
Reasons for and against Nutritional Interventions. An Exploration in the Nursing Home Setting

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Residents’ Characteristics
2.4. Nutritional Status
2.5. Nutritional Interventions
2.6. Reasons for or against Nutritional Interventions
2.7. Data Analyses
3. Results
3.1. Residents’ Characteristics and Nutritional Status
3.2. Nutritional Interventions
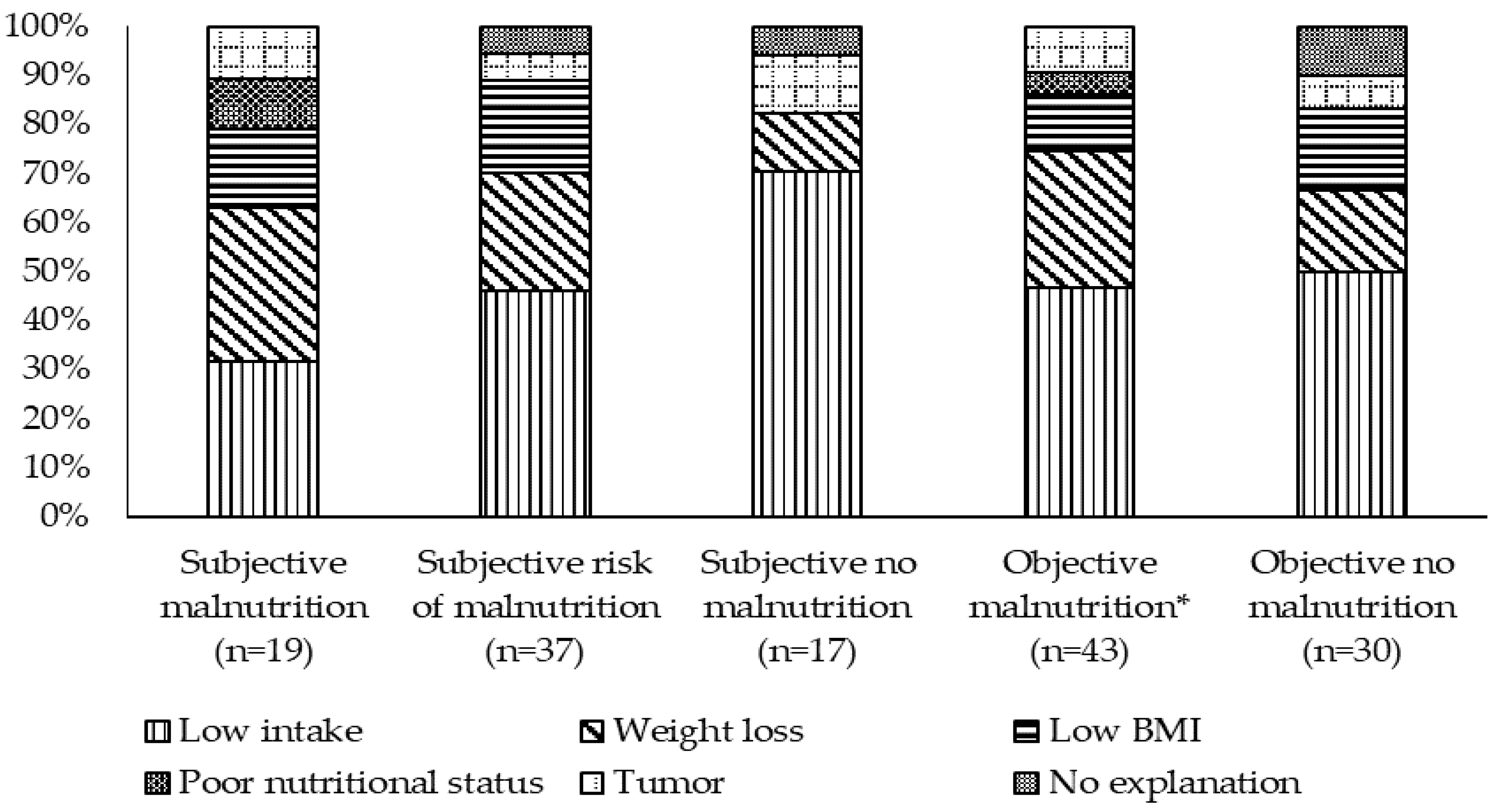
3.3. Reasons for Nutritional Interventions
3.4. Reasons against Nutritional Interventions
4. Discussion
4.1. Nutritional Interventions
4.2. Reasons for Nutritional Interventions
4.3. Reasons against Nutritional Interventions
4.4. Objective Malnutrition Criteria
4.5. Recognition of MN by Nurses
4.6. Strengths and Weaknesses of the Study
4.7. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Total | Subjective Judgement | Objective Criteria * | ||||
|---|---|---|---|---|---|---|
| n = 246 | MN n = 27 | At Risk n = 63 | No MN n = 156 | MN n = 81 | No MN n = 165 | |
| BMI [kg/m2], mean ± SD | 25.1 ± 5.2 | 17.7 ± 1.5 | 23.3 ± 2.5 | 27.1 ± 5.1 | 21.3 ± 3.9 | 27.0 ± 4.8 |
| BMI < 20 kg/m2, n (%) | 37 (15.0) | 25 (92.6) | 7 (11.1) | 5 (3.2) | 37 (45.7) | 0 (0.0) |
| Weight loss ≥ 5% in last 3 months, n (%) | 30 (12.2) | 7 (25.9) | 20 (31.7) | 3 (1.9) | 30 (37.0) | 0 (0.0) |
| Intake ≤ 1/4 of the meal, n (%) | 38 (15.4) | 12 (44.4) | 12 (19.0) | 14 (9.0) | 38 (46.9) | 0 (0.0) |
| Objective Criteria * | |||||
|---|---|---|---|---|---|
| MN | No MN | Total | |||
| MN | n | 27 | 0 | 27 | |
| row % | (100.0) | (0.0) | (100.0) | ||
| column % | (33.3) | (0.0) | (11.0) | ||
| n | 33 | 30 | 63 | ||
| Subjective | At risk | row % | (52.4) | (47.6) | (100.0) |
| judgement | column % | (40.7) | (18.2) | (25.6) | |
| n | 21 | 135 | 156 | ||
| No MN | No MN row % | (13.5) | (86.5) | (100.0) | |
| Column % | (25.9) | (81.8) | (63.4) | ||
| n | 165 | 81 | 246 | ||
| Total | row % | (67.1) | (32.9) | (100.0) | |
| coumn % | (100.0) | (100.0) | (100.0) | ||
References
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolters, M.; Volkert, D.; Streicher, M.; Kiesswetter, E.; Torbahn, G.; O’Connor, E.M.; O’Keeffe, M.; Kelly, M.; O’Herlihy, E.; O’Toole, P.W. Prevalence of malnutrition using harmonized definitions in older adults from different settings–A MaNuEL study. Clin. Nutr. 2019, 38, 2389–2398. [Google Scholar] [CrossRef] [Green Version]
- Volkert, D.; Pauly, L.; Stehle, P.; Sieber, C.C. Prevalence of malnutrition in orally and tube-fed elderly nursing home residents in Germany and its relation to health complaints and dietary intake. Gastroenterol. Res. Pract. 2011, 2011, 247315. [Google Scholar] [CrossRef] [PubMed]
- Tamura, B.K.; Bell, C.L.; Masaki, K.H.; Amella, E.J. Factors associated with weight loss, low BMI, and malnutrition among nursing home patients: A systematic review of the literature. J. Am. Med. Dir. Assoc. 2013, 14, 649–655. [Google Scholar] [CrossRef]
- Baldwin, C.; Kimber, K.L.; Gibbs, M.; Weekes, C.E. Supportive interventions for enhancing dietary intake in malnourished or nutritionally at-risk adults. Cochrane Database Syst. Rev. 2016, 12, Cd009840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muscaritoli, M.; Krznarić, Z.; Singer, P.; Barazzoni, R.; Cederholm, T.; Golay, A.; Van Gossum, A.; Kennedy, N.; Kreymann, G.; Laviano, A.; et al. Effectiveness and efficacy of nutritional therapy: A systematic review following Cochrane methodology. Clin. Nutr. 2017, 36, 939–957. [Google Scholar] [CrossRef]
- Abizanda, P.; Sinclair, A.; Barcons, N.; Lizán, L.; Rodríguez-Mañas, L. Costs of Malnutrition in Institutionalized and Community-Dwelling Older Adults: A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 17–23. [Google Scholar] [CrossRef]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA(®). Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef]
- Bell, C.L.; Lee, A.S.; Tamura, B.K. Malnutrition in the nursing home. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 17–23. [Google Scholar] [CrossRef]
- Van Nie-Visser, N.C.; Meijers, J.; Schols, J.; Lohrmann, C.; Bartholomeyczik, S.; Spreeuwenberg, M.; Halfens, R. Which characteristics of nursing home residents influence differences in malnutrition prevalence? An international comparison of The Netherlands, Germany and Austria. Br. J. Nutr. 2014, 111, 1129–1136. [Google Scholar] [CrossRef] [Green Version]
- Streicher, M.; Themessl-Huber, M.; Schindler, K.; Sieber, C.C.; Hiesmayr, M.; Volkert, D. Who receives oral nutritional supplements in nursing homes? Results from the nutritionDay project. Clin. Nutr. 2017, 36, 1360–1371. [Google Scholar] [CrossRef]
- Valentini, L.; Schindler, K.; Schlaffer, R.; Bucher, H.; Mouhieddine, M.; Steininger, K.; Tripamer, J.; Handschuh, M.; Schuh, C.; Volkert, D.; et al. The first nutritionDay in nursing homes: Participation may improve malnutrition awareness. Clin. Nutr. 2009, 28, 109–116. [Google Scholar] [CrossRef]
- Stange, I.; Bartram, M.; Liao, Y.; Poeschl, K.; Kolpatzik, S.; Uter, W.; Sieber, C.C.; Stehle, P.; Volkert, D. Effects of a low-volume, nutrient- and energy-dense oral nutritional supplement on nutritional and functional status: A randomized, controlled trial in nursing home residents. J. Am. Med. Dir. Assoc. 2013, 14, 628.e1–628.e8. [Google Scholar] [CrossRef]
- Parsons, E.L.; Stratton, R.J.; Cawood, A.L.; Smith, T.R.; Elia, M. Oral nutritional supplements in a randomised trial are more effective than dietary advice at improving quality of life in malnourished care home residents. Clin. Nutr. 2017, 36, 134–142. [Google Scholar] [CrossRef]
- Malafarina, V.; Serra Rexach, J.A.; Masanes, F.; Cruz-Jentoft, A.J. Effects of high-protein, high-calorie oral nutritional supplementation in malnourished older people in nursing homes: An observational, multi-center, prospective study (PROT-e-GER). Protocol and baseline population characteristics. Maturitas 2019, 126, 73–79. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Roberts, H.C.; Lim, S.E.R.; Cox, N.J.; Ibrahim, K. The Challenge of Managing Undernutrition in Older People with Frailty. Nutrients 2019, 11, 808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkert, D.; Weber, J.; Kiesswetter, E.; Sulz, I.; Hiesmayr, M. Nutritional situation in hospitols and nursing homes—Evaluation of the German nutritionDay data. In 14. DGE-Nutrition Report; German Nutrition Society (DGE), Ed.; German Nutrition Society: Bonn, Germay, 2020; pp. 199–258. [Google Scholar]
- Johnson, S.; Nasser, R.; Banow, T.; Cockburn, T.; Voegeli, L.; Wilson, O.; Coleman, J. Use of oral nutrition supplements in long-term care facilities. Can. J. Diet. Pract. Res. 2009, 70, 194–198. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S. Diagnostic criteria for malnutrition–an ESPEN consensus statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, C.; de Souto Barreto, P.; Ghisolfi, A.; Guyonnet, S.; Dorigny, B.; Vellas, B.; Rolland, Y. Indicators of oral nutritional supplements prescription in nursing home residents: A cross-sectional study. Clin. Nutr. 2016, 35, 1047–1052. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.L.; Tamura, B.K.; Masaki, K.H.; Amella, E.J. Prevalence and measures of nutritional compromise among nursing home patients: Weight loss, low body mass index, malnutrition, and feeding dependency, a systematic review of the literature. J. Am. Med. Dir. Assoc. 2013, 14, 94–100. [Google Scholar] [CrossRef]
- Streicher, M.; Themessl-Huber, M.; Schindler, K.; Sieber, C.C.; Hiesmayr, M.; Volkert, D. nutritionDay in Nursing Homes-The Association of Nutritional Intake and Nutritional Interventions With 6-Month Mortality in Malnourished Residents. J. Am. Med. Dir. Assoc. 2017, 18, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firnhaber, G.C.; Roberson, D.W.; Kolasa, K.M. Nursing staff participation in end-of-life nutrition and hydration decision-making in a nursing home: A qualitative study. J. Adv. Nurs. 2020, 76, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- Loofs, T.S.; Haubrick, K. End-of-Life Nutrition Considerations: Attitudes, Beliefs, and Outcomes. Am. J. Hosp. Palliat. Med. 2020, 1049909120960124. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Visser, M.; Corish, C.; Geisler, C.; De Groot, L.; Cruz-Jentoft, A.; Lohrmann, C.; O’Connor, E.; Schindler, K.; de van der Schueren, M. Joint action malnutrition in the elderly (MaNuEL) knowledge hub: Summary of project findings. Eur. Geriatr. Med. 2020, 11, 169–177. [Google Scholar] [CrossRef]
- Pauly, L.; Stehle, P.; Volkert, D. Nutritional situation of elderly nursing home residents. Z. Gerontol. Geriatr. 2007, 40, 3–12. [Google Scholar] [CrossRef]
- Suominen, M.H.; Sandelin, E.; Soini, H.; Pitkala, K.H. How well do nurses recognize malnutrition in elderly patients? Eur. J. Clin. Nutr. 2009, 63, 292–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, J. Tackling undernutrition through appropriate supplement prescribing. Br. J. Community Nurs. 2003, 8, 343–352. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kiljunen, O.; Välimäki, T.; Kankkunen, P.; Partanen, P. Competence for older people nursing in care and nursing homes: An integrative review. Int. J. Older People Nurs. 2017, 12, e12146. [Google Scholar] [CrossRef]


| Subjective Judgement | Objective Criteria | ||||||
|---|---|---|---|---|---|---|---|
| Total | MN | At risk | No MN | MN | No MN | ||
| n = 246 | n = 27 | n = 63 | n = 156 | n = 81 | n = 165 | ||
| Gender, female, n (%) | 166 (67.5) | 22 (81.4) | 38 (60.3) | 106 (67.9) | 63 (77.8) | 103 (62.4) | |
| Age (years), mean ± SD (95% CI) | 83.6 ± 8.3 (82.6–84.7) | 87.5 ± 7.4 (84.5–90.4) | 84.6 ± 8.4 (82.5–86.8) | 82.5 ± 8.1 (81.2–83.8) | 85.3 ± 8.2 (83.4–87.1) | 82.8 ± 8.2 (81.5–84.1) | |
| BMI [kg/m2], <20 | 37 (15.0) | 25 (67.6) | 7 (18.9) | 5 (13.5) | 37 (100.0) | 0 (0.0) | |
| Weight loss, ≥5% within 3 months | 30 (12.2) | 7 (23.3) | 20 (66.7) | 3 (10.0) | 30 (100.0) | 0 (0.0) | |
| Poor intake, ≤1/4 of the meal | 38 (15.4) | 12 (31.6) | 12 (31.6)) | 14 (36.8) | 38 (100.0) | 0 (0.0) | |
| Dementia, | Severe | 110 (44.7) | 17 (63.0) | 32 (50.8) | 61 (39.1) | 41 (50.6) | 69 (41.8) |
| n (%) | Mild | 98 (39.8) | 6 (22.2) | 25 (39.7) | 67 (42.9) | 28 (34.6) | 70 (42.4) |
| No | 38 (15.5) | 4 (14.8) | 6 (9.5) | 28 ((18.0) | 12 (14.8) | 26 (15.8) | |
| Depression | Severe | 56 (22.8) | 7 (26.0) | 15 (23.8) | 34 (21.8) | 20 (24.7) | 36 (21.8) |
| n (%) | Mild | 91 (37.0) | 11 (40.7) | 18 (28.6) | 62 (39.7) | 27 (33.3) | 64 (38.8) |
| No | 99 (40.2) | 9 (33.3) | 30 (47.6) | 60 (38.5) | 34 (42.0) | 65 (39.4) | |
| Number of drugs, median (95% CI) | 7 (6.5–7.3) | 5 (4.3–6.7) | 7 (5.9–7.3) | 7 (6.8–7.8) | 7 (5.7–7.1) | 7 (6.7–7.6) | |
| Bedridden or | 109 (44.3) | 18 (66.7) | 30 (47.6) | 61 (39.1) | 39 (48.2) | 70 (42.4) | |
| chairbound | |||||||
| Mobility | Able to go around | 124 (50.4) | 8 (29.6) | 32 (50.8) | 84 (53.8) | 39 (48.2) | 85 (51.6) |
| n (%) | in the unit | ||||||
| Goes out of the unit | 13 (5.3) | 1 (3.7) | 1 (1.6) | 11 (7.1) | 3 (3.6) | 10 (6.0) | |
| Dysphagia n (%) | 54 (22.0) | 14 (51.9) | 20 (31.7) | 20 (12.8) | 26 (32.1) | 28 (17.0) | |
| Assistance at the meal (%) | 80 (32.5) | 19 (70.4) | 24 (38.1) | 37 (23.7) | 36 844.4) | 44 (26.7) | |
| BMI < 20 kg/m2 | Weight Loss ≥5% in Last 3 Months | Intake ≤1/4 of the Meal | |
|---|---|---|---|
| A living will (n = 6) | 5 | 0 | 1 |
| Terminal situation (n = 1) | 1 | 0 | 0 |
| Refusal by legal guardian (n = 1) | 1 | 0 | 0 |
| Awaiting further weight trends (n = 10) | 1 | 4 | 5 |
| Awaiting results of dietary records (n = 1) | 0 | 1 | 0 |
| Sufficient weight (n = 6) | 0 | 0 | 6 |
| Not judged as malnourished (n = 5) | 4 | 0 | 1 |
| Adequate BMI (n = 5) | 0 | 2 | 3 |
| No weight loss (n = 2) | 0 | 2 | 0 |
| Sufficient intake (n = 1) | 1 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grosshauser, F.J.; Kiesswetter, E.; Torbahn, G.; Sieber, C.C.; Volkert, D. Reasons for and against Nutritional Interventions. An Exploration in the Nursing Home Setting. Geriatrics 2021, 6, 90. https://doi.org/10.3390/geriatrics6030090
Grosshauser FJ, Kiesswetter E, Torbahn G, Sieber CC, Volkert D. Reasons for and against Nutritional Interventions. An Exploration in the Nursing Home Setting. Geriatrics. 2021; 6(3):90. https://doi.org/10.3390/geriatrics6030090
Chicago/Turabian StyleGrosshauser, Franz J., Eva Kiesswetter, Gabriel Torbahn, Cornel C. Sieber, and Dorothee Volkert. 2021. "Reasons for and against Nutritional Interventions. An Exploration in the Nursing Home Setting" Geriatrics 6, no. 3: 90. https://doi.org/10.3390/geriatrics6030090
APA StyleGrosshauser, F. J., Kiesswetter, E., Torbahn, G., Sieber, C. C., & Volkert, D. (2021). Reasons for and against Nutritional Interventions. An Exploration in the Nursing Home Setting. Geriatrics, 6(3), 90. https://doi.org/10.3390/geriatrics6030090