
Influence of Morphometry on Echocardiographic Measurements in Cavalier King Charles Spaniels: An Inverse Probability Weighting Analysis

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population, Research Question and Statistical Framework
2.2. Inclusion Criteria and Clinical Examination
2.3. Echocardiography and Assessment of Leaflet Measurements, MVP Severity and Jet Size
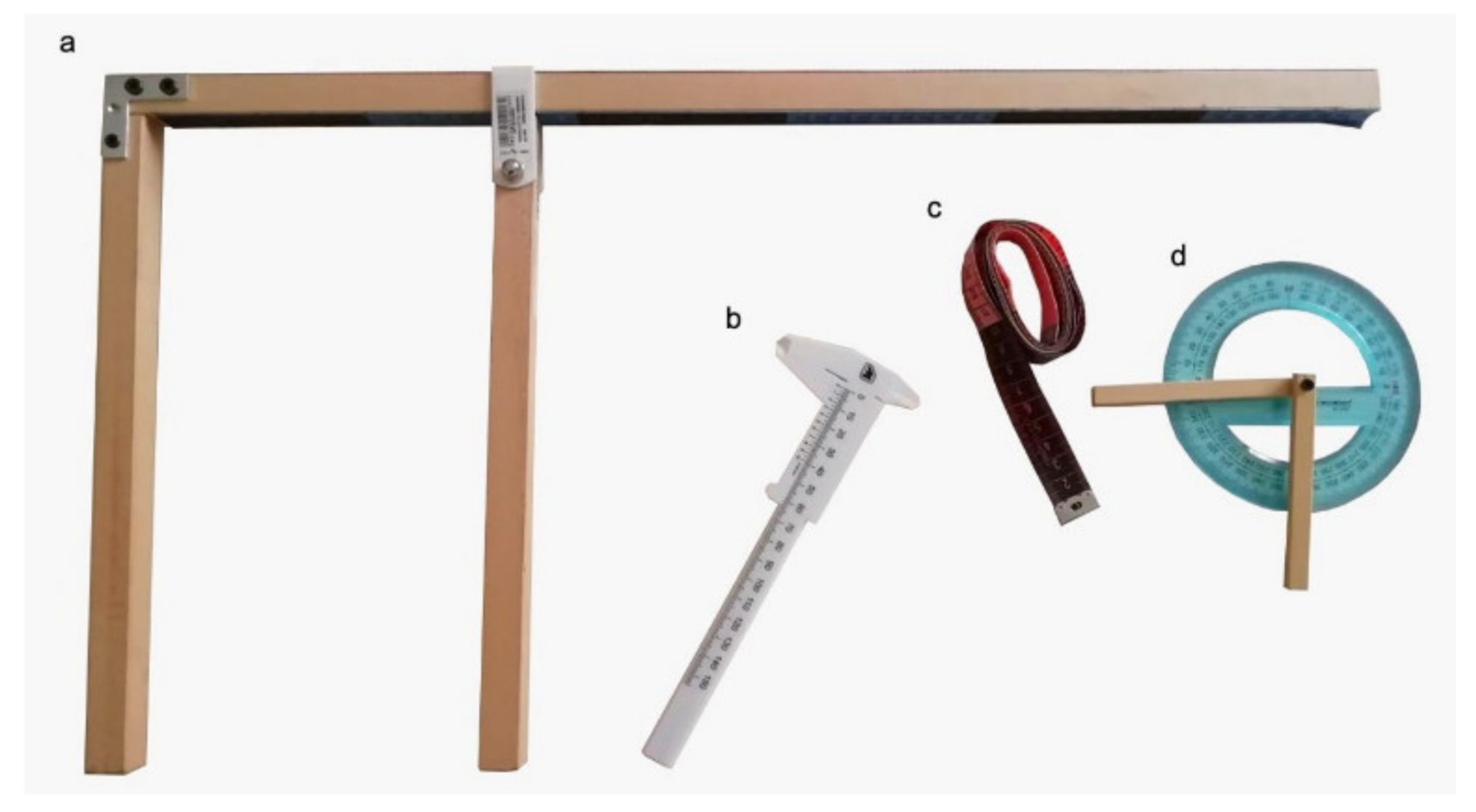
2.4. Morphometrics
2.5. Exclusion Criteria
2.6. Statistical Methods
3. Results
3.1. Clinical and Echocardiographic Results
3.2. Morphometric Measurements
3.3. Settings for IPW Analysis
3.4. IPW Analyses for Ordinal Variables
3.5. IPW Analyses for Continuous Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Detweiler, D.K.; Patterson, D.F. The prevalence and types of cardiovascular disease in dogs. Ann. N. Y. Acad. Sci 1965, 127, 481–516. [Google Scholar] [CrossRef] [PubMed]
- Swenson, L.; Häggström, J.; Kvart, C.; Juneja, R.K. Relationship between parental cardiac status in cavalier king Charles spaniels and prevalence and severity of chronic valvular disease in offspring. J. Am. Vet. Med. Assoc. 1996, 208, 2009–2012. [Google Scholar] [PubMed]
- Olsen, L.H.; Fredholm, M.; Pedersen, H.D. Epidemiology and Inheritance of Mitral Valve Prolapse in Dachshunds. J. Vet. Intern. Med. 1999, 13, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Madsen, M.B.; Olsen, L.H.; Häggström, J.; Höglund, K.; Ljungvall, I.; Falk, T.; Wess, G.; Stephenson, H.; Dukes-McEwan, J.; Chetboul, V.; et al. Identification of 2 loci associated with development of myxomatous mitral valve disease in cavalier king Charles spaniels. J. Hered. 2011, 102, S62–S67. [Google Scholar] [CrossRef] [PubMed]
- Lewis, T.; Swift, S.; Woolliams, J.A.; Blott, S. Heritability of premature mitral valve disease in cavalier king Charles spaniels. Vet. J. 2011, 188, 73–76. [Google Scholar] [CrossRef]
- Birkegard, A.C.; Reimann, M.J.; Martinussen, T.; Häggström, J.; Pedersen, H.D.; Olsen, L.H. Breeding restrictions decrease the prevalence of myxomatous mitral valve disease in cavalier king Charles spaniels over an 8- to 10-year period. J. Vet. Intern. Med. 2016, 30, 63–68. [Google Scholar] [CrossRef]
- Parker, H.G.; Kilroy-Glynn, P. Myxomatous mitral valve disease in dogs: Does size matter? J. Vet. Cardiol. 2012, 14, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Thrusfield, M.V.; Aikten, C.G.G.; Darke, P.G.G. Observations on breed and sex in relation to canine heart valve incompetence. J. Small Anim. Pract. 1985, 26, 709–717. [Google Scholar] [CrossRef]
- Pedersen, H.D.; Lorentzen, K.A.; Kristensen, B.Ø. Echocardiographic mitral valve prolapse in Cavalier King Charles Spaniels: Epidemiology and prognostic significance for regurgitation. Vet. Rec. 1999, 144, 315–320. [Google Scholar] [CrossRef]
- Egenvall, A.; Bonnett, B.N.; Häggström, J. Heart disease as a cause of death in insured Swedish dogs younger than 10 years of age. J. Vet. Intern. Med. 2006, 20, 894–903. [Google Scholar] [CrossRef]
- Darke, P.G. Valvular incompetence in cavalier king Charles spaniels. Vet. Rec. 1987, 120, 365–366. [Google Scholar] [CrossRef]
- Borgarelli, M.; Savarino, P.; Crosara, S.; Santilli, R.A.; Chiavegato, D.; Poggi, M.; Bellino, C.; La Rosa, G.; Zanatta, R.; Haggstrom, J. Survival characteristics and prognostic variables of dogs with mitral regurgitation attributable to myxomatous valve disease. J. Vet. Intern. Med. 2008, 22, 120–128. [Google Scholar] [CrossRef]
- Atkins, C.; Bonagura, J.; Ettinger, S.; Fox, P.; Gordon, S.; Haggstrom, J.; Hamlin, R.; Keene, B.; Luis-Fuentes, V.; Stepien, R. Guidelines for the diagnosis and treatment of canine chronic valvular heart disease. J. Vet. Intern. Med. 2009, 23, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Keene, B.W.; Atkins, C.E.; Bonagura, J.D.; Fox, P.R.; Häggström, J.; Fuentes, V.L.; Oyama, M.A.; Rush, J.E.; Stepien, R.; Uechi, M. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J. Vet. Intern. Med. 2019, 33, 1127–1140. [Google Scholar] [CrossRef] [PubMed]
- Bagardi, M.; Bionda, A.; Locatelli, C.; Cortellari, M.; Frattini, S.; Negro, A.; Crepaldi, P.; Brambilla, P.G. Echocardiographic Evaluation of the Mitral Valve in Cavalier King Charles Spaniels. Animals 2020, 10, 1895. [Google Scholar] [CrossRef] [PubMed]
- Hernán, M.A.; Robins, J.M. Causal Inference: What If, 1st ed.; Taylor & Francis Inc.: Abingdon, UK, 2020. [Google Scholar]
- Cole, S.R.; Hernán, M.A. Constructing inverse probability weights for marginal structural models. Am. J. Epidemiol. 2008, 168, 656–664. [Google Scholar] [CrossRef]
- Williams, J.R.; Crespi, C.M. Causal inference for multiple continuous exposures via the multivariate generalized propensity score. arXiv 2020, arXiv:2008.13767v1. [Google Scholar]
- Rishniw, M. Murmur grading in humans and animals: Past and present. J. Vet. Cardiol. 2018, 20, 223–233. [Google Scholar] [CrossRef]
- Acierno, M.J.; Brown, S.; Coleman, A.E.; Jepson, R.E.; Papich, M.; Stepien, R.L.; Syme, H.M. ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J. Vet. Intern. Med. 2018, 32, 1803–1822. [Google Scholar] [CrossRef]
- Stepien, R.L.; Rapoport, G.S.; Henik, R.A.; Wenholz, L.; Thomas, C.B. Comparative diagnostic test characteristics of oscillometric and Doppler ultrasonographic methods in the detection of systolic hypertension in dogs. J. Vet. Intern. Med. 2003, 17, 65–72. [Google Scholar] [CrossRef]
- Thomas, W.P.; Gaber, C.E.; Jacobs, G.J.; Kaplan, P.M.; Lombard, C.W.; Moise, N.S.; Moses, B.L. Recommendations for standards in transthoracic two-dimensional echocardiography in the dog and cat. J. Vet. Intern. Med. 1993, 7, 247–252. [Google Scholar] [CrossRef]
- Wesselowski, S.R.; Borgarelli, M.; Menciotti, G.; Abbott, J. Echocardiographic anatomy of the mitral valve in healthy dogs and dogs with myxomatous mitral valve disease. J. Vet. Cardiol. 2015, 17, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Terzo, E.; Di Marcello, M.; McAllister, H.; Glazier, B.; Coco, D.L.; Locatelli, C.; Palermo, V.; Brambilla, P.G. Echocardiographic assessment of 537 dogs with mitral valve prolapse and leaflet involvement. Vet. Radiol. Ultrasound 2009, 50, 416–422. [Google Scholar] [CrossRef]
- Dukes-McEwan, J.; Borgarelli, M.; Tidholm, A.; Vollmar, C.; Häggström, J.; ESVC Taskforce for Canine Dilated Cardiomyopathy. Proposed guidelines for the diagnosis of canine idiopathic dilated cardiomyopathy. J. Vet. Cardiol. 2003, 5, 7–19. [Google Scholar] [CrossRef]
- Wess, G.; Domenech, O.; Dukes-McEwan, J.; Häggström, J.; Gordon, S. European Society of Veterinary Cardiology screening guidelines for dilated cardiomyopathy in Doberman Pinschers. J. Vet. Cardiol. 2017, 19, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Teichholz, L.E.; Kreulen, T.; Herman, M.V.; Gorlin, R. Problems in echocardiographic volume determinations: Echocardiographic-angiographic correlations in the presence or absence of asynergy. Am. J. Cardiol. 1976, 37, 7–11. [Google Scholar] [CrossRef]
- Cornell, C.C.; Kittleson, M.D.; Della Torre, P.; Häggström, J.; Lombard, C.W.; Pedersen, H.D.; Vollmar, A.; Wey, A. Allometric scaling of M-mode cardiac measurements in normal adult dogs. J. Vet. Intern. Med. 2004, 18, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Hansson, K.; Häggström, J.; Kvart, C.; Lord, P. Left atrial to aortic root indices using two-dimensional and M-mode echocardiography in cavalier King Charles spaniels with and without left atrial enlargement. Vet. Radiol. Ultrasound 2002, 43, 568–575. [Google Scholar] [CrossRef]
- Larouche-Lebel, E.; Loughran, K.A.; Oyama, M.A. Echocardiographic indices and severity of mitral regurgitation in dogs with preclinical degenerative mitral valve disease. J. Vet. Intern. Med. 2019, 33, 489–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rishniw, M.; Caivano, D.; Dickson, D.; Vatne, L.; Harris, J.; Matos, J.N. Two-dimensional echocardiographic left- atrial-to-aortic ratio in healthy adult dogs: A reexamination of reference intervals. J. Vet. Cardiol. 2019, 26, 29–38. [Google Scholar] [CrossRef]
- Chetboul, V.; Tissier, R. Echocardiographic assessment of canine degenerative mitral valve disease. J. Vet. Cardiol. 2012, 14, 127–148. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Stern, J.A.; Hsue, W.; Song, K.H.; Ontiveros, E.S.; Fuentes, V.L.; Stepien, R.L. Severity of mitral valve degeneration is associated with chromosome 15 loci in whippet dogs. PLoS ONE 2015, 10, e0141234. [Google Scholar]
- Häggström, J.; Hansson, K.; Kvart, C.; Swenson, L. Chronic valvular disease in the cavalier king Charles spaniel in Sweden. Vet. Rec. 1992, 131, 549–553. [Google Scholar]
- Canton, M. Dogs and Dog Breeds, Volume II, 2nd ed.; Antonio Crepaldi Editore: Porto Viro, Italy, 2011. [Google Scholar]
- Packer, R.M.A.; Hendricks, A.; Tivers, M.S.; Burn, C.C. Impact of Facial Conformation on Canine Health: Brachycephalic Obstructive Airway Syndrome. PLoS ONE 2015, 10, e0137496. [Google Scholar]
- Liu, N.C.; Troconis, E.L.; Kalmar, L.; Price, D.J.; Wright, H.E.; Adams, V.J.; Sargan, D.R.; Ladlow, J.R. Conformational risk factors of brachycephalic obstructive airway syndrome (BOAS) in pugs, French bulldogs, and bulldogs. PLoS ONE 2017, 12, e0181928. [Google Scholar] [CrossRef] [Green Version]
- WSAVA Nutritional Assessment Guidelines Task Force Members. WSAVA nutritional assessment guidelines. J. Feline Med. Surg. 2011, 13, 516–525. [Google Scholar] [CrossRef]
- Robins, J.M.; Hernán, M.A.; Brumback, B. Marginal Structural Models and Causal Inference in Epidemiology. Epidemiology 2000, 11, 550–560. [Google Scholar] [CrossRef]
- Lumley, T. Analysis of Complex Survey Samples. J. Stat. Softw. 2004, 9, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, M.; Wing, J.; Weston, S.; Williams, A.; Keefer, C.; Engelhardt, A.; Cooper, T.; Mayer, Z.; Kenkel, B.; Team, R.C.; et al. caret: Classification and Regression Training. 20 March 2020. Available online: https://cran.r-project.org/package=caret (accessed on 4 March 2021).
- Greenwell, B.; McCarthy, A.; Boehmke, B.; Liu, D. Sure: Surrogate Residuals for Ordinal and General Regression Models. 19 September 2017. Available online: https://cran.r-project.org/package=sure (accessed on 4 March 2021).
- Weisberg, S. Applied Linear Regression, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2005. [Google Scholar]
- R Core Team. The R Project for Statistical Computing. R Version 4.0.4 (Lost Library Book) [Software]. 15 February 2021. Available online: http://www.r-project.org/ (accessed on 4 March 2021).
- Bon Tempo, C.P.; Ronan, J.A.; de Leon, A.C.; Twigg, H.L. Radiographic appearance of the thorax in systolic click—Late systolic murmur syndrome. Am. J. Cardiol. 1975, 36, 27–31. [Google Scholar] [CrossRef]
- Zema, M.J.; Chiaramida, S.; DeFilipp, G.J.; Goldman, M.A.; Pizzarello, R.A. Somatotype and idiopathic mitral valve prolapse. Catheter. Cardiovasc. Diagn. 1982, 8, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Menciotti, G.; Franchini, A.; Jeong, H. Prevalence of Mitral Regurgitation in Cavalier King Charles Spaniels with No or Low-Grade Murmurs. In Proceedings of the ECVIM-CA Online Congress, Barcelona, Spain, 15 January 2020. [Google Scholar]
- Perry, G.J.; Bouchard, A. Doppler echocardiographic evaluation of mitral regurgitation. Cardiol. Clin. 1990, 8, 265–275. [Google Scholar] [CrossRef]
- Pedersen, H.D.; Häggström, J.; Falk, T.; Mow, T.; Olsen, L.H.; Iversen, L.; Jensen, A.L. Auscultation in mild mitral regurgitation in dogs: Observer variation, effects of physical maneuvers, and agreement with color Doppler echocardiography and phonocardiography. J. Vet. Intern. Med. 1999, 13, 56–64. [Google Scholar] [CrossRef]
- Menciotti, G.; Borgarelli, M.; Aherne, M.; Camacho, P.; Häggström, J.; Ljungvall, I.; Lahmers, S.M.; Abbott, J.A. Comparison of the mitral valve morphologies of Cavalier King Charles Spaniels and dogs of other breeds using 3Dtransthoracic echocardiography. J. Vet. Intern. Med. 2018, 32, 1564–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Body Measurements | Thorax Measurements | Head Measurements |
|---|---|---|
| Height at the withers (WH): distance of the withers from the ground, measured at the top of the shoulder blades. | Height (TH): distance between the back and the sternum, measured behind the shoulders. | Head length (HL): measured from the top of the occipital ridge to the horizontal line joining the two inner corners of the eyelids. |
| Body length (BL): distance between the tip of the shoulder and the tip of the buttock. | Width (TW): measured just behind the shoulders. | Nose length (NL): measured from the horizontal line joining the two inner corners of the eyelids to the cranial extremity of the truffle. |
| Width at the chest (CW): measured at the shoulder–humeral joints. | Length (TL): distance between the shoulder tip and the midline of the last rib. | Head + nose length (HNL): HL + NL. |
Circumference (TC1, TC2, TC3):
| Head width (HW): measured at the zygomatic arches. | |
| Head stop angle (HA): angle obtained, with the head seen in profile, by the intersection of a line tangent to the frontal region (between the two orbits) and the line of the upper part of the nasal barrel. | ||
| Body indexes | ||
| Cephalic index: (HW × 100)/HNL. | ||
| Craniofacial ratio (CFR): NL/HL. | ||
| Thoracic index: (TW × 100)/TH; height thorax index: (TH × 100)/WH. | ||
| Volume index: (body weight × 100)/WH. | ||
| Body size: (WH × 100)/BL. | ||
| (a) Clinical data, indexed mitral valve measurements, MVP, jet size, murmur severity, and score of severity | ||||||||||||
| Age (y) | Body weight (Kg) | Sex | AMVL (cm) | AMVW (cm) | AMVA (cm) | MVAd (cm) | MVAs (cm) | SI | MVP | Jet size | Heart murmur severity | Score of severity |
| 4.16 (2.91–6.00) | 9.15 *,† (7.80–10.23) | F (n.35) NF (n.5) M (n.11) NM (n.2) | 0.70 (0.63–0.79) | 0.14 (0.12–0.16) | 0.08 (0.06–0.11) | 0.78 (0.74–0.88) | 0.61 (0.55–0.66) | 1.37 (1.24–1.50) | 0 (n.1) 1 (n.31)2 (n.19)3 (n.1) | 0 (n.6) 1 (n.18) 2 (n.7) 3 (n.14)4 (n.7) | 0 (n.26) 1 (n.20) 2 (n.6) | 2.69 (2.01–3.45) |
| (b) Body and thoracic morphometric measurements | ||||||||||||
| Body morphometric measurements | Thoracic morphometric measurements | |||||||||||
| WH | BL | CW | TH | TW | TL | TC1 | TC2 | TC3 | ||||
| 29.20 (27.78–31.58) | 33.75 (29.70–35.85) | 12.25 (11.45–13.53) | 14.95 (13.58–16.13) | 11.95 (11.28–13.00) | 20.15 (18.68–22.10) | 47.00 (45.00–49.63) | 47.50 (46.00–50.63) | 45.50 (43.58–49.50) | ||||
| (c) Head morphometric measurements and physical data | ||||||||||||
| Head morphometric measurements | Physical data | |||||||||||
| HL | NL | HNL | HW | HA | Coat color type | BCS | ||||||
| 7.70 (7.20–8.13) | 3.20 (2.80–3.50) | 10.95 (10.20–11.85) | 7.75 (7.50–8.10) | 115.00 (110.00–120.00) | (n. 35) B (n. 4) B&T (n. 2) R (n. 11) T | (n. 6) 3 (n. 10) 4 (n. 26) 5 (n. 10) 6 | ||||||
| (d) Body indexes | ||||||||||||
| Cephalic index | Craniofacial ratio (CFR) | Thoracic index | Height thorax index | Volume index | Body size | |||||||
| 71.97 (68.08–75.50) | 0.40 (0.36–0.44) | 83.08 (75.54–86.83) | 0.5 (0.49–0.53) | 30.82 (25.97–34.31) | 88.40 (83.54–93.09) | |||||||
| Regression Analysis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| BL | TH | TW | TL | TC1 | TC2 | TC3 | HL | NL | HA | |
| a. Ordinal variables | ||||||||||
| MVP | ||||||||||
| Jet size | ** n | |||||||||
| Heart murmur intensity | * n | ** n | ||||||||
| b. Continuous variables | ||||||||||
| AMVL | * p | |||||||||
| AMVW | * p | * n | ||||||||
| AMVA | ||||||||||
| MVAd | * p | * n | *** p | *** n | *** p | * n | *** p | *** n | *** p | |
| MVAs | ** n | * p | *** p | |||||||
| SI | ** p | ** p | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagardi, M.; Ghilardi, S.; Locatelli, C.; Bionda, A.; Polli, M.; Bussadori, C.M.; Colombo, F.M.; Pazzagli, L.; Brambilla, P.G. Influence of Morphometry on Echocardiographic Measurements in Cavalier King Charles Spaniels: An Inverse Probability Weighting Analysis. Vet. Sci. 2021, 8, 205. https://doi.org/10.3390/vetsci8100205
Bagardi M, Ghilardi S, Locatelli C, Bionda A, Polli M, Bussadori CM, Colombo FM, Pazzagli L, Brambilla PG. Influence of Morphometry on Echocardiographic Measurements in Cavalier King Charles Spaniels: An Inverse Probability Weighting Analysis. Veterinary Sciences. 2021; 8(10):205. https://doi.org/10.3390/vetsci8100205
Chicago/Turabian StyleBagardi, Mara, Sara Ghilardi, Chiara Locatelli, Arianna Bionda, Michele Polli, Claudio M. Bussadori, Fabio M. Colombo, Laura Pazzagli, and Paola G. Brambilla. 2021. "Influence of Morphometry on Echocardiographic Measurements in Cavalier King Charles Spaniels: An Inverse Probability Weighting Analysis" Veterinary Sciences 8, no. 10: 205. https://doi.org/10.3390/vetsci8100205
APA StyleBagardi, M., Ghilardi, S., Locatelli, C., Bionda, A., Polli, M., Bussadori, C. M., Colombo, F. M., Pazzagli, L., & Brambilla, P. G. (2021). Influence of Morphometry on Echocardiographic Measurements in Cavalier King Charles Spaniels: An Inverse Probability Weighting Analysis. Veterinary Sciences, 8(10), 205. https://doi.org/10.3390/vetsci8100205