Trauma-Associated Pulmonary Laceration in Dogs—A Cross Sectional Study of 364 Dogs

 ,
, 
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design, Sample and Setting
2.2. MDCT Scanning Techniques
2.3. Image Analyses
2.4. Statistical Methods
3. Results
3.1. Characteristics of the MDCT Study Population
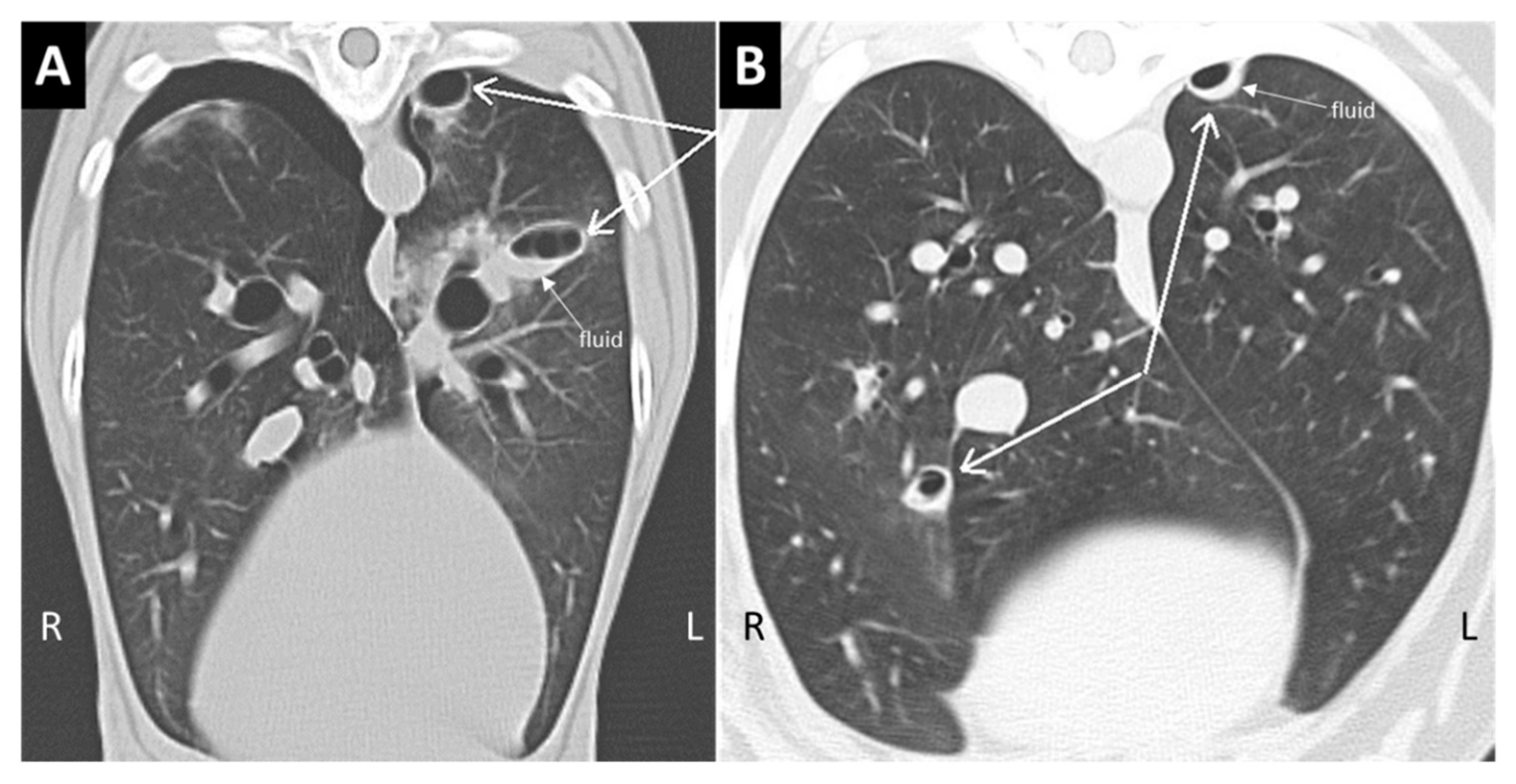
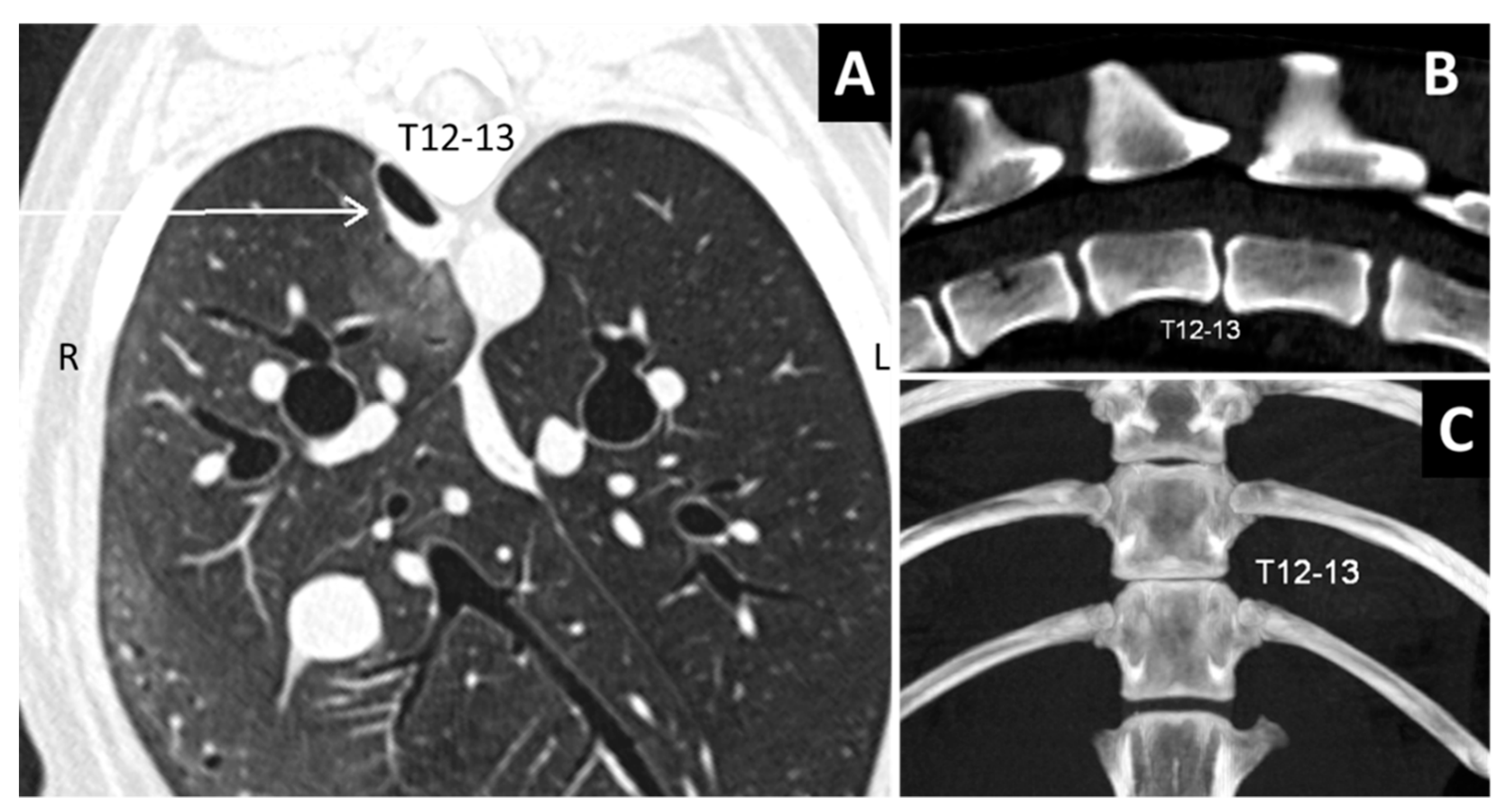
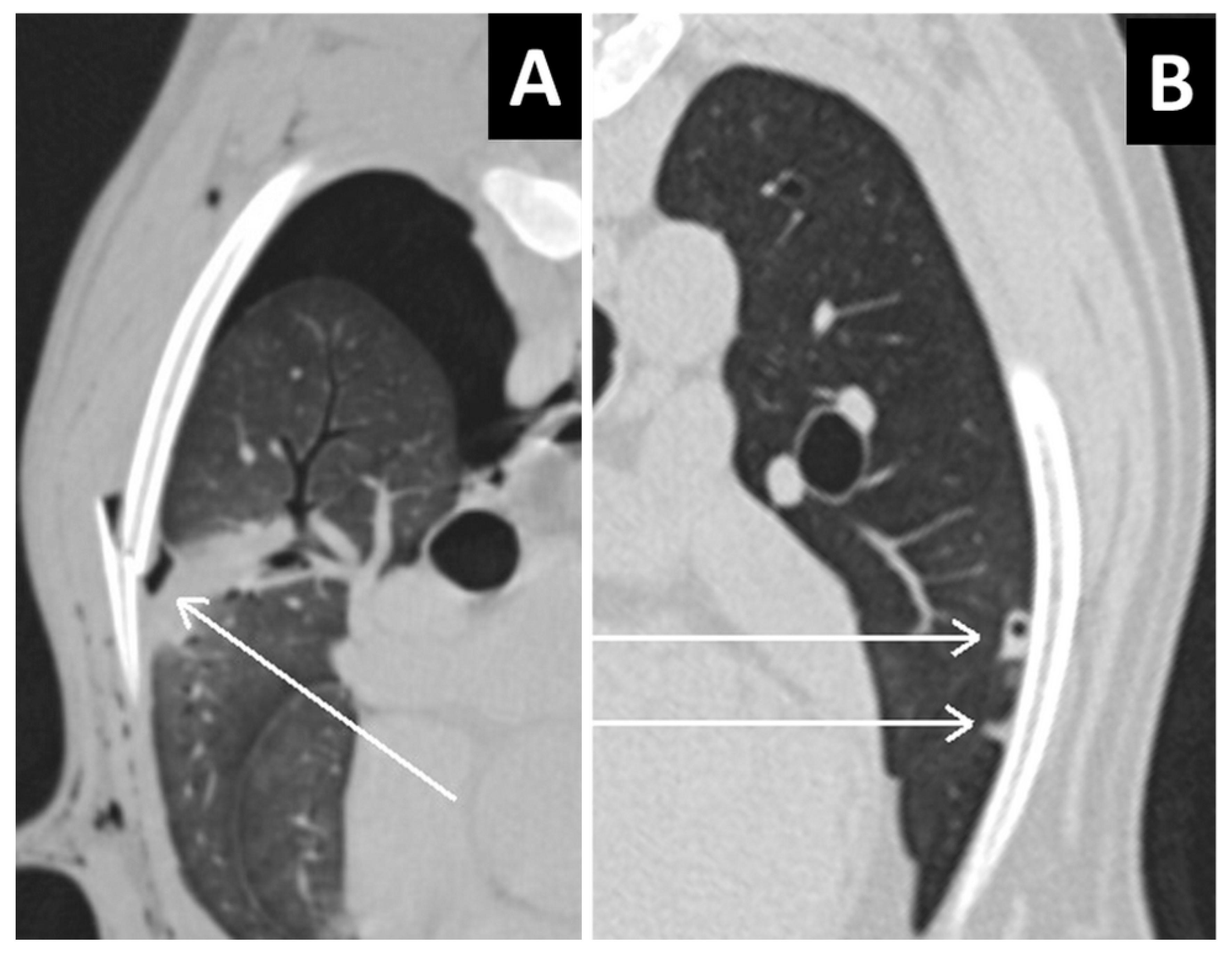
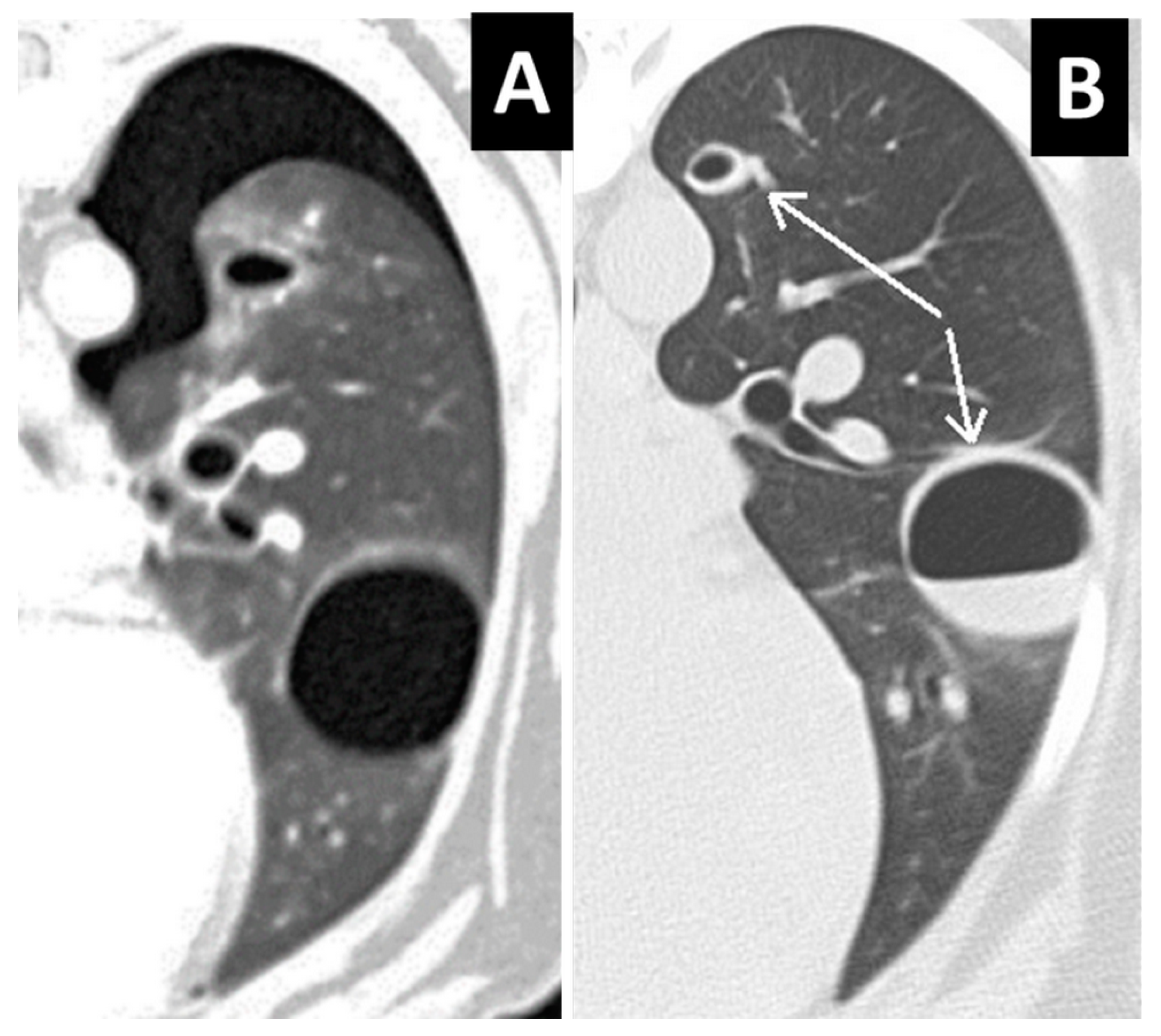
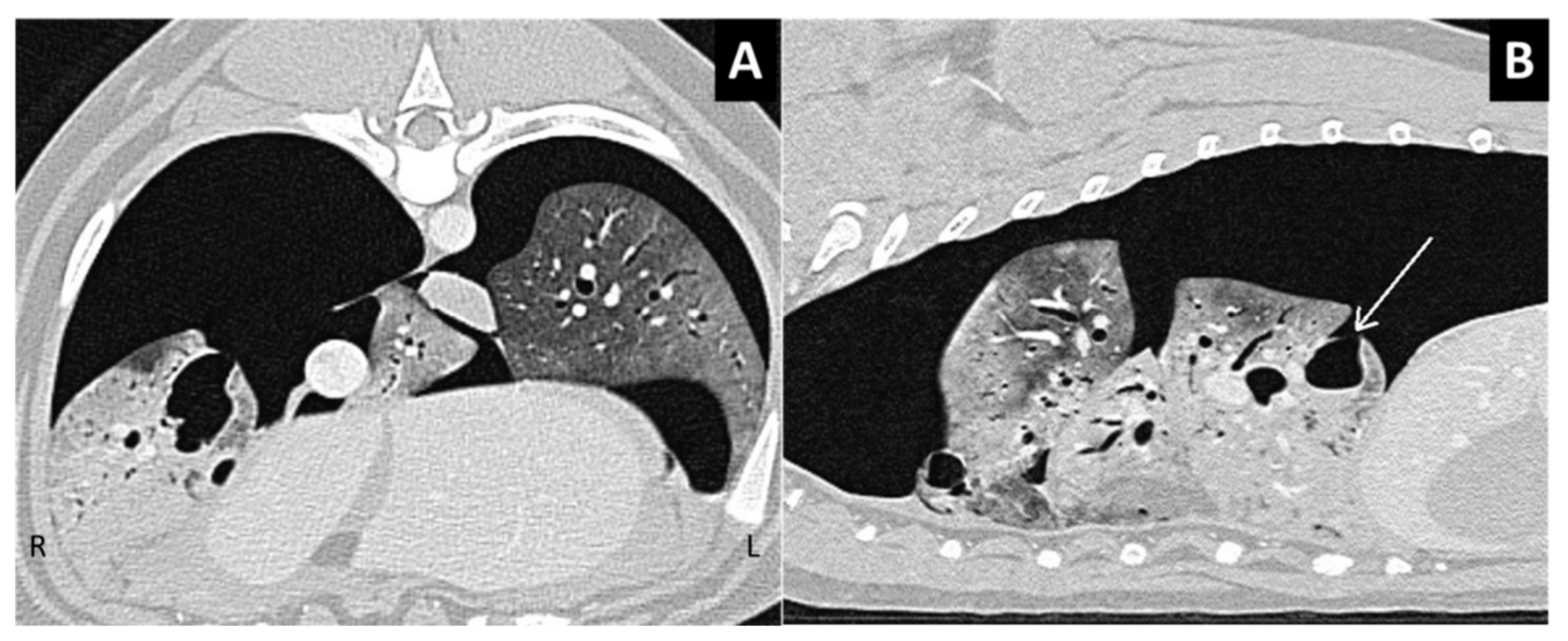
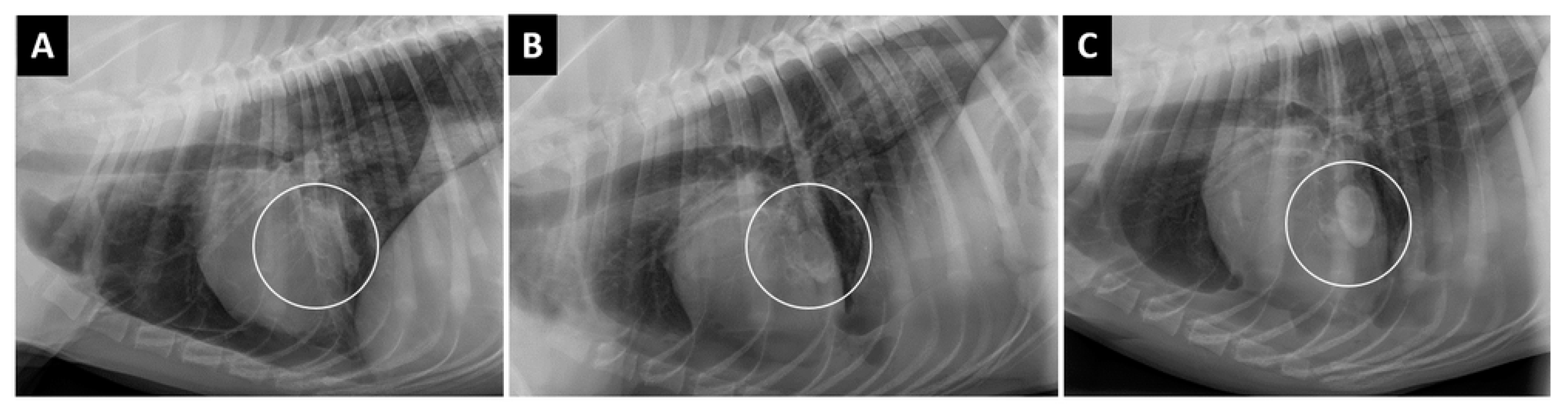
3.2. Characteristics of Lung Laceration
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Spackman, C.J.; Caywood, D.D.; Feeney, D.A.; Johnston, G.R. Thoracic wall and pulmonary trauma in dogs sustaining fractures as a result of motor vehicle accidents. J. Am. Vet. Med. Assoc. 1984, 185, 975–977. [Google Scholar] [PubMed]
- Simpson, S.A.; Syring, R.; Otto, C.M. Severe blunt trauma in dogs: 235 cases (1997–2003). J. Vet. Emerg. Crit. Care (San Antonio) 2009, 19, 588–602. [Google Scholar] [CrossRef] [PubMed]
- Streeter, E.M.; Rozanski, E.A.; Laforcade-Buress, A.D.; Freeman, L.M.; Rush, J.E. Evaluation of vehicular trauma in dogs: 239 cases (January–December 2001). J. Am. Vet. Med. Assoc. 2009, 235, 405–408. [Google Scholar] [CrossRef] [PubMed]
- Intarapanich, N.P.; McCobb, E.C.; Reisman, R.W.; Rozanski, E.A.; Intarapanich, P.P. Characterization and comparison of injuries caused by accidental and non-accidental blunt force trauma in dogs and cats. J. Forensic Sci. 2016, 61, 993–999. [Google Scholar] [CrossRef]
- Wagner, R.B.; Crawford, W.O., Jr.; Schimpf, P.P. Classification of parenchymal injuries of the lung. Radiology 1988, 167, 77–82. [Google Scholar] [CrossRef]
- Sangster, G.P.; González-Beicos, A.; Carbo, A.I.; Heldmann, M.G.; Ibrahim, H.; Carrascosa, P.; D’Agostino, H.B. Blunt traumatic injuries of the lung parenchyma, pleura, thoracic wall, and intrathoracic airways: Multidetector computer tomography imaging findings. Emerg. Radiol. 2007, 14, 297–310. [Google Scholar] [CrossRef]
- Powell, L.L.; Rozanski, E.A.; Tidwell, A.S.; Rush, J.E. A Retrospective Analysis of Pulmonary Contusion Secondary to Motor Vehicular Accidents in 143 Dogs: 1994–1997. J. Vet. Emerg. Crit. Care 1999, 9, 127–136. [Google Scholar] [CrossRef]
- Ressel, L.; Hetzel, U.; Ricci, E. Blunt Force Trauma in Veterinary Forensic Pathology. Vet. Pathol. 2016, 53, 941–961. [Google Scholar] [CrossRef]
- Greene, R. Lung alterations in thoracic trauma. J. Thorac. Imaging 1987, 2, 1–11. [Google Scholar] [CrossRef]
- Cho, H.J.; Jeon, Y.B.; Ma, D.S.; Lee, J.N.; Chung, M. Traumatic pulmonary pseudocysts after blunt chest trauma: Prevalence, mechanisms of injury, and computed tomography findings. J. Trauma Acute Care Surg. 2015, 79, 425–430. [Google Scholar] [CrossRef]
- Kaewlai, R.; Avery, L.L.; Asrani, A.V.; Novelline, R.A. Multidetector CT of blunt thoracic trauma. Radiographics 2008, 28, 1555–1570. [Google Scholar] [CrossRef] [PubMed]
- Lamb, C.R.; Neiger, R. Radiology corner: Differential diagnosis of pulmonary cavitary lesions. Vet. Radiol. Ultrasound 2000, 41, 340–341. [Google Scholar] [CrossRef] [PubMed]
- Oura, T.J.; Rozanski, E.A.; King, R.G.P.; Sato, A.F. What is your diagnosis? J. Am. Vet. Med. Assoc. 2008, 232, 357–358. [Google Scholar] [CrossRef] [PubMed]
- Dancer, S.C.; Le Roux, C.; Fosgate, G.T.; Kirberger, R.M. Radiography is less sensitive relative to CT for detecting thoracic radiographic changes in dogs affected by blunt trauma secondary to a motor vehicle accident. Vet. Radiol. Ultrasound 2019, 60, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Barge, P.; Fernández-Del Palacio, M.J.; Santarelli, G.; Soler, M.; Agut, A. Traumatic pulmonary pseudocysts associated to pneumothorax and rib fractures in a dog. Vet. Rec. Case Rep. 2018, 6, e000593. [Google Scholar] [CrossRef]
- Bertolini, G. The Lung and Airways. In Body MDCT in Small Animals; Bertolini, G., Ed.; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Mulholland, N.; Keir, I. Traumatic Pulmonary Pseudocysts in a Young Dog Following Non-penetrating Blunt Thoracic Trauma. Front. Vet. Sci. 2019, 6, 237. [Google Scholar] [CrossRef]
- Dante Yeh, D.; Jaron, L. Murray & Nadel’s Textbook of Respiratory Medicine, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2010; Volume 2, Chapter 76; p. 1358. [Google Scholar]
- Armstrong, L.B.; Mooney, D.P. Pneumatoceles in pediatric blunt trauma: Common and benign. J. Pediatr. Surg. 2018, 53, 1310–1312. [Google Scholar] [CrossRef]
- Yang, T.C.; Huang, C.H.; Yu, J.W.; Hsieh, F.C.; Huang, Y.F. Traumatic pneumatocele. Pediatr. Neonatol. 2010, 51, 135–138. [Google Scholar] [CrossRef]
- Sorsdahl, O.A.; Powell, J.W. Cavitary pulmonary lesions following non-penetrating chest trauma in children. Am. J. Roentgenol. 1965, 95, 118–124. [Google Scholar] [CrossRef]
- Hollister, M.; Stern, E.J.; Steinberg, K.P. Type 2 pulmonary laceration: A marker of blunt highenergy injury to the lung. AJR Am. J. Roentgenol. 1995, 165, 1126. [Google Scholar] [CrossRef][Green Version]
- Ulutas, H.; Celik, M.R.; Ozgel, M.; Soysal, O. Kuzucu APulmonary pseudocyst secondary to blunt or penetrating chest trauma: Clinical course and diagnostic issues. Eur. J. Trauma Emerg. Surg. 2014, 41, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Melloni, G.; Cremona, G.; Ciriaco, P.; Pansera, M.; Carretta, A.; Negri, G.; Zannini, P. Diagnosis and treatment of traumatic pulmonary pseudocysts. J. Trauma 2003, 54, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Kato, R.; Horunouchi, H.; Maeneka, Y. Traumatic pulmonary pseudocyst. Report of twelwe cases. J. Thorac. Cardiovasc. Surg. 1989, 97, 309–312. [Google Scholar] [CrossRef]
- Phillips, B.; Shaw, J.; Turco, L.; McDonald, D.; Carey, J.; Balters, M.; Asensio, J.A. Traumatic pulmonary pseudocyst: An underreported entity. Injury 2017, 48, 214–220. [Google Scholar] [CrossRef]
- Miller, L.A. Chest wall, lung, and pleural space trauma. Radiol. Clin. N. Am. 2006, 44, 213–224. [Google Scholar] [CrossRef]
- Oikonomou, A.; Prassopoulos, P. CT imaging of blunt chest trauma. Insights Imaging 2011, 2, 281–295. [Google Scholar] [CrossRef]
- Kaira, K.; Ishizuka, T.; Yanagitani, N.; Sunaga, N.; Hisada, T.; Mori, M. Pulmonary traumatic pneumatocele and hematoma. Jpn. J. Radiol. 2009, 27, 100–102. [Google Scholar] [CrossRef]
- Nishiumi, N.; Maitani, F.; Tsurumi, T.; Kaga, K.; Iwasaki, M.; Inoue, H. Blunt chest trauma with deep pulmonary laceration. Ann. Thorac. Surg. 2001, 71, 314–318. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Breed | Frequency |
|---|---|
| Mongrel | 14 |
| German Shepherd | 3 |
| Boxer | 2 |
| Italian Corso Dog | 2 |
| Labrador Retriever | 2 |
| Whippet | 2 |
| American Staffordshire Terrier | 1 |
| Australian Shepherd Dog | 1 |
| Bernese Mountain Dog | 1 |
| Brittany Spaniel | 1 |
| Chihuahua | 1 |
| Chow-chow | 1 |
| Czechoslovakian Wolfdog | 1 |
| Dachshund | 1 |
| Dobermann | 1 |
| English Cocker Spaniel | 1 |
| English Setter | 1 |
| French Bulldog | 1 |
| German Short- Haired Pointing Dog | 1 |
| Italian Segugio | 1 |
| Maremma And Abruzzese Sheepdog | 1 |
| Miniature Poodle | 1 |
| Rottweiler | 1 |
| Weimaraner | 1 |
| Yorkshire Terrier | 1 |
| Zwergpinscher | 1 |
| Parametric | Median 1 | IQR 1 | Median 0 | IQR 0 | p |
| Temperature (°C) | 38.5 | 0.91 | 38.4 | 1.01 | 0.32 |
| Heart rate (bpm) | 124 | 45.2 | 120 | 40 | 0.71 |
| Respiratory rate (bpm) | 45 | 34,5 | 40 | 36 | 0.13 |
| Length of hospitalization (days) | 5 | 4.8 | 5 | 4 | 0.45 |
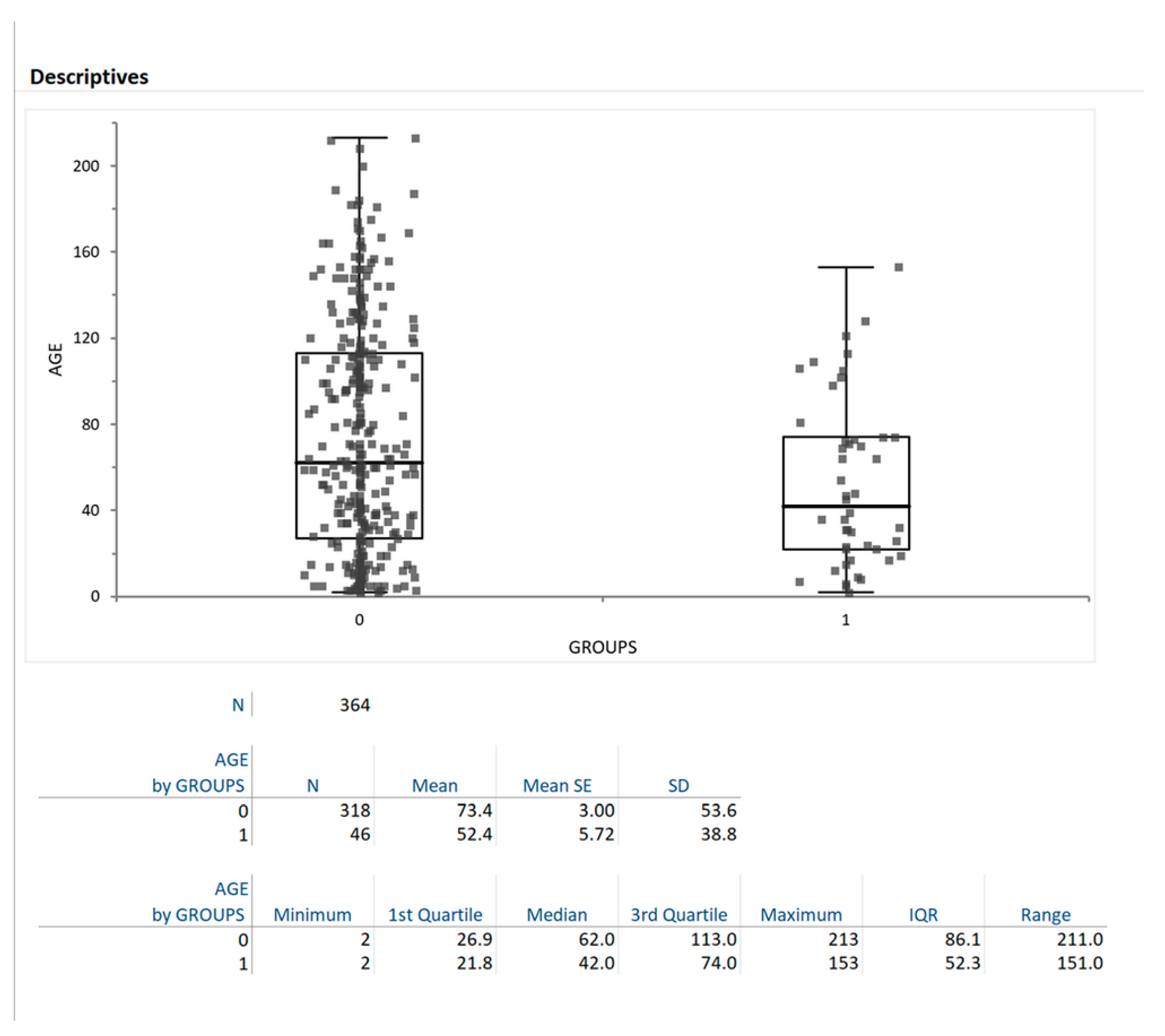
| Age (months) | 42 | 52.3 | 62 | 86.1 | 0.02 |
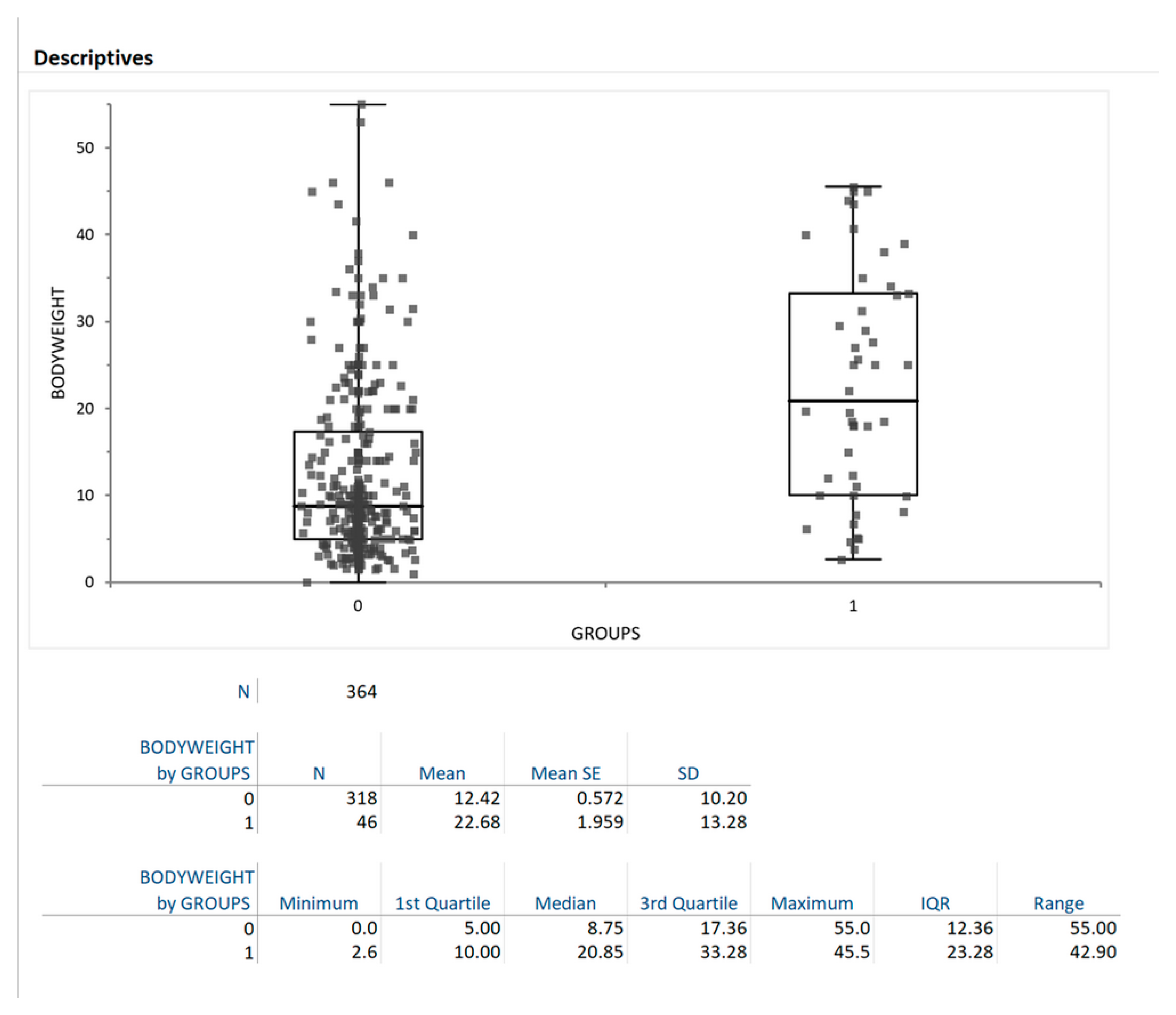
| Bodyweight (kg) | 20.8 | 23.3 | 8.7 | 12.4 | <0.0001 |
| Non Parametric | Mean 1 | IQR 1 | Mean 0 | IQR 0 | p |
| Mean blood pressure (mmHg) | 125 | 30.4 | 120 | 39.7 | 0.34 |
| Sex | 17F | 29M | 127F | 191M | 0.66 |
| Sexual status (female) | 9I | 8NI | 80I | 47NI | 0.42 |
| Frequency of hospitalization | 7NH | 39H | 56NH | 262H | 0.68 |
| 30-day mortality | 6D | 40ND | 48D | 270ND | 0.71 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertolini, G.; Briola, C.; Angeloni, L.; Costa, A.; Rocchi, P.; Caldin, M. Trauma-Associated Pulmonary Laceration in Dogs—A Cross Sectional Study of 364 Dogs. Vet. Sci. 2020, 7, 41. https://doi.org/10.3390/vetsci7020041
Bertolini G, Briola C, Angeloni L, Costa A, Rocchi P, Caldin M. Trauma-Associated Pulmonary Laceration in Dogs—A Cross Sectional Study of 364 Dogs. Veterinary Sciences. 2020; 7(2):41. https://doi.org/10.3390/vetsci7020041
Chicago/Turabian StyleBertolini, Giovanna, Chiara Briola, Luca Angeloni, Arianna Costa, Paola Rocchi, and Marco Caldin. 2020. "Trauma-Associated Pulmonary Laceration in Dogs—A Cross Sectional Study of 364 Dogs" Veterinary Sciences 7, no. 2: 41. https://doi.org/10.3390/vetsci7020041
APA StyleBertolini, G., Briola, C., Angeloni, L., Costa, A., Rocchi, P., & Caldin, M. (2020). Trauma-Associated Pulmonary Laceration in Dogs—A Cross Sectional Study of 364 Dogs. Veterinary Sciences, 7(2), 41. https://doi.org/10.3390/vetsci7020041