Immunofluorescent Localization of Plakoglobin Is Altered in Endomyocardial Biopsy Samples from Dogs with Clinically Relevant Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)

 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Endomyocardial Biopsies
2.3. Sample Preparation
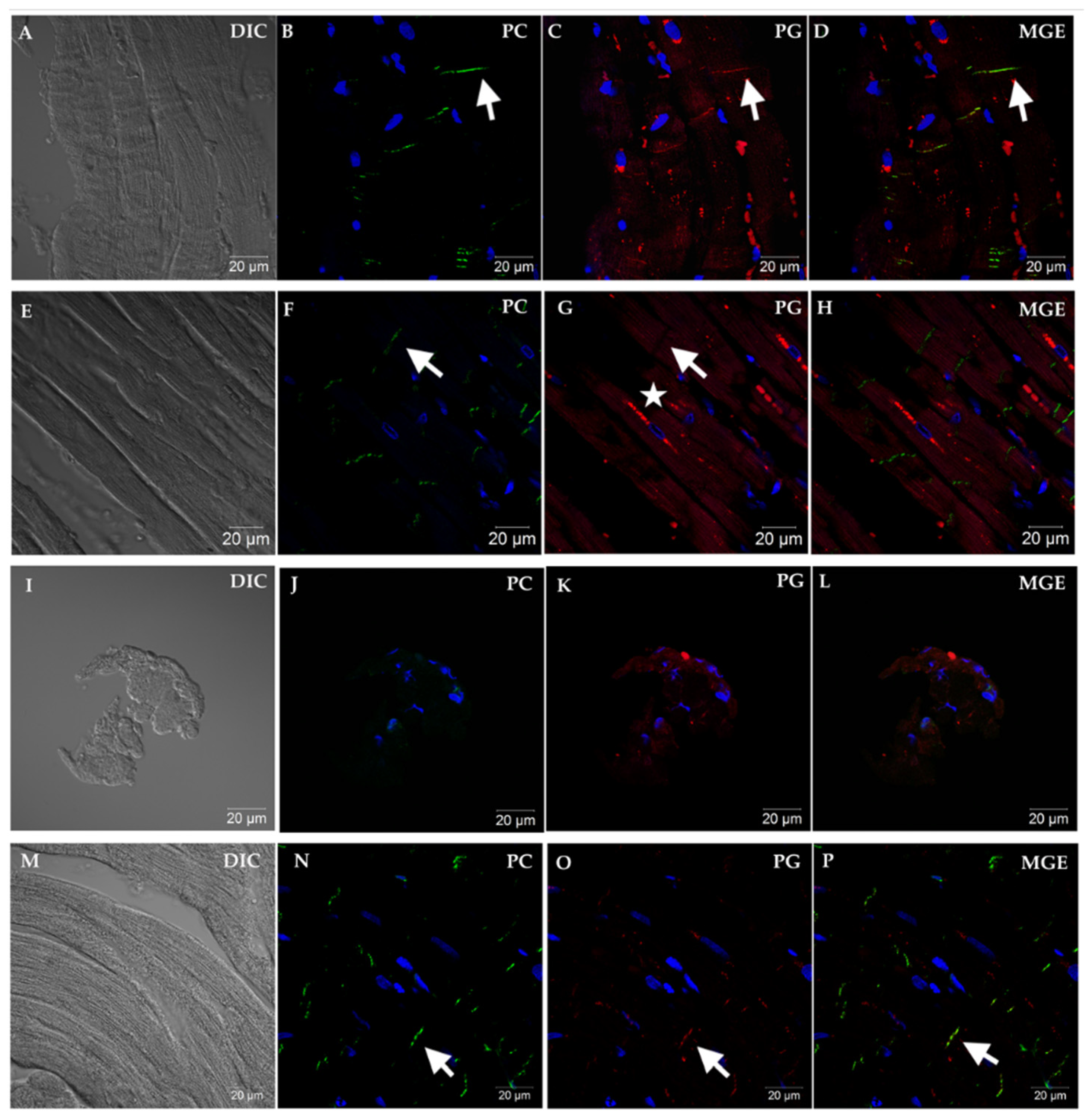
2.4. Confocal Microscopy
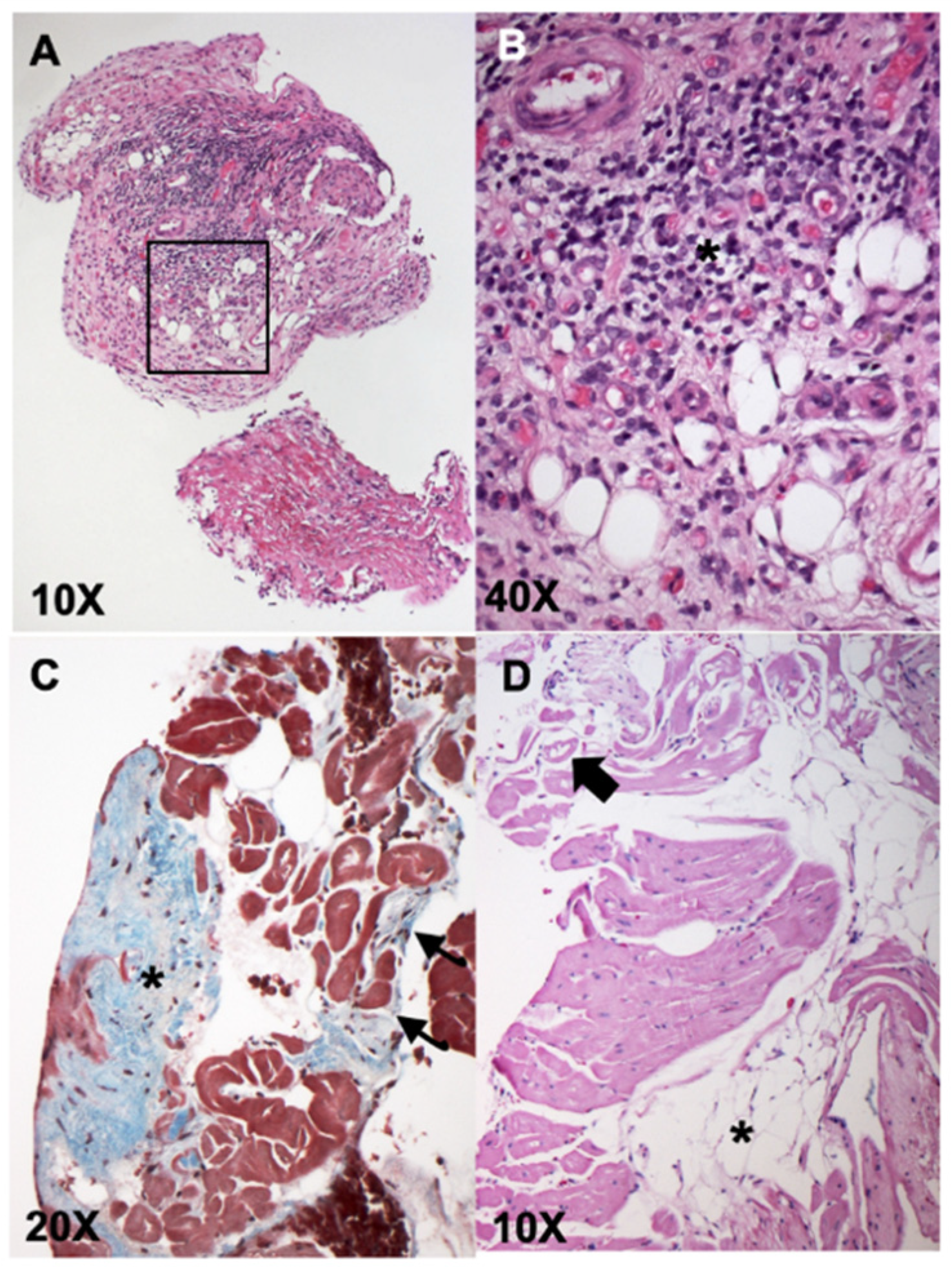
2.5. Histopathology
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Basso, C.; Fox, P.R.; Meurs, K.M.; Towbin, J.A.; Spier, A.W.; Calabrese, F.; Maron, B.J.; Thiene, G. Arrhythmogenic right ventricular cardiomyopathy causing sudden cardiac death in boxer dogs: A new animal model of human disease. Circulation 2004, 109, 1180–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham, S.M.; Sweeney, J.T.; MacGregor, J.; Barton, B.A.; Rush, J.E. Clinical Features of English Bulldogs with Presumed Arrhythmogenic Right Ventricular Cardiomyopathy: 31 Cases (2001–2013). J. Am. Anim. Hosp. Assoc. 2018, 54, 95–102. [Google Scholar] [CrossRef]
- Santilli, R.A.; Bontempi, L.V.; Perego, M. Ventricular tachycardia in English bulldogs with localised right ventricular outflow tract enlargement. J. Small Anim. Pract. 2011, 52, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Santilli, R.A.; Bontempi, L.V.; Perego, M.; Fornai, L.; Basso, C. Outflow tract segmental arrhythmogenic right ventricular cardiomyopathy in an English Bulldog. J. Vet. Cardiol. 2009, 11, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Basso, C.; Thiene, G.; McKenna, W.J.; Davies, M.J.; Fontaliran, F.; Nava, A.; Silvestri, F.; Blomstrom-Lundqvist, C.; Wlodarska, E.K.; et al. Spectrum of clinicopathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia: A multicenter study. J. Am. Coll. Cardiol. 1997, 30, 1512–1520. [Google Scholar] [CrossRef] [Green Version]
- Oxford, E.M.; Everitt, M.; Coombs, W.; Fox, P.R.; Kraus, M.; Gelzer, A.R.; Saffitz, J.; Taffet, S.M.; Moïse, N.S.; Delmar, M. Molecular composition of the intercalated disc in a spontaneous canine animal model of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Heart Rhythm. 2007, 4, 1196–1205. [Google Scholar] [CrossRef] [Green Version]
- Vila, J.; Pariaut, R.; Moïse, N.S.; Oxford, E.M.; Fox, P.R.; Reynolds, C.A.; Saelinger, C. Structural and molecular pathology of the atrium in boxer arrhythmogenic right ventricular cardiomyopathy. J. Vet. Cardiol. 2017, 19, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Spier, A.W.; Meurs, K.M. Evaluation of spontaneous variability in the frequency of ventricular arrhythmias in Boxers with arrhythmogenic right ventricular cardiomyopathy. J. Am. Vet. Med. Assoc. 2004, 224, 538–541. [Google Scholar] [CrossRef]
- Meurs, K.M.; Mauceli, E.; Lahmers, S.; Acland, G.M.; White, S.N.; Lindblad-Toh, K. Genome-wide association identifies a deletion in the 3′ untranslated region of striatin in a canine model of arrhythmogenic right ventricular cardiomyopathy. Hum. Genet. 2010, 128, 315–324. [Google Scholar] [CrossRef] [Green Version]
- Meurs, K.M.; Stern, J.A.; Sisson, D.D.; Kittleson, M.D.; Cunningham, S.M.; Ames, M.K.; Atkins, C.E.; DeFrancesco, T.; Hodge, T.E.; Keene, B.W.; et al. Association of dilated cardiomyopathy with the striatin mutation genotype in boxer dogs. J. Vet. Intern. Med. 2013, 27, 1437–1440. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, D.; Fatah, M.; Akdis, D.; Spears, D.A.; Koopmann, T.T.; Mittal, K.; Rafiq, M.A.; Cattanach, B.M.; Zhao, Q.; Healey, J.S.; et al. An autoantibody identifies arrhythmogenic right ventricular cardiomyopathy and participates in its pathogenesis. Eur. Heart J. 2018, 39, 3932–3944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, F.I.; McKenna, W.J.; Sherrill, D.; Basso, C.; Bauce, B.; Bluemke, D.A.; Calkins, H.; Corrado, D.; Cox, M.G.; Daubert, J.P.; et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: Proposed modification of the task force criteria. Circulation 2010, 121, 1533–1541. [Google Scholar] [CrossRef] [PubMed]
- Oxford, E.M.; Danko, C.G.; Kornreich, B.G.; Maass, K.; Hemsley, S.A.; Raskolnikov, D.; Fox, P.R.; Delmar, M.; Moïse, N.S. Ultrastructural changes in cardiac myocytes from boxer dogs with arrhythmogenic right ventricular cardiomyopathy. J. Vet. Cardiol. 2011, 13, 101–113. [Google Scholar] [CrossRef] [Green Version]
- Femia, G.; Hsu, C.; Singarayar, S.; Sy, R.W.; Kilborn, M.; Parker, G.; McGuire, M.; Semsarian, C.; Puranik, R. Impact of new task force criteria in the diagnosis of arrhythmogenic right ventricular cardiomyopathy. Int. J. Cardiol. 2014, 171, 179–183. [Google Scholar] [CrossRef]
- Kaplan, S.R.; Gard, J.J.; Carvajal-Huerta, L.; Ruiz-Cabezas, J.C.; Thiene, G.; Saffitz, J.E. Structural and molecular pathology of the heart in Carvajal syndrome. Cardiovasc. Pathol. 2004, 13, 26–32. [Google Scholar] [CrossRef]
- Kaplan, S.R.; Gard, J.J.; Protonotarios, N.; Tsatsopoulou, A.; Spiliopoulou, C.; Anastasakis, A.; Squarcioni, C.P.; McKenna, W.J.; Thiene, G.; Basso, C.; et al. Remodeling of myocyte gap junctions in arrhythmogenic right ventricular cardiomyopathy due to a deletion in plakoglobin (Naxos disease). Heart Rhythm. 2004, 1, 3–11. [Google Scholar] [CrossRef]
- Asimaki, A.; Tandri, H.; Huang, H.; Halushka, M.K.; Gautam, S.; Basso, C.; Thiene, G.; Tsatsopoulou, A.; Protonotarios, N.; McKenna, W.J.; et al. A new diagnostic test for arrhythmogenic right ventricular cardiomyopathy. N. Engl. J. Med. 2009, 360, 1075–1084. [Google Scholar] [CrossRef]
- Asimaki, A.; Saffitz, J.E. The role of endomyocardial biopsy in ARVC: Looking beyond histology in search of new diagnostic markers. J. Cardiovasc. Electrophysiol. 2011, 22, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Gomes, J.; Finlay, M.; Ahmed, A.K.; Ciaccio, E.J.; Asimaki, A.; Saffitz, J.E.; Quarta, G.; Nobles, M.; Syrris, P.; Chaubey, S.; et al. Electrophysiological abnormalities precede overt structural changes in arrhythmogenic right ventricular cardiomyopathy due to mutations in desmoplakin -a combined murine and human study. Eur. Heart J. 2012, 33, 1942–1953. [Google Scholar] [CrossRef] [Green Version]
- Santilli, R.A.; Grego, E.; Battaia, S.; Gianella, P.; Tursi, M.; Di Girolamo, N.; Biasato, I.; Perego, M. Prevalence of selected cardiotropic pathogens in the myocardium of adult dogs with unexplained myocardial and rhythm disorders or with congenital heart disease. J. Am. Vet. Med. Assoc. 2019, 255, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- Oxford, E.M.; Danko, C.G.; Fox, P.R.; Kornreich, B.; Moïse, N. Change in β-catenin localization suggests involvement of the canonical Wnt pathway in Boxer dogs with arrhythmogenic right ventricular cardiomyopathy. J. Vet. Intern. Med. 2014, 28, 92–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Chen, L.; Chen, Z.; Song, J. Remodelling of myocardial intercalated disc protein connexin 43 causes increased susceptibility to malignant arrhythmias in ARVC/D patients. Forensic Sci. Int. 2017, 275, 14–22. [Google Scholar] [CrossRef]
- Cerrone, M.; Agullo-Pascual, E.; Delmar, M. The Intercalated Disc: A molecular network that integrates electrical coupling, intercellular adhesion, and cell excitability. In Cardiac Electrophysiology: From Cell to Bedside, 6th ed.; Zipes, D.P., Jalife, J., Eds.; Elsevier: St. Louis, MO, USA, 2013; pp. 215–227. [Google Scholar]
- Basso, C.; Ronco, F.; Marcus, F.; Abudureheman, A.; Rizzo, S.; Frigo, A.C.; Bauce, B.; Maddalena, F.; Nava, A.; Corrado, D.; et al. Quantitative assessment of endomyocardial biopsy in arrhythmogenic right ventricular cardiomyopathy/dysplasia: An in vitro validation of diagnostic criteria. Eur. Heart J. 2008, 29, 2760–2771. [Google Scholar] [CrossRef]
- Wagner, J.P. The Boxer, 1st ed.; Orange Judd: Chicago, IL, USA, 1947. [Google Scholar]
- Campuzano, O.; Alcalde, M.; Iglesias, A.; Barahona-Dussault, C.; Sarquella-Brugada, G.; Benito, B.; Arzamendi, D.; Flores, J.; Leung, T.K.; Talajic, M.; et al. Arrhythmogenic right ventricular cardiomyopathy: Severe structural alterations are associated with inflammation. J. Clin. Pathol. 2012, 65, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Eason, B.D.; Leach, S.B.; Kuroki, K. Arrhythmogenic right ventricular cardiomyopathy in a weimaraner. Can. Vet. J. 2015, 56, 1035–1039. [Google Scholar] [PubMed]
- Nakao, S.; Hirakawa, A.; Yamamoto, S.; Kobayashi, M.; Machida, N. Pathologic features of arrhythmogenic right ventricular cardiomyopathy in middle-aged dogs. J. Vet. Med. Sci. 2011, 73, 1031–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bright, J.M.; McEntee, M. Isolated right ventricular cardiomyopathy in a dog. J. Am. Vet. Med. Assoc. 1995, 207, 64–66. [Google Scholar]
- Mohr, A.J.; Kirberger, R.M. Arrhythmogenic right ventricular cardiomyopathy in a dog. J. S. Afr. Vet. Assoc. 2000, 71, 125–130. [Google Scholar] [CrossRef] [Green Version]
- Simpson, K.W.; Bonagura, J.D.; Eaton, K.A. Right ventricular cardiomyopathy in a dog. J. Vet. Intern. Med. 1994, 8, 306–309. [Google Scholar] [CrossRef]
- Fernandez del Palacio, M.J.; Bernal, L.J.; Bayon, A.; Bernabé, A.; De Oca, R.M.; Seva, J. Arrhythmogenic right ventricular dysplasia/cardiomyopathy in a Siberian husky. J. Small Anim. Pract. 2001, 42, 137–142. [Google Scholar] [CrossRef]
- Steinberg, D.M.; Fine, J.; Chappell, R. Sample size for positive and negative predictive value in diagnostic research using case-control designs. Biostatistics 2009, 10, 94–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oxford, E.M.; Pariaut, R.; Tursi, M.; Fox, P.R.; Santilli, R.A. Immunofluorescent Localization of Plakoglobin Is Altered in Endomyocardial Biopsy Samples from Dogs with Clinically Relevant Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC). Vet. Sci. 2021, 8, 248. https://doi.org/10.3390/vetsci8110248
Oxford EM, Pariaut R, Tursi M, Fox PR, Santilli RA. Immunofluorescent Localization of Plakoglobin Is Altered in Endomyocardial Biopsy Samples from Dogs with Clinically Relevant Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC). Veterinary Sciences. 2021; 8(11):248. https://doi.org/10.3390/vetsci8110248
Chicago/Turabian StyleOxford, Eva M., Romain Pariaut, Massimiliano Tursi, Philip R. Fox, and Roberto A. Santilli. 2021. "Immunofluorescent Localization of Plakoglobin Is Altered in Endomyocardial Biopsy Samples from Dogs with Clinically Relevant Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)" Veterinary Sciences 8, no. 11: 248. https://doi.org/10.3390/vetsci8110248
APA StyleOxford, E. M., Pariaut, R., Tursi, M., Fox, P. R., & Santilli, R. A. (2021). Immunofluorescent Localization of Plakoglobin Is Altered in Endomyocardial Biopsy Samples from Dogs with Clinically Relevant Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC). Veterinary Sciences, 8(11), 248. https://doi.org/10.3390/vetsci8110248