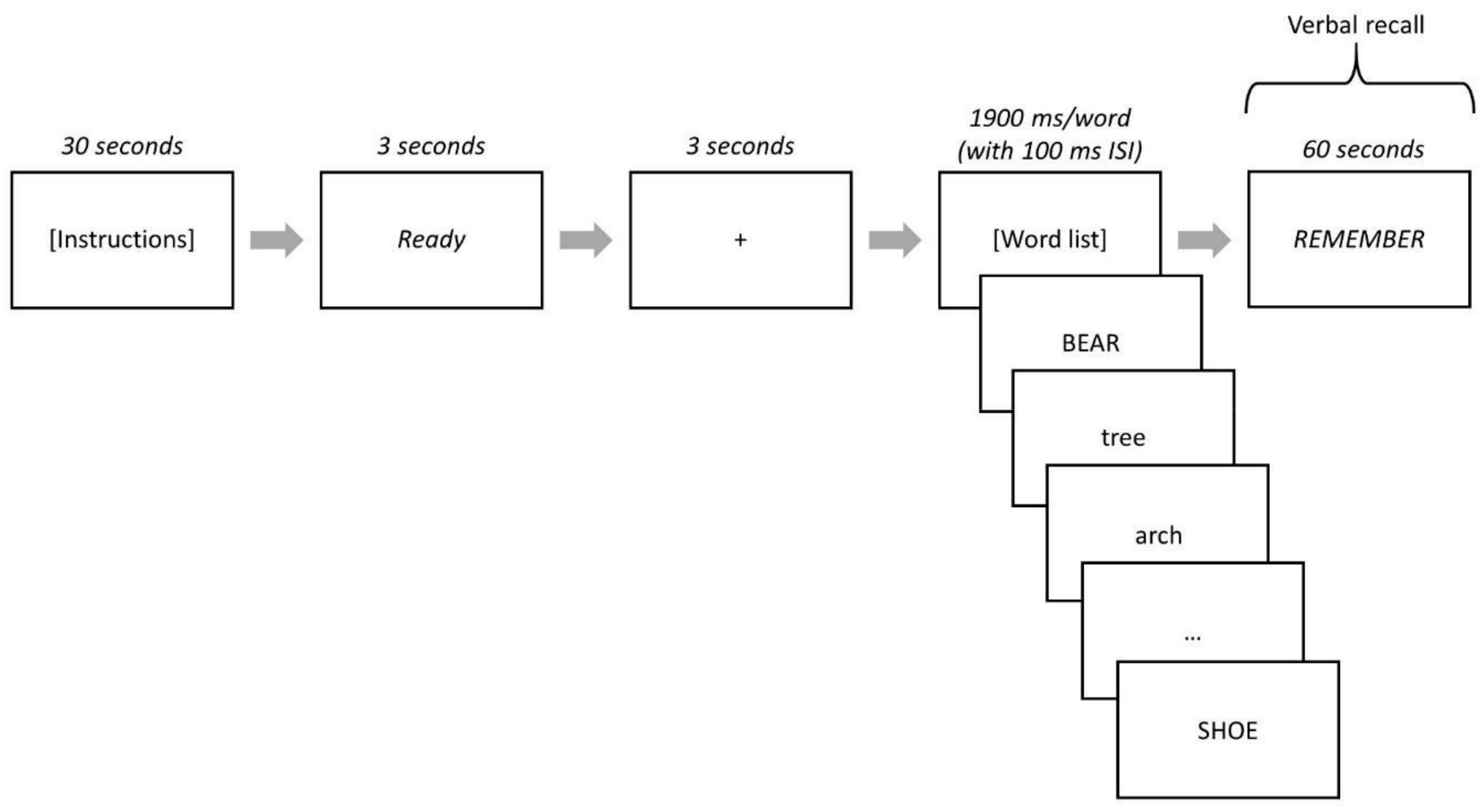
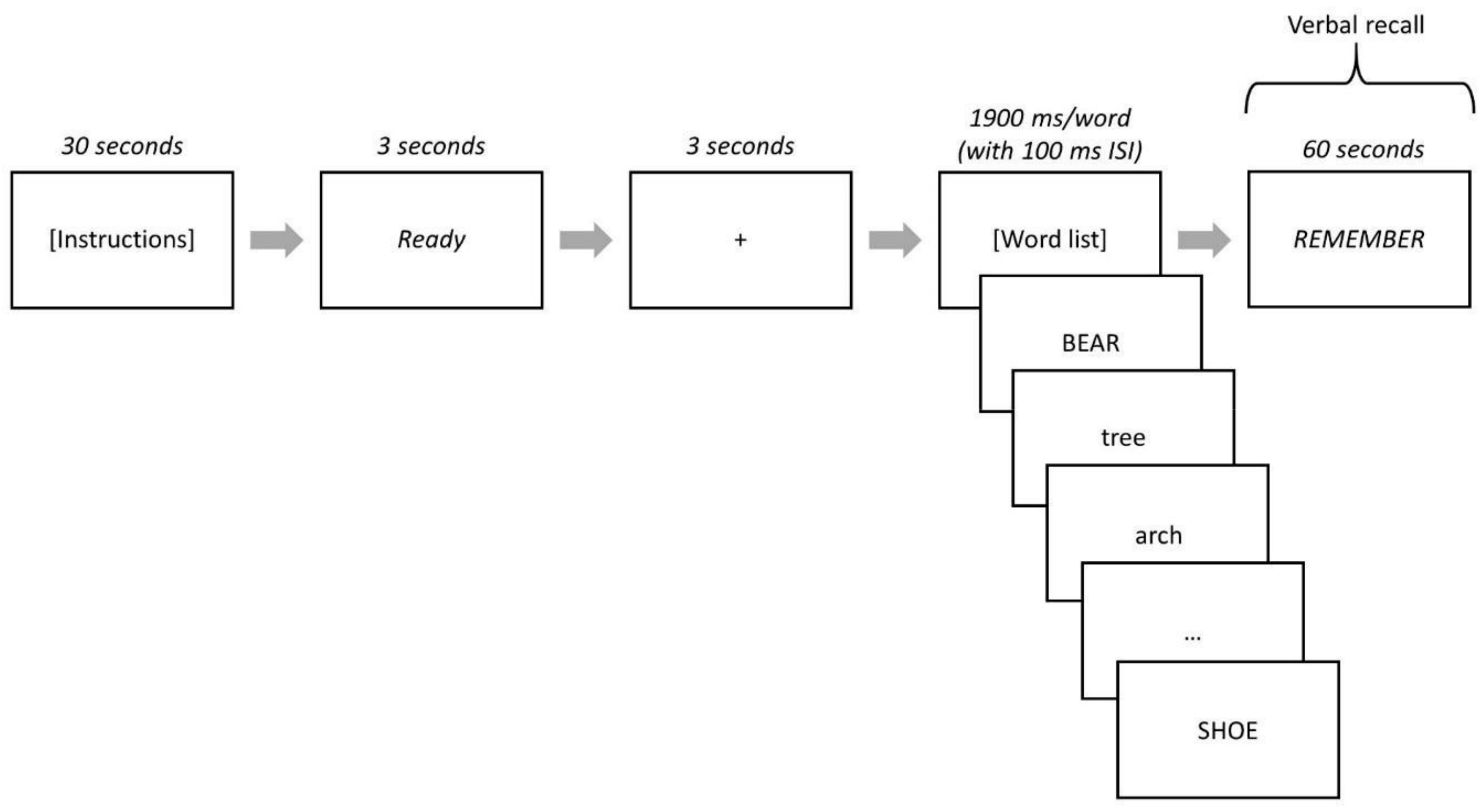
2.2. Strategic Processing Task and Procedures
2.3. EEG Data Collection and Preprocessing
2.4. ERSP Analysis
2.5. ERSP Power Estimation
2.6. Statistical Analysis
3. Results
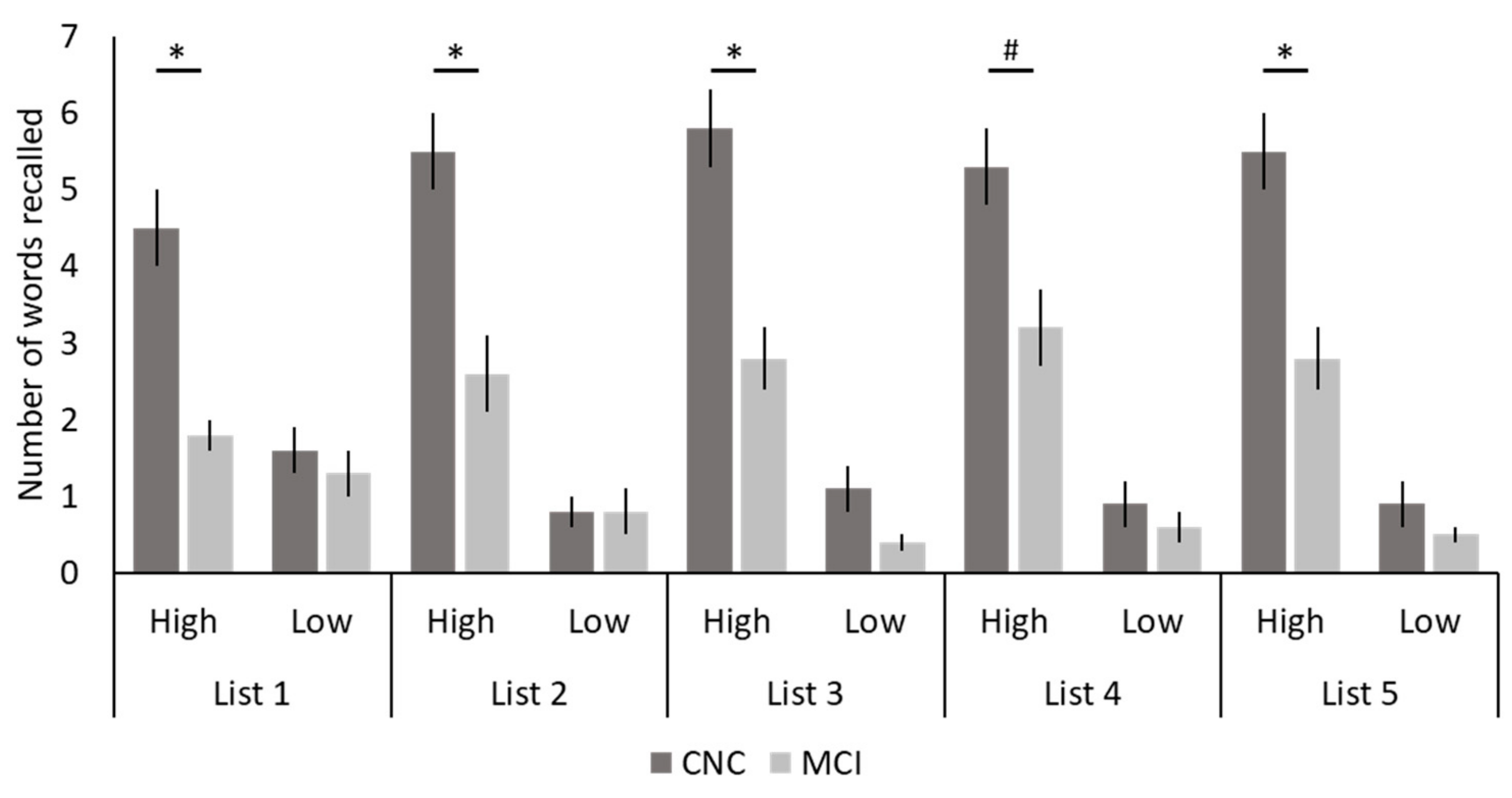
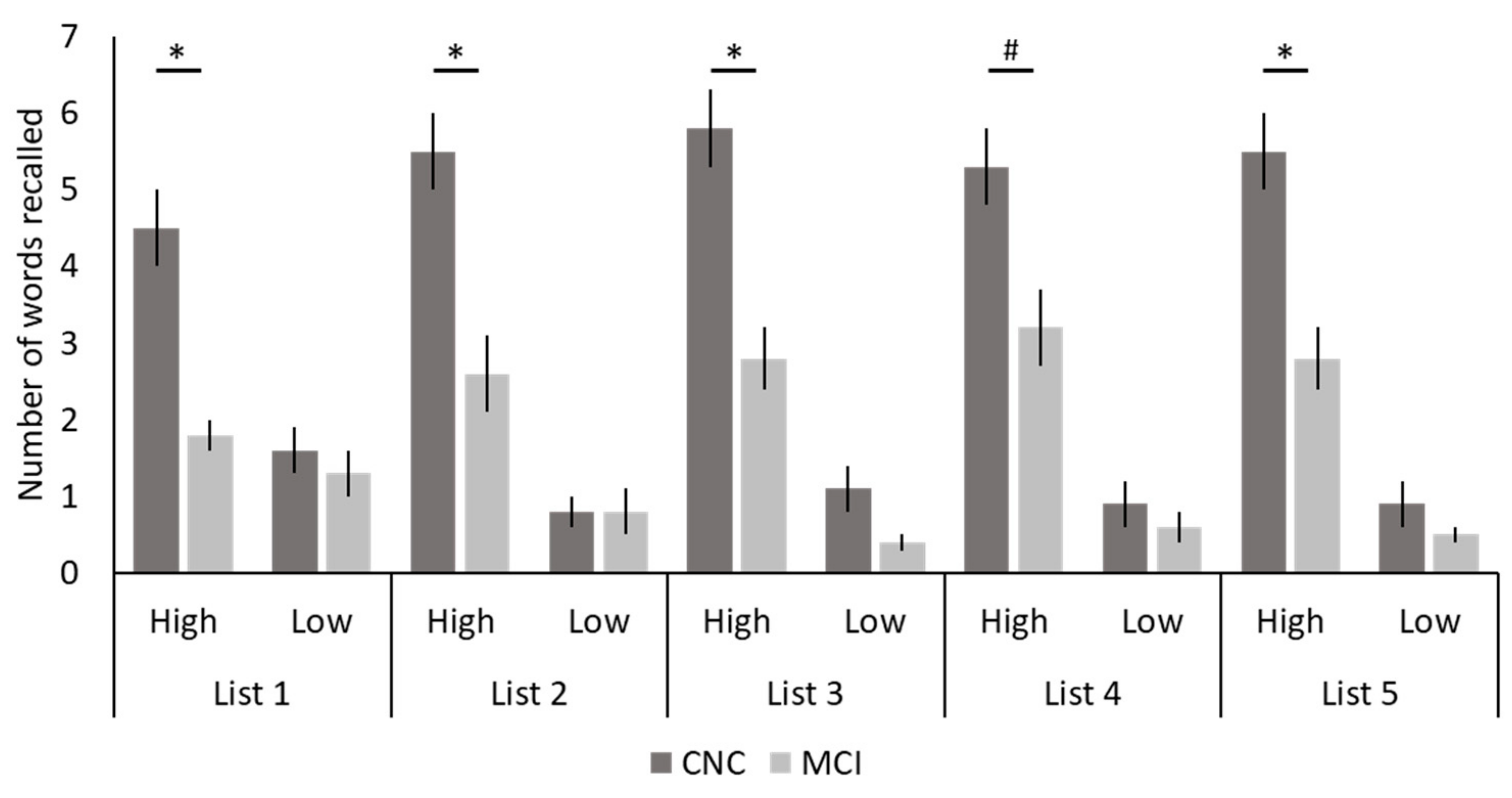
3.1. Task-Related Behavioral Data
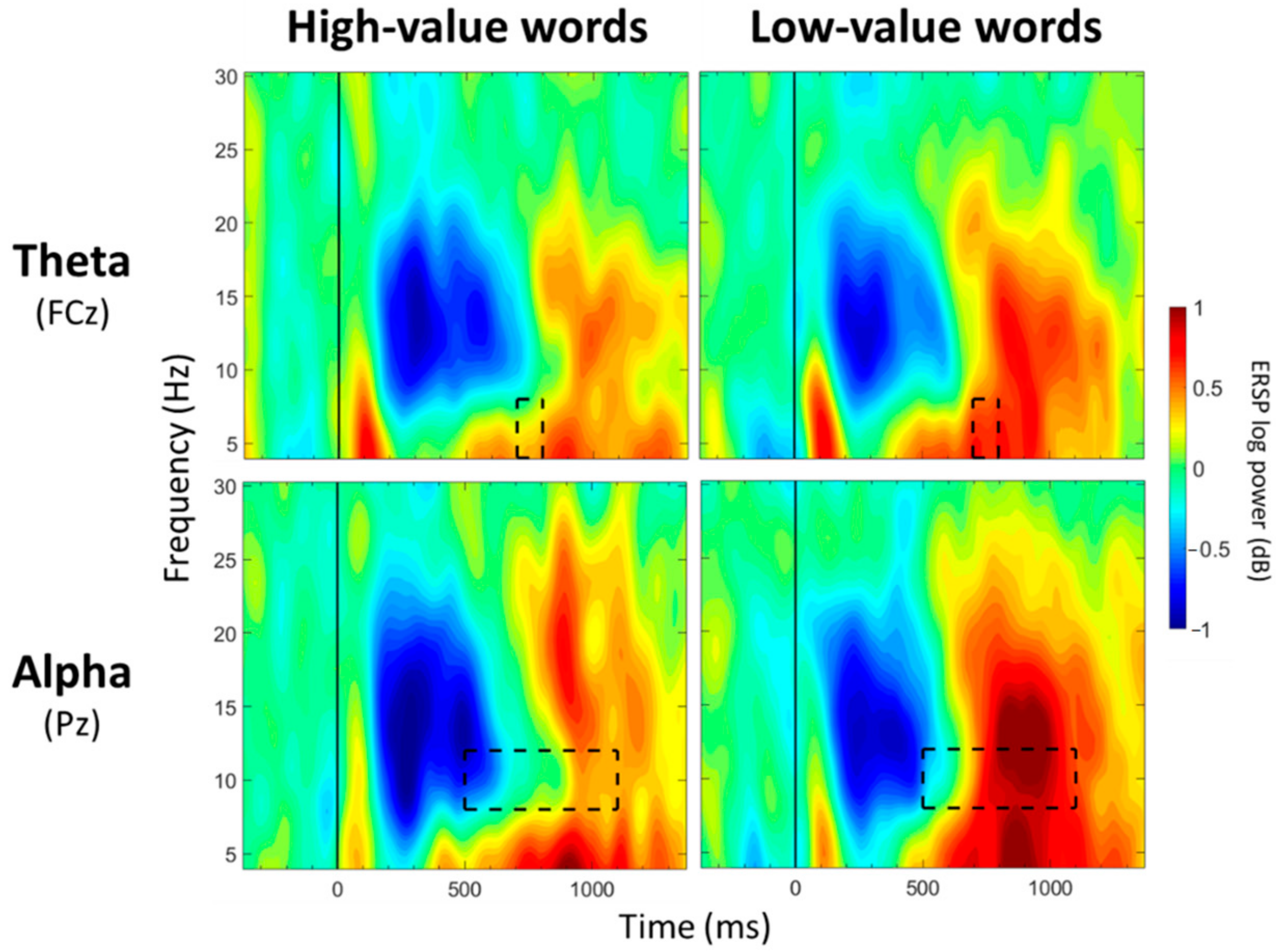
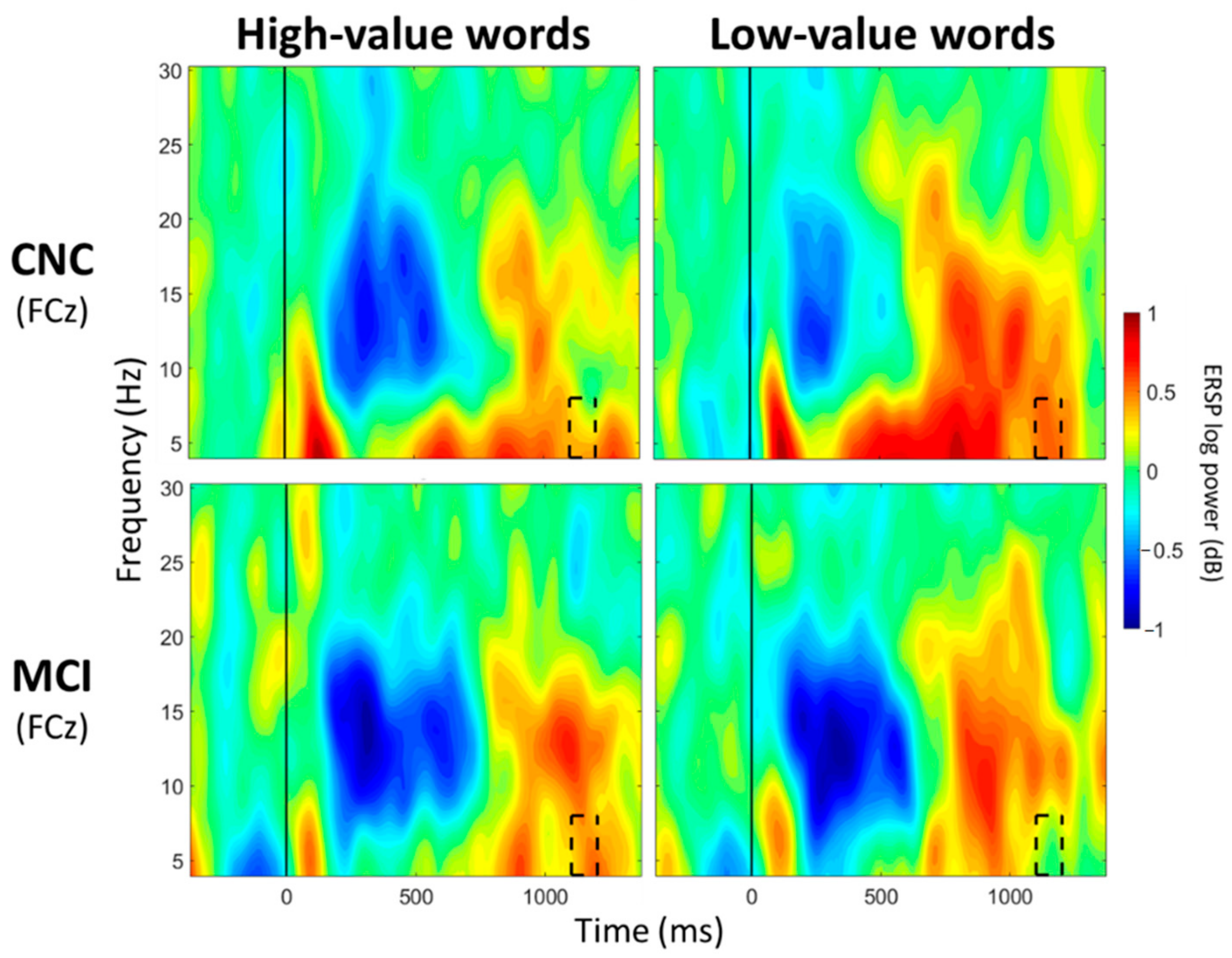
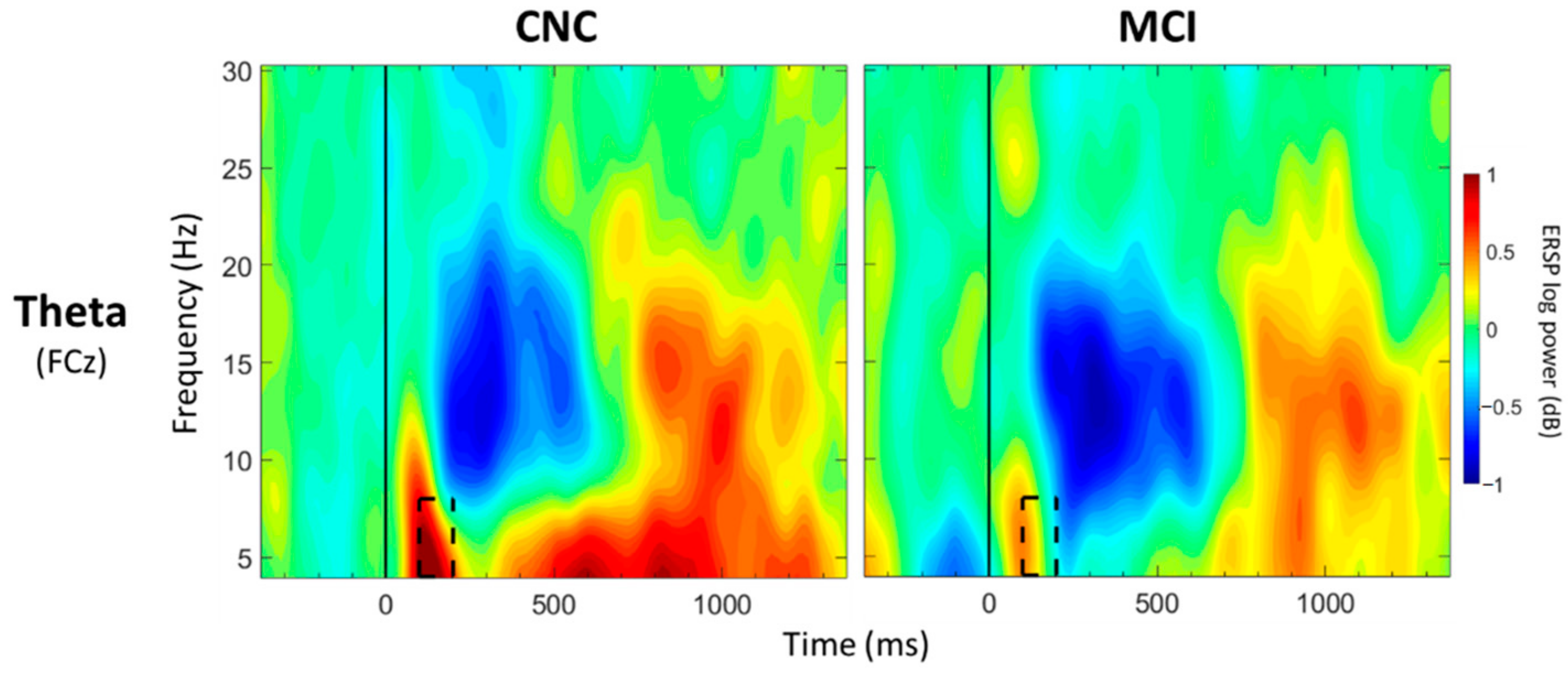
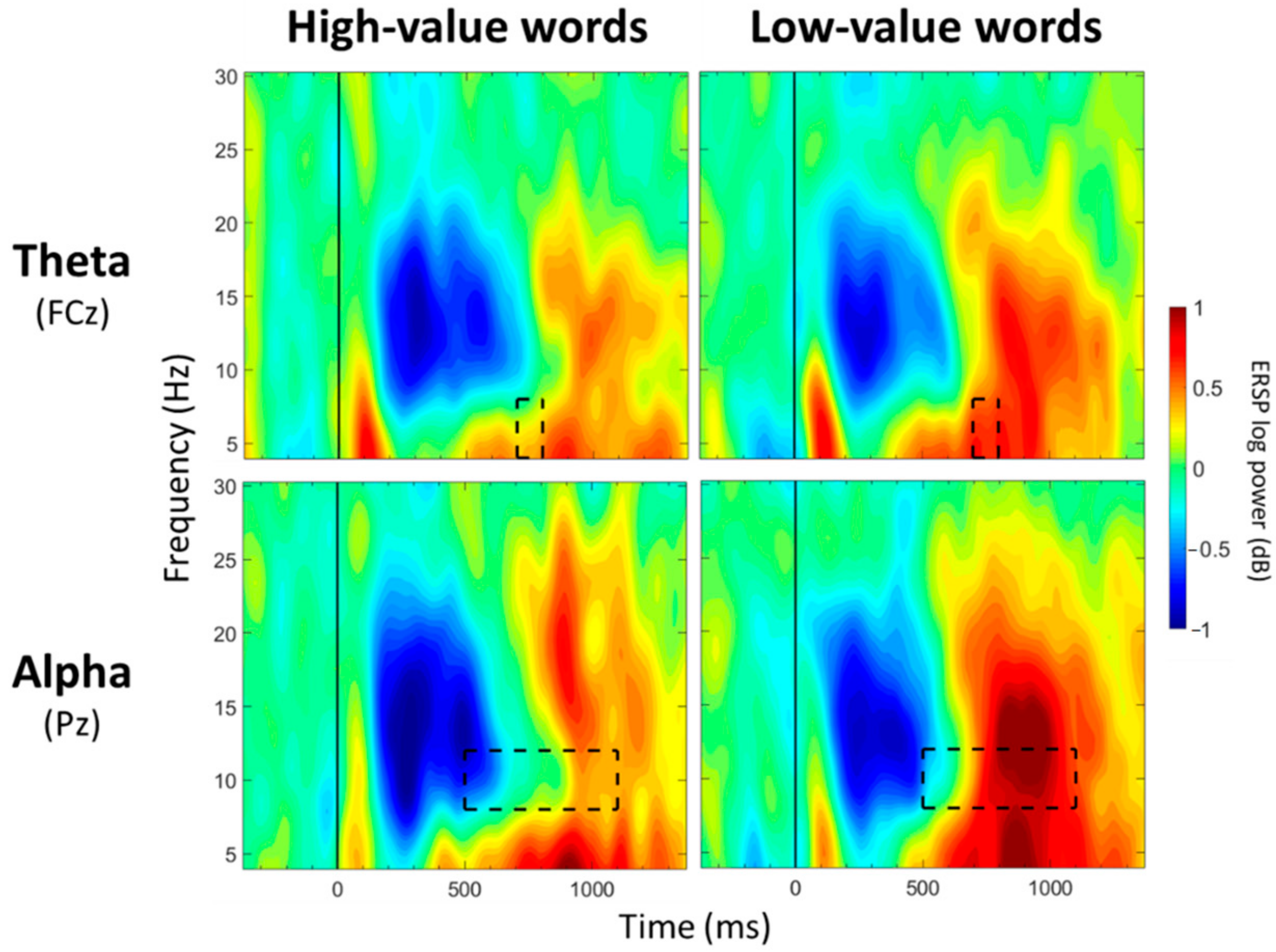
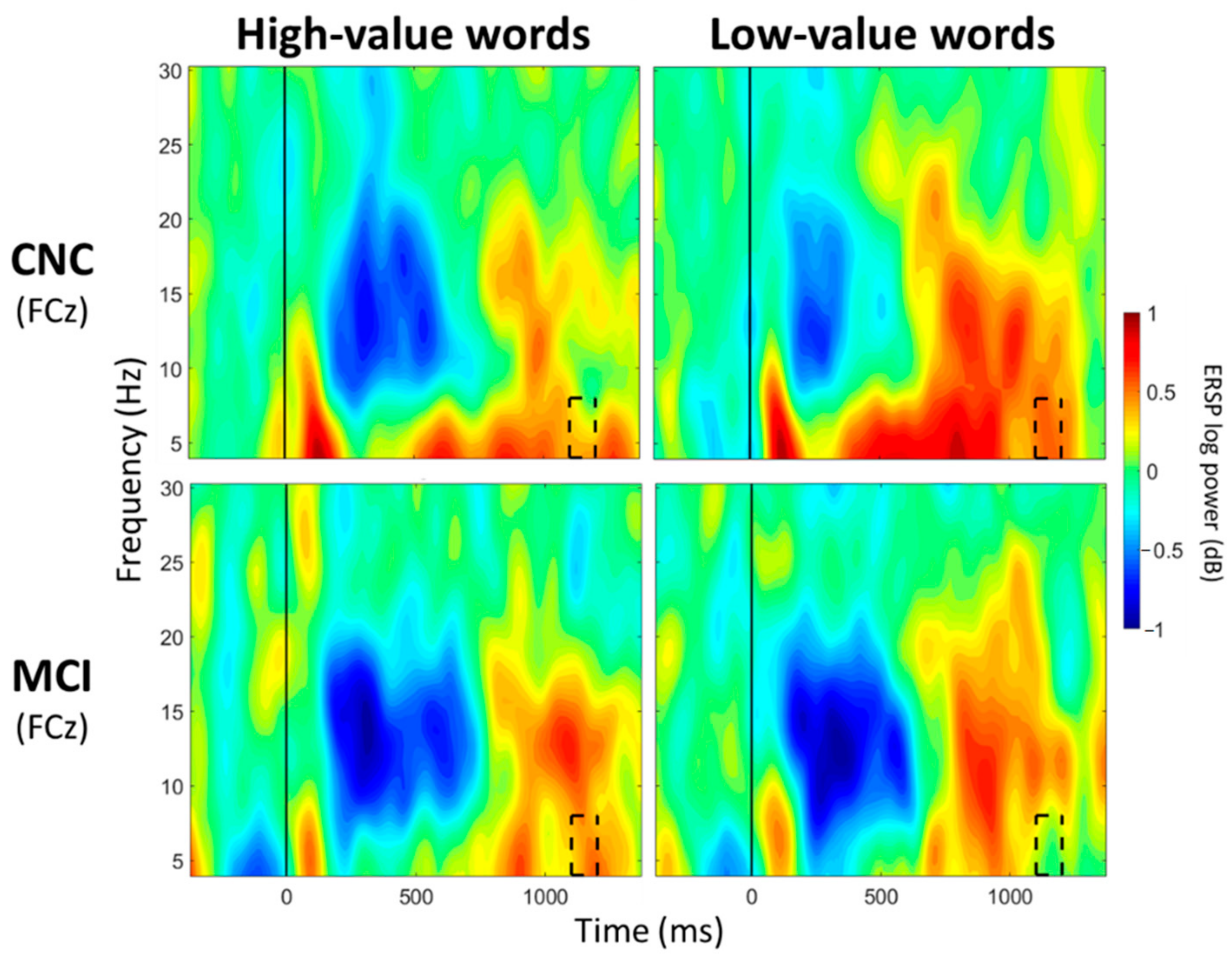
3.2. Theta Band (4–8 Hz) Mean Power
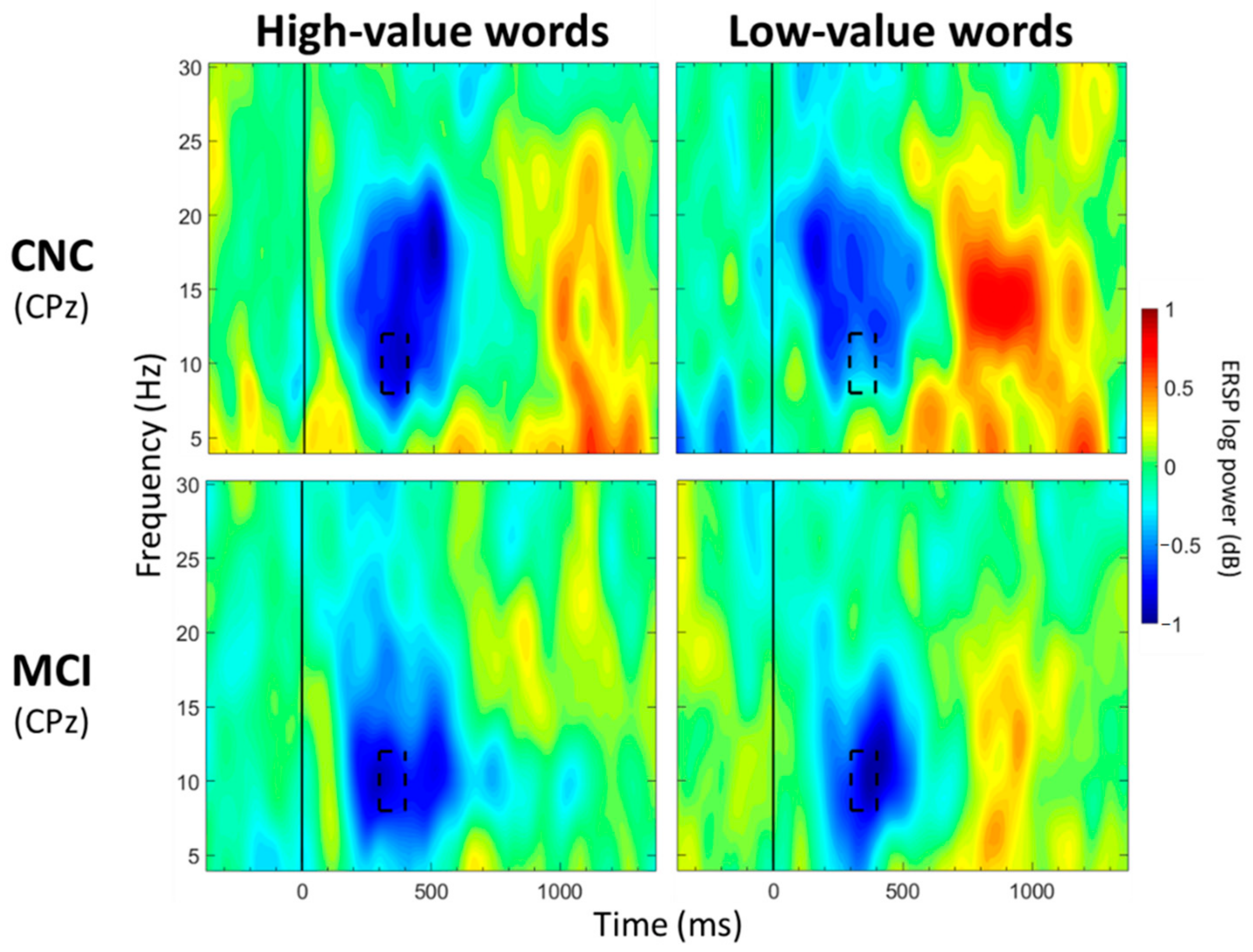
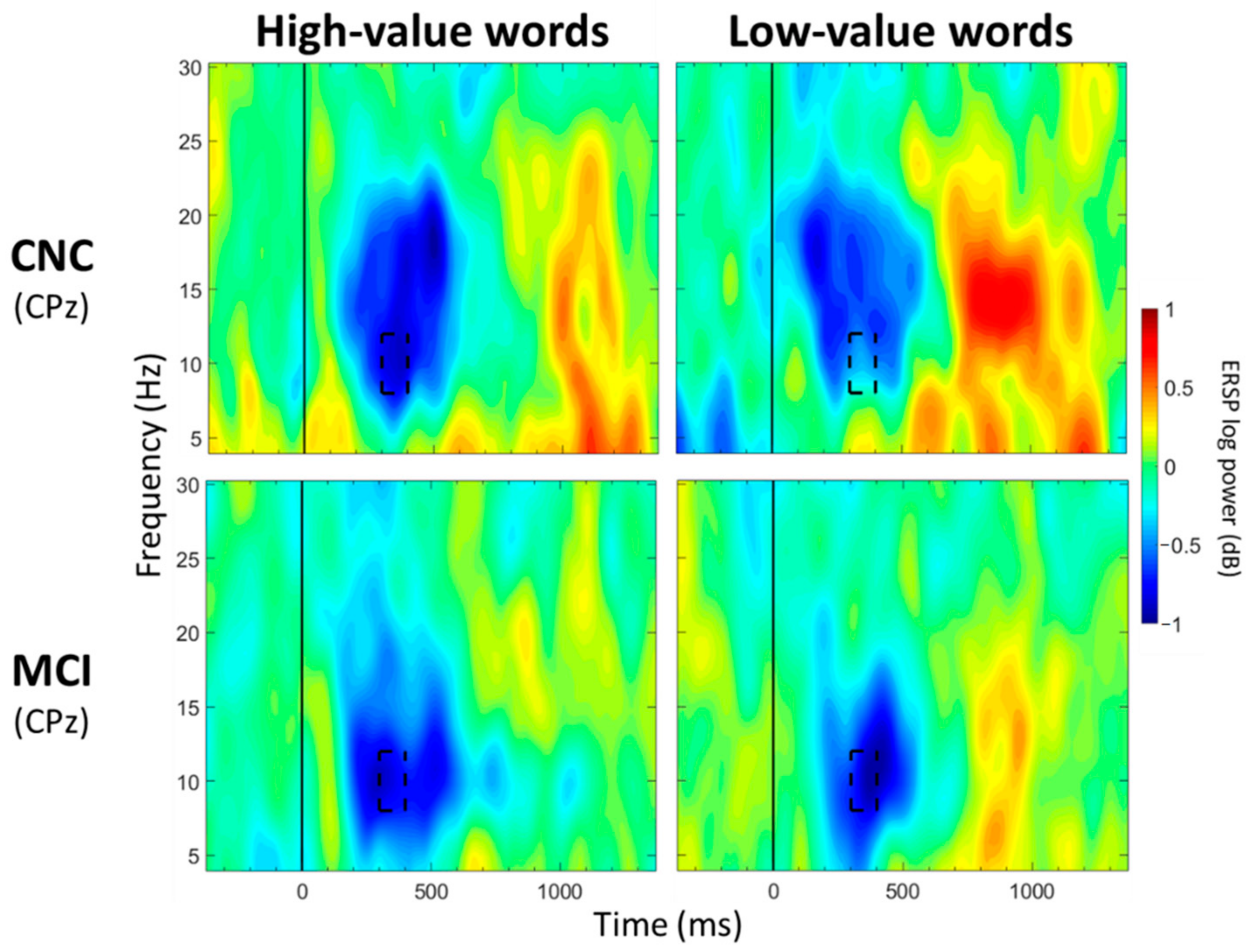
3.3. Alpha Band (8–12 Hz) Mean Power
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Castel, A.D. The Adaptive and Strategic Use of Memory by Older Adults: Evaluative Processing and Value-Directed Remembering. Psychol. Learn. Motiv. 2007, 48, 225–270. [Google Scholar] [CrossRef]
- Castel, A.D.; Benjamin, A.S.; Craik, F.I.M.; Watkins, M.J. The effects of aging on selectivity and control in short-term recall. Mem. Cognit. 2002, 30, 1078–1085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castel, A.D.; Farb, N.A.; Craik, F. Memory for general and specific value information in younger and older adults: Measuring the limits of strategic control. Mem. Cognit. 2007, 35, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Castel, A.D.; Humphreys, K.L.; Lee, S.S.; Galván, A.; Balota, D.A.; McCabe, D.P. The development of memory efficiency and value-directed remembering across the life span: A cross-sectional study of memory and selectivity. Dev. Psychol. 2011, 47, 1553–1564. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, L.T.; Marini, F.; Shende, S.A.; Llano, D.A.; Mudar, R.A. Investigating EEG theta and alpha oscillations as measures of value-directed strategic processing in cognitively normal younger and older adults. Behav. Brain Res. 2020, 391, 112702. [Google Scholar] [CrossRef]
- Castel, A.D.; Balota, D.A.; McCabe, D.P. Memory efficiency and the strategic control of attention at encoding: Impairments of value-directed remembering in Alzheimer’s disease. Neuropsychology 2009, 23, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.; Irish, M.; Savage, G.; Hodges, J.R.; Piguet, O.; Hornberger, M. Strategic value-directed learning and memory in Alzheimer’s disease and behavioural-variant frontotemporal dementia. J. Neuropsychol. 2018, 13, 328–353. [Google Scholar] [CrossRef] [Green Version]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C. Mild Cognitive Impairment. N. Engl. J. Med. 2011, 364, 2227–2234. [Google Scholar] [CrossRef] [Green Version]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack Jr, C.R.; Kaye, J.; Montine, T.J.; et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef] [Green Version]
- Farias, S.T.; Mungas, D.; Reed, B.R.; Harvey, D.; DeCarli, C. Progression of mild cognitive impairment to dementia in clinic- vs community-based cohorts. Arch. Neurol. 2009, 66, 1151–1157. [Google Scholar] [CrossRef] [Green Version]
- Manly, J.J.; Tang, M.X.; Schupf, N.; Stern, Y.; Vonsattel, J.P.; Mayeux, R. Frequency and course of mild cognitive impairment in a multiethnic community. Ann. Neurol. 2008, 63, 494–506. [Google Scholar] [CrossRef] [Green Version]
- Plassman, B.L.; Langa, K.M.; Fisher, G.G.; Heeringa, S.G.; Weir, D.R.; Ofstedal, M.B.; Burke, J.R.; Hurd, M.D.; Potter, G.G.; Rodgers, W.L.; et al. Prevalence of cognitive impairment without dementia in the United States. Ann. Intern. Med. 2008, 148, 427–434. [Google Scholar] [CrossRef] [Green Version]
- De Jager, C.A.; Hogervorst, E.; Combrinck, M.; Budge, M.M. Sensitivity and specificity of neuropsychological tests for mild cognitive impairment, vascular cognitive impairment and Alzheimer’s disease. Psychol. Med. 2003, 33, 1039–1050. [Google Scholar] [CrossRef]
- De Jager, C.A.; Budge, M.M. Stability and predictability of the classification of mild cognitive impairment as assessed by episodic memory test performance over time. Neurocase 2005, 11, 72–79. [Google Scholar] [CrossRef]
- Salmon, D.P. Neuropsychological features of mild cognitive impairment and preclinical Alzheimer’s disease. Curr. Top. Behav. Neurosci. 2012, 10, 187–212. [Google Scholar] [CrossRef]
- Greenaway, M.C.; Lacritz, L.H.; Binegar, D.; Weiner, M.F.; Lipton, A.; Munro Cullum, C. Patterns of verbal memory performance in mild cognitive impairment, Alzheimer disease, and normal aging. Cogn. Behav. Neurol. 2006, 19, 79–84. [Google Scholar] [CrossRef]
- Libon, D.J.; Xie, S.X.; Eppig, J.; Wicas, G.; Lamar, M.; Lippa, C.; Bettcher, B.M.; Price, C.C.; Giovannetti, T.; Swenson, R.; et al. The heterogeneity of mild cognitive impairment: A neuropsychological analysis. J. Int. Neuropsychol. Soc. 2010, 16, 84–93. [Google Scholar] [CrossRef] [Green Version]
- Libon, D.J.; Bondi, M.W.; Price, C.C.; Lamar, M.; Eppig, J.; Wambach, D.M.; Nieves, C.; Delano-Wood, L.; Giovannetti, T.; Lippa, C.; et al. Verbal serial list learning in mild cognitive impairment: A profile analysis of interference, forgetting, and errors. J. Int. Neuropsychol. Soc. 2011, 17, 905–914. [Google Scholar] [CrossRef] [Green Version]
- Mistridis, P.; Krumm, S.; Monsch, A.U.; Berres, M.; Taylor, K.I. The 12 Years Preceding Mild Cognitive Impairment Due to Alzheimer’s Disease: The Temporal Emergence of Cognitive Decline. J. Alzheimer’s Dis. 2015, 48, 1095–1107. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Ribeiro, F.; Guerreiro, M.; De Mendonca, A. Verbal learning and memory deficits in Mild Cognitive Impairment. J. Clin. Exp. Neuropsychol. 2007, 29, 187–197. [Google Scholar] [CrossRef]
- Teng, E.; Tingus, K.D.; Lu, P.H.; Cummings, J.L. Persistence of neuropsychological testing deficits in mild cognitive impairment. Dement. Geriatr. Cogn. Disord. 2009, 28, 168–178. [Google Scholar] [CrossRef] [Green Version]
- Arnaiz, E.; Almkvist, O. Neuropsychological features of mild cognitive impairment and preclinical Alzheimer’s disease. Acta Neurol. Scand. Suppl. 2003, 179, 34–41. [Google Scholar] [CrossRef]
- Belleville, S.; Chertkow, H.; Gauthier, S. Working memory and control of attention in persons with Alzheimer’s disease and mild cognitive impairment. Neuropsychology 2007, 21, 458–469. [Google Scholar] [CrossRef]
- McLaughlin, P.M.; Borrie, M.J.; Murtha, S.J.E. Shifting efficacy, distribution of attention and controlled processing in two subtypes of mild cognitive impairment: Response time performance and intraindividual variability on a visual search task. Neurocase 2010, 16, 408–417. [Google Scholar] [CrossRef]
- McLaughlin, P.M.; Anderson, N.D.; Rich, J.B.; Chertkow, H.; Murtha, S.J.E. Visual Selective Attention in Amnestic Mild Cognitive Impairment. J. Gerontol. Ser. B 2013, 69, 881–891. [Google Scholar] [CrossRef] [Green Version]
- Okonkwo, O.C.; Wadley, V.G.; Ball, K.; Vance, D.E.; Crowe, M. Dissociations in visual attention deficits among persons with mild cognitive impairment. Neuropsychol. Dev. Cogn. Sect. B Aging Neuropsychol. Cogn. 2008, 15, 492–505. [Google Scholar] [CrossRef] [PubMed]
- Saunders, N.L.J.; Summers, M.J. Attention and working memory deficits in mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2009, 32, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Saunders, N.L.; Summers, M.J. Longitudinal deficits to attention, executive, and working memory in subtypes of mild cognitive impairment. Neuropsychology 2011, 25, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Tales, A.; Haworth, J.; Nelson, S.; Snowden, R.J.; Wilcock, G. Abnormal visual search in mild cognitive impairment and Alzheimer’s disease. Neurocase 2005, 11, 80–84. [Google Scholar] [CrossRef]
- Tales, A.; Bayer, A.J.; Haworth, J.; Snowden, R.J.; Philips, M.; Wilcock, G. Visual Search in Mild Cognitive Impairment: A Longitudinal Study. J. Alzheimer’s Dis. 2011, 24, 151–160. [Google Scholar] [CrossRef] [Green Version]
- Bélanger, S.; Belleville, S.; Gauthier, S. Inhibition impairments in Alzheimer’s disease, mild cognitive impairment and healthy aging: Effect of congruency proportion in a Stroop task. Neuropsychologia 2010, 48, 581–590. [Google Scholar] [CrossRef]
- Bélanger, S.; Belleville, S. Semantic inhibition impairment in mild cognitive impairment: A distinctive feature of upcoming cognitive decline? Neuropsychology 2009, 23, 592–606. [Google Scholar] [CrossRef] [Green Version]
- Chow, R.; Rabi, R.; Paracha, S.; Vasquez, B.P.; Hasher, L.; Alain, C.; Anderson, N.D. Reaction Time Intraindividual Variability Reveals Inhibitory Deficits in Single- and Multiple-Domain Amnestic Mild Cognitive Impairment. J. Gerontol. B Psychol. Sci. Soc. Sci. 2022, 77, 71–83. [Google Scholar] [CrossRef]
- Traykov, L.; Raoux, N.; Latour, F.; Gallo, L.; Hanon, O.; Baudic, S.; Bayle, C.; Wenisch, E.; Remy, P.; Rigaud, A.-S. Executive functions deficit in mild cognitive impairment. Cogn. Behav. Neurol. 2007, 20, 219–224. [Google Scholar] [CrossRef] [Green Version]
- Wylie, S.A.; Ridderinkhof, K.R.; Eckerle, M.K.; Manning, C.A. Inefficient response inhibition in individuals with mild cognitive impairment. Neuropsychologia 2007, 45, 1408–1419. [Google Scholar] [CrossRef]
- Zheng, D.; Dong, X.; Sun, H.; Xu, Y.; Ma, Y.; Wang, X. The overall impairment of core executive function components in patients with amnestic mild cognitive impairment: A cross-sectional study. BMC Neurol. 2012, 12, 138. [Google Scholar] [CrossRef] [Green Version]
- Jack, C.R., Jr.; Holtzman, D.M. Biomarker modeling of Alzheimer’s disease. Neuron 2013, 80, 1347–1358. [Google Scholar] [CrossRef] [Green Version]
- Jack, C.R.; Knopman, D.S.; Jagust, W.J.; Petersen, R.C.; Weiner, M.W.; Aisen, P.S.; Shaw, L.M.; Vemuri, P.; Wiste, H.J.; Weigand, S.D.; et al. Tracking pathophysiological processes in Alzheimer’s disease: An updated hypothetical model of dynamic biomarkers. Lancet Neurol. 2013, 12, 207–216. [Google Scholar] [CrossRef] [Green Version]
- Pfurtscheller, G.; Lopes da Silva, F.H. Event-related EEG/MEG synchronization and desynchronization: Basic principles. Clin. Neurophysiol. 1999, 110, 1842–1857. [Google Scholar] [CrossRef]
- Nguyen, L.T.; Marini, F.; Zacharczuk, L.; Llano, D.A.; Mudar, R.A. Theta and alpha band oscillations during value-directed strategic processing. Behav. Brain Res. 2019, 367, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Caravaglios, G.; Muscoso, E.G.; Di Maria, G.; Costanzo, E. Patients with mild cognitive impairment have an abnormal upper-alpha event-related desynchronization/synchronization (ERD/ERS) during a task of temporal attention. J. Neural. Transm. 2015, 122, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Cummins, T.D.; Broughton, M.; Finnigan, S. Theta oscillations are affected by amnestic mild cognitive impairment and cognitive load. Int. J. Psychophysiol. 2008, 70, 75–81. [Google Scholar] [CrossRef]
- Deiber, M.-P.; Ibanez, V.; Missonnier, P.; Herrmann, F.; Fazio-Costa, L.; Gold, G.; Giannakopoulos, P. Abnormal-induced theta activity supports early directed-attention network deficits in progressive MCI. Neurobiol. Aging 2009, 30, 1444–1452. [Google Scholar] [CrossRef]
- Deiber, M.-P.; Meziane, H.B.; Hasler, R.; Rodriguez, C.; Toma, S.; Ackermann, M.; Herrmann, F.; Giannakopoulos, P. Attention and Working Memory-Related EEG Markers of Subtle Cognitive Deterioration in Healthy Elderly Individuals. J. Alzheimer’s Dis. 2015, 47, 335–349. [Google Scholar] [CrossRef]
- Fraga, F.J.; Mamani, G.Q.; Johns, E.; Tavares, G.; Falk, T.H.; Phillips, N.A. Early diagnosis of mild cognitive impairment and Alzheimer’s with event-related potentials and event-related desynchronization in N-back working memory tasks. Comput. Methods Progr. Biomed. 2018, 164, 1–13. [Google Scholar] [CrossRef]
- Goodman, M.S.; Zomorrodi, R.; Kumar, S.; Barr, M.S.; Daskalakis, Z.J.; Blumberger, D.M.; Fischer, C.E.; Flint, A.; Mah, L.; Herrmann, N.; et al. Changes in Theta but not Alpha Modulation Are Associated with Impairment in Working Memory in Alzheimer’s Disease and Mild Cognitive Impairment. J. Alzheimer’s Dis. 2019, 68, 1085–1094. [Google Scholar] [CrossRef]
- Nguyen, L.T.; Mudar, R.A.; Chiang, H.S.; Schneider, J.M.; Maguire, M.J.; Kraut, M.A.; Hart, J. Theta and alpha alterations in amnestic mild cognitive impairment in semantic Go/NoGo tasks. Front. Aging Neurosci. 2017, 9, 1999. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef]
- Petersen, R.C.; Caracciolo, B.; Brayne, C.; Gauthier, S.; Jelic, V.; Fratiglioni, L. Mild cognitive impairment: A concept in evolution. J. Intern. Med. 2014, 275, 214–228. [Google Scholar] [CrossRef]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nasreddine, Z.; Phillips, N.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Bergeron, D.; Flynn, K.; Verret, L.; Poulin, S.; Bouchard, R.W.; Bocti, C.; Fulop, T.; Lacombe, G.; Gauthier, S.; Nasreddine, Z.; et al. Multicenter Validation of an MMSE-MoCA Conversion Table. J. Am. Geriatr. Soc. 2017, 65, 1067–1072. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Coltheart, M. The MRC Psycholinguistic Database. Q. J. Exp. Psychol. Sect. A 1981, 33, 497–505. [Google Scholar] [CrossRef]
- Brysbaert, M.; New, B. Moving beyond Kučera and Francis: A critical evaluation of current word frequency norms and the introduction of a new and improved word frequency measure for American English. Behav. Res. Methods 2009, 41, 977–990. [Google Scholar] [CrossRef] [Green Version]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Grandchamp, R.; Delorme, A. Single-trial normalization for event-related spectral decomposition reduces sensitivity to noisy trials. Front. Psychol. 2011, 2, 236. [Google Scholar] [CrossRef] [Green Version]
- Cavanagh, J.F.; Frank, M.J. Frontal theta as a mechanism for cognitive control. Trends Cogn. Sci. 2014, 18, 414–421. [Google Scholar] [CrossRef] [Green Version]
- Hanslmayr, S.; Staudig, T.; Fellner, M.C. Oscillatory power decreases and long-term memory: The information via desynchronization hypothesis. Front. Hum. Neurosci. 2012, 6, 74. [Google Scholar] [CrossRef] [Green Version]
- Ishii, R.; Shinosaki, K.; Ukai, S.; Inouye, T.; Ishihara, T.; Yoshimine, T.; Hirabuki, N.; Asada, H.; Kihara, T.; Robinson, S.E.; et al. Medial prefrontal cortex generates frontal midline theta rhythm. Neuroreport 1999, 10, 675–679. [Google Scholar] [CrossRef]
- Kawasaki, M.; Kitajo, K.; Yamaguchi, Y. Dynamic links between theta executive functions and alpha storage buffers in auditory and visual working memory. Eur. J. Neurosci. 2010, 31, 1683–1689. [Google Scholar] [CrossRef] [Green Version]
- Grunwald, M.; Busse, F.; Hensel, A.; Riedel-Heller, S.; Kruggel, F.; Arendt, T.; Wolf, H.; Gertz, H.J. Theta-power differences in patients with mild cognitive impairment under rest condition and during haptic tasks. Alzheimer Dis. Assoc. Disord. 2002, 16, 40–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luckhaus, C.; Grass-Kapanke, B.; Blaeser, I.; Ihl, R.; Supprian, T.; Winterer, G.; Zielasek, J.; Brinkmeyer, J. Quantitative EEG in progressing vs stable mild cognitive impairment (MCI): Results of a 1-year follow-up study. Int. J. Geriatr. Psychiatry 2008, 23, 1148–1155. [Google Scholar] [CrossRef] [PubMed]
- Mazaheri, A.; Segaert, K.; Olichney, J.; Yang, J.C.J.-C.; Niu, Y.-Q.; Shapiro, K.; Bowman, H. EEG oscillations during word processing predict MCI conversion to Alzheimer’s disease. NeuroImage Clin. 2018, 17, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Missonnier, P.; Gold, G.; Herrmann, F.R.; Fazio-Costa, L.; Michel, J.-P.; Deiber, M.-P.; Michon, A.; Giannakopoulos, P. Decreased theta event-related synchronization during working memory activation is associated with progressive mild cognitive impairment. Dement. Geriatr. Cogn. Disord. 2006, 22, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Knowlton, B.J.; Castel, A.D. Memory and reward-based learning: A value-directed remembering perspective. Annu. Rev. Psychol. 2022, 73, 25–52. [Google Scholar] [CrossRef]
- Murphy, D.H.; Castel, A.D. The role of attention and aging in the retrieval dynamics of value-directed remembering. Q. J. Exp. Psychol. 2022, 75, 954–968. [Google Scholar] [CrossRef]
- Malek-Ahmadi, M.; Raj, A.; Small, B.J. Semantic clustering as a neuropsychological predictor for amnestic-MCI. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2011, 18, 280–292. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, P.M.; Wright, M.J.; Larocca, M.; Nguyen, P.T.; Teng, E.; Apostolova, L.G.; Ringman, J.M.; Zhou, Y.; Cummings, J.L.; Woo, E. The “Alzheimer’s type” profile of semantic clustering in amnestic mild cognitive impairment. J. Int. Neuropsychol. Soc. 2014, 20, 402–412. [Google Scholar] [CrossRef] [Green Version]
- Price, S.E.; Kinsella, G.J.; Ong, B.; Mullaly, E.; Phillips, M.; Pangnadasa-Fox, L.; Perre, D.; Storey, E. Learning and memory in amnestic mild cognitive impairment: Contribution of working memory. J. Int. Neuropsychol. Soc. 2010, 16, 342–351. [Google Scholar] [CrossRef]
- Hennessee, J.P.; Patterson, T.K.; Castel, A.D.; Knowlton, B.J. Forget me not: Encoding processes in value-directed remembering. J. Mem. Lang. 2019, 106, 29–39. [Google Scholar] [CrossRef] [Green Version]
- Cavanagh, J.F.; Shackman, A.J. Frontal midline theta reflects anxiety and cognitive control: Meta-analytic evidence. J. Physiol.-Paris 2015, 109, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Nigbur, R.; Ivanova, G.; Stürmer, B. Theta power as a marker for cognitive interference. Clin. Neurophysiol. 2011, 122, 2185–2194. [Google Scholar] [CrossRef]
- Hanslmayr, S.; Spitzer, B.; Bäuml, K.H. Brain oscillations dissociate between semantic and nonsemantic encoding of episodic memories. Cereb. Cortex 2009, 19, 1631–1640. [Google Scholar] [CrossRef] [Green Version]
- Klimesch, W. EEG alpha and theta oscillations reflect cognitive and memory performance: A review and analysis. Brain research. Brain Res. Rev. 1999, 29, 169–195. [Google Scholar] [CrossRef]
- Cohen, M.S.; Rissman, J.; Suthana, N.A.; Castel, A.D.; Knowlton, B.J. Effects of aging on value-directed modulation of semantic network activity during verbal learning. NeuroImage 2016, 125, 1046–1062. [Google Scholar] [CrossRef] [Green Version]
- Hennessee, J.P.; Reggente, N.; Cohen, M.S.; Rissman, J.; Castel, A.D.; Knowlton, B.J. White matter integrity in brain structures supporting semantic processing is associated with value-directed remembering in older adults. Neuropsychologia 2019, 129, 246–254. [Google Scholar] [CrossRef] [Green Version]
- Bell-McGinty, S.; Lopez, O.L.; Meltzer, C.C.; Scanlon, J.M.; Whyte, E.M.; Dekosky, S.T.; Becker, J.T. Differential cortical atrophy in subgroups of mild cognitive impairment. Arch. Neurol. 2005, 62, 1393–1397. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.F.; Huang, L.L.; Li, H.Y.; Qian, Y.; Yang, D.; Qing, Z.; Luo, C.M.; Li, M.C.; Zhang, B.; Xu, Y. Microstructural disruption of the right inferior fronto-occipital and inferior longitudinal fasciculus contributes to WMH-related cognitive impairment. CNS Neurosci. Ther. 2020, 26, 576–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karas, G.; Sluimer, J.; Goekoop, R.; van der Flier, W.; Rombouts, S.A.; Vrenken, H.; Scheltens, P.; Fox, N.; Barkhof, F. Amnestic mild cognitive impairment: Structural MR imaging findings predictive of conversion to Alzheimer disease. AJNR Am. J. Neuroradiol. 2008, 29, 944–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Zheng, G.; Zheng, Y.; Xiong, Z.; Xia, R.; Zhou, W.; Wang, Q.; Liang, S.; Tao, J.; Chen, L. Alterations in resting-state functional connectivity of the default mode network in amnestic mild cognitive impairment: An fMRI study. BMC Med. Imaging 2017, 17, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, D.B.; Ryman, S.G.; Hartman, A.P.; Wertz, C.J.; Vakhtin, A.A.; Alzheimer’s Disease Neuroimaging Initiative. Specific white matter tracts and diffusion properties predict conversion from mild cognitive impairment to Alzheimer’s disease. Front. Aging Neurosci. 2021, 13, 711579. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, Y.; Lan, K.; Huang, X.; He, Y.; Yang, F.; Li, J.; Hu, Q.; Xu, J.; Yu, H. Gray matter atrophy in amnestic mild cognitive impairment: A voxel-based meta-analysis. Front. Aging Neurosci. 2021, 13, 627919. [Google Scholar] [CrossRef]
- Coutinho, G.; Drummond, C.; de Oliveira-Souza, R.; Moll, J.; Tovar-Moll, F.; Mattos, P. Immediate story recall in elderly individuals with memory complaints: How much does it contribute to memory assessment? Int. Psychogeriatr. 2015, 27, 1679–1686. [Google Scholar] [CrossRef]
- De Simone, M.S.; Perri, R.; Fadda, L.; De Tollis, M.; Turchetta, C.S.; Caltagirone, C.; Carlesimo, G.A. Different deficit patterns on word lists and short stories predict conversion to Alzheimer’s disease in patients with amnestic mild cognitive impairment. J. Neurol. 2017, 264, 2258–2267. [Google Scholar] [CrossRef] [PubMed]
- Kavé, G.; Heinik, J. Neuropsychological evaluation of mild cognitive impairment: Three case reports. Clin. Neuropsychol. 2004, 18, 362–372. [Google Scholar] [CrossRef]
- Tremont, G.; Miele, A.; Smith, M.M.; Westervelt, H.J. Comparison of verbal memory impairment rates in mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2010, 32, 630–636. [Google Scholar] [CrossRef]
- Paller, K.A.; Wagner, A.D. Observing the transformation of experience into memory. Trends Cogn. Sci. 2002, 6, 93–102. [Google Scholar] [CrossRef]
- Wagner, A.D.; Koutstaal, W.; Schacter, D.L. When encoding yields remembering: Insights from event-related neuroimaging. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1999, 354, 1307–1324. [Google Scholar] [CrossRef]
- Werkle-Bergner, M.; Muller, V.; Li, S.-C.; Lindenberger, U. Cortical EEG correlates of successful memory encoding: Implications for lifespan comparisons. Neurosci. Biobehav. Rev. 2006, 30, 839–854. [Google Scholar] [CrossRef] [Green Version]
- Dunlosky, J.; Hertzog, C. Measuring strategy production during associative learning: The relative utility of concurrent versus retrospective reports. Mem. Cognit. 2001, 29, 247–253. [Google Scholar] [CrossRef]
- Taconnat, L.; Raz, N.; Toczé, C.; Bouazzaoui, B.; Sauzéon, H.; Fay, S.; Isingrini, M. Ageing and organisation strategies in free recall: The role of cognitive flexibility. Eur. J. Cogn. Psychol. 2009, 21, 347–365. [Google Scholar] [CrossRef]
- Witte, K.L.; Freund, J.S.; Brown-Whistler, S. Adult age differences in free recall and category clustering. Exp. Aging Res. 1993, 19, 15–28. [Google Scholar] [CrossRef]
- Kuhlmann, B.G.; Touron, D.R. Aging and memory improvement through semantic clustering: The role of list-presentation format. Psychol. Aging 2016, 31, 771–785. [Google Scholar] [CrossRef] [Green Version]
- Naveh-Benjamin, M.; Brav, T.K.; Levy, O. The associative memory deficit of older adults: The role of strategy utilization. Psychol. Aging 2007, 22, 202–208. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CNC (n = 18) | MCI (n = 18) | p-Value | |
|---|---|---|---|
| Demographics | |||
| Age (years) | 74.5 (4.7) | 76.7 (4.2) | 0.146 |
| Education (years) | 16.3 (3.0) | 16.0 (3.4) | 0.795 |
| Sex | 15F/3M | 15F/3M | 1.00 |
| Cognitive Testing | |||
| Montreal Cognitive Assessment | 27.4 (1.4) | 21.3 (3.9) | <0.001 ** |
| LM—Immediate (Story A) | 15.9 (3.2) a | 8.2 (3.1) a | <0.001 ** |
| LM—Delayed (Story A) | 14.1 (4.2) a | 4.0 (3.1) a | <0.001 ** |
| Letter fluency (F, A, S) | 49.2 (8.8) | 38.0 (14.4) | 0.008 ** |
| Category fluency (Animals) | 19.9 (4.0) | 13.9 (4.8) | <0.001 ** |
| Boston Naming Test (30 items) | 27.8 (1.6) | 26.6 (2.5) a | 0.116 |
| Trail Making Test A (s) | 27.7 (6.9) | 34.0 (16.6) | 0.145 |
| Trail Making Test B (s) | 80.2 (29.0) | 130.1 (59.1) | 0.003 ** |
| Digit span—forward | 6.5 (1.5) a | 7.0 (1.2) a | 0.347 |
| Digit span—backward | 5.1 (1.2) a | 5.2 (1.3) a | 0.880 |
| Main Effect: Group | Main Effect: Value | Interaction: Group x Value | ||
|---|---|---|---|---|
| List 1 | F(1,34) p | 34.62 <0.001 ** | 17.61 <0.001 ** | 8.08 0.008 ** |
| List 2 | F(1,34) p | 23.12 <0.001 ** | 51.85 <0.001 ** | 10.42 0.003 ** |
| List 3 | F(1,34) p | 26.22 <0.001 ** | 83.32 <0.001 ** | 8.70 0.006 ** |
| List 4 | F(1,34) p | 14.27 <0.001 ** | 54.22 <0.001 ** | 3.50 0.070 |
| List 5 | F(1,34) p | 30.26 <0.001 ** | 67.89 <0.001 ** | 7.79 0.009 ** |
| Time (ms) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–100 | 100–200 | 200–300 | 300–400 | 400–500 | 500–600 | 600–700 | 700–800 | 800–900 | 900–1000 | 1000–1100 | 1100–1200 | 1200–1300 | ||
| Theta (4–8 Hz) | ||||||||||||||
| Fz | F(1,34) p | 0.08 0.784 | 3.59 0.066 | 1.35 0.253 | 1.27 0.268 | 0.69 0.412 | 0.92 0.343 | 1.42 0.242 | 0.61 0.441 | 0.68 0.414 | 0.85 0.362 | 1.26 0.270 | 0.92 0.345 | 0.08 0.773 |
| FCz | F(1,34) p | 0.28 0.600 | 5.55 0.024 0.14 | 3.13 0.086 | 3.65 0.065 | 2.98 0.093 | 1.78 0.192 | 1.86 0.181 | 0.74 0.395 | 0.78 0.384 | 0.32 0.577 | 0.91 0.346 | 0.66 0.423 | 0.69 0.413 |
| Alpha (8–12 Hz) | ||||||||||||||
| CPz | F(1,34) p | 0.01 0.938 | 0.06 0.810 | 0.09 0.766 | 0.35 0.556 | 0.43 0.515 | 2.08 0.158 | 0.82 0.371 | 1.33 0.257 | 0.26 0.613 | 0.43 0.516 | 3.47 0.071 | 2.14 0.153 | 1.60 0.214 |
| Pz | F(1,34) p | 0.49 0.489 | 0.06 0.802 | 0.04 0.847 | 0.35 0.559 | 0.53 0.473 | 2.92 0.096 | 3.19 0.083 | 1.93 0.174 | 0.60 0.443 | 1.53 0.225 | 1.91 0.176 | 2.13 0.154 | 1.04 0.315 |
| Time (ms) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–100 | 100–200 | 200–300 | 300–400 | 400–500 | 500–600 | 600–700 | 700–800 | 800–900 | 900–1000 | 1000–1100 | 1100–1200 | 1200–1300 | ||
| Theta (4–8 Hz) | ||||||||||||||
| Fz | F(1,34) p | 0.59 0.446 | 0.06 0.805 | 0.00 0.977 | 0.42 0.519 | 0.57 0.454 | 1.94 0.172 | 2.43 0.129 | 3.13 0.086 | 3.20 0.083 | 1.87 0.180 | 1.28 0.266 | 0.54 0.468 | 0.58 0.452 |
| FCz | F(1,34) p | 0.60 0.444 | 0.24 0.625 | 0.03 0.874 | 0.29 0.595 | 2.77 0.105 | 0.74 0.396 | 1.84 0.183 | 6.21 0.018 0.15 | 1.65 0.207 | 0.90 0.351 | 0.01 0.937 | 0.01 0.942 | 0.45 0.506 |
| Alpha (8–12 Hz) | ||||||||||||||
| CPz | F(1,34) p | 0.00 0.977 | 0.09 0.767 | 1.36 0.252 | 3.78 0.060 | 0.15 0.699 | 7.81 0.008 0.19 | 3.73 0.062 | 13.34 0.001 0.28 | 11.45 0.002 0.25 | 6.90 0.013 0.17 | 1.73 0.197 | 0.08 0.772 | 0.00 0.982 |
| Pz | F(1,34) p | 0.47 0.495 | 0.00 0.971 | 0.97 0.332 | 0.00 0.973 | 0.00 0.973 | 6.23 0.018 0.16 | 11.61 0.002 0.26 | 27.89 <0.001 0.45 | 36.07 <0.001 0.52 | 19.44 <0.001 0.36 | 5.93 0.020 0.15 | 0.75 0.394 | 0.26 0.617 |
| Time (ms) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–100 | 100–200 | 200–300 | 300–400 | 400–500 | 500–600 | 600–700 | 700–800 | 800–900 | 900–1000 | 1000–1100 | 1100–1200 | 1200–1300 | ||
| Theta (4–8 Hz) | ||||||||||||||
| Fz | F(1,34) p | 0.07 0.793 | 0.49 0.490 | 0.02 0.875 | 1.33 0.258 | 0.54 0.467 | 0.35 0.560 | 0.17 0.681 | 1.88 0.179 | 0.15 0.699 | 0.00 0.994 | 0.40 0.532 | 1.26 0.269 | 0.49 0.489 |
| FCz | F(1,34) p | 0.17 0.681 | 0.40 0.533 | 2.15 0.152 | 2.01 0.166 | 2.60 0.116 | 2.09 0.157 | 0.76 0.391 | 2.17 0.150 | 0.89 0.352 | 0.17 0.681 | 0.00 0.989 | 4.76 0.036 0.12 | 0.34 0.566 |
| Alpha (8–12 Hz) | ||||||||||||||
| CPz | F(1,34) p | 0.20 0.662 | 0.02 0.902 | 0.94 0.339 | 5.85 0.021 0.15 | 0.95 0.336 | 0.12 0.733 | 0.03 0.857 | 0.29 0.592 | 0.10 0.757 | 0.40 0.530 | 1.22 0.276 | 0.03 0.854 | 0.02 0.886 |
| Pz | F(1,34) p | 1.17 0.287 | 0.10 0.755 | 0.03 0.864 | 3.18 0.084 | 3.09 0.088 | 2.42 0.129 | 0.97 0.331 | 2.01 0.165 | 2.37 0.133 | 0.11 0.747 | 0.29 0.593 | 0.03 0.870 | 0.00 0.992 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, L.T.; Lydon, E.A.; Shende, S.A.; Llano, D.A.; Mudar, R.A. Disrupted Value-Directed Strategic Processing in Individuals with Mild Cognitive Impairment: Behavioral and Neural Correlates. Geriatrics 2022, 7, 56. https://doi.org/10.3390/geriatrics7030056
Nguyen LT, Lydon EA, Shende SA, Llano DA, Mudar RA. Disrupted Value-Directed Strategic Processing in Individuals with Mild Cognitive Impairment: Behavioral and Neural Correlates. Geriatrics. 2022; 7(3):56. https://doi.org/10.3390/geriatrics7030056
Chicago/Turabian StyleNguyen, Lydia T., Elizabeth A. Lydon, Shraddha A. Shende, Daniel A. Llano, and Raksha A. Mudar. 2022. "Disrupted Value-Directed Strategic Processing in Individuals with Mild Cognitive Impairment: Behavioral and Neural Correlates" Geriatrics 7, no. 3: 56. https://doi.org/10.3390/geriatrics7030056
APA StyleNguyen, L. T., Lydon, E. A., Shende, S. A., Llano, D. A., & Mudar, R. A. (2022). Disrupted Value-Directed Strategic Processing in Individuals with Mild Cognitive Impairment: Behavioral and Neural Correlates. Geriatrics, 7(3), 56. https://doi.org/10.3390/geriatrics7030056