
Maternal Left Ventricular Diastolic and Systolic Function during Normal Pregnancy in Saint Bernard Dogs

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals and Follow-Up
2.2. Echocardiographic Evaluation
2.3. Blood Pressure Measurement
2.4. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kametas, N.A.; McAuliffe, F.; Cook, B.; Nicolaides, K.; Chambers, J. Maternal left ventricular transverse and long-axis systolic function during pregnancy. Ultrasound Obstet. Gynecol. 2001, 18, 467–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesa, A.; Jessurun, C.; Hernandez, A.; Adam, K.; Brown, D.; Vaughn, W.K.; Wilansky, S. Left ventricular diastolic function in normal human pregnancy. Circulation 1999, 99, 511–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valensise, H.; Novelli, G.P.; Vasapollo, B.; Borzi, M.; Arduini, D.; Galante, A.; Romanini, C. Maternal cardiac systolic and diastolic function: Relationship with uteroplacental resistances. A Doppler and echocardiographic longitudinal study. Ultrasound Obstet. Gynecol. 2000, 15, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Abbott, J.A. The effect of pregnancy on echocardiographic variables in healthy bitches. J. Vet. Cardiol. 2010, 12, 123–128. [Google Scholar] [CrossRef]
- Blanco, P.G.; Tortora, M.; Rodríguez, R.; Arias, D.O.; Gobello, C. Ultrasonographic assessment of maternal cardiac function and peripheral circulation during normal gestation in dogs. Vet. J. 2011, 190, 154–159. [Google Scholar] [CrossRef]
- Blanco, P.; Batista, P.; Gómez, F.; Arias, D.; Gobello, C. Echocardiographic and Doppler assessment of maternal cardiovascular function in normal and abnormal canine pregnancies. Theriogenology 2012, 78, 1235–1242. [Google Scholar] [CrossRef]
- Williams, J.G.; Rincon-Skinner, T.; Sun, D.; Wang, Z.; Zhang, S.; Zhang, X.; Hintze, T.H. Role of nitric oxide in the coupling of myocardial oxygen consumption and coronary vascular dynamics during pregnancy in the dog. Am. J. Physiol. Circ. Physiol. 2007, 293, H2479–H2486. [Google Scholar] [CrossRef] [PubMed]
- Almeida, V.T.; Uscategui, R.A.; Camacho, A.A.; Sousa, M.G.; Santos, V.J.; Maronezi, M.C.; Vicente, W.R.; Feliciano, M.; Camacho, A.A. Influence of estrous cycle and gestation on cardiovascular system of bitches. Anim. Reprod. Sci. 2018, 192, 35–43. [Google Scholar] [CrossRef]
- Fok, W.Y.; Chan, L.Y.; Wong, J.T.; Yu, C.M.; Lau, T.K. Left ventricular diastolic function during normal pregnancy: Assessment by spectral tissue Doppler imaging. Ultrasound Obstet. Gynecol. 2006, 28, 789–793. [Google Scholar] [CrossRef]
- Zentner, D.; Du Plessis, M.; Brennecke, S.; Wong, J.; Grigg, L.; Harrap, S. Deterioration in cardiac systolic and diastolic function late in normal human pregnancy. Clin. Sci. 2009, 116, 599–606. [Google Scholar] [CrossRef] [Green Version]
- Toaldo, M.B.; Poser, H.; Menciotti, G.; Battaia, S.; Contiero, B.; Cipone, M.; Diana, A.; Mazzotta, E.; Guglielmini, C. Utility of Tissue Doppler Imaging in the Echocardiographic Evaluation of Left and Right Ventricular Function in Dogs with Myxomatous Mitral Valve Disease with or without Pulmonary Hypertension. J. Vet. Intern. Med. 2016, 30, 697–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chetboul, V. Advanced Techniques in Echocardiography in Small Animals. Vet. Clin. N. Am. Small Anim. Pr. 2010, 40, 529–543. [Google Scholar] [CrossRef] [PubMed]
- Lakoumentas, J.A.; Panou, F.K.; Kotseroglou, V.K.; Aggeli, K.I.; Harbis, P.K. The Tei index of myocardial performance: Applications in cardiology. Hell. J. Cardiol. 2005, 46, 52–58. [Google Scholar]
- Gerede, D.M.; Turhan, S.; Kaya, C.T.; Ozcan, O.U.; Goksuluk, H.; Vurgun, V.K.; Dinçer, I.; Kutlay, S.; Erturk, S.; Erol, C. Effects of Hemodialysis on Tei Index: Comparison between Flow Doppler and Tissue Doppler Imaging. Echocardiography 2015, 32, 1520–1526. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, K.; Balci, S.; Duzenli, M.A.; Can, I.; Yazici, M.; Aygul, N.; Altunkeser, B.B.; Altintepe, L.; Turk, S. Effect of Preload and Heart Rate on the Doppler and Tissue Doppler-derived Myocardial Performance Index. Clin. Cardiol. 2007, 30, 342–348. [Google Scholar] [CrossRef]
- Duvekot, J.J.; Cheriex, E.C.; Pieters, F.A.; Menheere, P.P.; Peeters, L.L. Early pregnancy changes in hemodynamics and volume homeostasis are consecutive adjustments triggered by a primary fall in systemic vascular tone. Am. J. Obstet. Gynecol. 1993, 169, 1382–1392. [Google Scholar] [CrossRef]
- Desai, D.K.; Moodley, J.; Naidoo, D.P. Echocardiographic Assessment of Cardiovascular Hemodynamics in Normal Pregnancy. Obstet. Gynecol. 2004, 104, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Kametas, N.; McAuliffe, F.; Hancock, J.; Chambers, J.; Nicolaides, K. Maternal left ventricular mass and diastolic function during pregnancy. Ultrasound Obstet. Gynecol. 2001, 18, 460–466. [Google Scholar] [CrossRef] [Green Version]
- Olsson, K.; Lagerstedt, A.S.; Bergström, A.; Häggström, J. Change of Diurnal Heart Rate Patterns during Pregnancy and Lactation in Dogs (Canis familiaris). Acta Vet. Scand. 2003, 44, 105–110. [Google Scholar] [CrossRef]
- Stoneham, A.E.; Graham, J.; Rozanski, E.A.; Rush, J.E. Pregnancy-Associated Congestive Heart Failure in a Cat. J. Am. Anim. Hosp. Assoc. 2006, 42, 457–461. [Google Scholar] [CrossRef]
- Martin, M.W.S.; Johnson, M.J.S.; Celona, B. Canine dilated cardiomyopathy: A retrospective study of signalment, presentation and clinical findings in 369 cases. J. Small Anim. Pract. 2009, 50, 23–29. [Google Scholar] [CrossRef]
- England, G.; Russo, M. Ultrasonographic characteristics of early pregnancy failure in bitches. Theriogenology 2006, 66, 1694–1698. [Google Scholar] [CrossRef] [PubMed]
- Thomas, W.P.; Gaber, C.E.; Jacobs, G.J.; Kaplan, P.M.; Lombard, C.W.; Vet, M.; Moise, N.S.; Moses, B.L. Recommendations for Standards in Transthoracic Two-Dimensional Echocardiography in the Dog and Cat. J. Vet. Intern. Med. 1993, 7, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Gottdiener, J.S.; Bednarz, J.; Devereux, R.; Gardin, J.; Klein, A.; Manning, W.J.; Morehead, A.; Kitzman, D.; Oh, J.; Quinones, M.; et al. American Society of Echocardiography recommendations for use of echocardiography in clinical trials. J. Am. Soc. Echocardiogr. 2004, 17, 1086–1119. [Google Scholar] [CrossRef] [PubMed]
- Madron, E.; Chetboul, V.; Bussadori, C. Global left ventricle systolic function assessment. In Clinical Echocardiography of the Dog and Cat. E. Madron; Elsevier: Amsterdam, The Netherlands, 2012; pp. 111–125. [Google Scholar]
- Moura, C.; Fontes-Sousa, A.P.; Teixeira-Pinto, A.; Areias, J.C.C.; Leite-Moreira, A.F. Agreement between echocardiographic techniques in assessment of the left ventricular myocardial performance index in rabbits. Am. J. Vet. Res. 2009, 70, 464–471. [Google Scholar] [CrossRef]
- Rysnik, M.K.; Cripps, P.; Iff, I. A clinical comparison between a non-invasive blood pressure monitor using high definition oscillometry (Memodiagnostic MD 15/90 Pro) and invasive arterial blood pressure measurement in anaesthetized dogs. Vet. Anaesth. Analg. 2013, 40, 503–511. [Google Scholar] [CrossRef]
- Di Salvo, P.; Bocci, F.; Zelli, R.; Polisca, A. Doppler evaluation of maternal and fetal vessels during normal gestation in the bitch. Res. Vet. Sci. 2006, 81, 382–388. [Google Scholar] [CrossRef]
- Wooding, F.; Flint, A. Placentation. In Marshall’s Physiology of Reproduction, 4th ed.; G.E. Lamming. Chapman & Hall: Avon, UK, 1994; Volume 3, pp. 233–460. [Google Scholar]
- Blanco, P.; Batista, P.; Re, N.; Mattioli, G.; Arias, D.; Gobello, C. Electrocardiographic Changes in Normal and Abnormal Canine Pregnancy. Reprod. Domest. Anim. 2011, 47, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Savu, O.; Jurcuţ, R.; Giuşcă, S.; Van Mieghem, T.; Gussi, I.; Popescu, B.A.; Ginghină, C.; Rademakers, F.; Deprest, J.; Voigt, J.-U. Morphological and Functional Adaptation of the Maternal Heart During Pregnancy. Circ. Cardiovasc. Imaging 2012, 5, 289–297. [Google Scholar] [CrossRef] [Green Version]
- Eghbali, M.; Deva, R.; Alioua, A.; Minosyan, T.Y.; Ruan, H.; Wang, Y.; Toro, L.; Stefani, E. Molecular and Functional Signature of Heart Hypertrophy During Pregnancy. Circ. Res. 2005, 96, 1208–1216. [Google Scholar] [CrossRef] [Green Version]
- Van Oppen, A.C.; Stigter, R.H.; Bruinse, H.W. Cardiac output in normal pregnancy: A critical review. Obstet. Gynecol. 1996, 87, 310–318. [Google Scholar] [CrossRef]
- Sadaniantz, A.; Kocheril, A.G.; Emaus, S.P.; Garber, C.E.; Parisi, A.F. Cardiovascular Changes in Pregnancy Evaluated by Two-dimensional and Doppler Echocardiography. J. Am. Soc. Echocardiogr. 1992, 5, 253–258. [Google Scholar] [CrossRef]
- Hori, Y.; Ukai, Y.; Hoshi, F.; Higuchi, S.-I. Volume loading–related changes in tissue Doppler images derived from the tricuspid valve annulus in dogs. Am. J. Vet. Res. 2008, 69, 33–38. [Google Scholar] [CrossRef]
- Bamfo, J.E.; Kametas, N.A.; Nicolaides, K.; Chambers, J.B.; Kametas, N.; Kametas, N. Maternal left ventricular diastolic and systolic long-axis function during normal pregnancy. Eur. J. Echocardiogr. 2007, 8, 360–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bamfo, J.E.A.K.; Kametas, N.A.; Nicolaides, K.; Chambers, J.B. Reference ranges for tissue Doppler measures of maternal systolic and diastolic left ventricular function. Ultrasound Obstet. Gynecol. 2007, 29, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlin, A.; Alfirevic, Z. Physiological changes of pregnancy and monitoring. Best Pr. Res. Clin. Obstet. Gynaecol. 2008, 22, 801–823. [Google Scholar] [CrossRef]
- Lee, B.-H.; Dukes-McEwan, J.; French, A.T.; Corcoran, B.M. Evaluation of a novel doppler index of combined systolic and diastolic myocardial performance in Newfoundland dogs with familial prevalence of dilated cardiomyopathy. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2002, 43, 154–165. [Google Scholar] [CrossRef]
- Sousa, M.G.; Carareto, R.; De-Nardi, A.B.; Brito, F.L.; Nunes, N.; Camacho, A.A. Effects of isoflurane on Tei-index of myocardial performance in healthy dogs. Can. Vet. J. = La Rev. Vet. Can. 2007, 48, 277–282. [Google Scholar]
- Gungoren, F.; Tanriverdi, Z.; Besli, F.; Barut, M.U.; Tascanov, M.B. The evaluation of diastolic function and myocardial performance index during pregnancy: A tissue Doppler echocardiography study. Echocardiography 2019, 36, 2152–2157. [Google Scholar] [CrossRef]


{kind=link}
| Variable | T1 (21–28 d) | T2 (40 d) | T3 (60 d) | Postpartum (4–8 wk) | p-Value | |
|---|---|---|---|---|---|---|
| BW (kg) | 59.67 ± 5.93 | 65.13 ± 6.82 | 71.50 ± 6.82 | 61.03 ± 4.42 | T3 vs. T1, T2 and PP ** | |
| BSA (m2) | 1.53 ± 0.10 | 1.62 ± 0.11 | 1.72 ± 0.11 | 1.55 ± 0.08 | T3 vs. T1, T2 and PP ** | |
| HR (bpm) | 117.2 ± 11.16 | 120.4 ± 14.42 | 128.4 ± 7.88 | 118.6 ± 8.95 | T3 vs. T1 and PP * | |
| SAP (mmHg) | 185.7 ± 19.37 | 167.6 ± 20.55 | 166.1 ± 25.47 | 130.9 ± 11.55 | PP vs. T1, T2 and T3 ** | |
| MAP (mmHg) | 139.8 ± 18.43 | 123.8 ± 19.29 | 118.9 ± 21.24 | 91.8 ± 9.73 | PP vs. T1, T2 and T3 ** | |
| DAP (mmHg) | 114.4 ± 18.2 | 100 ± 19.06 | 93.8 ± 18.55 | 70.5 ± 8.57 | PP vs. T1, T2 and T3 ** | |
| LVDd (mm) | 48.64 ± 4.32 | 48.14 ± 4.37 | 49.79 ± 4.56 | 47.82 ± 2.81 | NS | |
| LVDs (mm) | 35.94 ± 4.94 | 36.63 ± 5.56 | 35.86 ± 4.33 | 34.49 ± 3.75 | NS | |
| LVPWd (mm) | 11.37 ± 1.11 | 11.26 ± 0.88 | 11.46 ± 1.08 | 11.60 ± 1.31 | NS | |
| LVPWs (mm) | 14.58 ± 1.56 | 14.27 ± 1.65 | 14.69 ± 1.58 | 15.47 ± 2.62 | NS | |
| IVSd (mm) | 11.28 ± 1.87 | 10.79 ± 1.29 | 11.83 ± 2.22 | 11.28 ± 1.92 | NS | |
| IVSs (mm) | 13.99 ± 2.32 | 13.57 ± 1.89 | 14.34 ± 2.37 | 13.81 ± 2.42 | NS | |
| LV mass (g) | 207.89 ± 38.38 | 199.14 ± 51.17 | 227.39 ± 60.38 | 205.40 ± 40.15 | NS | |
| EPSS (mm) | 7.08 ± 2.01 | 6.96 ± 2.37 | 5.87 ± 3.95 | 6.61 ± 0.81 | NS | |
| FS (%) | 26.25 ± 5.88 | 24.22 ± 6.80 | 28.02 ± 4.99 | 27.97 ± 5.24 | NS | |
| EF (%) | 55.87 ± 7.06 | 55.29 ± 9.03 | 58.63 ± 4.46 | 58.88 ± 4.35 | NS | |
| SV (mL) | 56.37 ± 13.26 | 50.86 ± 9.43 | 63.32 ± 15.38 | 57.13 ± 10.43 | NS | |
| CO (L/min) | 6.57 ± 1.49 | 6.12 ± 1.37 | 8.12 ± 1.96 | 6.79 ± 1.43 | T3 vs. PP * | |
| LA (mm) | 38.85 ± 5.59 | 41.55 ± 9.25 | 38.90 ± 8.33 | 41.59 ± 7.19 | NS | |
| Ao (mm) | 28.69 ± 2.80 | 28.80 ± 1.68 | 28.83 ± 2.40 | 29.25 ± 3.21 | NS | |
| LA/Ao | 1.36 ± 0.16 | 1.44 ± 0.31 | 1.34 ± 0.24 | 1.43 ± 0.25 | T3 vs. T2 * | |
| AoV (m/s) | 1.28 ± 0.19 | 1.28 ± 0.15 | 1.48 ± 0.16 | 1.32 ± 0.17 | T3 vs. T1 ** | |
| E (m/s) | 0.68 ± 0.08 | 0.75 ± 0.12 | 0.75 ± 0.13 | 0.76 ± 0.09 | T1 vs. T2 and T3 * | |
| A (m/s) | 0.61 ± 0.07 | 0.71 ± 0.11 | 0.74 ± 0.15 | 0.72 ± 0.08 | T1 vs. T2, T3 and PP * | |
| E/A ratio | 1.12 ± 0.08 | 1.04 ± 0.12 | 1.02 ± 0.12 | 1.07 ± 0.13 | NS | |
| Pul (m/s) | 0.92 ± 0.16 | 0.95 ± 0.12 | 1.15 ± 0.16 | 1.05 ± 0.11 | T3 vs. T1 and T2 * | |
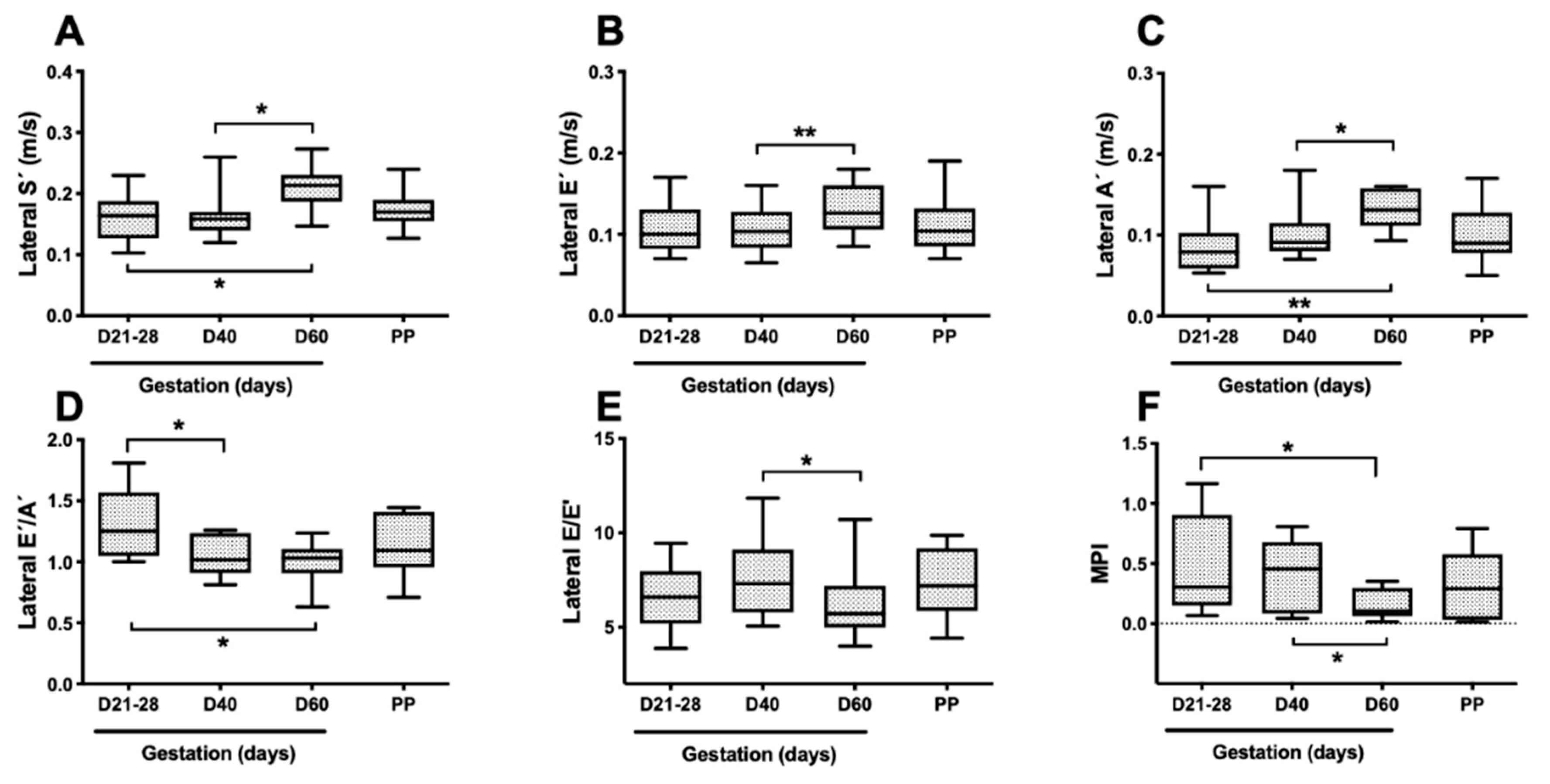
| MPI | 0.47 ± 0.40 | 0.41±0.29 | 0.16 ± 0.12 | 0.33 ± 0.29 | T3 vs. T1 and T2 * | |
| Septal wall | S’ (m/s) | 0.11 ± 0.02 | 0.12 ± 0.03 | 0.12 ± 0.02 | 0.13 ± 0.03 | NS |
| E’ (m/s) | 0.09 ± 0.03 | 0.08 ± 0.02 | 0.09 ± 0.02 | 0.09 ± 0.02 | NS | |
| A’ (m/s) | 0.08 ± 0.03 | 0.08 ± 0.02 | 0.09 ± 0.01 | 0.08 ± 0.02 | NS | |
| E/E’ ratio | 8.44 ± 2.80 | 9.36 ± 2.35 | 8.95 ± 2.83 | 8.84 ± 1.95 | NS | |
| E’/A’ ratio | 1.21 ± 0.37 | 1.03 ± 0.18 | 0.97 ± 0.19 | 1.11 ± 0.20 | NS | |
| Lateral wall | S’ (m/s) | 0.16 ± 0.04 | 0.16 ± 0.04 | 0.21 ± 0.04 | 0.17 ± 0.04 | T3 vs. T1 and T2 * |
| E’ (m/s) | 0.11 ± 0.03 | 0.11 ± 0.03 | 0.13 ± 0.03 | 0.11 ± 0.04 | T3 vs. T2 ** | |
| A’ (m/s) | 0.09 ± 0.03 | 0.10 ± 0.03 | 0.13 ± 0.02 | 0.10 ± 0.03 | T3 vs. T1 and T2 ** | |
| E/E’ ratio | 6.68 ± 1.76 | 7.54 ± 2.16 | 6.15 ± 1.95 | 7.20 ± 1.83 | T3 vs. T2 ** | |
| E’/A’ ratio | 1.30 ± 0.29 | 0.94 ± 0.32 | 1.00 ± 0.17 | 1.03 ± 0.14 | T1 vs. T2 and T3 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lobo, L.; Esteves-Guimarães, J.; Oliveira, P.; Salazar, L.; Pereira, A.; Fontes-Sousa, A.P. Maternal Left Ventricular Diastolic and Systolic Function during Normal Pregnancy in Saint Bernard Dogs. Vet. Sci. 2021, 8, 306. https://doi.org/10.3390/vetsci8120306
Lobo L, Esteves-Guimarães J, Oliveira P, Salazar L, Pereira A, Fontes-Sousa AP. Maternal Left Ventricular Diastolic and Systolic Function during Normal Pregnancy in Saint Bernard Dogs. Veterinary Sciences. 2021; 8(12):306. https://doi.org/10.3390/vetsci8120306
Chicago/Turabian StyleLobo, Luís, Joana Esteves-Guimarães, Pedro Oliveira, Luís Salazar, André Pereira, and Ana Patrícia Fontes-Sousa. 2021. "Maternal Left Ventricular Diastolic and Systolic Function during Normal Pregnancy in Saint Bernard Dogs" Veterinary Sciences 8, no. 12: 306. https://doi.org/10.3390/vetsci8120306
APA StyleLobo, L., Esteves-Guimarães, J., Oliveira, P., Salazar, L., Pereira, A., & Fontes-Sousa, A. P. (2021). Maternal Left Ventricular Diastolic and Systolic Function during Normal Pregnancy in Saint Bernard Dogs. Veterinary Sciences, 8(12), 306. https://doi.org/10.3390/vetsci8120306