
Smartphone Applications Designed to Improve Older People’s Chronic Pain Management: An Integrated Systematic Review

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Background
3. Aims
4. Methods
4.1. Design
4.2. Search Strategy
4.3. Eligibility Criteria
(“Pain” [MeSH Terms]) AND (“aged”[All Fields] OR “aged”[MeSH Terms] OR “elderly”[All Fields] OR “old”[All Fields] OR “seniors”[All Fields] OR “senior”[All Fields]) AND (“telemedicine”[MeSH Terms] OR “telemedicine”[All Fields] OR “tele-medicine”[All Fields] OR “telehealth”[All Fields] OR “tele-health”[All Fields] OR “mhealth”[All Fields] OR “m-health”[All Fields] OR “ehealth”[All Fields] OR “e-health”[All Fields])
4.4. Quality Assessment
4.5. Data Abstraction and Synthesis
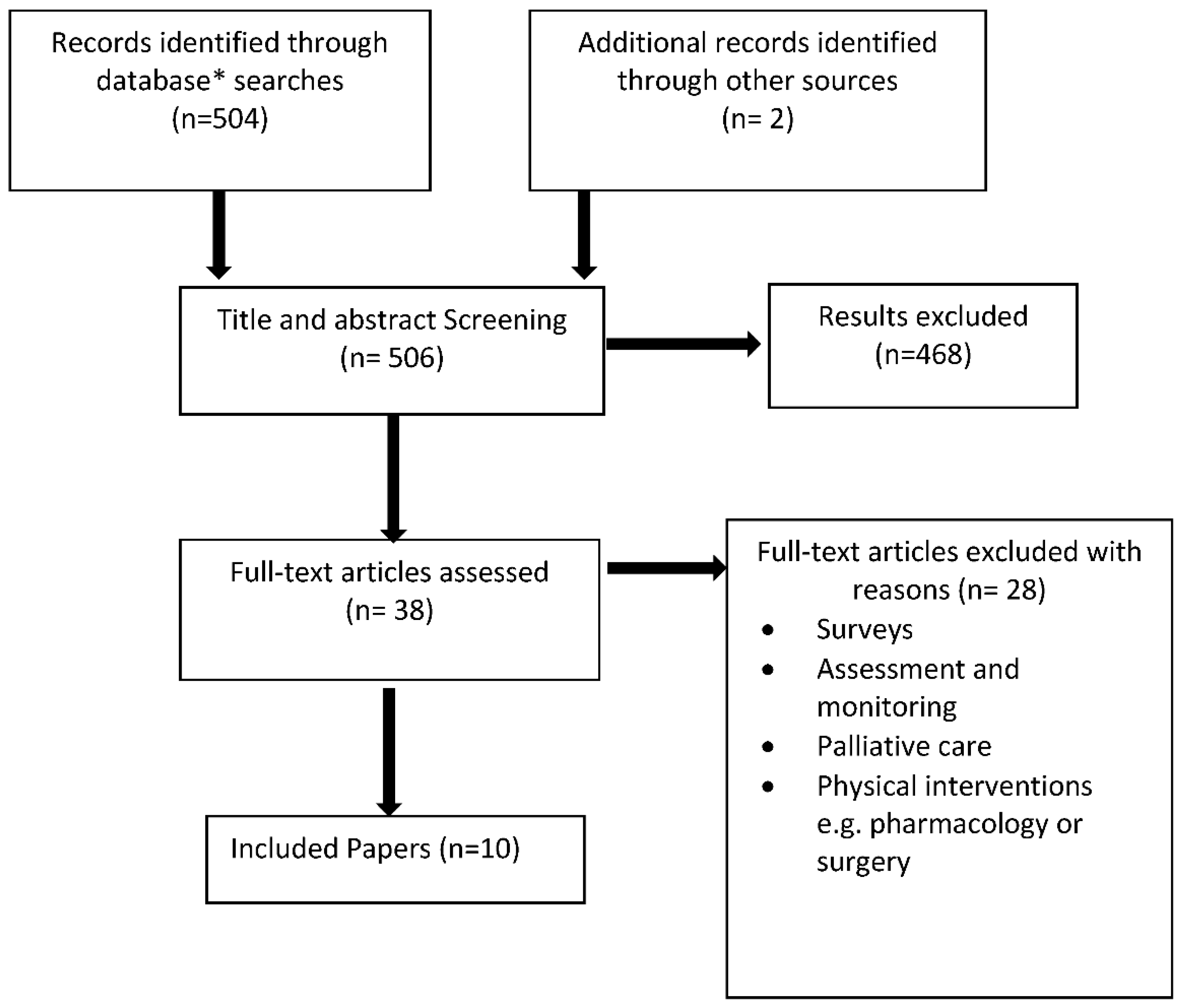
5. Results
5.1. Study Characteristics
5.2. The Potential Benefits and Serviceabilityfor Older Adults
5.3. Clinical and Service User Involvement in Development
5.4. Support or Perceived Barriers for Clinicians and Service Users in Their Effective Use
5.5. Use of Data
6. Discussion
6.1. Review Limitations
6.2. Implications for Practice
6.3. Recommendations for Research
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- European Commission. 2018 Ageing Report: Policy Challenges for Ageing Societies. Brussels: European Commission. 17 December 2019. Available online: https://ec.europa.eu/info/news/economyfinance/policy-implications-ageing-examined-new-report-2018-may-25_en (accessed on 6 April 2021).
- Schofield, P. Pain in Older Adults: Epidemiology, Impact and Barriers to Management. Rev. Pain 2007, 1, 12–14. [Google Scholar] [CrossRef]
- Breivik, H.; Eisenberg, E.; O’Brien, T. The individual and societal burden of chronic pain in Europe: The case for strategic pri-oritisation and action to improve knowledge and availability of appropriate care. BMC Public Health 2013, 13, 1229. Available online: http://www.biomedcentral.com/1471-2458/13/1229 (accessed on 6 April 2021). [CrossRef] [PubMed]
- Eccleston, C.; Blyth, F.M.; Dear, B.F.; Fisher, E.A.; Keefe, F.J.; Lynch, M.E.; Palermo, T.M.; Reid, M.C.; Williams, A.C.D.C. Managing patients with chronic pain during the COVID-19 outbreak: Considerations for the rapid introduction of remotely supported (eHealth) pain management services. Pain 2020, 161, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Blyth, F.M.; Schneider, C.H. Global burden of pain and global pain policy—Creating a purposeful body of evidence. Pain 2018, 159, S43–S48. [Google Scholar] [CrossRef] [PubMed]
- Fayaz, A.; Croft, P.; Langford, R.M.; Donaldson, L.J.; Jones, G.T. Prevalence of chronic pain in the UK: A systematic review and meta-analysis of population studies. BMJ Open 2016, 6, e010364. [Google Scholar] [CrossRef] [PubMed]
- Landmark, T.; Dale, O.; Romundstad, P.; Woodhouse, A.; Kaasa, S.; Borchgrevink, P.C. Development and course of chronic pain over 4 years in the general population: The HUNT pain study. Eur. J. Pain 2018, 22, 1606–1616. [Google Scholar] [CrossRef] [PubMed]
- Reid, K.J.; Harker, J.; Bala, M.M.; Truyers, C.; Kellen, E.; Bekkering, G.E.; Kleijnen, J. Epidemiology of chronic non-cancer pain in Europe: Narrative review of prevalence, pain treatments and pain impact. Curr. Med. Res. Opin. 2010, 27, 449–462. [Google Scholar] [CrossRef]
- Bonathan, C.; Hearn, L.; Williams, A.C.D.C. Socioeconomic status and the course and consequences of chronic pain. Pain Manag. 2013, 3, 159–162. [Google Scholar] [CrossRef]
- Larsson, C.; Hansson, E.E.; Sundquist, K.; Jakobsson, U. Chronic pain in older adults: Prevalence, incidence, and risk factors. Scand. J. Rheumatol. 2017, 46, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, Z.; Zajacova, A.; Grol-Prokopczyk, H. Trends in Pain Prevalence among Adults Aged 50 and Older across Europe, 2004 to 2015. J. Aging Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Dall, T.M.; Gallo, P.D.; Chakrabarti, R.; West, T.; Semilla, A.P.; Storm, M.V. An Aging Population And Growing Disease Burden Will Require A Large And Specialized Health Care Workforce By 2025. Health Aff. 2013, 32, 2013–2020. [Google Scholar] [CrossRef]
- Marjanovic, S.; Altenhofer, M.; Hocking, L.; Jones, M.M.; Parks, S.; Ghiga, I.; Cox, C.; Galai, K.; Ling, T. Innovating for Improved Healthcare: Policy and Practice for a Thriving NHS.; Rand Corporation: Santa Monica, CA, USA, 2020. [Google Scholar]
- WHO. Health and Sustainable Development, Telehealth. 2020. Available online: https://www.who.int/gho/goe/telehealth/en/ (accessed on 6 April 2021).
- Lindsay, S.; Jackson, D.; Schofield, G.; Olivier, P. Engaging Older People Using Participatory Design. ACM Press. 5 May 2012, p. 1199. Available online: http://dl.acm.org/citation.cfm?doid=2207676.2208570 (accessed on 6 April 2021).
- Joe, J.; Demiris, G. Older adults and mobile phones for health: A review. J. Biomed. Inform. 2013, 46, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Segar, J.; Rogers, A.; Salisbury, C.; Thomas, C. Roles and identities in transition: Boundaries of work and inter-professional relationships at the interface between telehealth and primary care. Health Soc. Care Community 2013, 21, 606–613. [Google Scholar] [CrossRef]
- Quinn, C.C.; Staub, S.; Barr, E.; Gruber-Baldini, A. Mobile Support for Older Adults and Their Caregivers: Dyad Usability Study. JMIR Aging 2019, 2, e12276. [Google Scholar] [CrossRef]
- Yerrakalva, D.; Yerrakalva, D.; Hajna, S.; Griffin, S. Effects of mobile health app interventions on sedentary time, physical activity, and fitness in older adults: Systematic review and meta-analysis. J. Med. Internet Res. 2019, 21, e14343. [Google Scholar] [CrossRef]
- Ahmad, N.A.; Ludin, A.F.M.; Shahar, S.; Noah, S.A.M.; Tohit, N.M. Willingness, perceived barriers and motivators in adopting mobile applications for health-related interventions among older adults: A scoping review protocol. BMJ Open 2020, 10, e033870. [Google Scholar] [CrossRef]
- Aslam, A.S.; van Luenen, S.; Aslam, S.; van Bodegom, D.; Chavannes, N.H. A Systematic Review on the use of mHealth to increase physical activity in older people. Clin. eHealth 2020, 3, 31–39. [Google Scholar] [CrossRef]
- Curtis, K.; Price, K. Factors that influence older people’s engagement with digital health technology. Nurs. Older People 2017, 29, 27–30. [Google Scholar] [CrossRef]
- Van Gemert-Pijnen, J.E.; Nijland, N.; Van Limburg, M.; Ossebaard, H.C.; Kelders, S.M.; Eysenbach, G.; Seydel, E.R. A Holistic Framework to Improve the Uptake and Impact of eHealth Technologies. J. Med. Internet Res. 2011, 13, e111. [Google Scholar] [CrossRef]
- Salisbury, C.; Thomas, C.; O’Cathain, A.; Rogers, A.; Pope, C.; Yardley, L.; Hollinghurst, S.; Fahey, T.; Lewis, G.; Large, S.; et al. Telehealth in Chronic disease: Mixed-methods study to develop the TECH conceptual model for inter-vention design and evaluation. BMJ Open 2015, 1, 5. [Google Scholar] [CrossRef] [PubMed]
- McDonough, C.C. University of Massachusetts Lowell The Effect of Ageism on the Digital Divide Among Older Adults. Gerontol. Geriatr. Med. 2016, 2, 1–7. [Google Scholar] [CrossRef]
- Barber, S.J. An examination of age-based stereotype threat about cognitive decline: Implications for stereotype-threat research and theory development. Perspect. Psychol. Sci. 2017, 12, 62–90. [Google Scholar] [CrossRef]
- Choi, E.Y.; Kim, Y.; Chipalo, E.; Lee, H.Y. Does Perceived Ageism Widen the Digital Divide? And Does It Vary by Gender? Gerontologist 2020, 60. [Google Scholar] [CrossRef] [PubMed]
- STATISA. Smartphone Ownership Penetration in the United Kingdom (UK) in 2012–2020, by Age. Statista. Available online: https://www.statista.com/statistics/271851/smartphone-owners-in-the-united-kingdom-uk-by-age/ (accessed on 6 April 2021).
- Mosa, A.S.M.; Yoo, I.; Sheets, L. A Systematic Review of Healthcare Applications for Smartphones. BMC Med. Inform. Decis. Mak. 2012, 12, 67. [Google Scholar] [CrossRef] [PubMed]
- Beratarrechea, A.; Lee, A.G.; Willner, J.M.; Jahangir, E.; Ciapponi, A.; Rubinstein, A. The Impact of Mobile Health Interventions on Chronic Disease Outcomes in Developing Countries: A Systematic Review. Telemed. e-Health 2014, 20, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Y.; Wei, C.; Yao, N.; Yuan, A.; Shan, Y.; Yuan, C. Smartphone Interventions for Long-Term Health Management of Chronic Diseases: An Integrative Review. Telemed. e-Health 2014, 20, 570–583. [Google Scholar] [CrossRef]
- Lee, J.-A.; Choi, M.; Lee, S.A.; Jiang, N. Effective behavioral intervention strategies using mobile health applications for chronic disease management: A systematic review. BMC Med. Inform. Decis. Mak. 2018, 18, 12. [Google Scholar] [CrossRef]
- Triantafyllidis, A.; Kondylakis, H.; Votis, K.; Tzovaras, D.; Maglaveras, N.; Rahimi, K. Features, outcomes, and challenges in mobile health interventions for patients living with chronic diseases: A review of systematic reviews. Int. J. Med. Inform. 2019, 132, 103984. [Google Scholar] [CrossRef]
- Wallace, L.S.; Dhingra, L.K. A systematic review of smartphone applications for chronic pain available for download in the United States. J. Opioid Manag. 2014, 10, 63–68. [Google Scholar] [CrossRef]
- Bhattarai, P.; Newton-John, T.R.O.; Phillips, J.L. Quality and Usability of Arthritic Pain Self-Management Apps for Older Adults: A Systematic Review. Pain Med. 2017, 19, 471–484. [Google Scholar] [CrossRef]
- Alexander, J.C.; Joshi, G.P. Smartphone applications for chronic pain management: A critical appraisal. J. Pain Res. 2016, 9, 731–734. [Google Scholar] [CrossRef] [PubMed]
- Bhattarai, P.; Phillips, J.L. The role of digital health technologies in management of pain in older people: An integrative review. Arch. Gerontol. Geriatr. 2017, 68, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Rosser, B.A.; Eccleston, C. Smartphone applications for pain management. J. Telemed. Telecare 2011, 17, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Salemohamed, N.; Stinson, J.; Carlin, L.; Seto, E.; Webster, F.; Furlan, A.D. Health care providers’ experiences and perceptions participating in a chronic pain telementoring education program: A qualitative study. Can. J. Pain 2020, 4, 111–121. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A.; Oakley, A.; Oliver, S.; Sutcliffe, K.; Rees, R.; Brunton, G.; Kavanagh, J. Integrating qualitative research with trials in systematic reviews. BMJ 2004, 328, 1010–1012. [Google Scholar] [CrossRef]
- Brown, P.; Brunnhuber, K.; Chalkidou, K.; Chalmers, I.; Clarke, M.; Fenton, M.; Forbes, C.; Glanville, J.; Hicks, N.J.; Moody, J.; et al. How to formulate research recommendations. BMJ 2006, 333, 804–806. [Google Scholar] [CrossRef] [PubMed]
- Hawker, S.; Payne, S.; Kerr, C.; Hardey, M.; Powell, J. Appraising the Evidence: Reviewing Disparate Data Systematically. Qual. Health Res. 2002, 12, 1284–1299. [Google Scholar] [CrossRef]
- Bedson, J.; Hill, J.; White, D.; Chen, Y.; Wathall, S.; Dent, S.; Cooke, K.; Van Der Windt, D. Development and validation of a pain monitoring app for patients with musculoskeletal conditions (The Keele pain recorder feasibility study). BMC Med. Inform. Decis. Mak. 2019, 19, 1–13. [Google Scholar] [CrossRef]
- Bhattarai, P.; Newton-John, T.; Phillips, J.L. Apps for Older People’s Pain Self-Management: Perspectives of Primary Care and Allied Health Clinicians. Pain Med. 2019, 21, 686–694. [Google Scholar] [CrossRef]
- Bhattarai, P.; Newton-John, T.R.; Phillips, J.L. Apps for pain self-management of older people’s arthritic pain, one size doesn’t fit all: A qualitative study. Arch. Gerontol. Geriatr. 2020, 89, 104062. [Google Scholar] [CrossRef]
- Currie, M.; Philip, L.J.; Roberts, A. Attitudes towards the use and acceptance of eHealth technologies: A case study of older adults living with chronic pain and implications for rural healthcare. BMC Health Serv. Res. 2015, 15, 1–12. [Google Scholar] [CrossRef]
- Docking, R.E.; Lane, M.; Schofield, P.A. Usability Testing of the iPhone App to Improve Pain Assessment for Older Adults with Cognitive Impairment (Prehospital Setting): A Qualitative Study. Pain Med. 2017, 19, 1121–1131. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.; Richardson, J.E.; Granieri, E.; Reid, M.C. Novel Telemedicine Technologies in Geriatric Chronic Non-Cancer Pain: Primary Care Providers’ Perspectives. Pain Med. 2014, 15, 206–213. [Google Scholar] [CrossRef]
- McDonald, D.D.; Walsh, S.; Vergara, C.; Gifford, T. Effect of a Virtual Pain Coach on Pain Management Discussions: A Pilot Study. Pain Manag. Nurs. 2013, 14, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.J.; Jessel, S.; Richardson, J.E.; Reid, M.C. Older adults are mobile too!Identifying the barriers and facilitators to older adults’ use of mHealth for pain management. BMC Geriatr. 2013, 13, 1–43. [Google Scholar] [CrossRef]
- Pimm, T.J.; Williams, L.J.; Reay, M.; Pickering, S.; Lota, R.; Coote, L.; Maloney, C.; Hancock, D.; Sarhan, F. An evaluation of a digital pain management programme: Clinical effectiveness and cost savings. Br. J. Pain 2020, 14, 238–249. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.E.; Lee, J.I.; Nirenberg, A.; Reid, M.C. The potential role for smartphones among older adults with chronic non cancer pain: A qualitative study. Pain Med. 2018, 19, 1132–1139. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Morley, S.; Williams, A.; Hussain, S. Estimating the clinical effectiveness of cognitive behavioural therapy in the clinic: Evaluation of a CBT informed pain management programme. Pain 2008, 137, 670–680. [Google Scholar] [CrossRef]
- Abbey, J.; Piller, N.; De Bellis, A.; Esterman, A.; Parker, D.; Giles, L.; Lowcay, B. The Abbey pain scale: A 1-minute numerical indicator for people with end-stage dementia. Int. J. Palliat. Nurs. 2004, 10, 6–13. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence Evidence Standards Framework for Digital Health Technologies. NICE. 2019. Available online: https://www.nice.org.uk/Media/Default/About/what-we-do/our-programmes/evidence-standards-framework/digital-evidence-standards-framework.pdf (accessed on 6 April 2021).
- Andersson, G. Internet-Delivered Psychological Treatments. Annu. Rev. Clin. Psychol. 2016, 12, 157–179. [Google Scholar] [CrossRef]
- Zlomke, K.R. Psychometric properties of internet administered versions of Penn State Worry Questionnaire (PSWQ) and Depression, Anxiety, and Stress Scale (DASS). Comput. Hum. Behav. 2009, 25, 841–843. [Google Scholar] [CrossRef]
- Harris, G. World Health Organization launches new app to improve care for ageing population. Br. J. Health Manag. 2020, 26, 48–49. [Google Scholar] [CrossRef]
- Hanlon, P.; Daines, L.; Campbell, C.; McKinstry, B.; Weller, D.; Pinnock, H. Telehealth Interventions to Support Self-Management of Long-Term Conditions: A Systematic Metareview of Diabetes, Heart Failure, Asthma, Chronic Obstructive Pulmonary Disease, and Cancer. J. Med. Internet Res. 2017, 19, e172. [Google Scholar] [CrossRef] [PubMed]
- Kristjánsdóttir, Ó.B.; Fors, E.A.; Eide, E.; Finset, A.; Stensrud, T.L.; Van Dulmen, S.; Wigers, S.H.; Eide, H.; Kelly, J.; Mooney, J.; et al. A Smartphone-Based Intervention With Diaries and Therapist-Feedback to Reduce Catastrophizing and Increase Functioning in Women With Chronic Widespread Pain: Randomized Controlled Trial. J. Med. Internet Res. 2013, 15, e5. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, R.L.; Schmid, C.H.; Marois, M.; Wilsey, B.; Ward, D.; Hays, R.D.; Duan, N.; Wang, Y.; Macdonald, S.; Jerant, A.; et al. Effect of Mobile Device–Supported Single-Patient Multi-crossover Trials on Treatment of Chronic Musculoskeletal Pain. JAMA Intern. Med. 2018, 178, 1368–1377. [Google Scholar] [CrossRef]
- Lin, J.; Faust, B.; Ebert, D.D.; Krämer, L.; Baumeister, H. A Web-Based Acceptance-Facilitating Intervention for Identifying Patients’ Acceptance, Uptake, and Adherence of Internet- and Mobile-Based Pain Interventions: Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e244. [Google Scholar] [CrossRef]
- Philip, L.; Roberts, A.; Currie, M.; Mort, A. Technology for Older Adults: Maximising Personal and Social Interaction: Exploring Opportunities for eHealth to Support the Older Rural Population with Chronic Pain. Scott. Geogr. J. 2015, 131, 181–193. [Google Scholar] [CrossRef]
- Suso-Ribera, C.; Mesas, Á.; Medel, J.; Server, A.; Márquez, E.; Castilla, D.; Zaragozá, I.; García-Palacios, A. Improving pain treatment with a smartphone app: Study protocol for a randomized controlled trial. Trials 2018, 19, 1–7. [Google Scholar] [CrossRef]
- Schofield, P.A.; Boarer, A.C.; Martin, D. Chatbot technology for the management of chronic pain in older adults. Geriatritcs 2020. accepted for publication. [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2019: Highlights. 2019. Available online: https://www.un.org/development/desa/publications/world-population-prospects-2019-highlights.html (accessed on 11 January 2020).
- Díaz-Bossini, J.M.; Moreno, L. Accessibility to mobile interfaces for older people. Procedia Comput. Sci. 2014, 27, 57–66. [Google Scholar] [CrossRef]
- Lynch, K.R.; Schwerha, D.J.; Johanson, G.A. Development of a weighted heuristic for website evaluation for older adults. Int. J. Hum. Comput. Interact. 2013, 6, 404–418. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Studies focused on older adults (≥60 years) or Health Professionals or Carers AND Chronic pain | Younger adults and those without chronic pain, mobility monitoring, surgical intervention, cancer treatment, palliative care or end-of-life support. |
| Intervention | Telehealth, virtual interventions via phone | Video consultation, instant messaging. Telehealth interventions directed at and solely experienced by health professionals. |
| Comparator | Any | - |
| Outcomes | Studies will not be selected on the basis of reported outcomes | - |
| Study Design | Published primary research studies, including both qualitative and quantitative research. | Non-telehealth related delivery of service research methodologies. Abstracts of unpublished studies. Opinion papers. Professional communications or letters. Literature reviews. Systematic reviews. Meta-analyses. Surveys. Not published in English. |
| Author, Country | Year | Study Type | Research Question | Main Findings | Identified App |
|---|---|---|---|---|---|
| Bedson, UK [43] | 2019 | Mixed n = 21 | To assess face, content and construct validity of data collection using the Pain Recorder in primary care patients receiving new analgesic prescriptions for musculoskeletal pain, as well as to assess its acceptability and clinical utility. | Early testing of an app in a small sample of people consulting with musculoskeletal pain in general practice showed promising results in terms of face and content validity, acceptability and clinical usefulness. | The Keele Pain Recorder- “developed by patients for patients, to improve the management of pain” https://www.keele.ac.uk/kpr/ accessed on 11 March 2021 |
| Bhattarai, Australia [44] | 2020 | Qualitative, feasibility study n = 17 | To explore the attitudes and perspectives of primary care and allied health clinicians regarding the integration of pain apps into their older arthritic patients’ pain self- management strategies. | Apps potential to support various aspects of patients’ self-management behaviours. | The DigiTech Pain Project, using the RAISE app |
| Bhattarai, Australia [45] | 2020 | Qualitative, feasibility study n = 18 | To explore the attitudes and experiences of older people with chronic arthritic pain towards using an app for their pain management. | Pain self-management apps have the potential to assist older people in their pain self-management process. | The DigiTech Pain Project, using the RAISE app |
| Currie, UK [46] | 2015 | Mixed Method n = 168 s | A mixed-methods study of older adults with chronic pain to examine attitudes towards, current use of and acceptance of the use of technology in healthcare. | E-health (including apps) has potential to supplement existing care. | - |
| Docking, UK [47] | 2018 | Qualitative (pilot) 24 paramedic students | Usability testing of a newly developed iPhone pain assessment application with potential users. | The pain assessment app constitutes a potentially useful tool (for paramedics) in the prehospital setting for those aged ≥60. | iPhone pain app developed in collaboration with the Computing and Mathematical Sciences (CMS) department at the University of Greenwich. |
| Levine, USA [48] | 2014 | Qualitative-(feasibility) focus groups in primary care n = 25 | To determine how novel telemedicine technologies, particularly smartphones, might be best used in the management of older adults with Chronic Non-Cancer Pain (CNCP). | No participants reported use of telemedicine in geriatric CNCP management. The results suggest that technologies including apps would find a welcome reception among primary care providers delivering care to older adults with CNCP. | - |
| McDonald (USA) [49] | 2013 | Pilot for RCT n = 23 | The more skillful that older adults are in using communication strategies, the more likely they will be to convey important osteoarthritis pain information to practitioners and to be prescribed more effective pain management treatments. | No significant difference in overall pain communication with the practitioner occurred between the pain communication plus virtual pain coach group and the pain communication-only group. | A “virtual pain coach” |
| Parker (USA)[50] | 2013 | Qualitative (feasibility) n = 41 (older adults) | To examine the willingness of older adults with chronic pain to adopt mHealth technologies. | Older adults with chronic pain are willing and interested in using mHealth including apps. | - |
| Pimm (UK) [51] | 2019 | Quasi Experimental n = 438 | To establish the clinical effectiveness of a web-based pain management programme (PMP), specifically whether it would lead to improved clinical outcomes and reduced healthcare costs in a real-world clinical setting. | A web-based pain management programme can be clinically effective and may be a useful addition to the treatments offered by pain management services. The older participants (50–90 years) were more likely to engage with and complete the programme. | “Pathway through Pain” app https://www.pathwaythroughpain.com/ accessed on 11 March 2021 |
| Richardson (USA) [52] | 2018 | n = 13 Qualitative | To determine the role that smartphones (apps) may play in supporting older adults with chronic noncancer pain (CNCP) in order to improve pain management in this expanding population. | Smartphone apps should support older adult needs to effectively communicate pain experiences with personal contacts and caregivers, as well as healthcare providers. | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dunham, M.; Bonacaro, A.; Schofield, P.; Bacon, L.; Spyridonis, F.; Mehrpouya, H. Smartphone Applications Designed to Improve Older People’s Chronic Pain Management: An Integrated Systematic Review. Geriatrics 2021, 6, 40. https://doi.org/10.3390/geriatrics6020040
Dunham M, Bonacaro A, Schofield P, Bacon L, Spyridonis F, Mehrpouya H. Smartphone Applications Designed to Improve Older People’s Chronic Pain Management: An Integrated Systematic Review. Geriatrics. 2021; 6(2):40. https://doi.org/10.3390/geriatrics6020040
Chicago/Turabian StyleDunham, Margaret, Antonio Bonacaro, Patricia Schofield, Liz Bacon, Fotios Spyridonis, and Hadi Mehrpouya. 2021. "Smartphone Applications Designed to Improve Older People’s Chronic Pain Management: An Integrated Systematic Review" Geriatrics 6, no. 2: 40. https://doi.org/10.3390/geriatrics6020040
APA StyleDunham, M., Bonacaro, A., Schofield, P., Bacon, L., Spyridonis, F., & Mehrpouya, H. (2021). Smartphone Applications Designed to Improve Older People’s Chronic Pain Management: An Integrated Systematic Review. Geriatrics, 6(2), 40. https://doi.org/10.3390/geriatrics6020040