


A High Grade Astrocytoma with Pilocytic Morphology in a 5-Month-Old American Bulldog
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
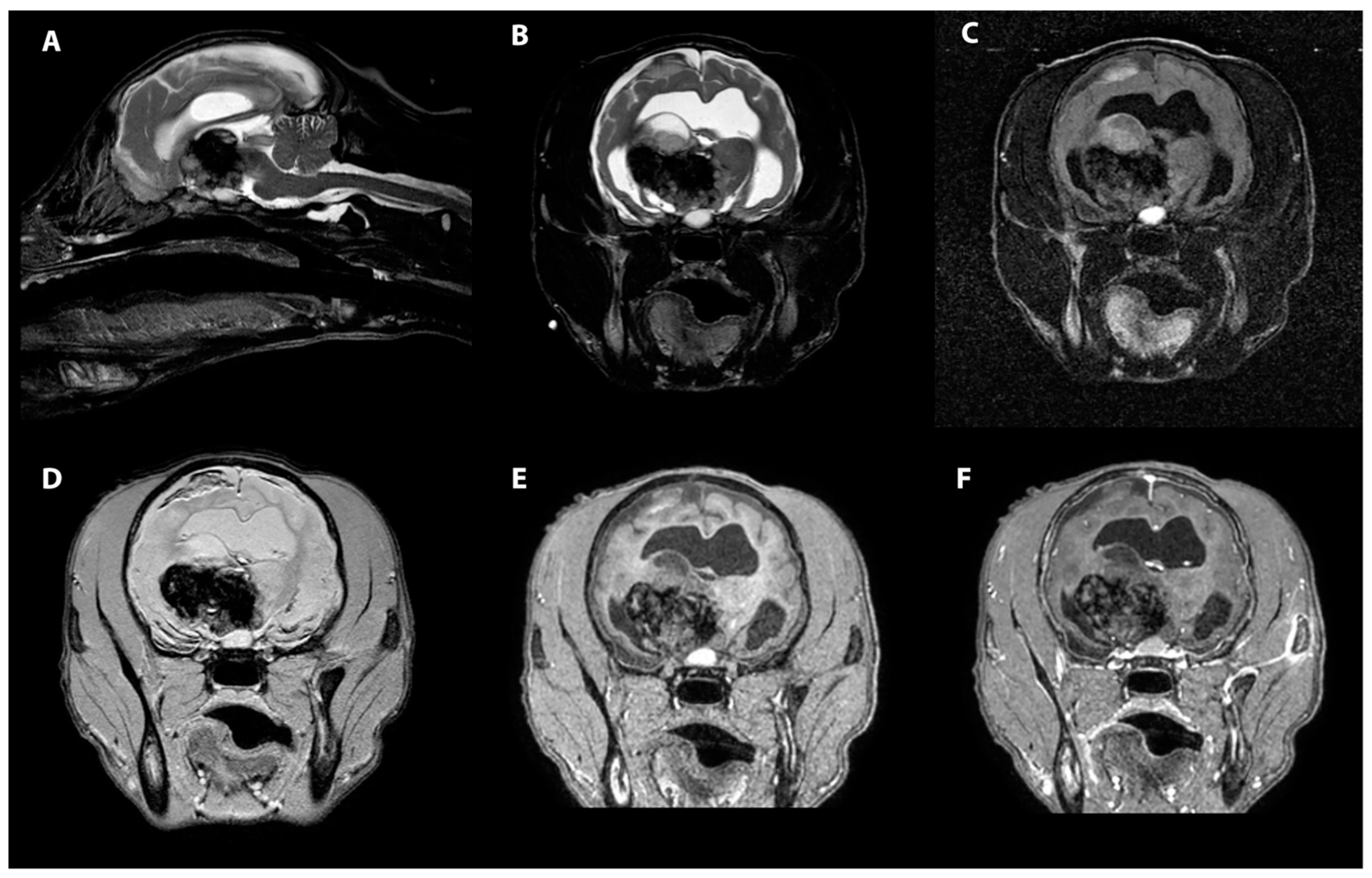
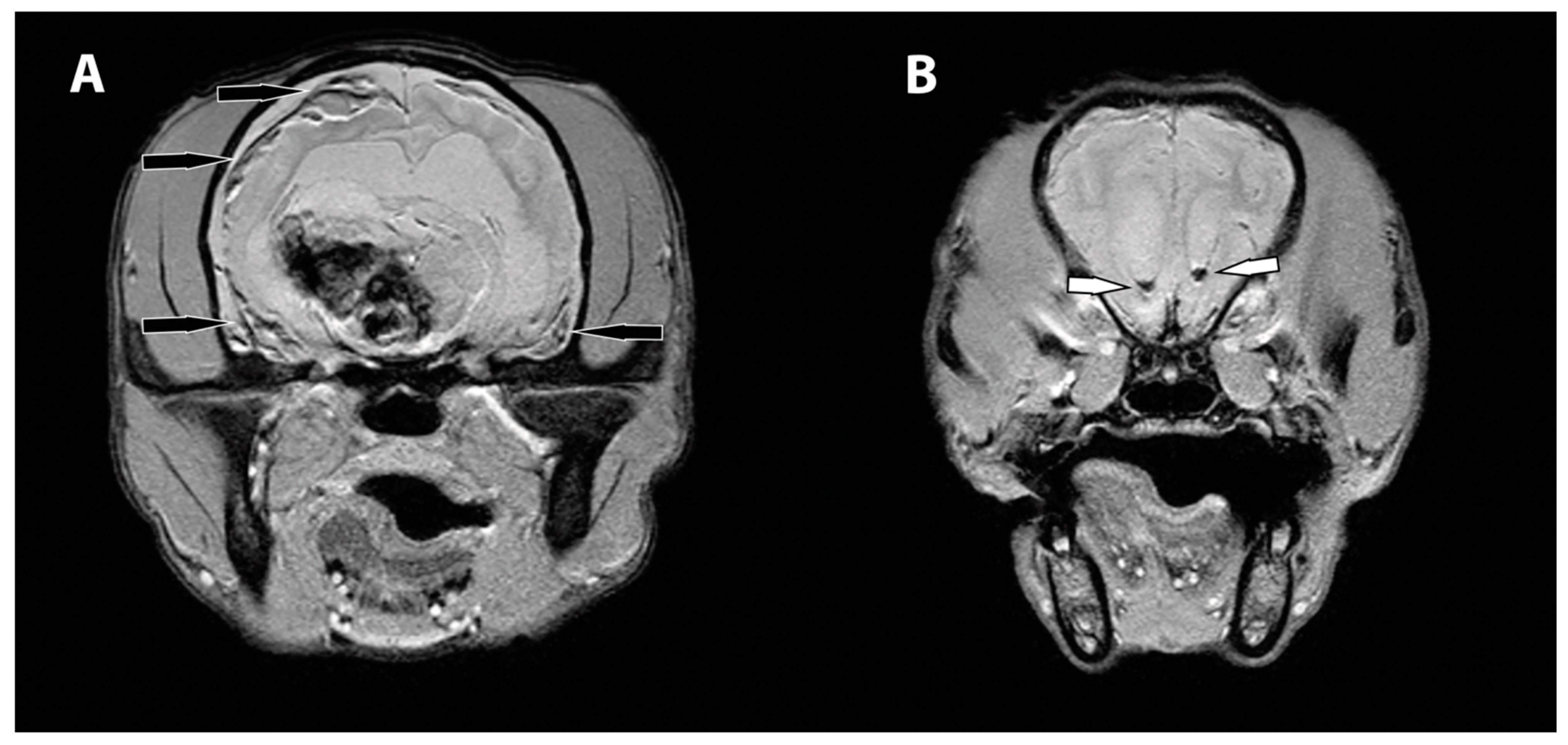
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorn, C.R.; Taylor, D.O.; Frye, F.L.; Hibbard, H.H. Survey of animal neoplasms in Alameda and Contra Costa Counties, California. I. Methodology and description of cases. J. Natl. Cancer Inst. 1968, 40, 295–305. [Google Scholar] [PubMed]
- Zaki, F.A. Spontaneous central nervous system tumors in the dog. Vet. Clin. N. Am. 1977, 7, 153–163. [Google Scholar] [CrossRef]
- Snyder, J.M.; Shofer, F.S.; Van Winkle, T.J.; Massicotte, C. Canine intracranial primary neoplasia: 173 cases (1986–2003). J. Vet. Intern. Med. 2006, 20, 669–675. [Google Scholar] [CrossRef]
- Song, R.B.; Vite, C.H.; Bradley, C.W.; Cross, J.R. Postmortem evaluation of 435 cases of intracranial neoplasia in dogs and relationship of neoplasm with breed, age, and body weight. J. Vet. Intern. Med. 2013, 27, 1143–1152. [Google Scholar] [CrossRef]
- Truve, K.; Dickinson, P.; Xiong, A.; York, D.; Jayashankar, K.; Pielberg, G.; Koltookian, M.; Muren, E.; Fuxelius, H.H.; Weishaupt, H.; et al. Utilizing the Dog Genome in the Search for Novel Candidate Genes Involved in Glioma Development-Genome Wide Association Mapping followed by Targeted Massive Parallel Sequencing Identifies a Strongly Associated Locus. PLoS Genet. 2016, 12, e1006000. [Google Scholar] [CrossRef]
- Miller, A.D.; Miller, C.R.; Rossmeisl, J.H. Canine Primary Intracranial Cancer: A Clinicopathologic and Comparative Review of Glioma, Meningioma, and Choroid Plexus Tumors. Front. Oncol. 2019, 9, 1151. [Google Scholar] [CrossRef]
- Ohgaki, H.; Kleihues, P. Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligodendroglial gliomas. J. Neuropathol. Exp. Neurol. 2005, 64, 479–489. [Google Scholar] [CrossRef]
- Voronina, N.; Aichmuller, C.; Kolb, T.; Korshunov, A.; Ryzhova, M.; Barnholtz-Sloan, J.; Cioffi, G.; Sill, M.; von Deimling, A.; Pfister, S.M.; et al. The age of adult pilocytic astrocytoma cells. Oncogene 2021, 40, 2830–2841. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Burkhard, C.; Di Patre, P.L.; Schuler, D.; Schuler, G.; Yasargil, M.G.; Yonekawa, Y.; Lutolf, U.M.; Kleihues, P.; Ohgaki, H. A population-based study of the incidence and survival rates in patients with pilocytic astrocytoma. J. Neurosurg. 2003, 98, 1170–1174. [Google Scholar] [CrossRef]
- Bian, S.X.; McAleer, M.F.; Vats, T.S.; Mahajan, A.; Grosshans, D.R. Pilocytic astrocytoma with leptomeningeal dissemination. Childs Nerv. Syst. 2013, 29, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Bouffet, E.; Jakacki, R.; Goldman, S.; Hargrave, D.; Hawkins, C.; Shroff, M.; Hukin, J.; Bartels, U.; Foreman, N.; Kellie, S.; et al. Phase II study of weekly vinblastine in recurrent or refractory pediatric low-grade glioma. J. Clin. Oncol. 2012, 30, 1358–1363. [Google Scholar] [CrossRef] [PubMed]
- Komotar, R.J.; Mocco, J.; Carson, B.S.; Sughrue, M.E.; Zacharia, B.E.; Sisti, A.C.; Canoll, P.D.; Khandji, A.G.; Tihan, T.; Burger, P.C.; et al. Pilomyxoid astrocytoma: A review. MedGenMed 2004, 6, 42. [Google Scholar]
- Komotar, R.J.; Mocco, J.; Jones, J.E.; Zacharia, B.E.; Tihan, T.; Feldstein, N.A.; Anderson, R.C. Pilomyxoid astrocytoma: Diagnosis, prognosis, and management. Neurosurg. Focus 2005, 18, E7. [Google Scholar] [CrossRef] [PubMed]
- Koehler, J.W.; Miller, A.D.; Miller, C.R.; Porter, B.; Aldape, K.; Beck, J.; Brat, D.; Cornax, I.; Corps, K.; Frank, C.; et al. A Revised Diagnostic Classification of Canine Glioma: Towards Validation of the Canine Glioma Patient as a Naturally Occurring Preclinical Model for Human Glioma. J. Neuropathol. Exp. Neurol. 2018, 77, 1039–1054. [Google Scholar] [CrossRef] [PubMed]
- Jose-Lopez, R.; Gutierrez-Quintana, R.; de la Fuente, C.; Manzanilla, E.G.; Sunol, A.; Pi Castro, D.; Anor, S.; Sanchez-Masian, D.; Fernandez-Flores, F.; Ricci, E.; et al. Clinical features, diagnosis, and survival analysis of dogs with glioma. J. Vet. Intern Med. 2021, 35, 1902–1917. [Google Scholar] [CrossRef]
- Stoica, G.; Kim, H.T.; Hall, D.G.; Coates, J.R. Morphology, immunohistochemistry, and genetic alterations in dog astrocytomas. Vet. Pathol. 2004, 41, 10–19. [Google Scholar] [CrossRef]
- Keller, E.T.; Madewell, B.R. Locations and types of neoplasms in immature dogs: 69 cases (1964–1989). J. Am. Vet. Med. Assoc. 1992, 200, 1530–1532. [Google Scholar]
- Kube, S.A.; Bruyette, D.S.; Hanson, S.M. Astrocytomas in young dogs. J. Am. Anim. Hosp. Assoc. 2003, 39, 288–293. [Google Scholar] [CrossRef]
- Nelson, R.W.; Morrison, W.B.; Lurus, A.G.; Miller, J.B. Diencephalic syndrome secondary to intracranial astrocytoma in a dog. J. Am. Vet. Med. Assoc. 1981, 179, 1004–1010. [Google Scholar]
- Walmsley, G.L.; Chandler, K.; Davies, E.S.; Lamb, C.R.; Smyth, B.; Summers, B.A. Multi-focal cerebral oligoastrocytoma in a puppy. J. Small Anim. Pract. 2009, 50, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.; Glass, E.; DeLahunta, A.; Jackson, B. Intracranial anaplastic astrocytoma in a 19-week-old boxer dog. J. Small Anim. Pract. 2011, 52, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Theeler, B.J.; Ellezam, B.; Sadighi, Z.S.; Mehta, V.; Tran, M.D.; Adesina, A.M.; Bruner, J.M.; Puduvalli, V.K. Adult pilocytic astrocytomas: Clinical features and molecular analysis. Neuro Oncol. 2014, 16, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Collins, V.P.; Jones, D.T.; Giannini, C. Pilocytic astrocytoma: Pathology, molecular mechanisms and markers. Acta Neuropathol. 2015, 129, 775–788. [Google Scholar] [CrossRef]
- Matyja, E.; Grajkowska, W.; Stepien, K.; Naganska, E. Heterogeneity of histopathological presentation of pilocytic astrocytoma-diagnostic pitfalls. A review. Folia Neuropathol. 2016, 54, 197–211. [Google Scholar] [CrossRef]
- Wisner, E.R.; Dickinson, P.J.; Higgins, R.J. Magnetic resonance imaging features of canine intracranial neoplasia. Vet. Radiol. Ultrasound 2011, 52, S52–S61. [Google Scholar] [CrossRef]
- Young, B.D.; Levine, J.M.; Porter, B.F.; Chen-Allen, A.V.; Rossmeisl, J.H.; Platt, S.R.; Kent, M.; Fosgate, G.T.; Schatzberg, S.J. Magnetic resonance imaging features of intracranial astrocytomas and oligodendrogliomas in dogs. Vet. Radiol. Ultrasound 2011, 52, 132–141. [Google Scholar] [CrossRef]
- Malik, A.; Deb, P.; Sharma, M.C.; Sarkar, C. Neuropathological spectrum of pilocytic astrocytoma: An Indian series of 120 cases. Pathol Oncol. Res. 2006, 12, 164–171. [Google Scholar] [CrossRef]
- Lee, Y.Y.; Van Tassel, P.; Bruner, J.M.; Moser, R.P.; Share, J.C. Juvenile pilocytic astrocytomas: CT and MR characteristics. AJR Am. J. Roentgenol. 1989, 152, 1263–1270. [Google Scholar] [CrossRef]
- Kumar, A.J.; Leeds, N.E.; Kumar, V.A.; Fuller, G.N.; Lang, F.F.; Milas, Z.; Weinberg, J.S.; Ater, J.L.; Sawaya, R. Magnetic resonance imaging features of pilocytic astrocytoma of the brain mimicking high-grade gliomas. J. Comput. Assist. Tomogr. 2010, 34, 601–611. [Google Scholar] [CrossRef]
- Nakano, Y.; Yamamoto, J.; Takahashi, M.; Soejima, Y.; Akiba, D.; Kitagawa, T.; Ueta, K.; Miyaoka, R.; Umemura, T.; Nishizawa, S. Pilocytic astrocytoma presenting with atypical features on magnetic resonance imaging. J. Neuroradiol. 2015, 42, 278–282. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muller, K.; Kim, E.; Lebowitz, A.; Daverio, H. A High Grade Astrocytoma with Pilocytic Morphology in a 5-Month-Old American Bulldog. Vet. Sci. 2022, 9, 580. https://doi.org/10.3390/vetsci9100580
Muller K, Kim E, Lebowitz A, Daverio H. A High Grade Astrocytoma with Pilocytic Morphology in a 5-Month-Old American Bulldog. Veterinary Sciences. 2022; 9(10):580. https://doi.org/10.3390/vetsci9100580
Chicago/Turabian StyleMuller, Kelly, Eunbee Kim, Abbie Lebowitz, and Heather Daverio. 2022. "A High Grade Astrocytoma with Pilocytic Morphology in a 5-Month-Old American Bulldog" Veterinary Sciences 9, no. 10: 580. https://doi.org/10.3390/vetsci9100580
APA StyleMuller, K., Kim, E., Lebowitz, A., & Daverio, H. (2022). A High Grade Astrocytoma with Pilocytic Morphology in a 5-Month-Old American Bulldog. Veterinary Sciences, 9(10), 580. https://doi.org/10.3390/vetsci9100580