Investigating On-Road Lane Maintenance and Speed Regulation in Post-Stroke Driving: A Pilot Case–Control Study

 ,
, _Sun.png) ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Data Collection
2.2.1. Procedure
2.2.2. Data Collection
2.3. Driving Performance Measures
2.3.1. Lane Keeping
2.3.2. Speed Control
2.4. Statistical Analysis
3. Results
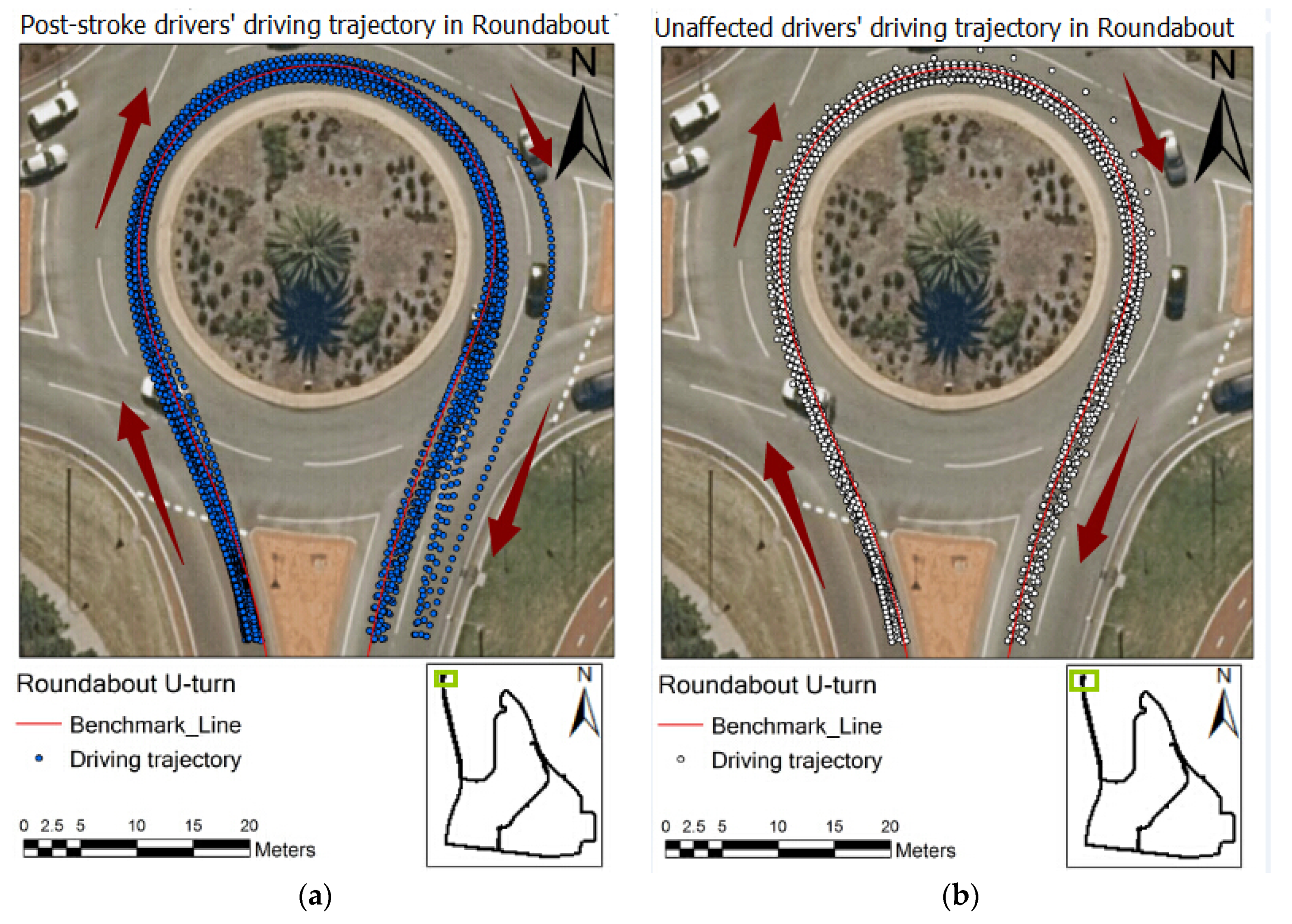
3.1. Spatial Analyses of Driving Trajectories across the Groups
3.2. Statistical Analyses of Driving Trajectories
3.2.1. Roundabout (U-Turn)
3.2.2. Left Turn
3.2.3. Straight Line One (Speed Limit of 50 km/h)
3.2.4. Straight Line Two (Speed Limit of 70 km/h)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Shapiro–Wilk Test | Levene’s Test | ||
|---|---|---|---|---|---|
| Lane deviation (Entire U-turn) | Post-stroke | Normal | 0.001 | 0.002 | 0.309 |
| SDLD (Entire U-turn) | Post-stroke | Normal | 0.001 | 0.015 | 0.058 |
| Lane deviation (Entry of U-turn) | Post-stroke | Normal | 0.405 | 0.065 | 0.365 |
| SDLD (Entry of U-turn) | Post-stroke | Normal | 0.041 | 0.198 | 0.896 |
| Lane deviation (Middle part of U-turn) | Post-stroke | Normal | 0.002 | 0.005 | 0.664 |
| SDLD (Middle part of U-turn) | Post-stroke | Normal | 0.000 | 0.141 | 0.396 |
| Lane deviation (Exit of U-turn) | Post-stroke | Normal | 0.001 | 0.209 | 0.130 |
| SDLD (Exit of U-turn) | Post-stroke | Normal | 0.002 | 0.266 | 0.036 |
| Driving speed (Exit of U-turn) | Post-stroke | Normal | 0.099 | 0.000 | 0.766 |
| Std. deviation of speed (Exit of U-turn) | Post-stroke | Normal | 0.700 | 0.495 | 0.214 |
| Lane deviation (Left turn) | Post-stroke | Normal | 0.004 | 0.971 | 0.329 |
| SDLD (Left turn) | Post-stroke | Normal | 0.000 | 0.542 | 0.077 |
| Lane deviation (Straight line) | Post-stroke | Normal | 0.827 | 0.154 | 0.639 |
| SDLD (Straight line) | Post-stroke | Normal | 0.676 | 0.140 | 0.522 |
| Driving speed | Post-stroke | Normal | 0.327 | 0.039 | 0.854 |
| Std. deviation of speed | Post-stroke | Normal | 0.002 | 0.154 | 0.411 |
| Lane deviation (Straight line) | Post-stroke | Normal | 0.412 | 0.222 | 0.022 |
| SDLD (Straight line) | Post-stroke | Normal | 0.004 | 0.044 | 0.879 |
| Driving speed | Post-stroke | Normal | 0.653 | 0.000 | 0.881 |
| Std. deviation of speed | Post-stroke | Normal | 0.032 | 0.002 | 0.977 |
References
- Burns, P.C. Navigation and the Mobility of Older Drivers. J. Gerontol. Ser. B 1999, 54, S49–S55. [Google Scholar] [CrossRef]
- Anstey, K.J.; Wood, J.M.; Lord, S.; Walker, J.G. Cognitive, sensory and physical factors enabling driving safety in older adults. Clin. Psychol. Rev. 2005, 25, 45–65. [Google Scholar] [CrossRef]
- Mathias, J.L.; Lucas, L.K. Cognitive predictors of unsafe driving in older drivers: A meta-analysis. Int. Psychogeriatr. 2009, 21, 637–653. [Google Scholar] [CrossRef]
- Sun, Q.; Xia, J.; Li, Y.; Foster, J.; Falkmer, T.; Lee, H. Unpacking older drivers’ maneuver at intersections: Their visual-motor coordination and underlying neuropsychological mechanisms. Transp. Res. Part F Traffic Psychol. Behav. 2018, 58, 11–18. [Google Scholar] [CrossRef]
- Sun, Q.; Xia, J.; Foster, J.; Falkmer, T.; Lee, H. Unpacking older drivers’ mobility at roundabouts: Their visual-motor coordination through driver–vehicle–environment interactions. Int. J. Sustain. Transp. 2019, 13, 627–638. [Google Scholar]
- Sun, Q.; Xia, J.; Foster, J.; Falkmer, T.; Lee, H. A psycho-Geoinformatics approach for investigating older adults’ driving behaviours and underlying cognitive mechanisms. Eur. Transp. Res. Rev. 2018, 10, 36. [Google Scholar] [CrossRef]
- Motta, K.; Lee, H.; Falkmer, T. Post-stroke driving: Examining the effect of executive dysfunction. J. Saf. Res. 2014, 49, 33.e1. [Google Scholar] [CrossRef] [PubMed]
- Poole, D.; Chaudry, F.; Jay, W.M. Stroke and driving. Top. Stroke Rehabil. 2008, 15, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Harbluk, J.L.; Noy, Y.I.; Eizenman, M. The Impact of Cognitive Distraction on Driver Visual Behaviour and Vehicle Control; Transport Canada: Ottawa, ON, Canada, 2002. [Google Scholar]
- Tan, K.; O’Driscoll, A.; O’Neill, D. Factors affecting return to driving post-stroke. Ir. J. Med. Sci. 2011, 180, 41–45. [Google Scholar] [CrossRef] [PubMed]
- National Stroke Foundation. Supports Limiting Life after Stroke New Report. 2014. Available online: https://strokefoundation.com.au/news/2015/05/18/supports-limiting-life-after-stroke-new-report (accessed on 1 July 2015).
- Terblanche, W.; Wilson, T. An Evaluation of Nearly-Extinct Cohort Methods for Estimating the Very Elderly Populations of Australia and New Zealand. PLoS ONE 2015, 10, e0123692. [Google Scholar] [CrossRef] [PubMed]
- McGwin, G.; Sims, R.V.; Pulley, L.; Roseman, J.M. Relations among Chronic Medical Conditions, Medications, and Automobile Crashes in the Elderly: A Population-based Case-Control Study. Am. J. Epidemiol. 2000, 152, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Rabadi, M.H.; Akinwuntan, A.; Gorelick, P. The Safety of Driving a Commercial Motor Vehicle after a Stroke. Stroke 2010, 41, 2991–2996. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rakotonirainy, A.; Steinhardt, D.; Delhomme, P.; Darvell, M.; Schramm, A. Older drivers’ crashes in Queensland, Australia. Accid. Anal. Prev. 2012, 48, 423–429. [Google Scholar] [CrossRef] [PubMed]
- He, J.; McCarley, J.S.; Kramer, A.F. Lane keeping under cognitive load: Performance changes and mechanisms. Hum. Factors J. Hum. Factors Ergon. Soc. 2014, 56, 414–426. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; Liu, Y. Concurrent processing of vehicle lane keeping and speech comprehension tasks. Accid. Anal. Prev. 2013, 59, 46–54. [Google Scholar] [CrossRef]
- Carsten, O.; Kircher, K.; Jamson, S. Vehicle-based studies of driving in the real world: The hard truth? Accid. Anal. Prev. 2013, 58, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Selander, H.; Lee, H.C.; Johansson, K.; Falkmer, T. Older drivers: On-road and off-road test results. Accid. Anal. Prev. 2011, 43, 1348–1354. [Google Scholar] [CrossRef]
- Blane, A.; Lee, H.; Falkmer, T.; Willstrand, T.D. Cognitive ability as a predictor of task demand and self-rated driving perfor-mance in post-stroke drivers—Implications for self-regulation. J. Transp. Health 2018, 9, 169–179. [Google Scholar] [CrossRef]
- Sun, Q.; Xia, J.; Foster, J.; Falkmer, T.; Lee, H. Pursuing Precise Vehicle Movement Trajectory in Urban Residential Area Using Multi-GNSS RTK Tracking. Transp. Res. Procedia 2017, 25, 2356–2372. [Google Scholar] [CrossRef]
- Sun, Q.; Odolinski, R.; Xia, J.; Foster, J.; Falkmer, T.; Lee, H. Validating the efficacy of GPS tracking vehicle movement for driving behaviour assessment. Travel Behav. Soc. 2017, 6, 32–43. [Google Scholar] [CrossRef]
- El-Rabbany, A. Introduction to GPS—The Satellite Navigation System, 2nd ed.; Artech House: Norwood, MA, USA, 2006. [Google Scholar]
- Perrier, M.-J.; Korner-Bitensky, N.; Petzold, A.; Mayo, N. The Risk of Motor Vehicle Crashes and Traffic Citations Post Stroke: A Structured Review. Top. Stroke Rehabil. 2010, 17, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Xia, J.; Nadarajah, N.; Falkmer, T.; Foster, J.; Lee, H. Assessing drivers’ visual-motor coordination using eye tracking, GNSS and GIS: A spatial turn in driving psychology. J. Spat. Sci. 2016, 61, 299–316. [Google Scholar] [CrossRef]
- Sun, Q.; Xia, J.; Foster, J.; Falkmer, T.; Lee, H. Driving manoeuvre during lane maintenance in older adults: Associations with neuropsychological scores. Transp. Res. Part F Traffic Psychol. Behav. 2018, 53, 117–129. [Google Scholar] [CrossRef]
- Peng, Y.; BoyleS, L.N.; Hallmark, L. Driver’s lane keeping ability with eyes off road: Insights from a naturalistic study. Accid. Anal. Prev. 2013, 50, 628–634. [Google Scholar] [CrossRef]
- White, R.W. Motivation reconsidered: The concept of competence. Psychol. Rev. 1959, 66, 297–333. [Google Scholar] [CrossRef]
- Chan, E.; Pradhan, A.K.; Pollatsek, A.; Knodler, M.A.; Fisher, D.L. Are driving simulators effective tools for evaluating novice drivers’ hazard anticipation, speed management, and attention maintenance skills? Transp. Res. Part F Traffic Psychol. Behav. 2010, 13, 343–353. [Google Scholar] [CrossRef]
- Weihong, G.; Blythe, P.T.; Edwards, S.; Pavkova, K.; Brennan, D. Effect of intelligent speed adaptation technology on older drivers’ driving performance. Intell. Transp. Syst. IET 2015, 9, 343–350. [Google Scholar]
- Selander, H.; Falkmer, T.; Bolin, I. Does automatic transmission improve driving behavior in older drivers? Gerontology 2012, 58, 181–187. [Google Scholar] [CrossRef]
- Reed, M.P.; Green, P.A. Comparison of driving performance on-road and in a low-cost simulator using a concurrent telephone dialling task. Ergonomics 1999, 42, 1015–1037. [Google Scholar] [CrossRef]
- Arenaza-Urquijo, E.M.; Landeau, B.; La Joie, R.; Mevel, K.; Mézenge, F.; Perrotin, A.; Chételat, G. Low-Cost Measures for Reducing Speeds at Curves on Two-Lane Rural Highways. Transp. Res. Rec. 2015, 2472, 142–154. [Google Scholar]
- Van Rossum, G.; Drake, F.L., Jr. Python Tutorial; Centrum voor Wiskunde en Informatica: Amsterdam, The Netherlands, 1995. [Google Scholar]
- IBM Corporation. IBM SPSS Statistics for Windows, Version 21.0; IBM Corp.: Armonk, NY, USA, 2012. [Google Scholar]
- McNamara, A.; Walker, R.; Ratcliffe, J.; George, S. Perceived confidence relates to driving habits post-stroke. Disabil. Rehabil. 2014, 37, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rand, D.; Katz, N.; Weiss, P.L. Intervention using the VMall for improving motor and functional ability of the upper extremity in post stroke participants. Eur. J. Phys. Rehabil. Med. 2009, 45, 119–121. [Google Scholar]
- Sawula, E.; Polgar, J.; Porter, M.M.; Gagnon, S.; Weaver, B.; Nakagawa, S.; Stinchcombe, A.; Bédard, M. The combined effects of on-road and simulator training with feedback on older drivers’ on-road performance: Evidence from a randomized controlled trial. Traffic Inj. Prev. 2018, 19, 241–249. [Google Scholar] [CrossRef] [PubMed]




| Statistical Test | Software | Data | Sample Size | Purpose | |
|---|---|---|---|---|---|
| Normality test | Kolmogorov–Smirnov test | SPSS 21.0 | Post-stroke and normal older driver groups | 14 participants in each group | To check the normality of the sample data |
| Parametric test | Two-tailed T-test | Python statistical analysis package | To exam the potential differences in lane keeping and speed control performance between the groups | ||
| One-way ANOVA test | SPSS 21.0 | ||||
| Non-Parametric test | Wilcoxon rank-sum test | Python statistical analysis package | |||
| Variable 1 | Group | Mean (std) | Median | IQR 2 | One-Way ANOVA Test | Two-Tailed T-Test | Wilcoxon Rank-Sum Test |
|---|---|---|---|---|---|---|---|
| Lane deviation (Entire U-turn) | Post-stroke | 0.78 (0.48) | 0.67 | 0.42 | 0.144 | 0.148 | 0.129 |
| Normal | 0.55 (0.26) | 0.49 | 0.14 | ||||
| SDLD (Entire U-turn) | Post-stroke | 0.60 (0.48) | 0.45 | 0.42 | 0.055 | 0.064 | 0.081 |
| Normal | 0.32 (0.11) | 0.36 | 0.09 | ||||
| Lane deviation (Entry of U-turn) | Post-stroke | 0.57 (0.27) | 0.49 | 0.47 | 0.766 | 0.766 | 0.783 |
| Normal | 0.61 (0.35) | 0.76 | 0.67 | ||||
| SDLD (Entry of U-turn) | Post-stroke | 0.23 (0.12) | 0.21 | 0.14 | 0.872 | 0.872 | 0.927 |
| Normal | 0.22 (0.10) | 0.23 | 0.19 | ||||
| Lane deviation (Middle part of U-turn) | Post-stroke | 0.55 (0.36) | 0.45 | 0.28 | 0.544 | 0.544 | 0.183 |
| Normal | 0.46 (0.40) | 0.30 | 0.50 | ||||
| SDLD (Middle part of U-turn) | Post-stroke | 0.29 (0.29) | 0.19 | 0.14 | 0.194 | 0.201 | 0.168 |
| Normal | 0.18 (0.10) | 0.16 | 0.11 | ||||
| Lane deviation (Exit of U-turn) | Post-stroke | 1.38 (1.24) | 1.05 | 0.75 | 0.043 * | 0.049 * | 0.035 * |
| Normal | 0.62 (0.37) | 0.63 | 0.68 | ||||
| SDLD (Exit of U-turn) | Post-stroke | 0.48 (0.43) | 0.31 | 0.35 | 0.026 * | 0.032 * | 0.027 * |
| Normal | 0.19 (0.11) | 0.19 | 0.14 | ||||
| Driving speed (km/h) (Exit of U-turn) | Post-stroke | 32.51 (3.06) | 31.27 | 5.35 | 0.634 | 0.635 | 0.783 |
| Normal | 31.71 (5.17) | 32.53 | 3.50 | ||||
| Std. deviation of speed (km/h) (Exit of U-turn) | Post-stroke | 5.17 (1.20) | 5.06 | 1.80 | 0.348 | 0.350 | 0.370 |
| Normal | 4.79 (0.81) | 4.60 | 1.08 |
| Variable | Group | Mean (std) | Median | IQR | One-Way ANOVA Test | Two-Tailed T-Test | Wilcoxon Rank-Sum Test |
|---|---|---|---|---|---|---|---|
| Lane deviation (Left turn) | Post-stroke | 0.52 (0.31) | 0.46 | 0.24 | 0.154 | 0.158 | 0.198 |
| Normal | 0.37 (0.16) | 0.37 | 0.17 | ||||
| SDLD (Left turn) | Post-stroke | 0.38 (0.39) | 0.23 | 0.16 | 0.106 | 0.117 | 0.291 |
| Normal | 0.20 (0.06) | 0.22 | 0.08 |
| Variable | Group | Mean (std) | Median | IQR | One-Way ANOVA Test | Two-Tailed T-Test | Wilcoxon Rank-Sum Test |
|---|---|---|---|---|---|---|---|
| Lane deviation (Straight line) | Post-stroke | 0.65 (0.26) | 0.68 | 0.34 | 0.104 | 0.104 | 0.118 |
| Normal | 0.83 (0.29) | 0.81 | 0.54 | ||||
| SDLD (Straight line) | Post-stroke | 0.24 (0.08) | 0.24 | 0.07 | 0.330 | 0.330 | 0.408 |
| Normal | 0.28 (0.11) | 0.26 | 0.13 | ||||
| Driving speed (km/h) | Post-stroke | 48.16 (6.72) | 49.33 | 6.85 | 0.285 | 0.286 | 0.198 |
| Normal | 45.00 (7.97) | 45.79 | 5.91 | ||||
| Std. deviation of speed (km/h) | Post-stroke | 2.58 (1.78) | 1.83 | 1.55 | 0.163 | 0.166 | 0.270 |
| Normal | 1.77 (0.96) | 1.75 | 1.20 |
| Variable | Group | Mean (std) | Median | IQR | One-Way ANOVA Test | Two-Tailed T-Test | Wilcoxon Rank-Sum Test |
|---|---|---|---|---|---|---|---|
| Lane deviation (Straight line) | Post-stroke | 0.30 (0.15) | 0.26 | 0.25 | 0.015 * | 0.019 * | 0.024 * |
| Normal | 0.60 (0.39) | 0.56 | 0.41 | ||||
| SDLD (Straight line) | Post-stroke | 0.14 (0.09) | 0.12 | 0.06 | 0.826 | 0.826 | 0.646 |
| Normal | 0.14 (0.08) | 0.12 | 0.07 | ||||
| Driving speed (km/h) | Post-stroke | 64.24 (6.04) | 63.66 | 8.98 | 0.521 | 0.521 | 0.963 |
| Normal | 62.38 (8.49) | 63.34 | 7.78 | ||||
| Std. deviation of speed (km/h) | Post-stroke | 1.68 (0.74) | 1.41 | 1.34 | 0.307 | 0.307 | 0.141 |
| Normal | 1.34 (0.91) | 1.07 | 1.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, H.; Sun, Q.; Blane, A.; Hughes, B.; Falkmer, T.; Xia, J. Investigating On-Road Lane Maintenance and Speed Regulation in Post-Stroke Driving: A Pilot Case–Control Study. Geriatrics 2021, 6, 16. https://doi.org/10.3390/geriatrics6010016
Zhou H, Sun Q, Blane A, Hughes B, Falkmer T, Xia J. Investigating On-Road Lane Maintenance and Speed Regulation in Post-Stroke Driving: A Pilot Case–Control Study. Geriatrics. 2021; 6(1):16. https://doi.org/10.3390/geriatrics6010016
Chicago/Turabian StyleZhou, Heng, Qian (Chayn) Sun, Alison Blane, Brett Hughes, Torbjörn Falkmer, and Jianhong (Cecilia) Xia. 2021. "Investigating On-Road Lane Maintenance and Speed Regulation in Post-Stroke Driving: A Pilot Case–Control Study" Geriatrics 6, no. 1: 16. https://doi.org/10.3390/geriatrics6010016
APA StyleZhou, H., Sun, Q., Blane, A., Hughes, B., Falkmer, T., & Xia, J. (2021). Investigating On-Road Lane Maintenance and Speed Regulation in Post-Stroke Driving: A Pilot Case–Control Study. Geriatrics, 6(1), 16. https://doi.org/10.3390/geriatrics6010016