
Effectiveness of a Nanohydroxyapatite-Based Hydrogel on Alveolar Bone Regeneration in Post-Extraction Sockets of Dogs with Naturally Occurring Periodontitis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal and Sample Selection
2.2. Preparation of Nanohydroxyapatite-Based Hydrogel (HAP Hydrogel)
2.3. The Characteristics of HAP hydrogel and Immersion Results in Simulated Body Fluid (SBF)
2.4. Post-Extraction Socket Preservation with HAP Hydrogel
2.5. Intra-Oral Dental Radiography
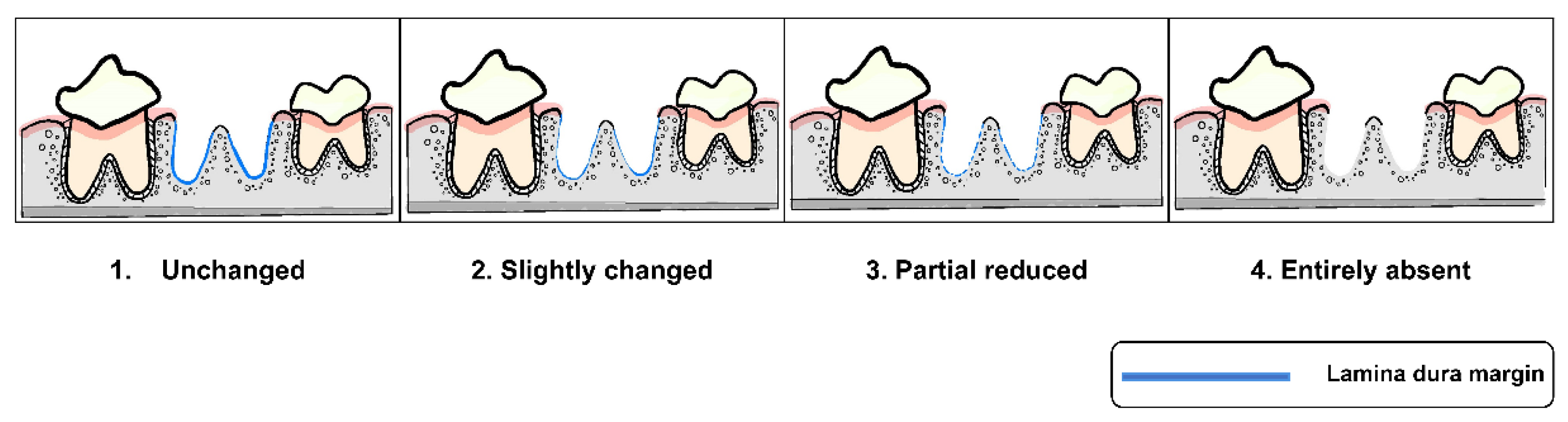
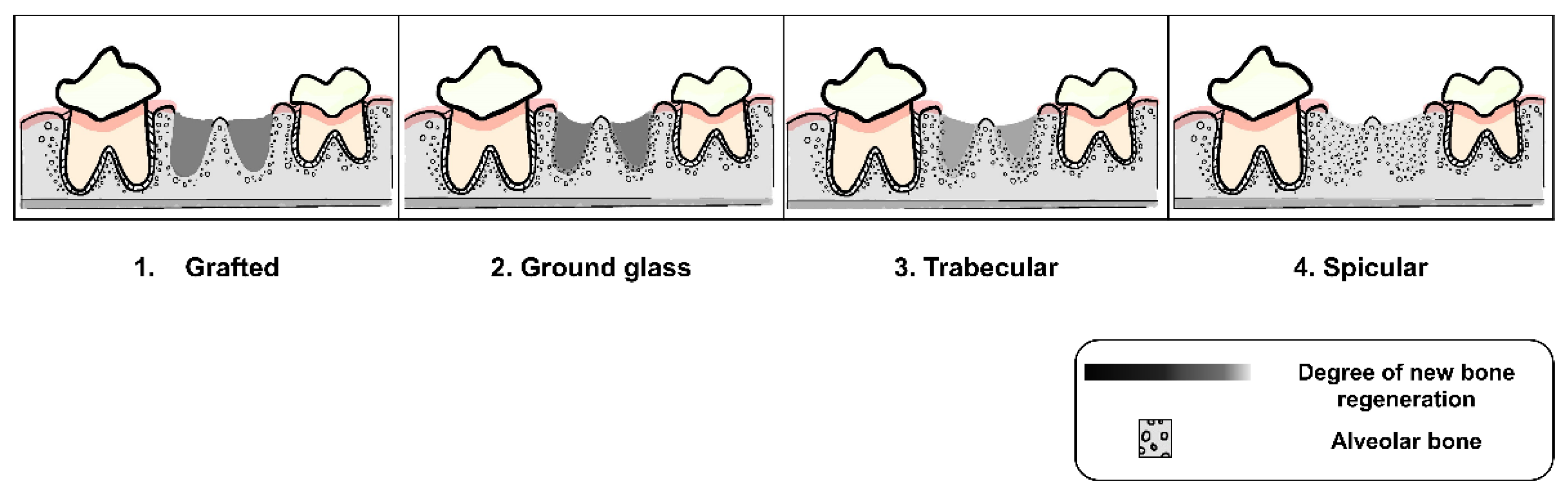
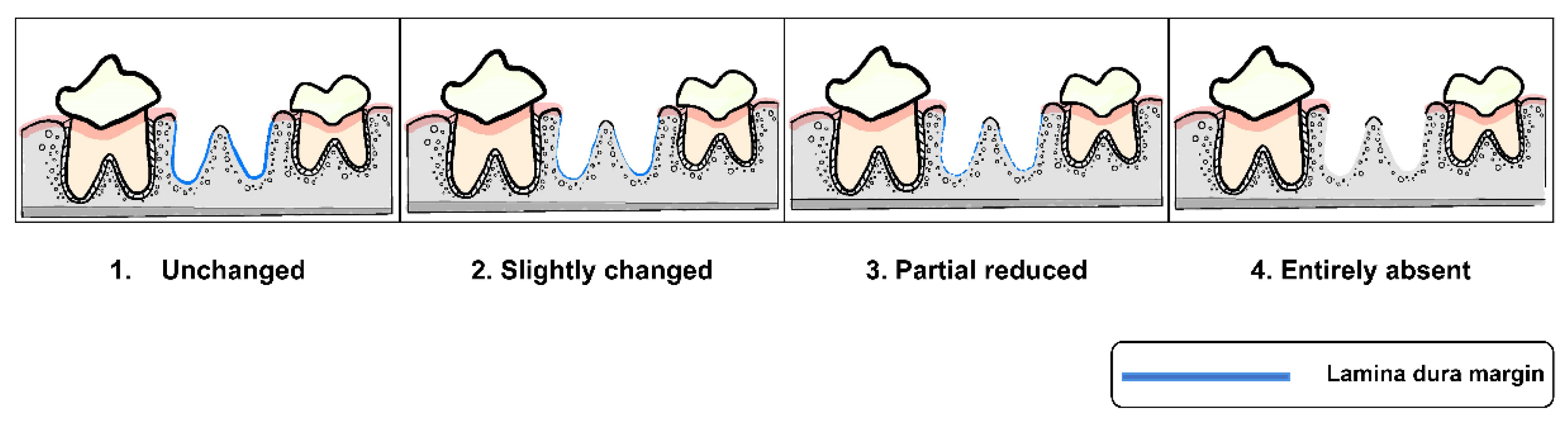
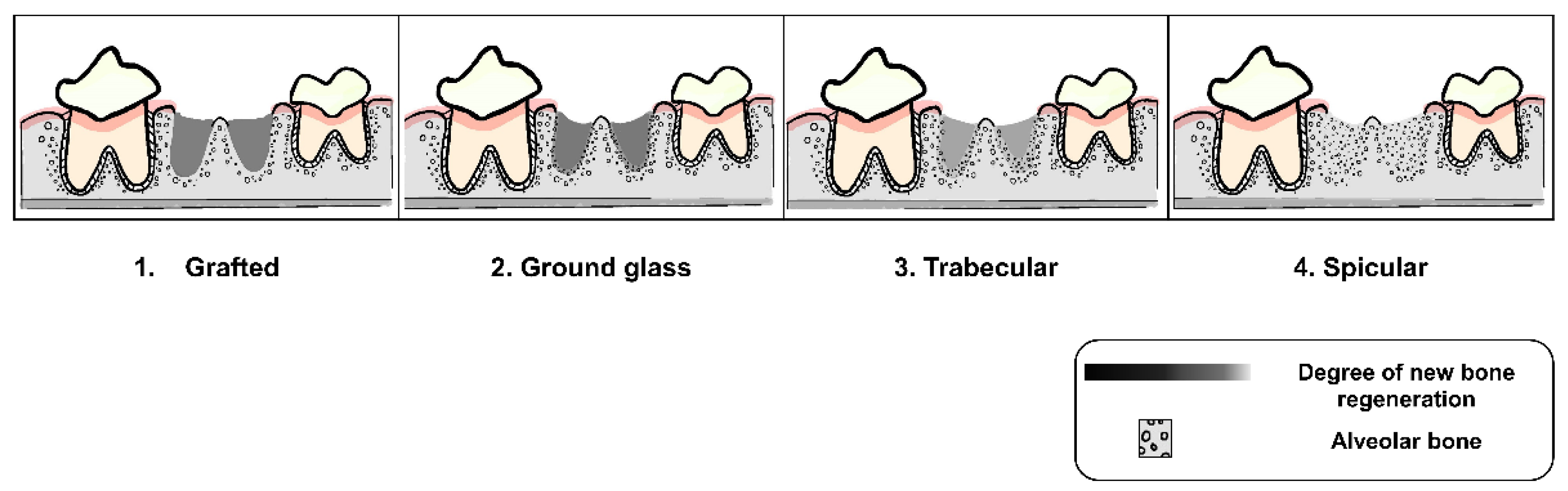
2.6. Radiographic Evaluation and Grading
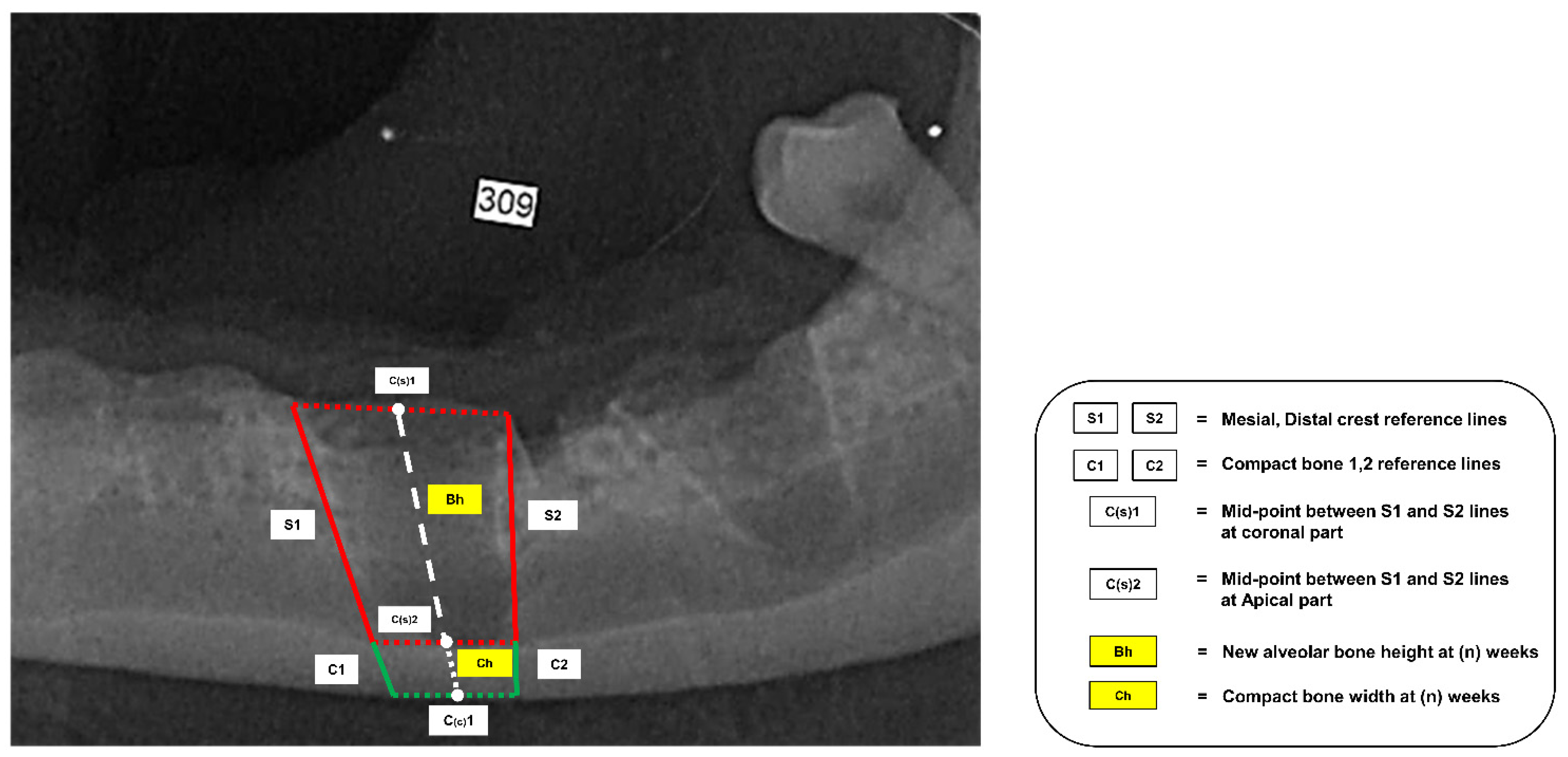
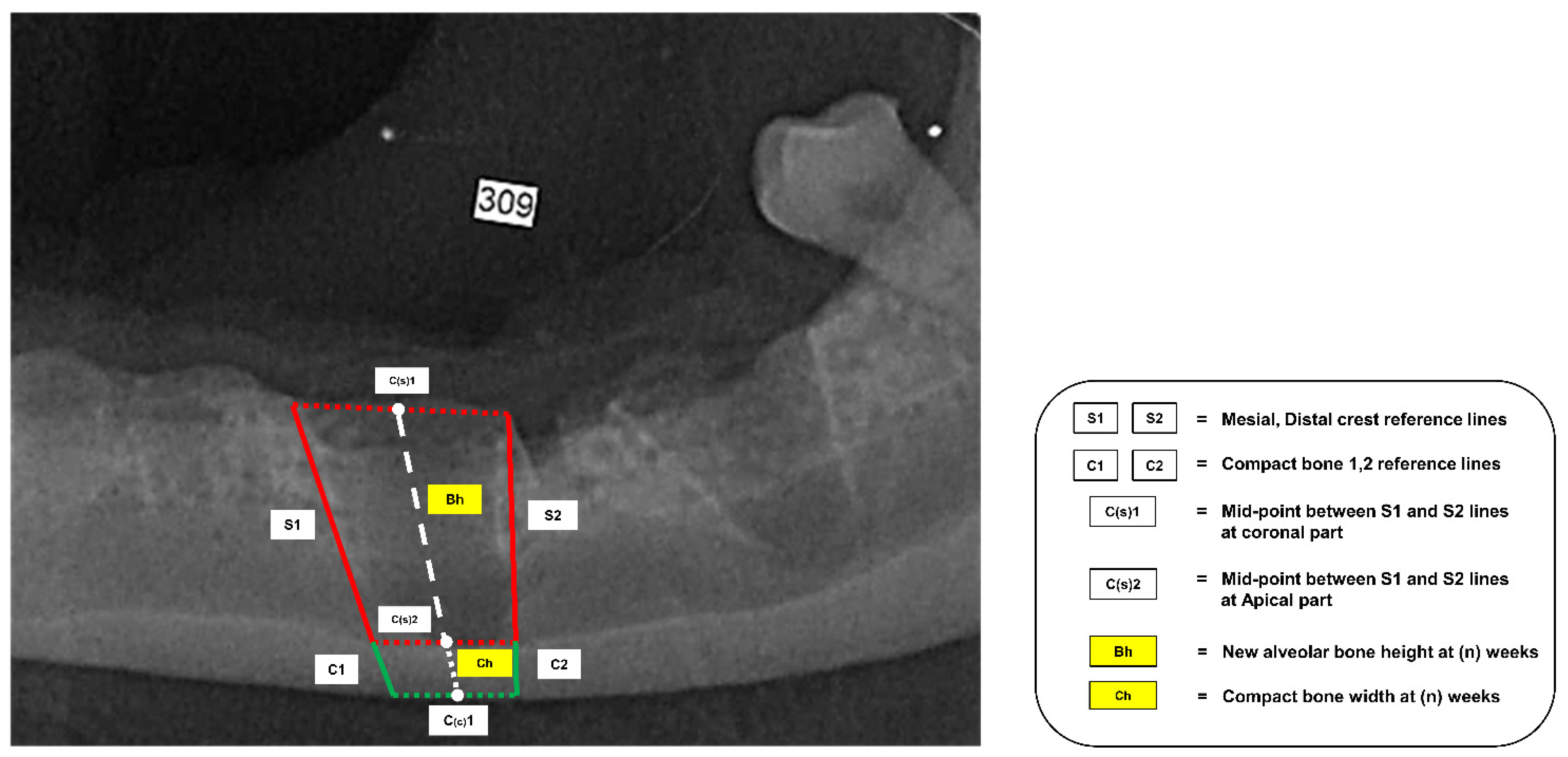
2.7. New Alveolar Bone Height Measurement
2.8. Alveolar Bone Density Analysis
2.9. Statistical Analysis
3. Results
3.1. Animals
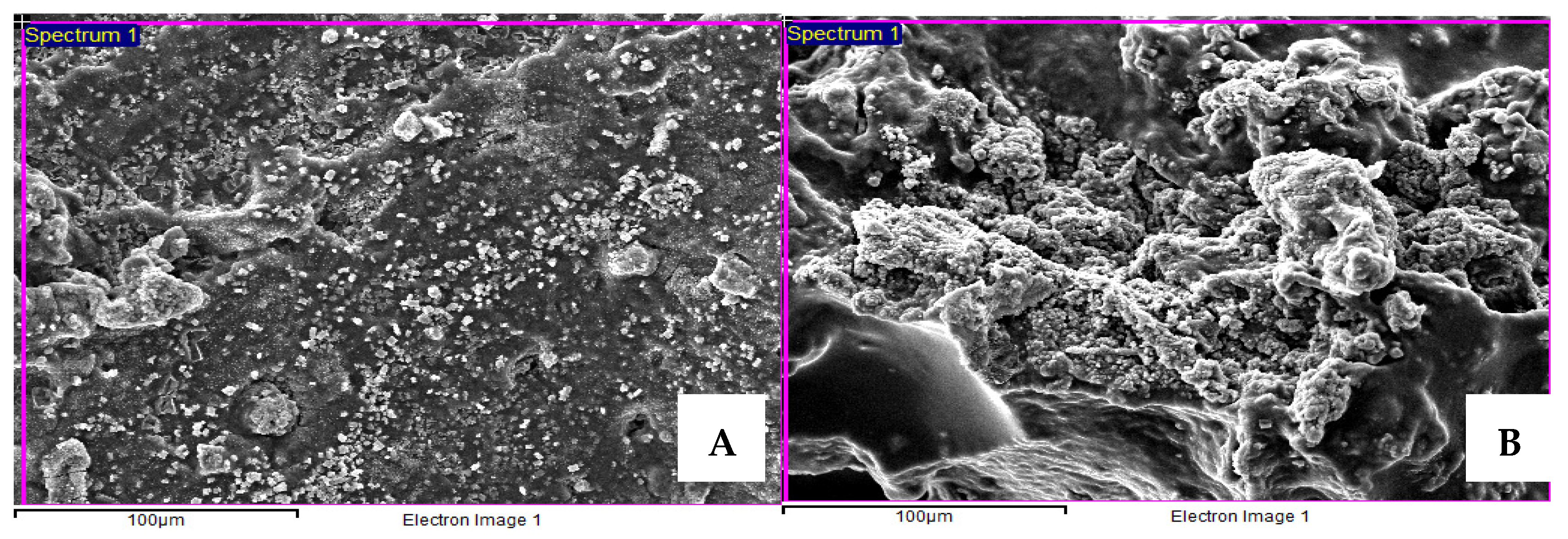
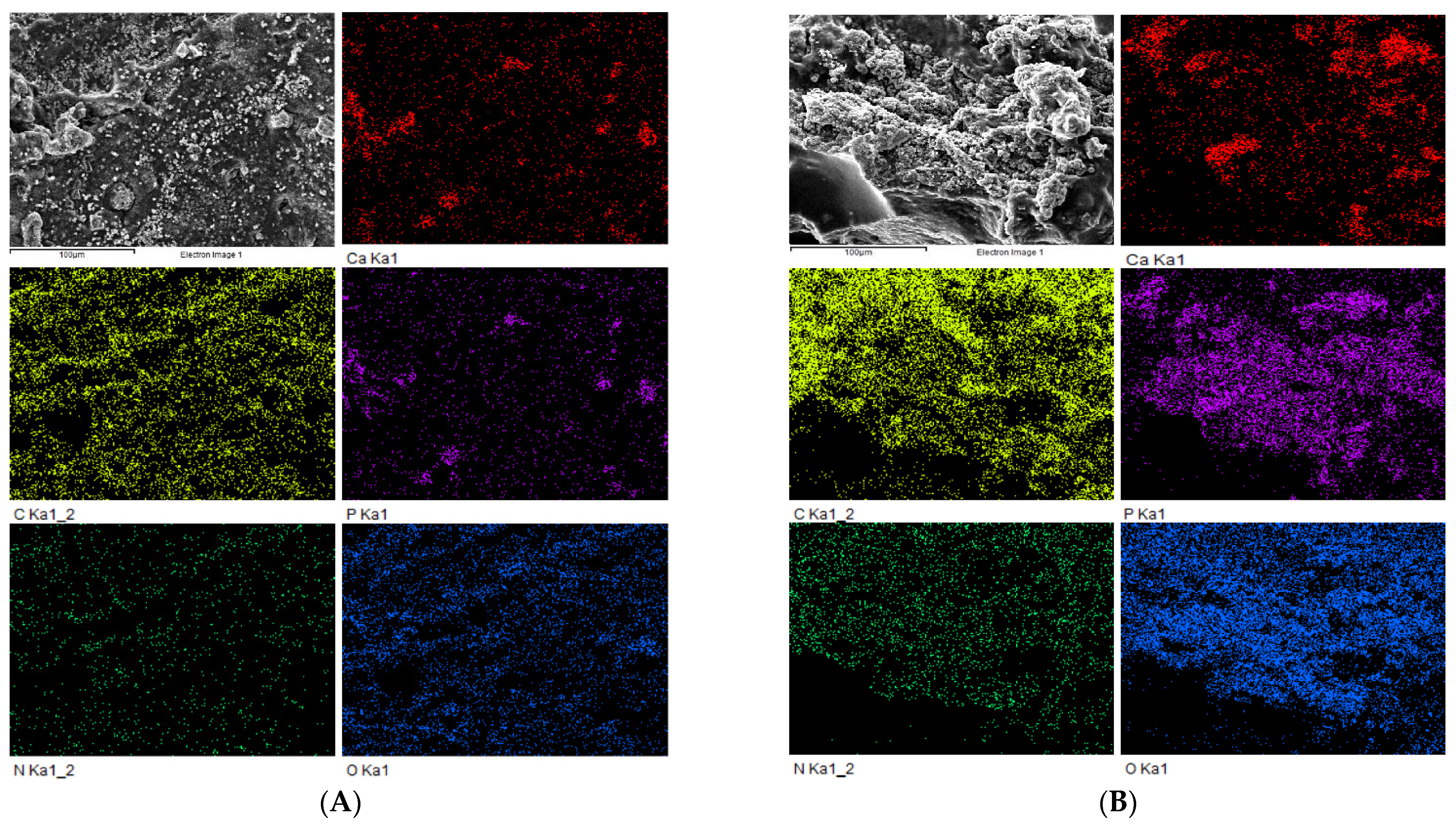
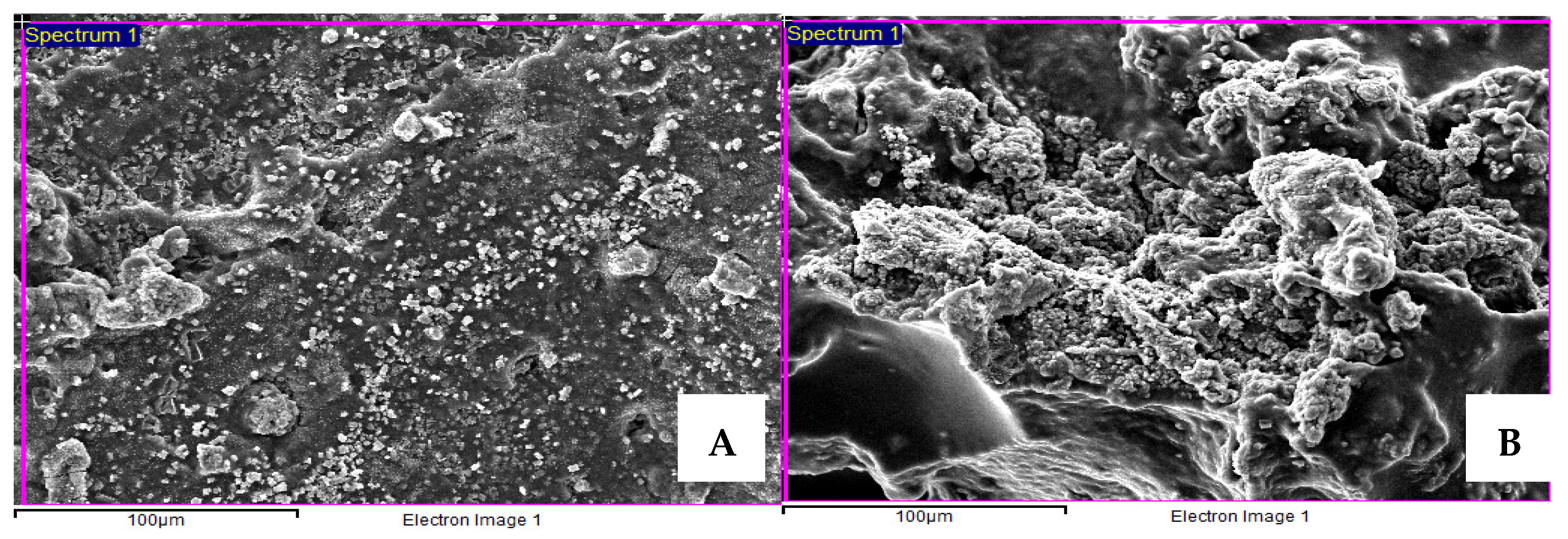
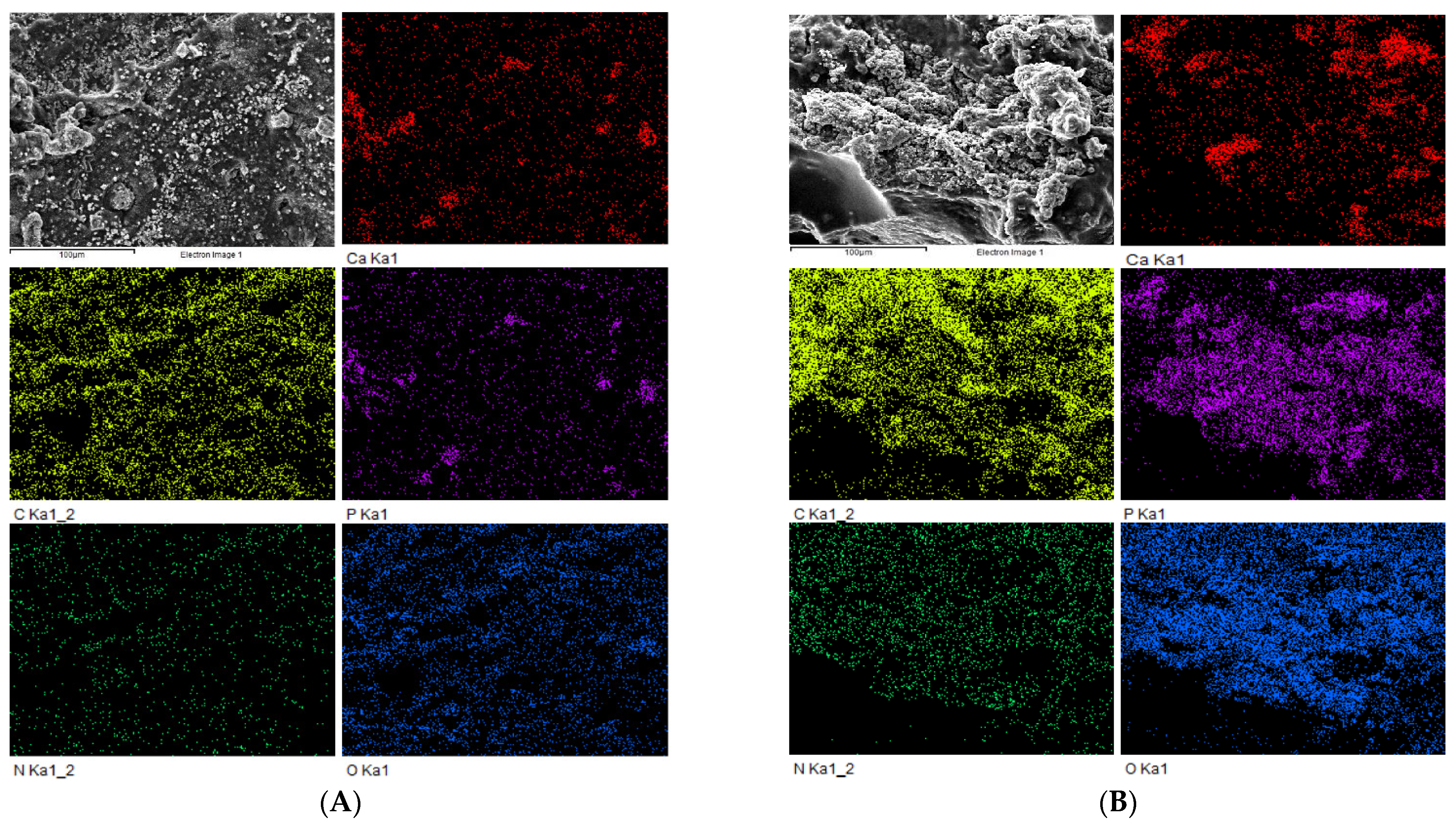
3.2. Scanning Electron Microscopy (SEM) and EDS Mapping Analysis of Nanohydroxyapatite-Based Hydrogel and Immersion Results in Simulated Body Fluid (SBF) for 14 Days
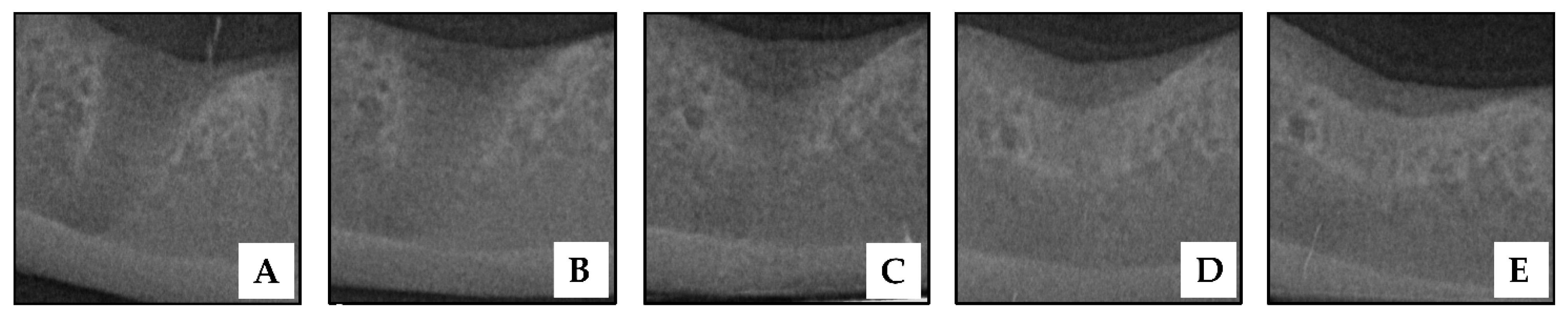
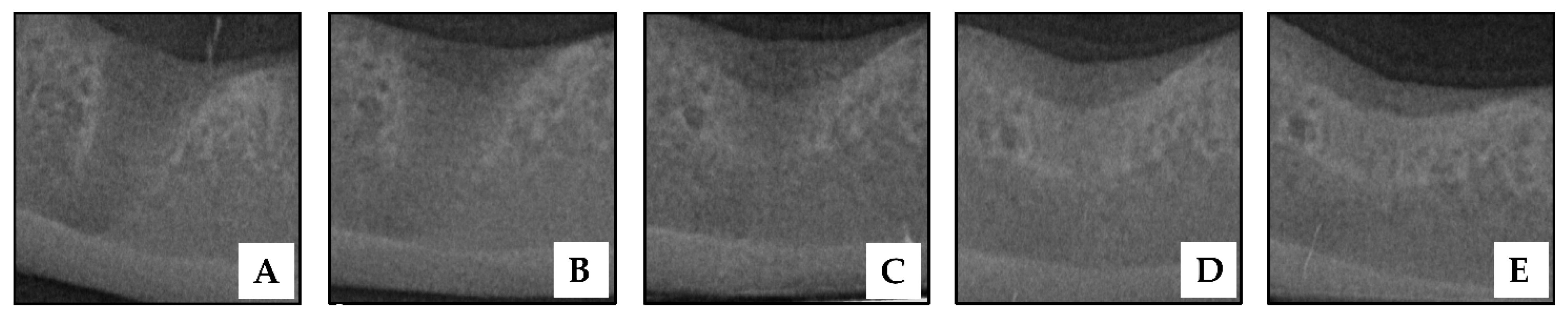
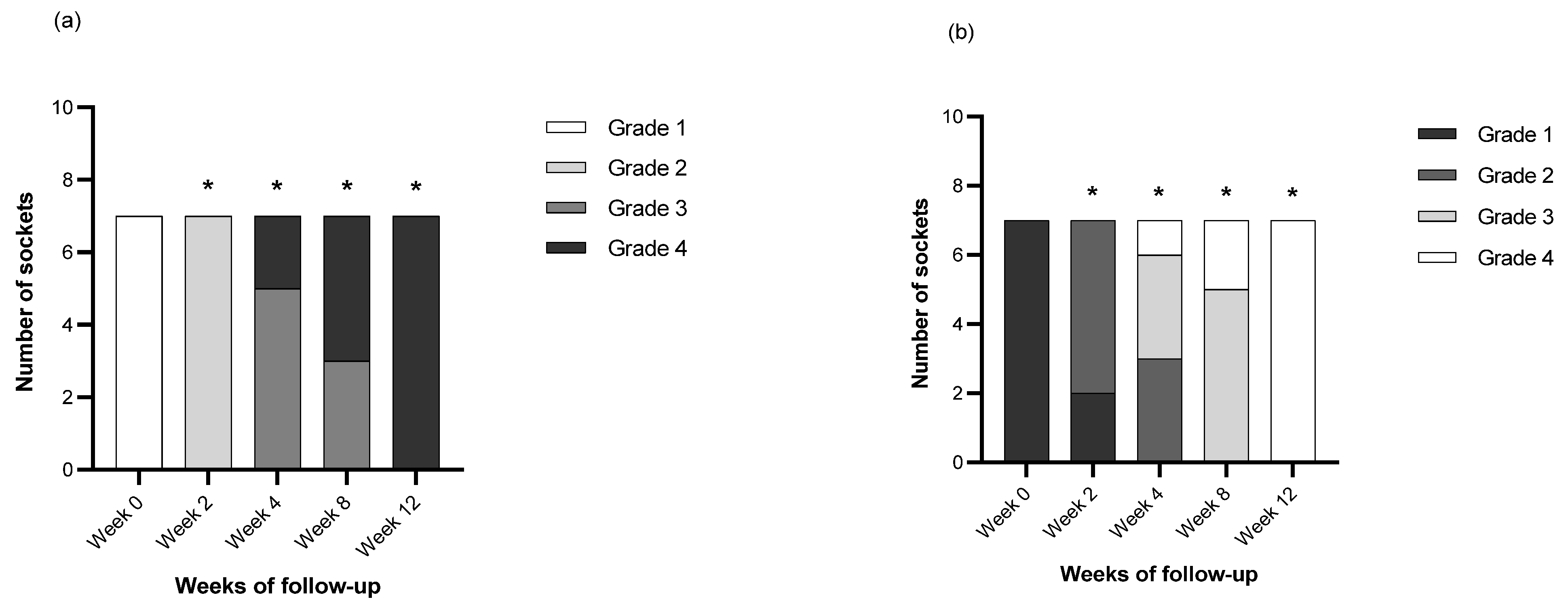
3.3. Radiographic Findings and Grading of Post-Extraction Socket Preservation with HAP Hydrogel
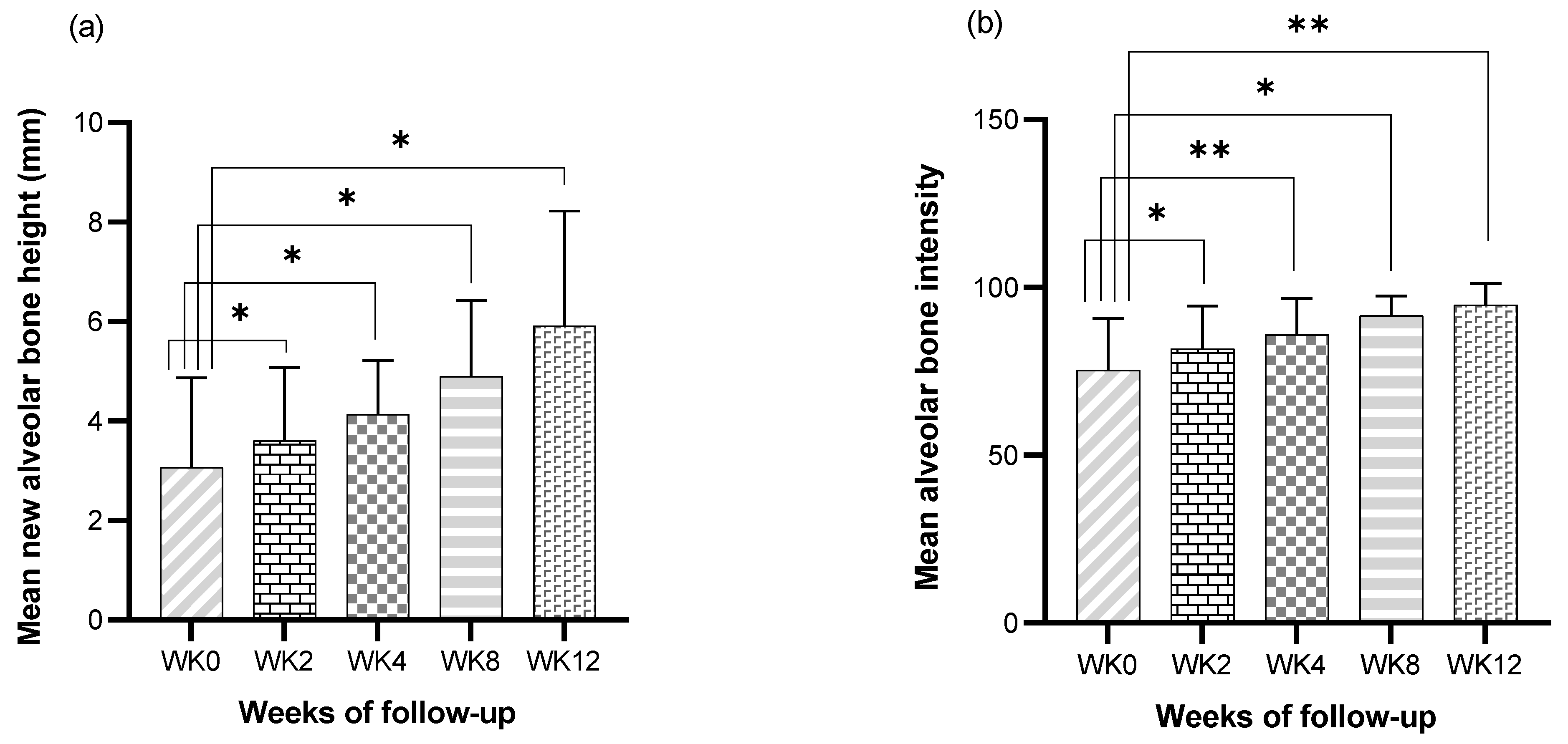
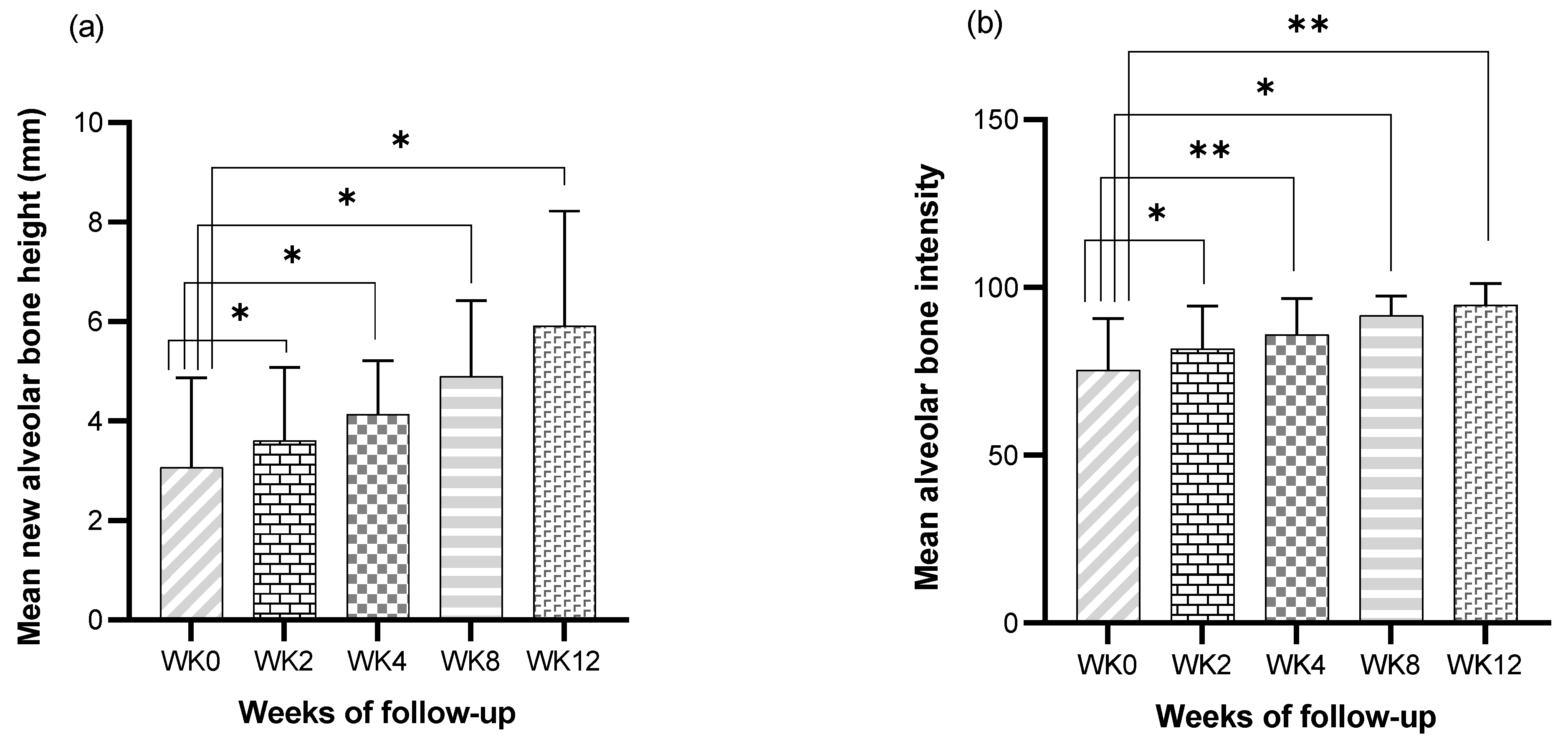
3.4. Bone Height Analysis of Post Extraction Socket Preservation with HAP Hydrogel
3.5. Bone Regeneration Analysis of Post-Extraction Socket Preservation with HAP Hydrogel

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | 2nd Weeks | 4th Weeks | 8th Weeks | 12th Weeks |
|---|---|---|---|---|
| Av.Bh (mm) | 3.61 ± 1.47 | 4.14 ± 1.06 | 4.90 ± 1.51 | 5.92 ± 2.30 |
| Av.BI | 81.68 ± 12.70 | 85.91 ± 10.83 | 91.74 ± 5.63 | 94.77 ± 6.41 |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wahl, D.A.; Czernuszka, J.T. Collagen-hydroxyapatite composites for hard tissue repair. Eur. Cell Mater. 2006, 11, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, N.A.; Borges, A.P.B.; Reis, E.C.C.; Sepúlveda, R.V.; Pontes, K.C.D.S. Prevalence of periodontal disease in dogs and owners’ level of awareness—A prospective clinical trial. Revista Ceres 2012, 59, 446–451. [Google Scholar] [CrossRef]
- Stella, J.L.; Bauer, A.E.; Croney, C.C. A cross-sectional study to estimate prevalence of periodontal disease in a population of dogs (Canis familiaris) in commercial breeding facilities in Indiana and Illinois. PLoS ONE 2018, 13, e0191395. [Google Scholar] [CrossRef] [PubMed]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol. 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [Green Version]
- Jayakumar, A.; Rohini, S.; Naveen, A.; Haritha, A.; Reddy, K. Horizontal alveolar bone loss: A periodontal orphan. J. Indian Soc. Periodontol. 2010, 14, 181–185. [Google Scholar] [CrossRef]
- Lopes, F.M.; Gioso, M.A.; Ferro, D.G.; Leon-Roman, M.A.; Venturini, M.A.; Correa, H.L. Oral fractures in dogs of Brazil—A retrospective study. J. Vet. Dent. 2005, 22, 86–90. [Google Scholar] [CrossRef]
- Kitshoff, A.M.; de Rooster, H.; Ferreira, S.M.; Steenkamp, G. A retrospective study of 109 dogs with mandibular fractures. Vet. Comp. Orthop. Traumatol. 2013, 26, 1–5. [Google Scholar] [CrossRef]
- Niemiec, B.A. Periodontal disease. Top. Companion Anim. Med. 2008, 23, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Scherer, E.; Hetzel, S.; Snyder, C.J. Assessment of the Role of the Mandibular First Molar Tooth in Mandibular Fracture Patterns of 29 Dogs. J. Vet. Dent. 2019, 36, 32–39. [Google Scholar] [CrossRef]
- Kyllar, M.; Witter, K. Prevalence of dental disorders in pet dogs. Vet. Med. 2012, 50, 496–505. [Google Scholar] [CrossRef] [Green Version]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone Healing and Soft Tissue Contour Changes Following Single-Tooth Extraction: A Clinical and Radiographic 12-Month Prospective Study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Hansson, S.; Halldin, A. Alveolar ridge resorption after tooth extraction: A consequence of a fundamental principle of bone physiology. J. Dent. Biomech. 2012, 3, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, D.J.; Deshpande, N.C.; Dave, D.H.; Narayankar, S.D. A comparative evaluation of extraction socket preservation with demineralized freeze-dried bone allograft alone and along with platelet-rich fibrin: A clinical and radiographic study. Contemp. Clin. Dent. 2016, 7, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Cardaropoli, D.; Tamagnone, L.; Roffredo, A.; Gaveglio, L.; Cardaropoli, G. Socket preservation using bovine bone mineral and collagen membrane: A randomized controlled clinical trial with histologic analysis. Int. J. Periodontics Restor. Dent. 2012, 32, 421–430. [Google Scholar]
- ELkarargy, A. Alveolar Sockets Preservation Using Hydroxyapatite/Beta tricalcium Phosphate with Hyaluronic Acid (Histomorphometric study). J. Am. Sci. 2013, 9, 556–563. [Google Scholar]
- Roveri, N.; Iafisco, M. Evolving application of biomimetic nanostructured hydroxyapatite. Nanotechnol. Sci. Appl. 2010, 3, 107–125. [Google Scholar] [CrossRef] [Green Version]
- Qiao, B.; Li, J.; Zhu, Q.; Guo, S.; Qi, X.; Li, W.; Wu, J.; Liu, Y.; Jiang, D. Bone plate composed of a ternary nano-hydroxyapatite/polyamide 66/glass fiber composite: Biomechanical properties and biocompatibility. Int. J. Nanomed. 2014, 9, 1423–1432. [Google Scholar] [CrossRef] [Green Version]
- Dumbleton, J.; Manley, M.T. Hydroxyapatite-Coated Prostheses in Total Hip and Knee Arthroplasty. J. Bone Joint Surg. Am. 2004, 86, 2536–2539. [Google Scholar] [CrossRef]
- Byun, S.H.; Lim, H.K.; Kim, S.M.; Lee, S.M.; Kim, H.E.; Lee, J.H. The Bioresorption and Guided Bone Regeneration of Absorbable Hydroxyapatite-Coated Magnesium Mesh. J. Craniofac. Surg. 2017, 28, 518–523. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, C.; Chen, Q.; Liu, H.; Deng, C.; Ling, P.; Cui, F.Z. Effects of the bilayer nano-hydroxyapatite/mineralized collagen-guided bone regeneration membrane on site preservation in dogs. J. Biomater. Appl. 2017, 32, 242–256. [Google Scholar] [CrossRef]
- Yousefi, A.-M.; Oudadesse, H.; Akbarzadeh, R.; Wers, E.; Lucas-Girot, A. Physical and biological characteristics of nanohydroxyapatite and bioactive glasses used for bone tissue engineering. Nanotechnol. Rev. 2014, 3, 527–552. [Google Scholar] [CrossRef]
- Sadat-Shojai, M.; Khorasani, M.T.; Dinpanah-Khoshdargi, E.; Jamshidi, A. Synthesis methods for nanosized hydroxyapatite with diverse structures. Acta Biomater. 2013, 9, 7591–7621. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, E.M. Hydrogel: Preparation, characterization, and applications: A review. J. Adv. Res. 2015, 6, 105–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoare, T.R.; Kohane, D.S. Hydrogels in drug delivery: Progress and challenges. Polymer 2008, 49, 1993–2007. [Google Scholar] [CrossRef] [Green Version]
- Ferraz, M.; Monteiro, F.; Manuel, C. Hydroxyapatite nanoparticles: A review of preparation methodologies. J. Appl. Biomater. Biomech. 2004, 2, 74–80. [Google Scholar]
- Seo, B.-M.; Miura, M.; Gronthos, S.; Mark Bartold, P.; Batouli, S.; Brahim, J.; Young, M.; Gehron Robey, P.; Wang, C.Y.; Shi, S. Investigation of multipotent postnatal stem cells from human periodontal ligament. Lancet 2004, 364, 149–155. [Google Scholar] [CrossRef]
- Lee, K.Y.; Mooney, D.J. Hydrogels for Tissue Engineering. Chem. Rev. 2001, 101, 1869–1880. [Google Scholar] [CrossRef] [PubMed]
- Drury, J.L.; Mooney, D.J. Hydrogels for tissue engineering: Scaffold design variables and applications. Biomaterials 2003, 24, 4337–4351. [Google Scholar] [CrossRef]
- Gibbs, D.M.; Black, C.R.; Dawson, J.I.; Oreffo, R.O. A review of hydrogel use in fracture healing and bone regeneration. J. Tissue Eng. Regen. Med. 2016, 10, 187–198. [Google Scholar] [CrossRef]
- Bai, X.; Gao, M.; Syed, S.; Zhuang, J.; Xu, X.; Zhang, X.Q. Bioactive hydrogels for bone regeneration. Bioact. Mater. 2018, 3, 401–417. [Google Scholar] [CrossRef]
- Cardaropoli, G.; Araujo, M.; Hayacibara, R.; Sukekava, F.; Lindhe, J. Healing of extraction sockets and surgically produced-augmented and non-augmented—Defects in the alveolar ridge. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 435–440. [Google Scholar] [CrossRef]
- Ho, K.N.; Salamanca, E.; Chang, K.C.; Shih, T.C.; Chang, Y.C.; Huang, H.M.; Teng, N.C.; Lin, C.T.; Feng, S.W.; Chang, W.J. A Novel HA/beta-TCP-Collagen Composite Enhanced New Bone Formation for Dental Extraction Socket Preservation in Beagle Dogs. Materials 2016, 9, 191. [Google Scholar] [CrossRef] [Green Version]
- Lamkhao, S.; Phaya, M.; Jansakun, C.; Chandet, N.; Thongkorn, K.; Rujijanagul, G.; Bangrak, P.; Randorn, C. Synthesis of Hydroxyapatite with Antibacterial Properties Using a Microwave-Assisted Combustion Method. Sci. Rep. 2019, 9, 4015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokubo, T.; Takadama, H. How useful is SBF in predicting in vivo bone bioactivity? Biomaterials 2006, 27, 2907–2915. [Google Scholar] [CrossRef] [PubMed]
- Gorrel, C.; Andersson, S.; Verhaert, L. Dental radiography. In Veterinary Dentistry for the General Practitioner, 2nd ed.; Elsevier Saunders: Edinburgh, Scotland, 2013; pp. 67–80. [Google Scholar]
- Haghighat, A.; Hekmatian, E.; Abdinian, M.; Sadeghkhani, E. Radiographic Evaluation of Bone Formation and Density Changes after Mandibular Third Molar Extraction: A 6 Month Follow up. Dent. Res. J. 2010, 8, 1–5. [Google Scholar]
- Silva, A.M.; Astolphi, R.D.; Perri, S.H.; Koivisto, M.B. Filling of extraction sockets of feline maxillary canine teeth with autogenous bone or bioactive glass. Acta Cir. Bras. 2013, 28, 856–862. [Google Scholar] [CrossRef] [Green Version]
- Tambella, A.M.; Bartocetti, F.; Rossi, G.; Galosi, L.; Catone, G.; Falcone, A.; Vullo, C. Effects of Autologous Platelet-Rich Fibrin in Post-Extraction Alveolar Sockets: A Randomized, Controlled Split-Mouth Trial in Dogs with Spontaneous Periodontal Disease. Animals 2020, 10, 1343. [Google Scholar] [CrossRef]
- Liu, X.; Chen, Y.; Huang, Q.; He, W.; Feng, Q.; Yu, B. A novel thermo-sensitive hydrogel based on thiolated chitosan/hydroxyapatite/beta-glycerophosphate. Carbohydr. Polym. 2014, 110, 62–69. [Google Scholar] [CrossRef]
- Pan, Y.; Zhao, Y.; Kuang, R.; Liu, H.; Sun, D.; Mao, T.; Jiang, K.; Yang, X.; Watanabe, N.; Mayo, K.H.; et al. Injectable hydrogel-loaded nano-hydroxyapatite that improves bone regeneration and alveolar ridge promotion. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 116, 111158. [Google Scholar] [CrossRef]
- Kandow, C.E.; Georges, P.C.; Janmey, P.A.; Beningo, K.A. Polyacrylamide Hydrogels for Cell Mechanics: Steps Toward Optimization and Alternative Uses. Cell Mech. 2007, 83, 29–46. [Google Scholar] [CrossRef]
- Fang, J.; Li, P.; Lu, X.; Fang, L.; Lu, X.; Ren, F. A strong, tough, and osteoconductive hydroxyapatite mineralized polyacrylamide/dextran hydrogel for bone tissue regeneration. Acta Biomater. 2019, 88, 503–513. [Google Scholar] [CrossRef]
- Prakash, N.; Karjodkar, F.R.; Sansare, K.; Sonawane, H.V.; Bansal, N.; Arwade, R. Visibility of lamina dura and periodontal space on periapical radiographs and its comparison with cone beam computed tomography. Contemp. Clin. Dent. 2015, 6, 21–25. [Google Scholar] [CrossRef]
- Gupta, A.; Rattan, V.; Rai, S. Efficacy of Chitosan in promoting wound healing in extraction socket: A prospective study. J. Oral Biol. Craniofacial Res. 2019, 9, 91–95. [Google Scholar] [CrossRef]
- Pagni, G.; Pellegrini, G.; Giannobile, W.V.; Rasperini, G. Postextraction alveolar ridge preservation: Biological basis and treatments. Int. J. Dent. 2012, 2012, 151030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelhamid, A. Alveolar Bone Preservation. Biological Basis and Techniques. Int. J. Dent. Sci. Res. 2017, 5, 56–58. [Google Scholar] [CrossRef]
- Lee, J.S.; Cha, J.K.; Kim, C.S. Alveolar ridge regeneration of damaged extraction sockets using deproteinized porcine versus bovine bone minerals: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2018, 20, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Mangos, J.F. The healing of extraction wounds. An experimental study based on microscopic and radiographic investigations. NZ Dent. J. 1941, 37, 4–24. [Google Scholar]
- Discepoli, N.; Vignoletti, F.; Laino, L.; de Sanctis, M.; Munoz, F.; Sanz, M. Early healing of the alveolar process after tooth extraction: An experimental study in the beagle dog. J. Clin. Periodontol. 2013, 40, 638–644. [Google Scholar] [CrossRef]
- Kattimani, V.S.; Chakravarthi, P.S.; Kanumuru, N.R.; Subbarao, V.V.; Sidharthan, A.; Kumar, T.S.; Prasad, L.K. Eggshell Derived Hydroxyapatite as Bone Graft Substitute in the Healing of Maxillary Cystic Bone Defects: A Preliminary Report. J. Int. Oral Health 2014, 6, 15–19. [Google Scholar]
- Lee, J.S.; Park, W.Y.; Cha, J.K.; Jung, U.W.; Kim, C.S.; Lee, Y.K.; Choi, S.H. Periodontal tissue reaction to customized nano-hydroxyapatite block scaffold in one-wall intrabony defect: A histologic study in dogs. J. Periodontal Implant Sci. 2012, 42, 50–58. [Google Scholar] [CrossRef]
- Wang, Y.F.; Wang, C.Y.; Wan, P.; Wang, S.G.; Wang, X.M. Comparison of bone regeneration in alveolar bone of dogs on mineralized collagen grafts with two composition ratios of nano-hydroxyapatite and collagen. Regen. Biomater. 2016, 3, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.J.; Kim, S.E.; Han, T.S.; Son, J.S.; Kang, S.S.; Choi, S.H. Bone Regeneration of Hydroxyapatite with Granular Form or Porous Scaffold in Canine Alveolar Sockets. Vivo 2017, 31, 335–341. [Google Scholar] [CrossRef]
- Araujo, M.G.; Lindhe, J. Ridge preservation with the use of Bio-Oss collagen: A 6-month study in the dog. Clin. Oral Implants Res. 2009, 20, 433–440. [Google Scholar] [CrossRef]
- Kim, J.H.; Koo, K.T.; Capetillo, J.; Kim, J.J.; Yoo, J.M.; Ben Amara, H.; Park, J.C.; Schwarz, F.; Wikesjo, U.M.E. Periodontal and endodontic pathology delays extraction socket healing in a canine model. J. Periodontal Implant Sci. 2017, 47, 143–153. [Google Scholar] [CrossRef] [Green Version]
- Bauer, T.; Muschler, G. Bone graft materials. An overview of the basic science. Clin. Orthop. Relat. Res. 2000, 371, 10–27. [Google Scholar] [CrossRef]
- Kattimani, V.S.; Kondaka, S.; Lingamaneni, K.P. Hydroxyapatite—Past, Present, and Future in Bone Regeneration. Bone Tissue Regen. Insights 2016, 7, BTRI-S36138. [Google Scholar] [CrossRef] [Green Version]
- Merrett, K.; Cornelius, R.M.; McClung, W.G.; Unsworth, L.D.; Sheardown, H. Surface analysis methods for characterizing polymeric biomaterials. J. Biomater. Sci. Polym. Ed. 2002, 13, 593–621. [Google Scholar] [CrossRef] [PubMed]
- Kokubo, T.; Takadama, H. Simulated Body Fluid (SBF) as a Standard Tool to Test the Bioactivity of Implants. In Handbook of Biomineralization: Biological Aspects and Structure Formation; Bauerlein, E., Ed.; Wiley-VCH Verlag GmbH: Weinheim, Germany, 2008; pp. 97–109. [Google Scholar]
- Roza, M.R.; Silva, L.A.; Barriviera, M.; Januario, A.L.; Bezerra, A.C.; Fioravanti, M.C. Cone beam computed tomography and intraoral radiography for diagnosis of dental abnormalities in dogs and cats. J. Vet. Sci. 2011, 12, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Del Pozo, J.L.; Patel, R. Clinical practice. Infection associated with prosthetic joints. N. Engl. J. Med. 2009, 361, 787–794. [Google Scholar] [CrossRef] [Green Version]
- Camps-Font, O.; Figueiredo, R.; Valmaseda-Castellon, E.; Gay-Escoda, C. Postoperative Infections After Dental Implant Placement: Prevalence, Clinical Features, and Treatment. Implant Dent. 2015, 24, 713–719. [Google Scholar] [CrossRef] [Green Version]
- Arciola, C.R.; Campoccia, D.; Montanaro, L. Implant infections: Adhesion, biofilm formation and immune evasion. Nat. Rev. Microbiol. 2018, 16, 397–409. [Google Scholar] [CrossRef] [PubMed]
- Costa-Pinto, A.R.; Lemos, A.L.; Tavaria, F.K.; Pintado, M. Chitosan and Hydroxyapatite Based Biomaterials to Circumvent Periprosthetic Joint Infections. Materials 2021, 14, 804. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Maiorani, C.; Preda, C.; Chiesa, A.; Esposito, F.; Pascadopoli, M.; Scribante, A. Management of Gingival Bleeding in Periodontal Patients with Domiciliary Use of Toothpastes Containing Hyaluronic Acid, Lactoferrin, or Paraprobiotics: A Randomized Controlled Clinical Trial. Appl. Sci. 2021, 11, 8586. [Google Scholar] [CrossRef]

| Age (Years) | 11 (8–15) |
| Sex | 4 Male, 1 Female |
| (2 intact male, 2 neuter male, 1 neuter female) | |
| Breeds | Poodle (2/5) |
| Shih Tzu (1/5) | |
| Pomeranian (1/5) | |
| Chihuahua (1/5) | |
| Body weight | 4.2 (3.55–9.8) |
| Periodontal stages | Grade 1 (0/5) |
| Grade 2 (0/5) | |
| Grade 3 (2/5) | |
| Grade 4 (3/5) | |
| Concurrent Diseases | Hepatobiliary problem (1/5) |
| Myxomatous mitral valve degeneration (1/5) | |
| Unremarkable (3/5) |
| Follow-Up Weeks | p-Value | |
|---|---|---|
| Criteria A | Criteria B | |
| Week 2 | 0.010 | 0.036 |
| Week 4 | 0.017 | 0.020 |
| Week 8 | 0.019 | 0.017 |
| Week 12 | 0.010 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanongpitchayes, K.; Randorn, C.; Lamkhao, S.; Chokethawai, K.; Rujijanagul, G.; Na Lampang, K.; Somrup, L.; Boonyapakorn, C.; Thongkorn, K. Effectiveness of a Nanohydroxyapatite-Based Hydrogel on Alveolar Bone Regeneration in Post-Extraction Sockets of Dogs with Naturally Occurring Periodontitis. Vet. Sci. 2022, 9, 7. https://doi.org/10.3390/vetsci9010007
Tanongpitchayes K, Randorn C, Lamkhao S, Chokethawai K, Rujijanagul G, Na Lampang K, Somrup L, Boonyapakorn C, Thongkorn K. Effectiveness of a Nanohydroxyapatite-Based Hydrogel on Alveolar Bone Regeneration in Post-Extraction Sockets of Dogs with Naturally Occurring Periodontitis. Veterinary Sciences. 2022; 9(1):7. https://doi.org/10.3390/vetsci9010007
Chicago/Turabian StyleTanongpitchayes, Kittidaj, Chamnan Randorn, Suphatchaya Lamkhao, Komsanti Chokethawai, Gobwute Rujijanagul, Kannika Na Lampang, Luddawon Somrup, Chavalit Boonyapakorn, and Kriangkrai Thongkorn. 2022. "Effectiveness of a Nanohydroxyapatite-Based Hydrogel on Alveolar Bone Regeneration in Post-Extraction Sockets of Dogs with Naturally Occurring Periodontitis" Veterinary Sciences 9, no. 1: 7. https://doi.org/10.3390/vetsci9010007
APA StyleTanongpitchayes, K., Randorn, C., Lamkhao, S., Chokethawai, K., Rujijanagul, G., Na Lampang, K., Somrup, L., Boonyapakorn, C., & Thongkorn, K. (2022). Effectiveness of a Nanohydroxyapatite-Based Hydrogel on Alveolar Bone Regeneration in Post-Extraction Sockets of Dogs with Naturally Occurring Periodontitis. Veterinary Sciences, 9(1), 7. https://doi.org/10.3390/vetsci9010007