

Osteoporosis Is Associated with Cerebral Small Vessel Disease in Stroke-Free Individuals: A Retrospective Observational Study
Abstract
1. Introduction
2. Materials and Methods
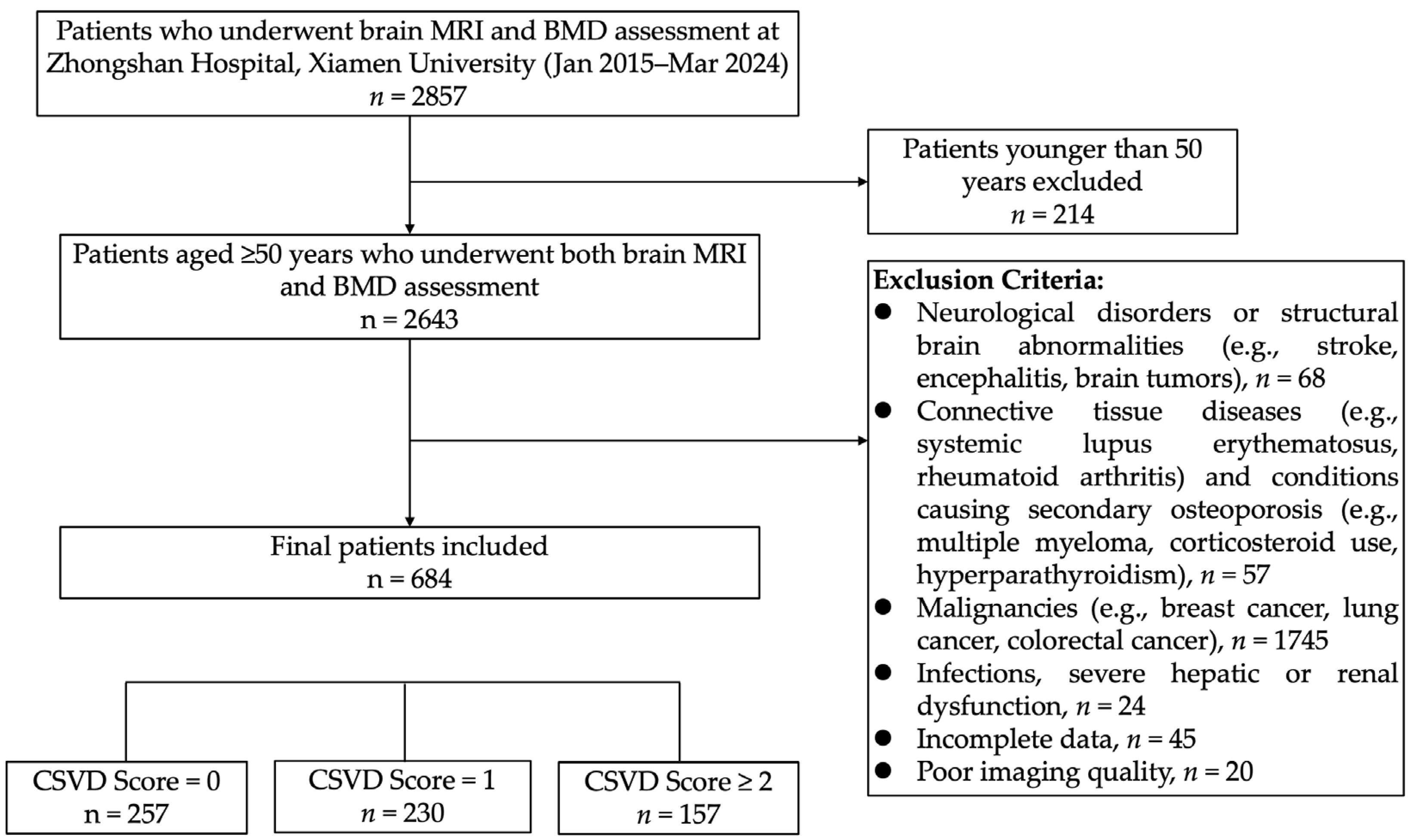
2.1. Study Participants and Data Collection
2.2. Measurement of CSVD
2.3. BMD Measurement
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Association Between Osteoporosis and CSVD Burden
4.2. Osteoporosis and Specific CSVD Imaging Markers
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CSVD | Cerebral Small Vessel Disease |
| EPVSs | Enlarged Perivascular Spaces |
| WMHs | White Matter Hyperintensities |
| BA | Brain Atrophy |
| BMD | Bone Mineral Density |
| CHD | Coronary Heart Disease |
| AF | Atrial Fibrillation |
| PAD | Peripheral Artery Disease |
| BMI | Body Mass Index |
| SBP | Systolic Blood Pressure |
| DBP | Diastolic Blood Pressure |
| WBC | White Blood Cell Count |
| RBC | Red Blood Cell Count |
| Hb | Hemoglobin |
| LDL-C | Low-Density Lipoprotein Cholesterol |
| TGs | Triglycerides |
| TC | Total Cholesterol |
| FPG | Fasting Plasma Glucose |
| ALT | Alanine Aminotransferase |
| eGFR | Estimated Glomerular Filtration Rate |
| CRP | C-Reactive Protein |
| DD | D-Dimer |
| TP | Total Protein |
| Alb | Albumin |
| Fbg | Fibrinogen |
| AST | Aspartate Aminotransferase |
| ALP | Alkaline Phosphatase |
| HDL-C | High-Density Lipoprotein Cholesterol |
| UA | Uric Acid |
References
- Wardlaw, J.M.; Smith, C.; Dichgans, M. Small vessel disease: Mechanisms and clinical implications. Lancet Neurol. 2019, 18, 684–696. [Google Scholar] [CrossRef] [PubMed]
- Staals, J.; Makin, S.D.; Doubal, F.N.; Dennis, M.S.; Wardlaw, J.M. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology 2014, 83, 1228–1234. [Google Scholar] [CrossRef] [PubMed]
- Cuadrado-Godia, E.; Dwivedi, P.; Sharma, S.; Ois Santiago, A.; Roquer Gonzalez, J.; Balcells, M.; Laird, J.; Turk, M.; Suri, H.S.; Nicolaides, A.; et al. Cerebral Small Vessel Disease: A Review Focusing on Pathophysiology, Biomarkers, and Machine Learning Strategies. J. Stroke 2018, 20, 302–320. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Su, Y.; Fu, J.; Shen, Y.; Dong, Q.; Cheng, X. Glymphatic pathway in sporadic cerebral small vessel diseases: From bench to bedside. Ageing Res. Rev. 2023, 86, 101885. [Google Scholar] [CrossRef]
- Kumar, A.A.; Yeo, N.; Whittaker, M.; Attra, P.; Barrick, T.R.; Bridges, L.R.; Dickson, D.W.; Esiri, M.M.; Farris, C.W.; Graham, D.; et al. Vascular Collagen Type-IV in Hypertension and Cerebral Small Vessel Disease. Stroke 2022, 53, 3696–3705. [Google Scholar] [CrossRef]
- Consensus development conference: Diagnosis, prophylaxis, and treatment of osteoporosis. Am. J. Med. 1993, 94, 646–650. [CrossRef]
- Hu, X.; Ma, S.; Chen, L.; Tian, C.; Wang, W. Association between osteoporosis and cardiovascular disease in elderly people: Evidence from a retrospective study. PeerJ 2023, 11, e16546. [Google Scholar] [CrossRef]
- Geng, G.; Li, Z.; Wang, S.; Yuan, T.; Quan, G. Association between bone mineral density and coronary plaque burden in patients with coronary artery disease: A cross-sectional study using quantitative computed tomography. Coron. Artery Dis. 2024, 35, 105–113. [Google Scholar] [CrossRef]
- Han, S.; Kim, N.R.; Kang, J.W.; Eun, J.S.; Kang, Y.M. Radial BMD and serum CTX-I can predict the progression of carotid plaque in rheumatoid arthritis: A 3-year prospective cohort study. Arthritis Res. Ther. 2021, 23, 258. [Google Scholar] [CrossRef]
- Liu, D.; Chen, L.; Dong, S.; Peng, Z.; Yang, H.; Chen, Y.; Li, L.; Zhou, H.; Zhou, R. Bone mass density and bone metabolism marker are associated with progression of carotid and cardiac calcified plaque in Chinese elderly population. Osteoporos. Int. 2019, 30, 1807–1815. [Google Scholar] [CrossRef]
- Shi, T.; Shen, S.; Shi, Y.; Wang, Q.; Zhang, G.; Lin, J.; Chen, J.; Bai, F.; Zhang, L.; Wang, Y.; et al. Osteocyte-derived sclerostin impairs cognitive function during ageing and Alzheimer’s disease progression. Nat. Metab. 2024, 6, 531–549. [Google Scholar] [CrossRef] [PubMed]
- Dauphinot, V.; Laurent, M.; Prodel, M.; Civet, A.; Vainchtock, A.; Moutet, C.; Krolak-Salmon, P.; Garnier-Crussard, A. Identification of profiles associated with conversions between the Alzheimer’s disease stages, using a machine learning approach. Alzheimers Res. Ther. 2024, 16, 166. [Google Scholar] [CrossRef]
- Tang, A.S.; Rankin, K.P.; Cerono, G.; Miramontes, S.; Mills, H.; Roger, J.; Zeng, B.; Nelson, C.; Soman, K.; Woldemariam, S.; et al. Leveraging electronic health records and knowledge networks for Alzheimer’s disease prediction and sex-specific biological insights. Nat. Aging 2024, 4, 379–395. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.H.; Huang, Y.P.; Yeh, K.C.; Pan, S.L. Osteoporosis and the Risk of Parkinson’s Disease: A Nationwide, Propensity Score-Matched, Longitudinal Follow-up Study. J. Clin. Endocrinol. Metab. 2021, 106, e763–e771. [Google Scholar] [CrossRef] [PubMed]
- Park, K.Y.; Jung, J.H.; Hwang, H.S.; Park, H.K.; Han, K.; Nam, G.E. Bone Mineral Density and the Risk of Parkinson’s Disease in Postmenopausal Women. Mov. Disord. 2023, 38, 1606–1614. [Google Scholar] [CrossRef]
- Kim, J.M.; Park, K.Y.; Kim, H.R.; Ahn, H.Y.; Pantoni, L.; Park, M.S.; Han, S.H.; Jung, H.B.; Bae, J. Association of Bone Mineral Density to Cerebral Small Vessel Disease Burden. Neurology 2021, 96, e1290–e1300. [Google Scholar] [CrossRef]
- Kalc, P.; Dahnke, R.; Hoffstaedter, F.; Gaser, C. Low bone mineral density is associated with gray matter volume decrease in UK Biobank. Front. Aging Neurosci. 2023, 15, 1287304. [Google Scholar] [CrossRef]
- Pan, H.; Cao, J.; Wu, C.; Huang, F.; Wu, P.; Lang, J.; Liu, Y. Osteoporosis is associated with elevated baseline cerebrospinal fluid biomarkers and accelerated brain structural atrophy among older people. Front. Aging Neurosci. 2022, 14, 958050. [Google Scholar] [CrossRef]
- Bae, I.S.; Kim, J.M.; Cheong, J.H.; Ryu, J.I.; Han, M.H. Association between bone mineral density and brain parenchymal atrophy and ventricular enlargement in healthy individuals. Aging 2019, 11, 8217–8238. [Google Scholar] [CrossRef]
- Li, X.; Wu, X.; Zhou, G.; Mo, D.; Lin, X.; Wang, P.; Zeng, Y.; Luo, M. Estimated bone mineral density and white matter hyperintensities: A bidirectional Mendelian randomization study. Bone 2024, 187, 117138. [Google Scholar] [CrossRef]
- Duering, M.; Biessels, G.J.; Brodtmann, A.; Chen, C.; Cordonnier, C.; de Leeuw, F.E.; Debette, S.; Frayne, R.; Jouvent, E.; Rost, N.S.; et al. Neuroimaging standards for research into small vessel disease-advances since 2013. Lancet Neurol. 2023, 22, 602–618. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef]
- Doubal, F.N.; MacLullich, A.M.; Ferguson, K.J.; Dennis, M.S.; Wardlaw, J.M. Enlarged perivascular spaces on MRI are a feature of cerebral small vessel disease. Stroke 2010, 41, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Gregson, C.L.; Armstrong, D.J.; Bowden, J.; Cooper, C.; Edwards, J.; Gittoes, N.J.L.; Harvey, N.; Kanis, J.; Leyland, S.; Low, R.; et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch. Osteoporos. 2022, 17, 58. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Wang, Y.; Wang, H.; Wang, L.; Huan, B.; Liu, C. Correlation study: Bone density and circulating inflammatory markers in postmenopausal patients. Immun. Inflamm. Dis. 2024, 12, e1365. [Google Scholar] [CrossRef]
- Leungsuwan, D.S.; Chandran, M. Bone Fragility in Diabetes and its Management: A Narrative Review. Drugs 2024, 84, 1111–1134. [Google Scholar] [CrossRef] [PubMed]
- Croll, P.H.; Boelens, M.; Vernooij, M.W.; van de Rest, O.; Zillikens, M.C.; Ikram, M.A.; Voortman, T. Associations of vitamin D deficiency with MRI markers of brain health in a community sample. Clin. Nutr. 2021, 40, 72–78. [Google Scholar] [CrossRef]
- Chung, P.W.; Park, K.Y.; Kim, J.M.; Shin, D.W.; Park, M.S.; Chung, Y.J.; Ha, S.Y.; Ahn, S.W.; Shin, H.W.; Kim, Y.B.; et al. 25-hydroxyvitamin D status is associated with chronic cerebral small vessel disease. Stroke 2015, 46, 248–251. [Google Scholar] [CrossRef]
- Dutka, M.; Garczorz, W.; Kosowska, A.; Buczek, E.; Godek, P.; Wojakowski, W.; Francuz, T. Osteoprotegerin Is Essential for the Development of Endothelial Dysfunction Induced by Angiotensin II in Mice. Int. J. Mol. Sci. 2024, 25, 6434. [Google Scholar] [CrossRef]
- Tschiderer, L.; Klingenschmid, G.; Nagrani, R.; Willeit, J.; Laukkanen, J.A.; Schett, G.; Kiechl, S.; Willeit, P. Osteoprotegerin and Cardiovascular Events in High-Risk Populations: Meta-Analysis of 19 Prospective Studies Involving 27,450 Participants. J. Am. Heart Assoc. 2018, 7, e009012. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.T.; Liu, M.H.; Xiong, Y.; Wang, Y.J.; Bu, X.L. Crosstalk between bone and brain in Alzheimer’s disease: Mechanisms, applications, and perspectives. Alzheimers Dement. 2024, 20, 5720–5739. [Google Scholar] [CrossRef]
- Liang, W.; Wei, T.; Hu, L.; Chen, M.; Tong, L.; Zhou, W.; Duan, X.; Zhao, X.; Zhou, W.; Jiang, Q.; et al. An integrated multi-omics analysis reveals osteokines involved in global regulation. Cell Metab. 2024, 36, 1144–1163.e1147. [Google Scholar] [CrossRef]
- Wang, Z.X.; Luo, Z.W.; Li, F.X.; Cao, J.; Rao, S.S.; Liu, Y.W.; Wang, Y.Y.; Zhu, G.Q.; Gong, J.S.; Zou, J.T.; et al. Aged bone matrix-derived extracellular vesicles as a messenger for calcification paradox. Nat. Commun. 2022, 13, 1453. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Chen, Y.; Guo, C.; Fu, Y.; Qin, C.; Zhu, Q.; Wang, J.; Zhang, R.; Tian, H.; Feng, R.; et al. Mutations in ARHGEF15 cause autosomal dominant hereditary cerebral small vessel disease and osteoporotic fracture. Acta Neuropathol. 2023, 145, 681–705. [Google Scholar] [CrossRef]
- Camon, C.; Garratt, M.; Correa, S.M. Exploring the effects of estrogen deficiency and aging on organismal homeostasis during menopause. Nat. Aging 2024, 4, 1731–1744. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.T.; Wang, Z.J.; Cai, H.Y.; Yuan, L.; Hu, M.M.; Wu, M.N.; Qi, J.S. Sex Differences in Neuropathology and Cognitive Behavior in APP/PS1/tau Triple-Transgenic Mouse Model of Alzheimer’s Disease. Neurosci. Bull. 2018, 34, 736–746. [Google Scholar] [CrossRef]
- Chakrabarti, S.; Morton, J.S.; Davidge, S.T. Mechanisms of estrogen effects on the endothelium: An overview. Can. J. Cardiol. 2014, 30, 705–712. [Google Scholar] [CrossRef]
- McCarthy, M.; Raval, A.P. The peri-menopause in a woman’s life: A systemic inflammatory phase that enables later neurodegenerative disease. J. Neuroinflamm. 2020, 17, 317. [Google Scholar] [CrossRef]
- Andrew, T.W.; Koepke, L.S.; Wang, Y.; Lopez, M.; Steininger, H.; Struck, D.; Boyko, T.; Ambrosi, T.H.; Tong, X.; Sun, Y.; et al. Sexually dimorphic estrogen sensing in skeletal stem cells controls skeletal regeneration. Nat. Commun. 2022, 13, 6491. [Google Scholar] [CrossRef]
- Rinonapoli, G.; Ruggiero, C.; Meccariello, L.; Bisaccia, M.; Ceccarini, P.; Caraffa, A. Osteoporosis in Men: A Review of an Underestimated Bone Condition. Int. J. Mol. Sci. 2021, 4, 2105. [Google Scholar] [CrossRef] [PubMed]
- Fleischman, D.A.; Arfanakis, K.; Leurgans, S.E.; Arvanitakis, Z.; Lamar, M.; Han, S.D.; Poole, V.N.; Bennett, D.A.; Barnes, L.L. Cerebral arteriolosclerosis, lacunar infarcts, and cognition in older Black adults. Alzheimers Dement. 2024, 20, 5375–5384. [Google Scholar] [CrossRef] [PubMed]
- Alber, J.; Alladi, S.; Bae, H.J.; Barton, D.A.; Beckett, L.A.; Bell, J.M.; Berman, S.E.; Biessels, G.J.; Black, S.E.; Bos, I.; et al. White matter hyperintensities in vascular contributions to cognitive impairment and dementia (VCID): Knowledge gaps and opportunities. Alzheimers Dement. 2019, 5, 107–117. [Google Scholar] [CrossRef]
- Georgakis, M.K.; Duering, M.; Wardlaw, J.M.; Dichgans, M. WMH and long-term outcomes in ischemic stroke: A systematic review and meta-analysis. Neurology 2019, 92, e1298–e1308. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| CSVD = 0 (257) | CSVD = 1 (230) | CSVD = 2 a (197) | p | F/H/χ2 e | |
|---|---|---|---|---|---|
| Age (year, median (IQR)) | 61 (56, 69) | 69 (61, 75) | 76 (69, 82) | <0.001 | 158.9 |
| SBP (mmHg, median (IQR)) | 127 (115, 142) | 133 (121, 145) | 138 (125, 152) | <0.001 | 29.3 |
| BMI (kg/m2, median (IQR)) | 23.61 (21.91, 24.83) | 23.44 (21.64, 25.64) | 23.56 (21.57, 24.95) | 0.713 | 0.7 |
| TP (g/L, median (IQR)) | 70.8 (67.4, 74.7) | 70.55 (66.8, 74.5) | 68.6 (64.8, 72.5) | <0.001 | 20.5 |
| Alb (g/L, median (IQR)) | 41.6 (39.2, 43.7) | 40.56 (38, 42.9) | 38.6 (36.1, 41.1) | <0.001 | 55.9 |
| ALT (U/L, median (IQR)) | 18.3 (13, 26.3) | 15.9 (12, 22.6) | 15.8 (12, 20.8) | <0.001 | 16.4 |
| AST (U/L, median (IQR)) | 20 (17.3, 26.7) | 19.4 (16.6, 23.5) | 20.2 (17, 24.8) | 0.194 | 3.3 |
| ALP (U/L, median (IQR)) | 77.2 (63, 92.2) | 77.95 (62.1, 94.5) | 79.7 (63.7, 93) | 0.870 | 0.3 |
| TC (mmol/L, median (IQR)) | 5.04 (4.23, 5.91) | 4.89 (4.2, 5.66) | 4.56 (3.88, 5.18) | <0.001 | 24.3 |
| HDL-C (mmol/L, median (IQR)) | 1.34 (1.12, 1.51) | 1.27 (1.08, 1.5) | 1.21 (1.01, 1.45) | 0.005 | 10.8 |
| LDL-C (mmol/L, median (IQR)) | 3.34 (2.69, 3.99) | 3.23 (2.67, 3.79) | 2.9 (2.39, 3.52) | <0.001 | 21.2 |
| TG (mmol/L, median (IQR)) | 1.28 (0.97, 1.81) | 1.47 (1.06, 1.97) | 1.23 (0.9, 1.76) | 0.008 | 9.7 |
| FPG (mmol/L, median (IQR)) | 5.47 (4.97, 6.55) | 5.74 (5.09, 6.9) | 5.75 (5.02, 6.89) | 0.090 | 4.8 |
| eGFR(mL/min/1.73 × m2, median (IQR)) | 94.7 (86.3, 102.3) | 89.6 (74.8, 96.5) | 84.2 (72.3, 91.9) | <0.001 | 72.3 |
| UA (umol/L, median (IQR)) | 334 (272.2, 394) | 347.9 (276.5, 404.9) | 328.1 (275, 403) | 0.492 | 1.4 |
| WBC (×109/L, median (IQR)) | 5.94 (5.09, 6.05) | 6.10 (5.14, 7.33) | 6.57 (5.61, 7.91) | <0.001 | 16.7 |
| PLT (×109/L, median (IQR)) | 229 (192, 262) | 222 (189, 265) | 228 (189, 264) | 0.732 | 0.6 |
| RBC (×1012/L, median (IQR)) | 4.38 (4.09, 4.73) | 4.31 (3.94, 4.66) | 4.17 (3.77, 4.52) | <0.001 | 18.7 |
| CRP (mg/L, median (IQR)) | 2 (0.88, 4.36) | 2.39 (0.97, 7) | 3 (1.22, 7.9) | 0.007 | 9.8 |
| DD (ug/mL, median (IQR)) | 0.36 (0.23, 0.87) | 0.51 (0.26, 1.14) | 0.76 (0.37, 1.35) | <0.001 | 9.2 |
| Fbg (g/L, median (IQR)) | 3.06 (2.64, 3.49) | 3.15 (2.72, 3.6) | 3.26 (2.78, 3.82) | 0.010 | 39.0 |
| Female, n (%) | 184 (71.6) | 156 (67.8) | 122 (61.9) | 0.092 | 4.8 |
| Diabetes, n (%) | 92 (35.8) | 91 (39.6) | 90 (45.7) | 0.102 | 4.6 |
| Hypertension, n (%) | 104 (40.5) | 125 (54.3) | 148 (75.1) | <0.001 | 54.2 |
| Dyslipidemia, n (%) | 108 (42.4) | 98 (42.6) | 67 (34.0) | 0.121 | 4.2 |
| PAD, n (%) | 92 (35.8) | 110 (47.8) | 120 (60.9) | <0.001 | 28.3 |
| Hyperuricemia, n (%) | 42 (16.7) | 45 (19.6) | 38 (19.3) | 0.787 | 0.7 |
| AF, n (%) | 1 (0.40) | 6 (2.60) | 7 (3.60) | 0.033 | 6.8 |
| CHD, n (%) | 13 (5.10) | 19 (8.30) | 31 (15.7) | <0.001 | 15.6 |
| Current smoking, n (%) | 21 (8.20) | 17 (7.40) | 15 (7.60) | 0.946 | 0.1 |
| Current dinking, n (%) | 16 (6.60) | 13 (5.70) | 10 (5.10) | 0.777 | 0.5 |
| Spine BMD (g/cm2, median (IQR)) | 1.007 (0.868, 1.126) | 0.937 (0.826, 1.807) | 0.926 (0.778, 1.098) | 0.002 | 12.4 |
| Hip BMD (g/cm2, mean ± SD) | 0.856 ± 0.143 | 0.799 ± 0.163 | 0.758 ± 0.174 | <0.001 | 21.5 |
| Normal b, n (%) | 49 (19.1) | 27 (11.7) | 14 (7.10) | <0.001 | 40.1 |
| Osteopenia c, n (%) | 126 (49.4) | 96 (41.7) | 65 (33.0) | ||
| Osteoporosis d, n (%) | 80 (31.5) | 107 (46.5) | 118 (59.9) | ||
| Normal (hip), n (%) | 65 (25.3) | 33 (14.3) | 16 (8.10) | <0.001 | 55.5 |
| Osteopenia (hip), n (%) | 138 (53.7) | 114 (49.6) | 79 (40.1) | ||
| Osteoporosis (hip), n (%) | 53 (21.0) | 83 (36.1) | 102 (51.8) | ||
| Normal (spine), n (%) | 101 (39.3) | 76 (33.0) | 64 (32.5) | 0.007 | 14.0 |
| Osteopenia (spine), n (%) | 92 (35.8) | 82 (35.7) | 53 (26.9) | ||
| Osteoporosis (spine), n (%) | 63 (24.9) | 72 (31.3) | 80 (40.6) |
| Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| Unadjusted OR (95%CI) | p | Adjusted OR (95%CI) | p | |
| Osteopenia a | 1.532 (0.974, 2.410) | 0.065 | 1.535 (0.924, 2.552) | 0.097 |
| Osteoporosis b | 3.333 (2.119, 5.243) | <0.001 * | 2.332 (1.345, 4.039) | 0.003 * |
| Hip osteopenia | 1.871 (1.241, 2.826) | 0.003 * | 1.787 (1.125, 2.806) | 0.014 * |
| Hip osteoporosis | 4.517 (2.921, 6.986) | <0.001 * | 2.598 (1.540, 4.384) | <0.001 * |
| Spine osteopenia | 0.971 (0.694, 1.359) | 0.866 | 1.225 (0.834, 1.796) | 0.300 |
| Spine osteoporosis | 1.69 (1.203, 2.375) | 0.002 * | 1.515 (1.01, 2.272) | 0.044 * |
| Hip BMD/(2 × LSD c) | 0.886 (0.853, 0.920) | <0.001 * | 0.929 (0.887, 0.972) | 0.001 * |
| Spine BMD/(2 × LSD d) | 0.953 (0.924, 0.982) | 0.002 * | 0.952 (0.917, 0.989) | 0.012 * |
| Variables | Male | Female | ||
|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | |
| Osteopenia a | 1.52 (0.756, 3.055) | 0.239 | 1.724 (0.771, 3.853) | 0.184 |
| Osteoporosis b | 2.332 (0.981, 5.540) | 0.055 | 2.529 (1.122, 5.703) | 0.025 * |
| Hip osteopenia | 1.938 (0.999, 3.765) | 0.050 | 1.993 (1.003, 3.962) | 0.049 * |
| Hip osteoporosis | 1.964 (0.801, 4.816) | 0.140 | 3.129 (1.517, 6.455) | 0.002 * |
| Spine osteopenia | 0.761(0.392, 1.476) | 0.420 | 1.558 (0.954, 2.549) | 0.077 |
| Spine osteoporosis | 1.625 (0.732, 3.603) | 0.232 | 1.755 (1.057, 2.912) | 0.030 * |
| Hip BMD/(2 × LSD c) | 0.973 (0.903, 1.050) | 0.491 | 0.907 (0.854, 0.963) | 0.001 * |
| Spine BMD/(2 × LSD d) | 0.959 (0.901, 1.021) | 0.197 | 0.944 (0.899, 0.993) | 0.025 * |
| Imaging Features | Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|---|
| Unadjusted OR (95%CI) | p | Adjusted OR (95%CI) | p | ||
| BA = 1 a | Osteopenia b | 0.923 (0.574, 1.482) | 0.740 | 0.608 (0.339, 1.090) | 0.095 |
| Osteoporosis c | 2.533 (1.562, 4.116) | <0.001 * | 1.030 (0.543, 1.952) | 0.928 | |
| Hip osteopenia | 1.243 (0.79, 1.956) | 0.346 | 0.726 (0.376, 1.400) | 0.339 | |
| Hip osteoporosis | 5.359 (2.97, 9.671) | <0.001 * | 2.141 (0.906, 5.060) | 0.083 | |
| Spine osteopenia | 0.903 (0.6, 1.36) | 0.626 | 0.961 (0.516, 1.79) | 0.899 | |
| Spine osteoporosis | 1.8 (1.139, 2.843) | 0.012 * | 1.019 (0.496, 2.095) | 0.959 | |
| BA = 2 a | Osteopenia b | 0.923 (0.574, 1.482) | 0.740 | 0.608 (0.339, 1.090) | 0.095 |
| Osteoporosis c | 2.533 (1.562, 4.116) | <0.001 * | 1.030 (0.543, 1.952) | 0.928 | |
| Hip osteopenia | 10.207 (4.238, 24.582) | 0.817 | 0.439 (0.136, 1.409) | 0.166 | |
| Hip osteoporosis | 0.904 (0.384, 2.219) | <0.001 * | 2.411 (0.642, 9.050) | 0.192 | |
| Spine osteopenia | 0.507 (0.697, 2.551) | 0.045 | 0.822 (0.309, 2.185) | 0.694 | |
| Spine osteoporosis | 1.333 (0.697, 2.551) | 0.385 | 0.731 (0.261, 2.043) | 0.550 | |
| Lacune | Osteopenia b | 1.354 (0.798, 2.295) | 0.261 | 1.292 (0.682, 2.449) | 0.432 |
| Osteoporosis c | 2.86 (1.703, −4.802) | <0.001 * | 1.773 (0.924, 3.403) | 0.085 | |
| Hip osteopenia | 1.626 (0.998, 2.649) | 0.051 | 1.492 (0.838, 2.659) | 0.174 | |
| Hip osteoporosis | 4.328 (2.619, 7.151) | <0.001 * | 2.215 (1.197, 4.100) | 0.011 * | |
| Spine osteopenia | 0.718 (0.492, 1.048) | 0.086 | 0.823 (0.523, 1.297) | 0.402 | |
| Spine osteoporosis | 1.378 (0.951, 1.997) | 0.090 | 0.622 (0.26, 1.485) | 0.419 | |
| Multiple lacunes d | Osteopenia b | 1.521 (0.733, 3.513) | 0.013 * | 1.606 (0.715, 3.606) | 0.251 |
| Osteoporosis c | 2.462 (1.212, 4.999) | 0.010 * | 1.73 (0.763, 3.921) | 0.189 | |
| Hip osteopenia | 1.55 (0.774, 3.102) | 0.216 | 1.497 (0.701, 3.198) | 0.297 | |
| Hip osteoporosis | 3.878 (1.962, 7.665) | <0.001 * | 2.274 (1.039, 4.98) | 0.04 * | |
| Spine osteopenia | 0.852 (0.531, 1.369) | 0.509 | 1.087 (0.637, 1.856) | 0.76 | |
| Spine osteoporosis | 1.084 (0.684, 1.72) | 0.731 | 1.025 (0.603, 1.743) | 0.926 | |
| EPVS ≥ 2 e | Osteopenia b | 1.499 (0.896, 2.507) | 0.123 | 1.673 (0.967, 2.896) | 0.066 |
| Osteoporosis c | 2.131 (1.282, 3.543) | 0.004 * | 2.222 (1.234, 4.004) | 0.008 | |
| Hip osteopenia | 1.628 (1.027, 2.581) | 0.038 * | 1.735 (1.058, 2.844) | 0.029 * | |
| Hip osteoporosis | 2.165 (1.342, 3.491) | 0.002 * | 1.99 (1.133, 3.495) | 0.017 * | |
| Spine osteopenia | 1.184 (0.815, 1.721) | 0.375 | 1.514 (1.004, 2.284) | 0.048 * | |
| Spine osteoporosis | 1.498 (1.029, 2.18) | 0.035 | 1.652 (1.075, 2.538) | 0.022 * | |
| WMH | Osteopenia b | 1.34 (0.812, 2.211) | 0.252 | 1.209 (0.676, 2.162) | 0.523 |
| Osteoporosis c | 2.759 (1.63, 4.668) | <0.001 * | 1.608 (0.849, 3.047) | 0.145 | |
| Hip osteopenia | 1.449 (0.925, 2.27) | 0.105 | 1.164 (0.694, 1.952) | 0.566 | |
| Hip osteoporosis | 4.064 (2.369, 6.971) | <0.001 * | 1.837 (0.974, 3.467) | 0.060 * | |
| Spine osteopenia | 0.882 (0.587, 1.325) | 0.545 | 1.052 (0.656, 1.685) | 0.834 | |
| Spine osteoporosis | 1.606 (1.024, 2.52) | 0.039 * | 1.336 (0.784, 2.276) | 0.287 | |
| Severe WMH f | Osteopenia b | 1.6 (0.774, 3.309) | 0.205 | 1.649 (0.716, 3.794) | 0.240 |
| Osteoporosis c | 3.386 (1.679, 6.83) | 0.001 * | 2.041 (0.901, 4.622) | 0.087 | |
| Hip osteopenia | 2.21 (1.088, 4.486) | 0.028 * | 2.061 (0.931, 4.562) | 0.075 | |
| Hip osteoporosis | 5.332 (2.642, 10.758) | <0.001 * | 2.611 (1.171, 5.823) | 0.019 * | |
| Spine osteopenia | 0.842 (0.532, 1.333) | 0.464 | 1.085 (0.633, 1.859) | 0.766 | |
| Spine osteoporosis | 1.402 (0.909, 2.162) | 0.126 | 1.193 (0.717, 1.987) | 0.497 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, X.; Chen, L.; Deng, M.; Liu, J.; Cai, J.; Su, C. Osteoporosis Is Associated with Cerebral Small Vessel Disease in Stroke-Free Individuals: A Retrospective Observational Study. Geriatrics 2025, 10, 66. https://doi.org/10.3390/geriatrics10030066
Xiao X, Chen L, Deng M, Liu J, Cai J, Su C. Osteoporosis Is Associated with Cerebral Small Vessel Disease in Stroke-Free Individuals: A Retrospective Observational Study. Geriatrics. 2025; 10(3):66. https://doi.org/10.3390/geriatrics10030066
Chicago/Turabian StyleXiao, Xueling, Luling Chen, Manxiang Deng, Jingqi Liu, Jiayan Cai, and Chuhan Su. 2025. "Osteoporosis Is Associated with Cerebral Small Vessel Disease in Stroke-Free Individuals: A Retrospective Observational Study" Geriatrics 10, no. 3: 66. https://doi.org/10.3390/geriatrics10030066
APA StyleXiao, X., Chen, L., Deng, M., Liu, J., Cai, J., & Su, C. (2025). Osteoporosis Is Associated with Cerebral Small Vessel Disease in Stroke-Free Individuals: A Retrospective Observational Study. Geriatrics, 10(3), 66. https://doi.org/10.3390/geriatrics10030066