
Comparative Review of Malignant Melanoma and Histologically Well-Differentiated Melanocytic Neoplasm in the Oral Cavity of Dogs

Abstract
:1. Introduction
2. Signalment and Presenting Signs
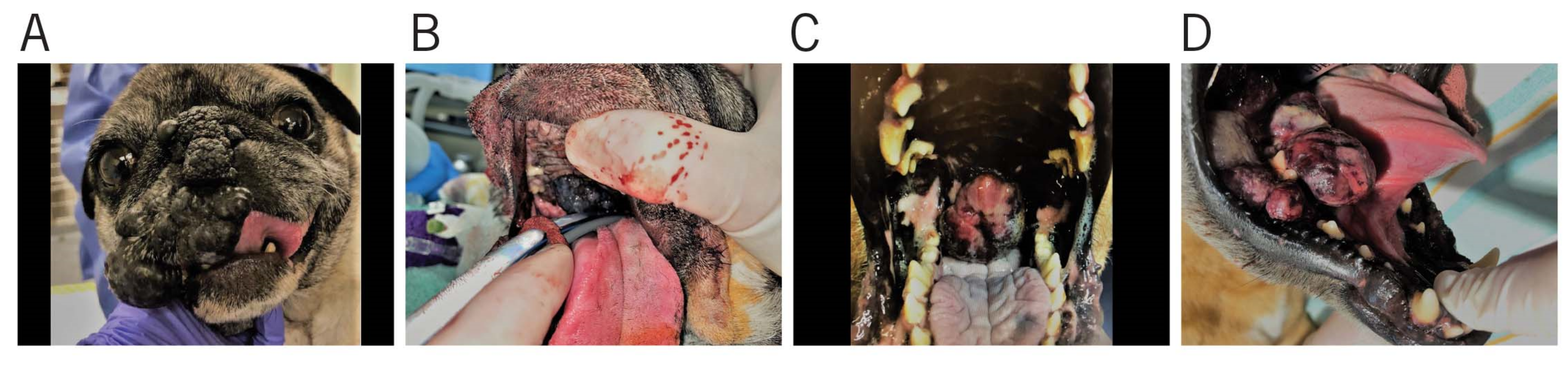
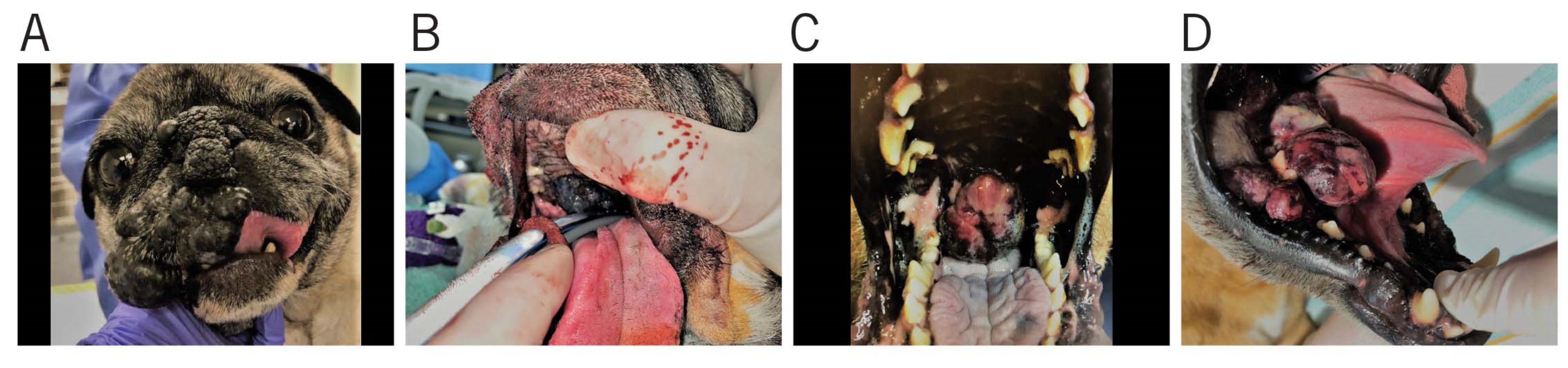
3. Gross Appearance and Cytology
4. Staging Diagnostics
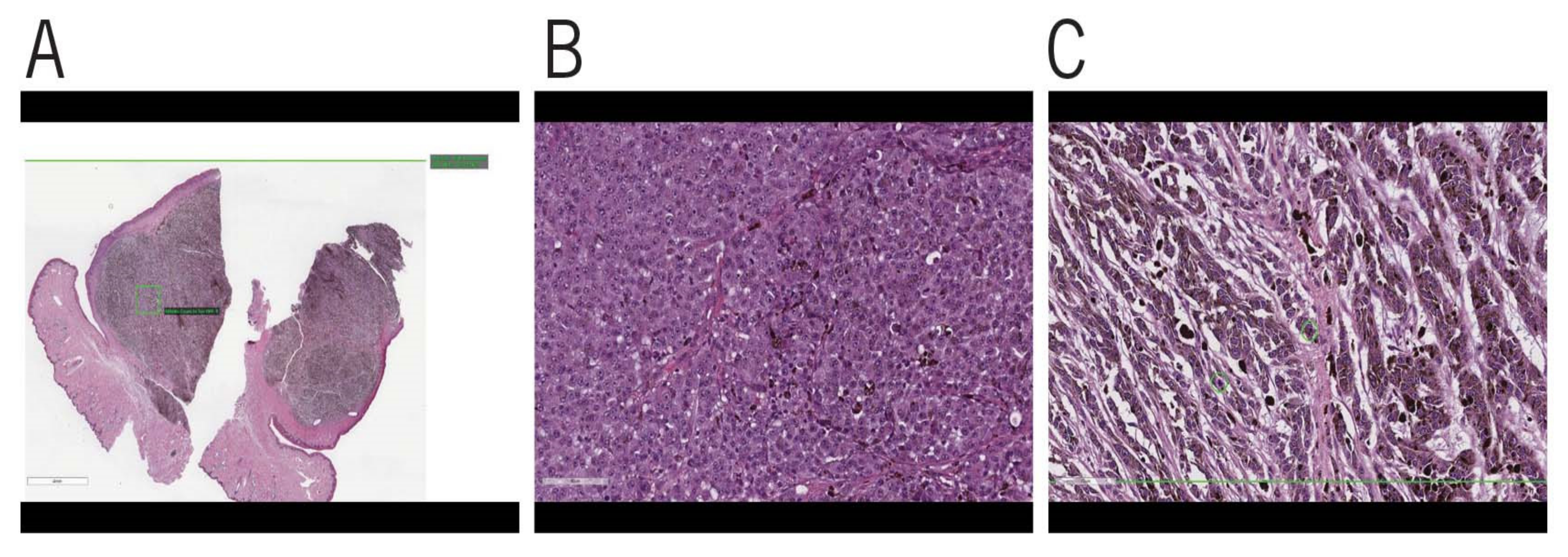
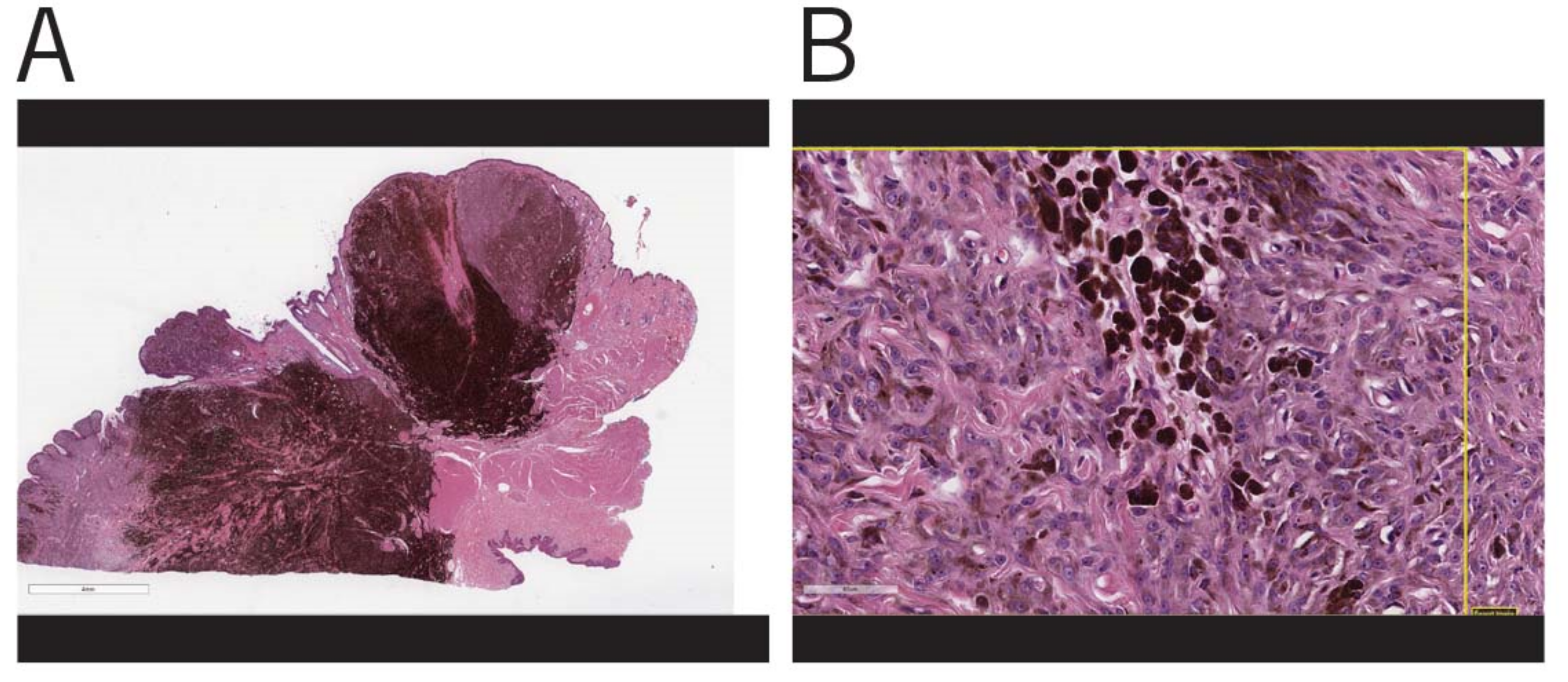
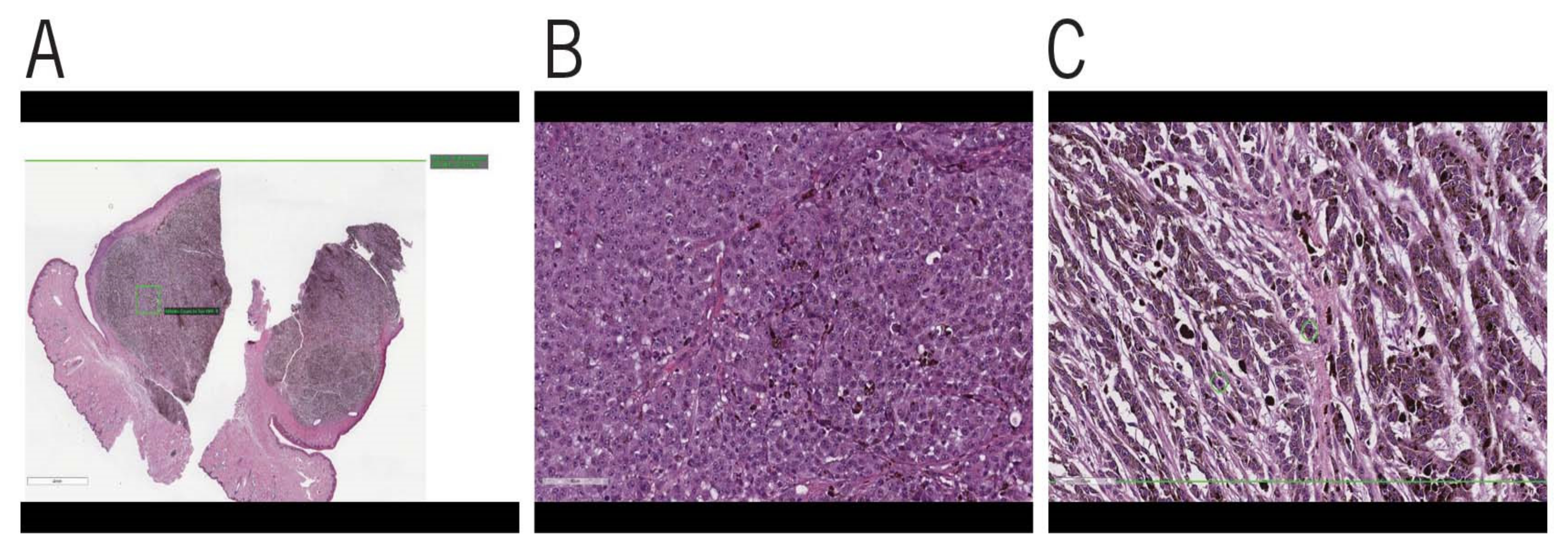
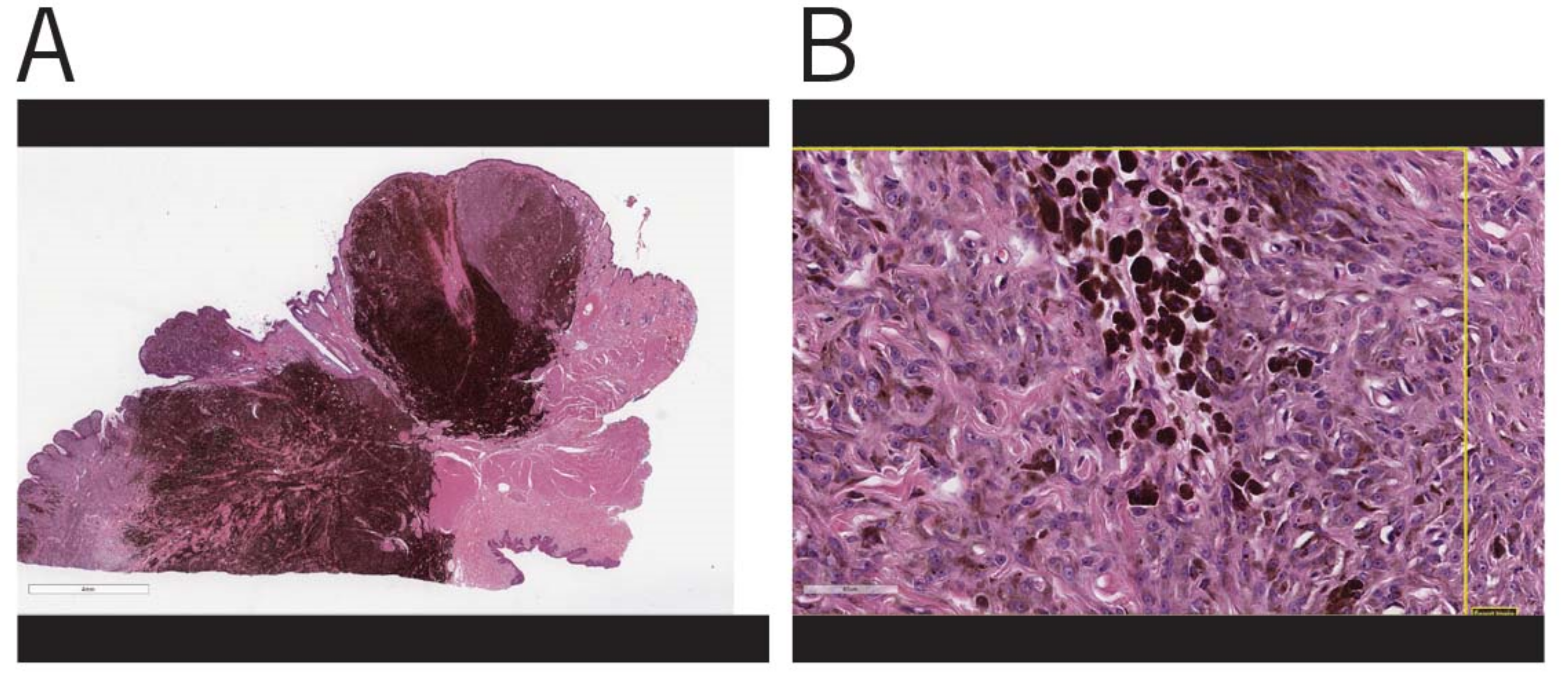
5. Histopathology
6. Treatment
7. Prognosis
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| OMM | Oral Malignant Melanoma |
| HWDMN | Histologically Well-Differentiated Melanocytic Neoplasm |
| MST | Median Survival Time |
| IMRT | Intensity-Modulated Radiation Therapy |
| RT | Radiation Therapy |
| WHO | World Health Organization |
References
- Mikiewicz, M.; Paździor-Czapula, K.; Gesek, M.; Lemishevskyi, V.; Otrocka-Domagała, I. Canine and Feline Oral Cavity Tumours and Tumour-like Lesions: A Retrospective Study of 486 Cases (2015–2017). J. Comp. Pathol. 2019, 172, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Sarowitz, B.N.; Davis, G.J.; Kim, S. Outcome and prognostic factors following curative-intent surgery for oral tumours in dogs: 234 cases (2004 to 2014). J. Small Anim. Pract. 2017, 58, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.H.; Goldschmidt, M.; McManus, P.M. A comparative review of melanocytic neoplasms. Vet. Pathol. 2002, 39, 651–678. [Google Scholar] [CrossRef] [PubMed]
- Brodey, R.S. The biological behaviour of canine oral and pharyngeal neoplasms. J. Small Anim. Pract. 1970, 11, 45–53. [Google Scholar] [CrossRef]
- Harvey, H.J. Oral tumors. Vet. Clin. N. Am. Small Anim. Pract. 1985, 15, 493–500. [Google Scholar] [CrossRef]
- Willcox, J.L.; Spriet, M.; Zwingenberger, A.L.; Phillips, K.L.; Burton, J.H.; Skorupski, K.A.; Hansen, K.S.; Affolter, V.K.; Woolard, K.D.; Beylin, D.; et al. Evaluation of accuracy for (18) F-FDG positron emission tomography and computed tomography for detection of lymph node metastasis in canine oral malignant melanoma. Vet. Comp. Oncol. 2021, 19, 463–472. [Google Scholar] [CrossRef]
- Harvey, H.J.; MacEwen, E.G.; Braun, D.; Patnaik, A.K.; Withrow, S.J.; Jongeward, S. Prognostic criteria for dogs with oral melanoma. J. Am. Vet. Med. Assoc. 1981, 178, 580–582. [Google Scholar] [PubMed]
- Tuohy, J.L.; Selmic, L.E.; Worley, D.R.; Ehrhart, N.P.; Withrow, S.J. Outcome following curative-intent surgery for oral melanoma in dogs: 70 cases (1998–2011). J. Am. Vet. Med. Assoc. 2014, 245, 1266–1273. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P.J.; Camps-Palau, M.A.; McKnight, J.A.; Leibman, N.F.; Craft, D.M.; Leung, C.; Liao, J.; Riviere, I.; Sadelain, M.; Hohenhaus, A.E.; et al. Development of a xenogeneic DNA vaccine program for canine malignant melanoma at the Animal Medical Center. Vaccine 2006, 24, 4582–4585. [Google Scholar] [CrossRef] [PubMed]
- Bateman, K.E.; Catton, P.A.; Pennock, P.W.; Kruth, S.A. 0-7-21 radiation therapy for the treatment of canine oral melanoma. J. Vet. Intern. Med. 1994, 8, 267–272. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. TNM Classification of Tumours in Domestic Animals; Owen, L.N., Ed.; World Health Organization: Geneva, Switzerland, 1980. [Google Scholar]
- Bergman, P.J. Canine Oral Melanoma. Clin. Tech. Small Anim. Pract. 2007, 22, 55–60. [Google Scholar] [CrossRef]
- Nishiya, A.T.; Massoco, C.O.; Felizzola, C.R.; Perlmann, E.; Batschinski, K.; Tedardi, M.V.; Garcia, J.S.; Mendonça, P.P.; Teixeira, T.F.; Zaidan Dagli, M.L. Comparative Aspects of Canine Melanoma. Vet. Sci. 2016, 3, 7. [Google Scholar] [CrossRef] [PubMed]
- Proulx, D.R.; Ruslander, D.M.; Dodge, R.K.; Hauck, M.L.; Williams, L.E.; Horn, B.; Price, G.S.; Thrall, D.E. A retrospective analysis of 140 dogs with oral melanoma treated with external beam radiation. Vet. Radiol. Ultrasound 2003, 44, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Théon, A.P.; Rodriguez, C.; Madewell, B.R. Analysis of prognostic factors and patterns of failure in dogs with malignant oral tumors treated with megavoltage irradiation. J. Am. Vet. Med. Assoc. 1997, 210, 778–784. [Google Scholar] [PubMed]
- Murphy, S.; Hayes, A.M.; Blackwood, L.; Maglennon, G.; Pattinson, H.; Sparkes, A.H. Oral malignant melanoma-the effect of coarse fractionation radiotherapy alone or with adjuvant carboplatin therapy. Vet. Comp. Oncol. 2005, 3, 222–229. [Google Scholar] [CrossRef]
- Freeman, K.P.; Hahn, K.A.; Harris, F.D.; King, G.K. Treatment of dogs with oral melanoma by hypofractionated radiation therapy and platinum-based chemotherapy (1987–1997). J. Vet. Intern. Med. 2003, 17, 96–101. [Google Scholar] [PubMed]
- Boston, S.E.; Lu, X.; Culp, W.T.; Montinaro, V.; Romanelli, G.; Dudley, R.M.; Liptak, J.M.; Mestrinho, L.A.; Buracco, P. Efficacy of systemic adjuvant therapies administered to dogs after excision of oral malignant melanomas: 151 cases (2001–2012). J. Am. Vet. Med. Assoc. 2014, 245, 401–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grosenbaugh, D.A.; Leard, A.T.; Bergman, P.J.; Klein, M.K.; Meleo, K.; Susaneck, S.; Hess, P.R.; Jankowski, M.K.; Jones, P.D.; Leibman, N.F.; et al. Safety and efficacy of a xenogeneic DNA vaccine encoding for human tyrosinase as adjunctive treatment for oral malignant melanoma in dogs following surgical excision of the primary tumor. Am. J. Vet. Res. 2011, 72, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Spangler, W.L.; Kass, P.H. The histologic and epidemiologic bases for prognostic considerations in canine melanocytic neoplasia. Vet. Pathol. 2006, 43, 136–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esplin, D.G. Survival of dogs following surgical excision of histologically well-differentiated melanocytic neoplasms of the mucous membranes of the lips and oral cavity. Vet. Pathol. 2008, 45, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Cangul, I.T.; van Garderen, E.; van der Linde-Sipman, J.S.; van den Ingh, T.S.; Schalken, J.A. Canine balloon and signet-ring cell melanomas: A histological and immunohistochemical characterization. J. Comp. Pathol. 2001, 125, 166–173. [Google Scholar] [CrossRef]
- Blanchard, T.; Bryant, N.; Mense, M. Balloon cell melanoma in three dogs: A histopathological, immunohistochemical and ultrastructural study. J. Comp. Pathol. 2001, 125, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Vara, J.A.; Beissenherz, M.E.; Miller, M.A.; Johnson, G.C.; Pace, L.W.; Fard, A.; Kottler, S.J. Retrospective study of 338 canine oral melanomas with clinical, histologic, and immunohistochemical review of 129 cases. Vet. Pathol. 2000, 37, 597–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Todoroff, R.J.; Brodey, R.S. Oral and pharyngeal neoplasia in the dog: A retrospective survey of 361 cases. J. Am. Vet. Med. Assoc. 1979, 175, 567–571. [Google Scholar]
- Miller, W.H., Jr.; Griffin, C.E.; Campbell, K.L. Muller and Kirk’s Small Animal Dermatology, 7th ed.; Elsevier Mosby: Saint Louis, MO, USA, 2013. [Google Scholar]
- Aloua, R.; Kaouani, A.; Kerdoud, O.; Salissou, I.; Slimani, F. Melanoma of the oral cavity: A silent killer. Ann. Med. Surg. 2021, 62, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Chae, Y.S.; Lee, J.Y.; Lee, J.W.; Park, J.Y.; Kim, S.M.; Lee, J.H. Survival of oral mucosal melanoma according to treatment, tumour resection margin, and metastases. Br. J. Oral Maxillofac. Surg. 2020, 58, 1097–1102. [Google Scholar] [CrossRef]
- Van der Waal, R.I.; Snow, G.B.; Karim, A.B.; van der Waal, I. Primary malignant melanoma of the oral cavity: A review of eight cases. Br. Dent. J. 1994, 176, 185–188. [Google Scholar]
- Patel, S.G.; Prasad, M.L.; Escrig, M.; Singh, B.; Shaha, A.R.; Kraus, D.H.; Boyle, J.O.; Huvos, A.G.; Busam, K.; Shah, J.P. Primary mucosal malignant melanoma of the head and neck. Head Neck 2002, 24, 247–257. [Google Scholar] [CrossRef]
- Gillard, M.; Cadieu, E.; De Brito, C.; Abadie, J.; Vergier, B.; Devauchelle, P.; Degorce, F.; Dréano, S.; Primot, A.; Dorso, L.; et al. Naturally occurring melanomas in dogs as models for non-UV pathways of human melanomas. Pigment. Cell Melanoma Res. 2014, 27, 90–102. [Google Scholar] [CrossRef]
- Goldschmidt, M.H. Benign and malignant melanocytic neoplasms of domestic animals. Am. J. Dermatopathol. 1985, 7, 203–212. [Google Scholar] [CrossRef]
- Prouteau, A.; André, C. Canine Melanomas as Models for Human Melanomas: Clinical, Histological, and Genetic Comparison. Genes 2019, 10, 501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, M.J.; Flaitz, C.M. Oral mucosal melanoma: Epidemiology and pathobiology. Oral Oncol. 2000, 36, 152–169. [Google Scholar] [CrossRef]
- Goubran, G.F.; O Adekeye, E.; Edwards, M.B. Melanoma of the face and mouth in Nigeria. A review and comment on three cases. Int. J. Oral Surg. 1978, 7, 453–462. [Google Scholar] [CrossRef]
- Tremblay, J.-F.; O’Brien, E.A.; Chauvin, P.J. Melanoma In Situ of the oral mucosa in an adolescent with dysplastic nevus syndrome. J. Am. Acad. Dermatol. 2000, 42, 844–846. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.E.; Packer, R.A. Association between lymph node size and metastasis in dogs with oral malignant melanoma: 100 cases (1987–2001). J. Am. Vet. Med. Assoc. 2003, 222, 1234–1236. [Google Scholar] [CrossRef]
- Langenbach, A.; McManus, P.M.; Hendrick, M.J.; Shofer, F.S.; Sorenmo, K.U. Sensitivity and specificity of methods of assessing the regional lymph nodes for evidence of metastasis in dogs and cats with solid tumors. J. Am. Vet. Med. Assoc. 2001, 218, 1424–1428. [Google Scholar] [CrossRef]
- Skinner, O.T.; Boston, S.E.; Souza, C.H.D.M. Patterns of lymph node metastasis identified following bilateral mandibular and medial retropharyngeal lymphadenectomy in 31 dogs with malignancies of the head. Vet. Comp. Oncol. 2017, 15, 881–889. [Google Scholar] [CrossRef]
- Hahn, K.A.; DeNicola, D.B.; Richardson, R.C.; Hahn, E.A. Canine oral malignant melanoma: Prognostic utility of an alternative staging system. J. Small Anim. Pract. 1994, 35, 251–256. [Google Scholar] [CrossRef]
- Weiss, E.; Frese, K. Tumours of the skin. Bull. World Health Organ. 1974, 50, 79–100. [Google Scholar]
- Head, K.W. Tumours of the upper alimentary tract. Bull. World Health Organ. 1976, 53, 145–166. [Google Scholar] [PubMed]
- Rabanal, R.H.; Fondevila, D.M.; Montané, V.; Domingo, M.; Ferrer, L. Immunocytochemical diagnosis of skin tumours of the dog with special reference to undifferentiated types. Res. Vet. Sci. 1989, 47, 129–133. [Google Scholar] [CrossRef]
- Sulaimon, S.; Kitchell, B.; Ehrhart, E. Immunohistochemical detection of melanoma-specific antigens in spontaneous canine melanoma. J. Comp. Pathol. 2002, 127, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Potts, B.C.; Smith, J.; Akke, M.; Macke, T.J.; Okazaki, K.; Hidaka, H.; Case, D.A.; Chazin, W.J. The structure of calcyclin reveals a novel homodimeric fold for S100 Ca(2+)-binding proteins. Nat. Struct. Biol. 1995, 2, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Ruiter, D.J.; Brocker, E.B. Immunohistochemistry in the evaluation of melanocytic tumors. Semin. Diagn. Pathol. 1993, 10, 76–91. [Google Scholar] [PubMed]
- Sandusky, G.E., Jr.; Carlton, W.W.; Wightman, K.A. Immunohistochemical staining for S100 protein in the diagnosis of canine amelanotic melanoma. Vet. Pathol. 1985, 22, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Rochaix, P.; Lacroix-Triki, M.; Lamant, L.; Pichereaux, C.; Valmary, S.; Puente, E.; Al Saati, T.; Monsarrat, B.; Susini, C.; Buscail, L.; et al. PNL2, a new monoclonal antibody directed against a fixative-resistant melanocyte antigen. Mod. Pathol. 2003, 16, 481–490. [Google Scholar] [CrossRef] [Green Version]
- Ramos-Vara, J.A.; Miller, M.A. Immunohistochemical identification of canine melanocytic neoplasms with antibodies to melanocytic antigen PNL2 and tyrosinase: Comparison with Melan A. Vet. Pathol. 2011, 48, 443–450. [Google Scholar] [CrossRef]
- Berrington, A.J.; Jimbow, K.; Haines, D.M. Immunohistochemical detection of melanoma-associated antigens on formalin-fixed, paraffin-embedded canine tumors. Vet. Pathol. 1994, 31, 455–461. [Google Scholar] [CrossRef] [Green Version]
- Oliver, J.L., 3rd; Wolfe, L.G. Antigen expression in canine tissues, recognized by a monoclonal antibody generated against canine melanoma cells. Am. J. Vet. Res. 1992, 53, 123–128. [Google Scholar]
- Smedley, R.C.; Spangler, W.L.; Esplin, D.G.; Kitchell, B.E.; Bergman, P.J.; Ho, H.Y.; Bergin, I.L.; Kiupel, M. Prognostic markers for canine melanocytic neoplasms: A comparative review of the literature and goals for future investigation. Vet. Pathol. 2011, 48, 54–72. [Google Scholar] [CrossRef]
- Tanaka, N.; Mimura, M.; Ichinose, S.; Odajima, T. Malignant melanoma in the oral region: Ultrastructural and immunohistochemical studies. Med. Electron. Microsc. 2001, 34, 198–205. [Google Scholar] [CrossRef]
- Brockley, L.K.; Cooper, M.A.; Bennett, P.F. Malignant melanoma in 63 dogs (2001–2011): The effect of carboplatin chemotherapy on survival. N. Z. Vet. J. 2013, 61, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Cancedda, S.; Rohrer Bley, C.; Aresu, L.; Dacasto, M.; Leone, V.F.; Pizzoni, S.; Gracis, M.; Marconato, L. Efficacy and side effects of radiation therapy in comparison with radiation therapy and temozolomide in the treatment of measurable canine malignant melanoma. Vet. Comp. Oncol. 2016, 14, e146–e157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawabe, M.; Mori, T.; Ito, Y.; Murakami, M.; Sakai, H.; Yanai, T.; Maruo, K. Outcomes of dogs undergoing radiotherapy for treatment of oral malignant melanoma: 111 cases (2006–2012). J. Am. Vet. Med. Assoc. 2015, 247, 1146–1153. [Google Scholar] [CrossRef] [PubMed]
- Boria, P.A.; Murry, D.J.; Bennett, P.F.; Glickman, N.W.; Snyder, P.W.; Merkel, B.L.; Schlittler, D.L.; Mutsaers, A.J.; Thomas, R.M.; Knapp, D.W. Evaluation of cisplatin combined with piroxicam for the treatment of oral malignant melanoma and oral squamous cell carcinoma in dogs. J. Am. Vet. Med. Assoc. 2004, 224, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Rassnick, K.M.; Ruslander, D.M.; Cotter, S.M.; Al-Sarraf, R.; Bruyette, D.S.; Gamblin, R.M.; Meleo, K.A.; Moore, A.S. Use of carboplatin for treatment of dogs with malignant melanoma: 27 cases (1989–2000). J. Am. Vet. Med. Assoc. 2001, 218, 1444–1448. [Google Scholar] [CrossRef] [PubMed]
- Dank, G.; Rassnick, K.M.; Sokolovsky, Y.; Garrett, L.D.; Post, G.S.; Kitchell, B.E.; Sellon, R.K.; Kleiter, M.; Northrup, N.; Segev, G. Use of adjuvant carboplatin for treatment of dogs with oral malignant melanoma following surgical excision. Vet. Comp. Oncol. 2014, 12, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Mihajlovic, M.; Vlajkovic, S.; Jovanovic, P.; Stefanovic, V. Primary mucosal melanomas: A comprehensive review. Int. J. Clin. Exp. Pathol. 2012, 5, 739–753. [Google Scholar] [PubMed]
- Thompson, L.D.R.; Wieneke, J.A.; Miettinen, M. Sinonasal tract and nasopharyngeal melanomas: A clinicopathologic study of 115 cases with a proposed staging system. Am. J. Surg. Pathol. 2003, 27, 594–611. [Google Scholar] [CrossRef] [PubMed]
- Lerner, B.A.; Stewart, L.A.; Horowitz, D.P.; Carvajal, R.D. Mucosal Melanoma: New Insights and Therapeutic Options for a Unique and Aggressive Disease. Oncology 2017, 31, e23–e32. [Google Scholar]
- Shoushtari, A.N.; Bluth, M.J.; Goldman, D.A.; Bitas, C.; Lefkowitz, R.A.; Postow, M.A.; Munhoz, R.R.; Buchar, G.; Hester, R.H.; Romero, J.A.; et al. Clinical features and response to systemic therapy in a historical cohort of advanced or unresectable mucosal melanoma. Melanoma Res. 2017, 27, 57–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman-Keller, M.; Weber, J.S. Anti-programmed death receptor 1 immunotherapy in melanoma: Rationale, evidence and clinical potential. Ther. Adv. Med. Oncol. 2015, 7, 12–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacEwen, E.G.; Kurzman, I.D.; Vail, D.M.; Dubielzig, R.R.; Everlith, K.; Madewell, B.R.; Rodriguez, C.O.; Phillips, B., Jr.; Zwahlen, C.H.; Obradovich, J.; et al. Adjuvant therapy for melanoma in dogs: Results of randomized clinical trials using surgery, liposome-encapsulated muramyl tripeptide, and granulocyte macrophage colony-stimulating factor. Clin. Cancer Res. 1999, 5, 4249–4258. [Google Scholar]
- Bergman, P.J.; McKnight, J.; Novosad, A.; Charney, S.; Farrelly, J.; Craft, D.; Wulderk, M.; Jeffers, Y.; Sadelain, M.; Hohenhaus, A.E.; et al. Long-term survival of dogs with advanced malignant melanoma after DNA vaccination with xenogeneic human tyrosinase: A phase I trial. Clin. Cancer Res. 2003, 9, 1284–1290. [Google Scholar] [PubMed]
- Ottnod, J.M.; Smedley, R.C.; Walshaw, R.; Hauptman, J.G.; Kiupel, M.; Obradovich, J.E. A retrospective analysis of the efficacy of Oncept vaccine for the adjunct treatment of canine oral malignant melanoma. Vet. Comp. Oncol. 2013, 11, 219–229. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Wolchok, J.D.; Hodi, F.S.; Hamid, O.; Kefford, R.; Weber, J.S.; Joshua, A.M.; Hwu, W.J.; Gangadhar, T.C.; et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: A randomised dose-comparison cohort of a phase 1 trial. Lancet 2014, 384, 1109–1117. [Google Scholar] [CrossRef]
- Topalian, S.L.; Sznol, M.; McDermott, D.F.; Kluger, H.M.; Carvajal, R.D.; Sharfman, W.H.; Brahmer, J.R.; Lawrence, D.P.; Atkins, M.B.; Powderly, J.D.; et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 2014, 32, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- MacEwen, E.G.; Patnaik, A.K.; Harvey, H.J.; Hayes, A.A.; Matus, R. Canine Oral Melanoma: Comparison of Surgery Versus Surgery Plus Corynebacterium parvum. Cancer Investig. 1986, 4, 397–402. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| T: Primary Tumor |
| T0—No evidence of tumor |
| T1—Tumor < 2 cm maximum diameter |
| T2—Tumor 2–4 cm maximum diameter |
| T3—Tumor > 4 cm maximum diameter |
| N: regional Lymph node |
| N0—No evidence of regional involvement |
| N1—Movable ipsilateral nodes |
| N2—Movable contralateral or bilateral nodes |
| N3—Fixed nodes |
|
|
| M: distant metastasis |
|---|
| M0—No evidence of distant metastasis |
| M1—Distant metastasis (including distant nodes) |
| Stage grouping |
| Stage I—T1 N0 M0 |
| Stage II—T2 N0 M0 |
| Stage III—T2 N1 M0 or T3 N0 M0 |
| Stage IV—Any T, any N and M1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, W.S.; Vinayak, A.; Powers, B. Comparative Review of Malignant Melanoma and Histologically Well-Differentiated Melanocytic Neoplasm in the Oral Cavity of Dogs. Vet. Sci. 2021, 8, 261. https://doi.org/10.3390/vetsci8110261
Kim WS, Vinayak A, Powers B. Comparative Review of Malignant Melanoma and Histologically Well-Differentiated Melanocytic Neoplasm in the Oral Cavity of Dogs. Veterinary Sciences. 2021; 8(11):261. https://doi.org/10.3390/vetsci8110261
Chicago/Turabian StyleKim, Won Suk, Arathi Vinayak, and Barbara Powers. 2021. "Comparative Review of Malignant Melanoma and Histologically Well-Differentiated Melanocytic Neoplasm in the Oral Cavity of Dogs" Veterinary Sciences 8, no. 11: 261. https://doi.org/10.3390/vetsci8110261
APA StyleKim, W. S., Vinayak, A., & Powers, B. (2021). Comparative Review of Malignant Melanoma and Histologically Well-Differentiated Melanocytic Neoplasm in the Oral Cavity of Dogs. Veterinary Sciences, 8(11), 261. https://doi.org/10.3390/vetsci8110261