Use of GPS for Older Adults to Decrease Driving Risk: Perceptions from Users and Non-Users

Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Participants
2.3. Procedure
3. Results
3.1. Usefulness
3.2. Ease of User Interface
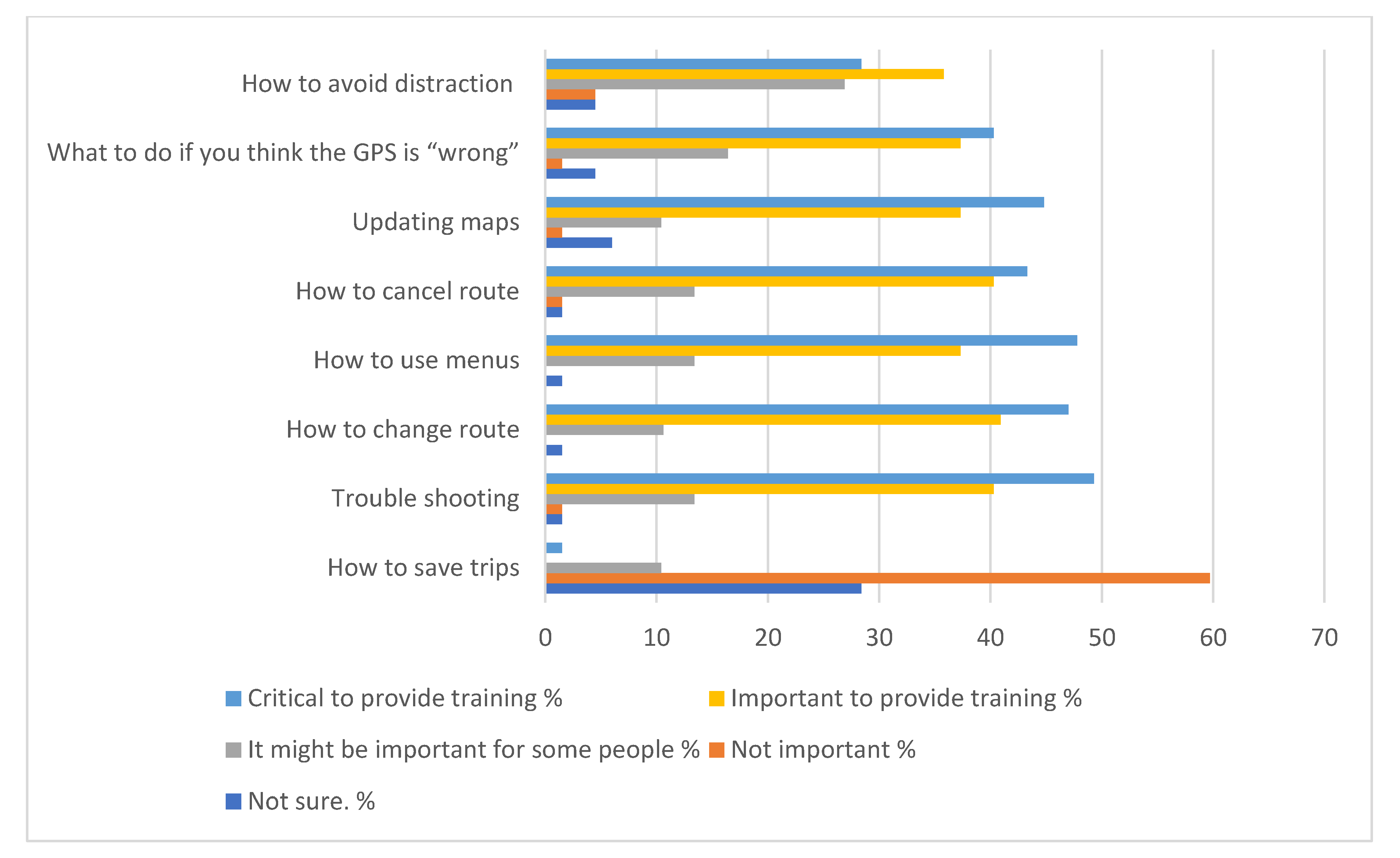
3.3. Training
4. Discussion
4.1. Training
4.2. Limitations
4.3. Implications
Funding
Conflicts of Interest
References
- Rosenbloom, S. The travel and mobility needs of older persons now and in the future. In Aging America and Transportation; Coughlin, J.D.A.L., Ed.; Springer Publishing: New York, NY, USA, 2012; pp. 39–54. [Google Scholar]
- Dickerson, A.E.; Molnar, L.J.; Bédard, M.; Eby, D.W.; Berg-Weger, M.; Choi, M.; Grigg, J.; Horowitz, A.; Meuser, T.; Myers, A.; et al. Transportation and Aging: An Updated Research Agenda to Advance Safe Mobility among Older Adults Transitioning From Driving to Non-driving. Gerontologist 2019, 59, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Lohman, M.C.; Mezuk, B. Trajectories of cognitive decline by driving mobility: Evidence from the Health and Retirement Study. Int. J. Geriatr. Psychiatry 2014, 29, 447–453. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, D.; Walshe, E.A.; Romer, D.; Winston, F.K. Transportation equity, health and aging: A novel approach to healthy longevity with benefits across the life span. Natl. Acad. Med. Perspect. 2019, 10.31478/201912a. [Google Scholar] [CrossRef]
- Wu, B. Social isolation and loneliness among older adults in the context of COVID-19: A global challenge. Glob. Health Res. Policy 2020, 5, 27. [Google Scholar] [CrossRef] [PubMed]
- Haustein, S.; Siren, A. Older People’s Mobility: Segments, Factors, Trends. Transp. Rev. 2015, 35, 466–487. [Google Scholar] [CrossRef]
- HLDI Bulletin. Predicted Availability of Safety Features on Registered Vehicles. 2012. Available online: https://www.iihs.org/media/db4aeba1-6209-4382-9ef2-275443fcccea/_LdQUQ/HLDI%20Research/Bulletins/hldi_bulletin_28.26.pdf (accessed on 15 July 2020).
- HLDI Bulletin. Predicted Availability and Fitment of Safety Features on Registered Vehicles. 2017. Available online: https://www.iihs.org/media/0a06d47a-84ba-44a0-b661-09f25e81d43d/q78xLA/HLDI%20Research/Bulletins/hldi_bulletin_34.28.pdf (accessed on 15 July 2020).
- Cicchino, J.B.; McCartt, A.T. Trends in older driver crash involvement rates and survivability in the United States: An update. Accid. Anal. Prev. 2014, 72, 44–54. [Google Scholar] [CrossRef]
- Theofilatos, A.; Yannis, G.; Kopelias, P.; Papadimitriou, F. Predicting Road Accidents: A Rare-events Modeling Approach. Transp. Res. Procedia 2016, 14, 3399–3405. [Google Scholar] [CrossRef]
- Transportation Research Board, Taxonomy and Terms for Stakeholders in Senior Mobility. 2016. Available online: http://onlinepubs.trb.org/Onlinepubs/circulars/ec211.pdf (accessed on 15 July 2020).
- May, A.J.; Ross, T.; Bayer, S.H. Drivers’ Information Requirements when Navigating in an Urban Environment. J. Navig. 2003, 56, 89–100. [Google Scholar] [CrossRef]
- Staplin, L.; Gish, K.W.; Wagner, E.K. MaryPODS revisited: Updated crash analysis and implications for screening program implementation. J. Saf. Res. 2003, 34, 389–397. [Google Scholar] [CrossRef]
- Iaria, G.; Palermo, L.; Committeri, G.; Barton, J.J.S. Age differences in the formation and use of cognitive maps. Behav. Brain Res. 2009, 196, 187–191. [Google Scholar] [CrossRef]
- Head, D.; Isom, M. Age effects on wayfinding and route learning skills. Behav. Brain Res. 2010, 209, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.D. A Technology Acceptance Model for Empirically Tesing New End-User Information Systems: Theory and Results. Ph.D. Thesis, Massachuesetts Institute of Technology, Cambridge, MA, USA, 1986. [Google Scholar]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef]
- Eby, D.W.; Kostyniuk, L.P. Maintaining older driver mobility and well-being with traveler information systems. Transp. Q. 1998, 52, 45–53. [Google Scholar]
- Cochran, L.M.; Dickerson, A.E. Driving while navigating: On-road driving performance using GPS or printed instructions. Can. J. Occup. Ther. 2019, 86, 61–69. [Google Scholar] [CrossRef]
- Chiang, D.P.; Brooks, A.M.; Weir, D.H. On the highway measures of driver glance behavior with an example automobile navigation system. Appl. Ergon. 2004, 35, 215–223. [Google Scholar] [CrossRef]
- Lee, W.-C.; Cheng, B.-W. Effects of using a portable navigation system and paper map in real driving. Accid. Anal. Prev. 2008, 40, 303–308. [Google Scholar] [CrossRef]
- Dopart, C.; Haggman, A.; Thornberry, C.; Mehler, B.; Dobres, J.; Reimer, B. A Driving Simulation Study Examining Destination Entry with iOS 5 Google Maps and a Garmin Portable GPS System. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, San Diego, CA, USA, 30 September–4 October 2013; pp. 1889–1893. [Google Scholar]
- Lo, V.E.-W.; Green, P.A.; Franzblau, A. Where Do People Drive? Navigation System Use by Typical Drivers and Auto Experts. J. Navig. 2011, 64, 357–373. [Google Scholar] [CrossRef]
- Green, P. Variations in Task Performance Between Younger and Older Drivers: UMTRI Research on Telematics. In Proceedings of the Association for the Advancement of Automotive Medicine Conference on Aging and Driving, Southfield, MI, USA, 19–20 February 2001. [Google Scholar]
- Zhong, J.Y.; Moffat, S.D. Age-Related Differences in Associative Learning of Landmarks and Heading Directions in a Virtual Navigation Task. Front. Aging Neurosci. 2016, 8, 122. [Google Scholar] [CrossRef]
- Vrkljan, B.H. Collaborative Learning Among Older Married Couples: An Exploratory Study. Educ. Gerontol. 2011, 37, 117–137. [Google Scholar] [CrossRef]
- Dennis Thomas, F.; Dickerson, A.E.; Graham, L.A.; Chandler Coleman, M.; Finstad, K.A.; Blomberg, R.D.; Wright, T.J. Teaching older drivers to navigate GPS technology. J. Saf. Res. 2020, 72, 165–171. [Google Scholar] [CrossRef]
- Bryden, K.J.; Charlton, J.L.; Oxley, J.A.; Lowndes, G.J. Self-reported wayfinding ability of older drivers. Accid. Anal. Prev. 2013, 59, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Portz, J.D.; Bayliss, E.A.; Bull, S.; Boxer, R.S.; Bekelman, D.B.; Gleason, K.; Czaja, S. Using the Technology Acceptance Model to Explore User Experience, Intent to Use, and Use Behavior of a Patient Portal Among Older Adults With Multiple Chronic Conditions: Descriptive Qualitative Study. J. Med Internet Res. 2019, 21, e11604. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Chan, A.H.S. A review of technology acceptance by older adults. Gerontechnology 2011, 10, 1–12. [Google Scholar] [CrossRef]
- Eby, D.W.; Molnar, L.J.; Zhang, L.; St Louis, R.M.; Zanier, N.; Kostyniuk, L.P.; Stanciu, S. Use, perceptions, and benefits of automotive technologies among aging drivers. Inj. Epidemiol. 2016, 3, 28. [Google Scholar] [CrossRef]
- Vrkljan, B.H.; Miller-Polgar, J. Advancements in vehicular technology: Potential implications for the older driver. Int. J. Veh. Inf. Commun. Syst. 2005, 1, 88–105. [Google Scholar] [CrossRef]
- Shaw, L.; Polgar, J.M.; Vrkljan, B.; Jacobson, J. Seniors’ perceptions of vehicle safety risks and needs. Am. J. Occup. Ther. 2010, 64, 215–224. [Google Scholar] [CrossRef]
- Rodgers, M.K.; Sindone, J.A.; Moffat, S.D. Effects of age on navigation strategy. Neurobiol. Aging 2012, 33, 202.e215-222. [Google Scholar] [CrossRef]
- Choi, Y.K. Examining the Feasibility of Internet of Things Technologies to Support Aging-in-Place. Ph.D. Thesis, University of Washington, Seattle, WA, USA, 2018. [Google Scholar]
- Mitzner, T.L.; Savla, J.; Boot, W.R.; Sharit, J.; Charness, N.; Czaja, S.J.; Rogers, W.A. Technology Adoption by Older Adults: Findings From the PRISM Trial. Gerontologist 2019, 59, 34–44. [Google Scholar] [CrossRef]
- Chappell, N.L.; Zimmer, Z. Receptivity to new technology among older adults. Disabil. Rehabil. 1999, 21, 222–230. [Google Scholar] [CrossRef]
- Mihailidis, A.; Cockburn, A.; Longley, C.; Boger, J. The Acceptability of Home Monitoring Technology Among Community-Dwelling Older Adults and Baby Boomers. Assist. Technol. 2008, 20, 1–12. [Google Scholar] [CrossRef]
- Vaportzis, E.; Giatsi Clausen, M.; Gow, A.J. Older Adults Perceptions of Technology and Barriers to Interacting with Tablet Computers: A Focus Group Study. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Mitzner, T.L.; Fausset, C.B.; Boron, J.B.; Adams, A.E.; Dijkstra, K.; Lee, C.C.; Rogers, W.A.; Fisk, A.D. Older adults’ training preferences for learning to use technology. In Proceedings of the Human Factors and Ergonomics Society, New York, NY, USA, 1 December 2008; pp. 2047–2051. [Google Scholar]
- Sangrar, R.; Mun, J.; Cammarata, M.; Griffith, L.E.; Letts, L.; Vrkljan, B. Older driver training programs: A systematic review of evidence aimed at improving behind-the-wheel performance. J. Saf. Res. 2019, 71, 295–313. [Google Scholar] [CrossRef] [PubMed]
- Eby, D.; Molnar, L.; Stanciu, S. Older Adults’ Attitudes and Opinions about Automated Vehicles: A Literature Review. 2018. Available online: http://www.atlas-center.org/wp-content/uploads/2018/11/ATLAS-Report-Older-Adults-and-Autonomous-Vehicles.pdf (accessed on 15 July 2020).
- Eby, D.W.; Molnar, L.J.; Zakrajsek, J.; Ryan, L.H.; Zanier, N.; St. Louis, R.M.; Stanciu, S.; LeBlanc, D.J.; Kostyniuk, L.P.; Smith, J.; et al. Use, Learning and Perceptions of In-Vehicle Technologies, and Vehicle Adaptations among Older Drivers: A LongROAD Study; AAA Foundation for Traffic Safety: Washington, DC, USA, 2017. [Google Scholar]



{kind=link}
{kind=link}
| Yes n (%) | No n (%) | χ2 | p | |
|---|---|---|---|---|
| Age: 60s | 5 (10) | 40 (35) | 5.61 | 0.02 |
| Age: 70s | 14 (9) | 30 (35) |
| Familiar n (%) | Unfamiliar n (%) | χ2 | p | |
|---|---|---|---|---|
| GPS was easier | 39 (43.8) | 27 (30.3) | 9.26 | 0.01 |
| About the same | 5 (5.6) | 8 (9.0) | ||
| Printed easier | 1 (1.1) | 9 (10.1) |
| Familiar n (%) | Unfamiliar n (%) | χ2 | p | |
|---|---|---|---|---|
| GPS | 37 (41.6) | 23 (25.8) | 9.49 | 0.009 |
| No preference | 5 (5.6) | 10 (11.2) | ||
| Printed | 3 (3.4) | 15 (16.9) |
| Familiar n (%) | Unfamiliar n (%) | χ2 | p | |
|---|---|---|---|---|
| Interest is Lower | 2 (2.2) | 1 (1.1) | 16.07 | 0.003 |
| Interest is the same | 30 (33.7) | 12 (13.5) | ||
| Interest is higher | 13 (14.6) | 31 (34.8) |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dickerson, A.E. Use of GPS for Older Adults to Decrease Driving Risk: Perceptions from Users and Non-Users. Geriatrics 2020, 5, 60. https://doi.org/10.3390/geriatrics5030060
Dickerson AE. Use of GPS for Older Adults to Decrease Driving Risk: Perceptions from Users and Non-Users. Geriatrics. 2020; 5(3):60. https://doi.org/10.3390/geriatrics5030060
Chicago/Turabian StyleDickerson, Anne E. 2020. "Use of GPS for Older Adults to Decrease Driving Risk: Perceptions from Users and Non-Users" Geriatrics 5, no. 3: 60. https://doi.org/10.3390/geriatrics5030060
APA StyleDickerson, A. E. (2020). Use of GPS for Older Adults to Decrease Driving Risk: Perceptions from Users and Non-Users. Geriatrics, 5(3), 60. https://doi.org/10.3390/geriatrics5030060