Anomalies of the Portal Venous System in Dogs and Cats as Seen on Multidetector-Row Computed Tomography: An Overview and Systematization Proposal


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Brief Anatomy Background
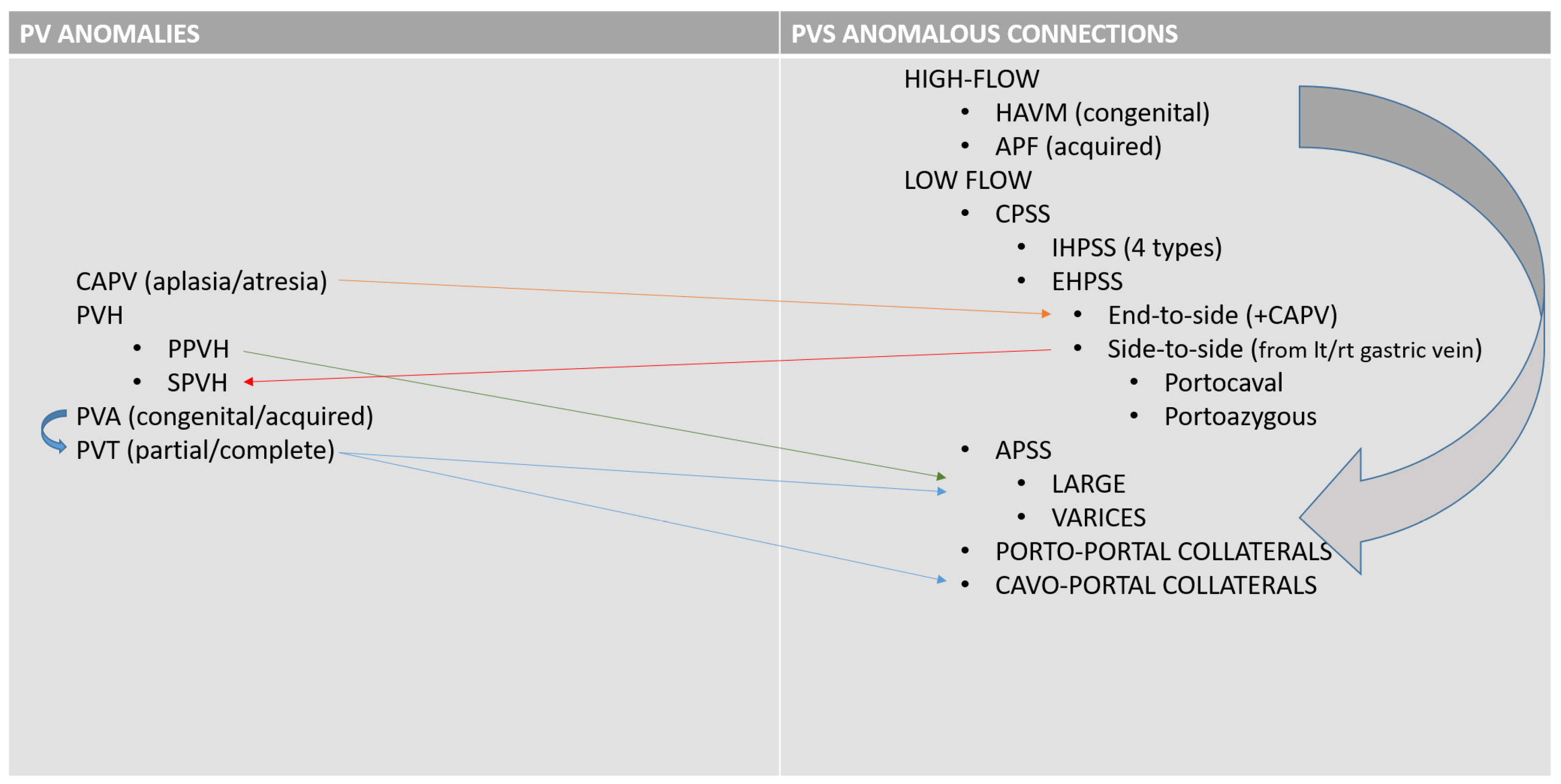
3. Portal System Venous Anomalies (PVSA)
3.1. Disorder of the Portal Vein System
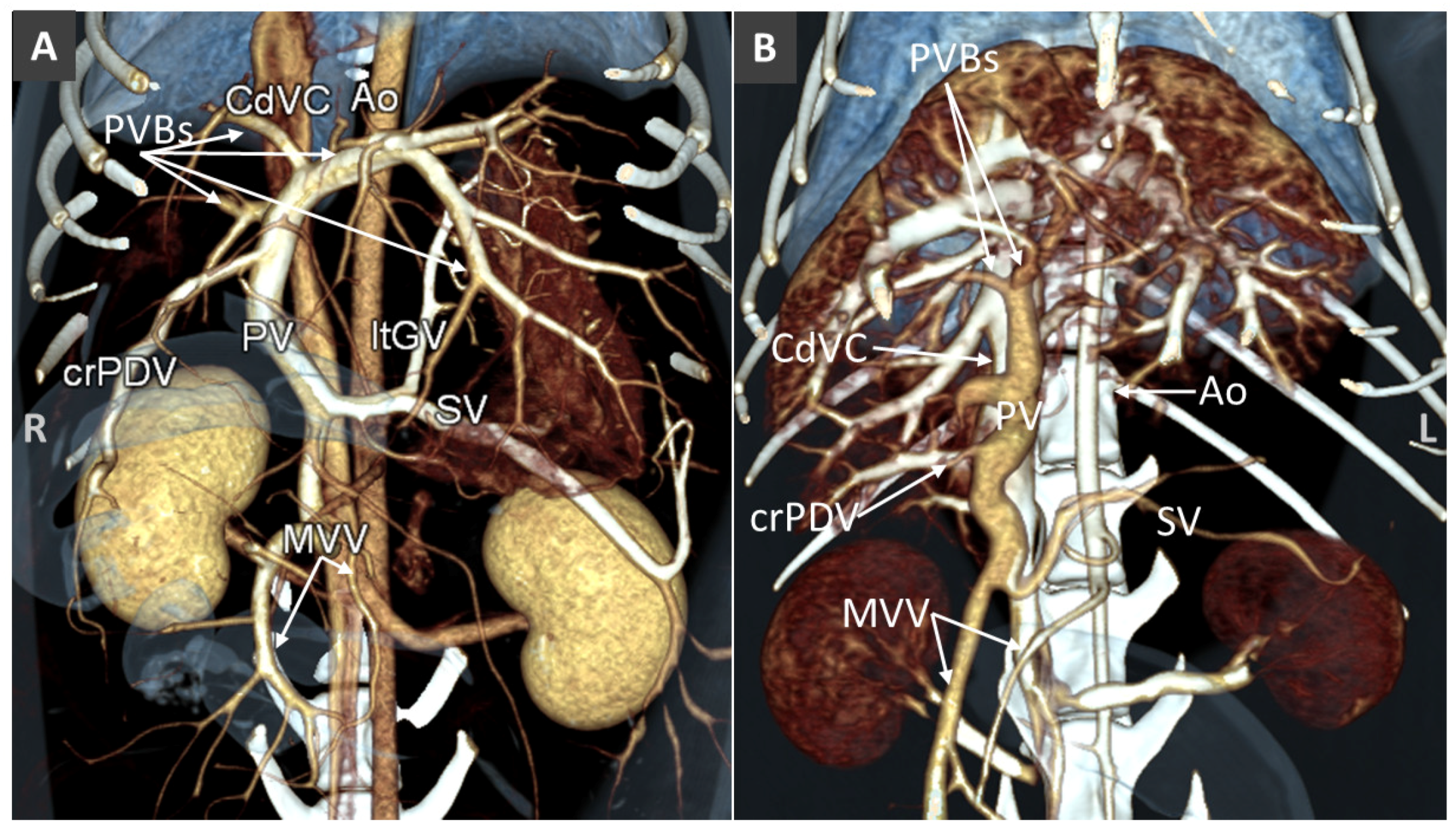
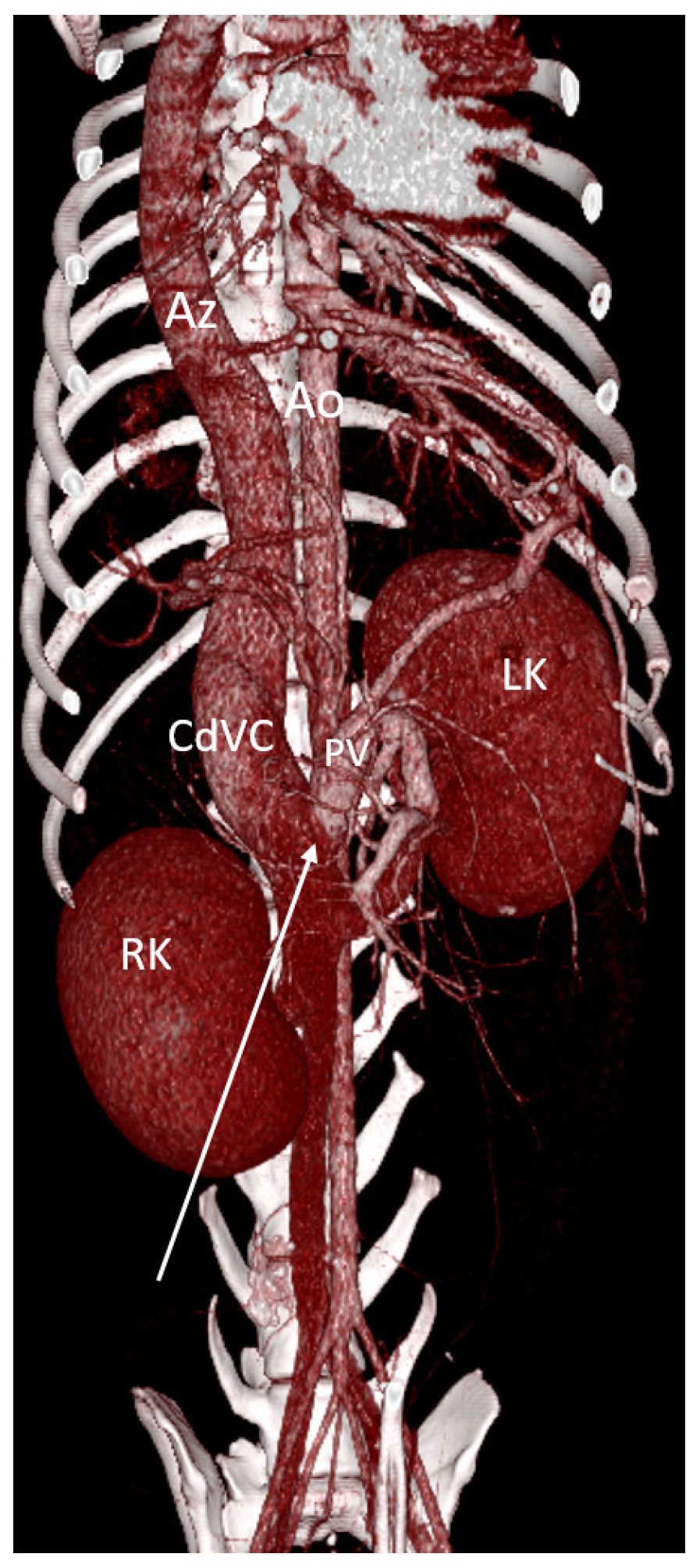
Congenital Absence of the Portal Vein (Aplasia and Atresia)
3.2. Portal Vein Hypoplasia
3.3. Portal Vein Aneurysm
3.4. Portal Vein Thrombosis
3.5. Anomalous Vascular Connections of the Portal Vein System
High-Flow Anomalous Portal Connections
3.6. Low-Flow Anomalous Portal Connections
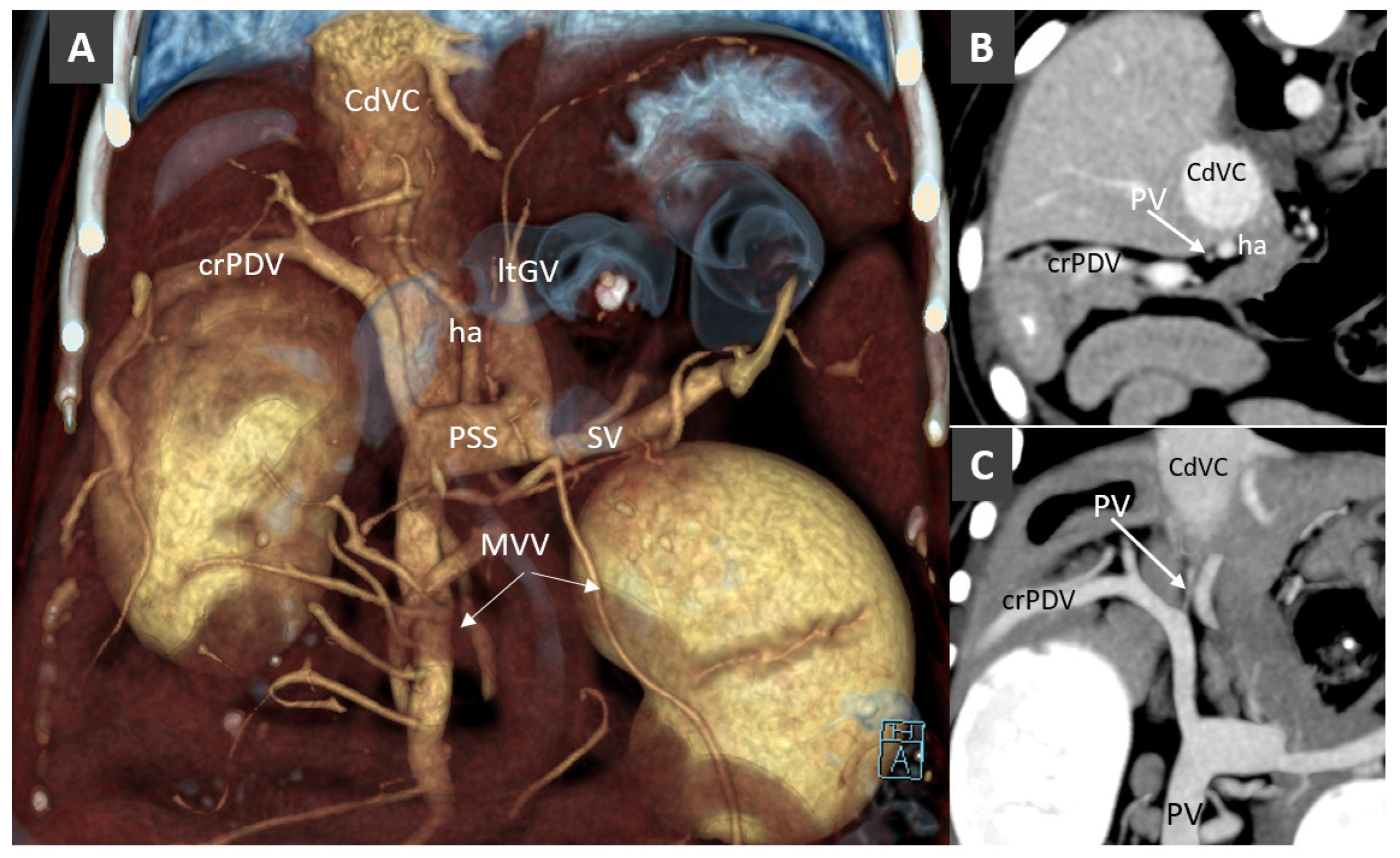
Congenital Portosystemic Shunt
3.7. Acquired Portosystemic Shunts (APSSs)
3.8. Porto-Portal Collaterals or Cavernous Transformation of the Portal Vein
4. Conclusions
Funding
Conflicts of Interest
References
- McMichael, J. The oxygen supply of the liver. Exp. Physiol. 1937, 27, 73–87. [Google Scholar] [CrossRef]
- Vollmar, B.; Menger, M.D. The hepatic microcirculation: Mechanistic contributions and therapeutic targets in liver injury and repair. Physiol. Rev. 2009, 89, 1269–1339. [Google Scholar] [CrossRef] [PubMed]
- Sleight, D.R.; Thomford, N.R. Gross anatomy and blood supply of canine liver. Anat. Rec. 1970, 166, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Vitums, A. Portal vein in the dog. Zbl. Vet. Med. 1959, 6, 723–741. [Google Scholar] [CrossRef]
- Suter, P.F. Portal Vein Anomalies in the Dog: Their Angiographic Diagnosis. Vet. Radiol. 1975, 16, 84–97. [Google Scholar] [CrossRef]
- Furneaux, R.W. Liver haemodynamics as they relate to portosystemic shunts in the dog: A review. Res. Vet. Sci. 2011, 91, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Van Steenbeek, F.G.; van den Bossche, L.; Leegwater, P.A.; Rothuizen, J. Inherited liver shunts in dogs elucidate pathways regulating embryonic development and clinical disorders of the portal vein. Mamm. Genome 2012, 23, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Van den Bossche, L.; van Steenbeek, F.G.; Favier, R.P.; Kummeling, A.; Leegwater, P.A.; Rothuizen, J. Distribution of extrahepatic congenital portosystemic shunt morphology in predisposed dog breeds. BMC Vet. Res. 2012, 8, 112. [Google Scholar] [CrossRef]
- Bertolini, G.; Rolla, E.C.; Zotti, A.; Caldin, M. Three-dimensional multislice helical computed tomography techniques for canine extra-hepatic portosystemic shunt assessment. Vet. Radiol. Ultrasound 2006, 47, 439–443. [Google Scholar] [CrossRef]
- Bertolini, G. Acquired portal collateral circulation in the dog and cat. Vet. Radiol. Ultrasound 2010, 51, 25–33. [Google Scholar] [CrossRef]
- Fukushima, K.; Kanemoto, H.; Ohno, K.; Takahashi, M.; Fujiwara, R.; Nishimura, R.; Tsujimoto, H. Computed tomographic morphology and clinical features of extrahepatic portosystemic shunts in 172 dogs in Japan. Vet. J. 2014, 199, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.C.; Nelson, L.L. Anatomy of extrahepatic portosystemic shunts in dogs as determined by computed tomography angiography. Vet. Radiol. Ultrasound 2011, 52, 498–506. [Google Scholar] [CrossRef]
- Or, M.; Ishigaki, K.; de Rooster, H.; Kutara, K.; Asano, K. Determination of Porto-Azygos Shunt Anatomy in Dogs by Computed Tomography Angiography. Vet. Surg. 2016, 45, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Buob, S.; Johnston, A.N.; Webster, C.R. Portal hypertension: Pathophysiology, diagnosis, and treatment. J. Vet. Intern. Med. 2011, 25, 169–186. [Google Scholar] [CrossRef] [PubMed]
- Hogan, D.F.; Benitez, M.E.; Parnell, N.K. Intravascular occlusion for the correction of extrahepatic portosystemic shunts in dogs. J. Vet. Intern. Med. 2010, 25, 1048–1054. [Google Scholar] [CrossRef]
- Weisse, C.; Berent, A.C.; Todd, K.; Solomon, J.A.; Cope, C. Endovascular evaluation and treatment of intrahepatic portosystemic shunts in dogs: 100 cases (2001–2011). J. Am. Vet. Med. Assoc. 2014, 244, 78–94. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.; Lim, C.; Oh, S.; Jung, J.; Chang, J.; Yoon, J.; Choi, M. Three-dimensional CT angiography of the canine hepatic vasculature. J. Vet. Sci. 2008, 9, 407–413. [Google Scholar] [CrossRef]
- Mai, W.; Weisse, C. Contrast-enhanced portal magnetic resonance angiography in dogs with suspected congenital portal vascular anomalies. Vet. Radiol. Ultrasound 2010, 52, 284–288. [Google Scholar] [CrossRef]
- Kim, S.E.; Giglio, R.F.; Reese, D.J.; Reese, S.L.; Bacon, N.J.; Ellison, G.W. Comparison of computed tomographic angiography and ultrasonography for the detection and characterization of portosystemic shunts in dogs. Vet. Radiol. Ultrasound 2013, 54, 569–574. [Google Scholar] [CrossRef]
- De Rycke, L.M.; Kromhout, K.J.; van Bree, H.J.; Bosmans, T.; Gielen, I.M. Computed tomography atlas of the normal cranial canine abdominal vasculature enhanced by dual-phase angiography. Anat. Histol. Embryol. 2014, 43, 413–422. [Google Scholar] [CrossRef]
- Parry, A.T.; White, R.N. Comparison of computed tomographic angiography and intraoperative mesenteric portovenography for extrahepatic portosystemic shunts. J. Small Anim. Pract. 2016, 58, 49–55. [Google Scholar] [CrossRef]
- Bertolini, G.; Prokop, M. Multidetector-row computed tomography: Technical basics and preliminary clinical applications in small animals. Vet. J. 2011, 189, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, G. Chapter 3.3 The Abdominal Vasculature, in Body MDCT in Small Animals; Springer International Verlag: Berlin, Germany, 2017; ISBN 978-3-319-46904-1. [Google Scholar]
- Wisner, E.R.; Zwingenberger, A.L. Chapter 5.2 Hepatovascular Disorders. In Atlas of Small Animal CT and MRI, 1st ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015. [Google Scholar]
- Simoens, P.; De Vos, N.R. Venae, veins. In Illustrated Veterinary Anatomical Nomenclature, 2nd ed.; Schaller, O., Ed.; Georg Thieme Verlag: Stuttgard, Germany, 2007; pp. 338–401. [Google Scholar]
- Kalt, D.J.; Stump, J.E. Gross anatomy of the canine portal vein. Anat. Histol. Embryol. 1993, 22, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Ursic, M.; Ravnik, D.; Hribernik, M.; Pecar, J.; Butinar, J.; Fazarinc, G. Gross anatomy of the portal vein and hepatic artery ramifications in dogs: Corrosion cast study. Anat. Histol. Embryol. 2007, 36, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Cullen, J.M.; van den Ingh, T.S.G.A.M.; Bunch, S.E.; Rothuizen, J.; Washabau, R.J.; Desmet, V.J. Morphological classification of circulatory disorders of the canine and feline liver. In WSAVA Standards for Clinical and Histological Diagnosis of Canine and Feline Liver Diseases; Elsevier Ltd.: Amsterdam, The Netherlands, 2006; pp. 41–59. [Google Scholar]
- Oishi, Y.; Tani, K.; Nakazawa, H.; Itamoto, K.; Haraguchi, T.; Taura, Y. Anatomical evaluation of hepatic vascular system in healthy beagles using X-ray contrast computed tomography. J. Vet. Med. Sci. 2015, 77, 925–929. [Google Scholar] [CrossRef] [PubMed]
- Abernethy, J. Account of two instances of uncommon formation in the viscera of the human body. Philos. Trans. R. Soc. 1793, 83, 59–66. [Google Scholar]
- Morgan, G.; Superina, R. Congenital absence of the portal vein: Two cases and a proposed classification system for portasystemic vascular anomalies. J. Pediatr. Surg. 1994, 29, 1239–1241. [Google Scholar] [CrossRef]
- Hunt, G.B.; Bellenger, C.R.; Borg, R.; Youmans, K.R.; Tisdall, P.L.; Malik, R. Congenital interruption of the portal vein and caudal vena cava in dogs: Six case reports and a review of the literature. Vet. Surg. 1998, 2, 203–215. [Google Scholar] [CrossRef]
- Cornillie, P.; Simoens, P. Prenatal development of the caudal vena cava in mammals: Review of the different theories with special reference to the dog. Anat. Histol. Embryol. 2005, 34, 364–372. [Google Scholar] [CrossRef]
- Payne, J.T.; Martin, R.A.; Constantinescue, G.M. The anatomy and embryology of portosystemic shunts in dogs and cats. Semin. Vet. Med. Surg. (Small Anim.) 1990, 5, 76–82. [Google Scholar]
- Zwingenberger, A.L.; Spriet, M.; Hunt, G.B. Imaging diagnosis-portal vein aplasia and interruption of the caudal vena cava in three dogs. Vet. Radiol. Ultrasound 2011, 52, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Van den Ingh, T.S.G.A.M.; Cullen, J.M.; Twedt, D.C.; Winkle, T.V.; Desmet, V.J.; Rothuizen, J. Morphological classification of biliary disorders of the canine and feline liver. In Standards for Clinical and Histological Diagnosis of Canine and Feline Liver Diseases, 1st ed.; Rothuizen, J., Bunch, S.E., Charles, J.A., Cullen, J.M., Desmet, V.J., Szatmari, V., Twedt, D.C., Van den Ingh, T.S.G.A.M., Winkle, T.V., Washabau, R.J., Eds.; Saunders: Amsterdam The Netherlands, 2006; pp. 61–76. [Google Scholar]
- Oui, H.; Kim, J.; Bae, Y.; Oh, J.; Park, S.; Lee, G.; Jeon, S.; Choi, J. Computed tomography angiography of situs inversus, portosystemic shunt and multiple vena cava anomalies in a dog. J. Vet. Med. Sci. 2013, 75, 1525–1528. [Google Scholar] [CrossRef] [PubMed]
- James, F.E.; Knowles, G.W.; Mansfield, C.S.; Robertson, I.D. Ascites due to pre-sinusoidal portal hypertension in dogs: A retrospective analysis of 17 cases. Aust. Vet. J. 2008, 86, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, J.S.; Hottinger, H.A.; Allen, L.; Phillips, L.; Aronson, L.R. Hepatic microvascular dysplasia in dogs: A retrospective study of 24 cases (1987–1995). J. Am. Anim. Hosp. Assoc. 2000, 36, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, L.; Hammond, G.; Mclauchlan, G. Primary portal vein hypoplasia and SLC2A9 mutation associated with urate urolithiasis in a Spanish water dog. Can. Vet. J. 2015, 56, 1153–1157. [Google Scholar]
- Rothuzien, J.; Bunch, S.E.; Charles, J.A. WSAVA Standards for Clinical and Histological Diagnosis of Canine and Feline Liver Diseases, 1st ed.; WB Saunders Elsevier: Philadelphia, PA, USA, 2006. [Google Scholar]
- Bertolini, G.; Caldin, M. Computed tomography findings in portal vein aneurysm of dogs. Vet. J. 2012, 193, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Miyawaki, S.; Washizu, M.; Maeda, S.; Shibata, S.; Watanabe, K.; Yamazoe, K. Portal vein aneurysm in a dog. J. Vet. Med. Sci. 2012, 74, 1191–1193. [Google Scholar] [CrossRef] [PubMed]
- Zwingenberger, A.L.; McLear, R.C.; Weisse, C. Diagnosis of arterioportal fistulae in four dogs using computed tomographic angiography. Vet. Radiol. Ultrasound 2005, 46, 472–477. [Google Scholar] [CrossRef]
- D’Anjou, M.A.; Huneault, L. Imaging diagnosis—Complex intrahepatic portosystemic shunt in a dog. Vet. Radiol. Ultrasound 2008, 49, 51–55. [Google Scholar] [CrossRef]
- Respess, M.; O’Toole, T.E.; Taeymans, O.; Rogers, C.L.; Johnston, A.; Webster, C.R. Portal vein thrombosis in 33 dogs: 1998–2011. J. Vet. Intern. Med. 2012, 26, 230–237. [Google Scholar] [CrossRef]
- Specchi, S.; Pey, P.; Ledda, G.; Lustgarten, M.; Thrall, D.; Bertolini, G. Computed tomographic and ultrasonographic characteristics of cavernous transformation of the obstructed portal vein in small animals. Vet. Radiol. Ultrasound 2015, 56, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, I.G.; Kirpensteijn, J.; Wolvekamp, W.T. Hepatic arteriovenous fistulae and portal vein hypoplasia in a Labrador retriever. J. Small Anim. Pract. 2001, 42, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Chanoit, G.; Kyles, A.E.; Weisse, C. Surgical and interventional radiographic treatment of dogs with hepatic arteriovenous fistulae. Vet. Surg. 2007, 36, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Specchi, S.; Rossi, F.; Weisse, C.; Morabito, S.; Petrovitch, N.P.; Drees, R.; Thierry, F.; Ricciardi, M.; Penchome, R.; Armenise, A.; et al. Canine and feline abdominal arterioportal communications can be classified based on branching patterns in computed tomographic angiography. Vet. Radiol. Ultrasound 2018, 59, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Weisse, C. Hepatic Arteriovenous Malformations (AVMs) and Fistulas. In Veterinary Image-Guided Interventions; Weisse, C., Berent, A., Eds.; John Wiley & Sons, Ltd.: Oxford, UK, 2015. [Google Scholar]
- Guzman, E.A.; McCahill, L.E.; Rogers, F.B. Arterioportal fistulas: Introduction of a novel classification with therapeutic implications. J. Gastrointest. Surg. 2006, 10, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.-L.; Zhang, J.-S. Hepatic perfusion disorders: Etiopathogenesis and related diseases. World J. Gastroenterol. WJG 2006, 12, 3265–3270. [Google Scholar] [CrossRef] [PubMed]
- Tisdall, P.L.C.; Hunt, B.; Borg, R.P.; Malik, R. Anatomy of the Ductus Venosus in Neonatal Dogs (Canis familiaris). Anat. Histol. Embryol. 1997, 26, 35–38. [Google Scholar] [CrossRef]
- Lamb, C.R.; White, R.N. Morphology of congenital intrahepatic portacaval shunts in dogs and cats. Vet. Rec. 1998, 142, 55–60. [Google Scholar] [CrossRef]
- White, R.N.; Burton, C.A. Anatomy of the patent ductus venosus in the dog. Vet. Rec. 2000, 146, 425–429. [Google Scholar] [CrossRef]
- Park, J.H.; Cha, S.H.; Han, J.K.; Han, M.C. Intrahepatic portosystemic venous shunt. AJR Am. J. Roentgenol. 1990, 155, 527–528. [Google Scholar] [CrossRef]
- Leeman, J.J.; Kim, S.E.; Reese, D.J.; Risselada, M.; Ellison, G.W. Multiple congenital PSS in a dog: Case report and literature review. J. Am. Anim. Hosp. Assoc. 2013, 49, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Tobias, K.M.; Rohrbach, B.W. Association of breed with the diagnosis of congenital portosystemic shunts in dogs: 2,400 cases (1980–2002). J. Am. Vet. Med. Assoc. 2003, 223, 1636–1639. [Google Scholar] [CrossRef] [PubMed]
- Tobias, K.M. Determination of inheritance of single congenital portosystemic shunts in Yorkshire terriers. J. Am. Anim. Hosp. Assoc. 2003, 39, 385–389. [Google Scholar] [CrossRef] [PubMed]
- White, R.N.; Parry, A.T. Morphology of congenital portosystemic shunts emanating from the left gastric vein in dogs and cats. J. Small Anim. Pract. 2013, 54, 459–467. [Google Scholar] [CrossRef] [PubMed]
- White, R.N.; Parry, A.T. Morphology of congenital portosystemic shunts involving the right gastric vein in dogs. J. Small Anim. Pract. 2015, 56, 430–440. [Google Scholar] [CrossRef] [PubMed]
- White, R.N.; Parry, A.T. Morphology of congenital portosystemic shunts involving the left colic vein in dogs and cats. J. Small Anim. Pract. 2016, 57, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Specchi, S.; Pey, P.; Javard, R.; Caron, I.; Bertolini, G. Mesenteric-reno-caval shunt in an aged dog. J. Small Anim. Pract. 2015, 56, 72. [Google Scholar] [CrossRef] [PubMed]
- Stringer, M.D. The clinical anatomy of congenital portosystemic venous shunts. Clin. Anat. 2008, 21, 147–157. [Google Scholar] [CrossRef]
- Blanc, T.; Guerin, F.; Franchi-Abella, S.; Jacquemin, E.; Pariente, D.; Soubrane, O.; Branchereau, S.; Gauthier, F. Congenital portosystemic shunts in children: A new anatomical classification correlated with surgical strategy. Ann. Surg. 2014, 260, 188–198. [Google Scholar] [CrossRef]
- Palerme, J.S.; Brown, J.C.; Marks, S.L.; Birkenheuer, A.J. Splenosystemic shunts in cats: A retrospective of 33 cases (2004–2011). J. Vet. Intern. Med. 2013, 27, 1347–1353. [Google Scholar] [CrossRef]
- Ricciardi, M. Splenophrenic portosystemic shunt in dogs with and without portal hypertension: Can acquired and congenital porto-caval connections coexist? Open Vet. J. 2016, 6, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.E. Portal hypertension. Part I. Pathophysiology and clinical consequences. Compend. Contin. Educ. Pract. Vet. 1987, 9, 741–748. [Google Scholar]
- Vitums, A. Portosystemic communications in the dog. Acta Anat. 1959, 39, 271–299. [Google Scholar] [CrossRef]
- Szatmari, V.; Rothuizen, J. Ultrasonographic identification and characterization of congenital portosystemic shunts and portal hypertensive disorders in dogs and cats. In WSAVA Standards for Clinical and Histopathological Diagnosis of Canine and Feline Liver Disease; Saunders Elsevier: Amsterdam, The Netherlands, 2006; pp. 15–39. [Google Scholar]
- Bertolini, G.; De Lorenzi, D.; Ledda, G.; Caldin, M. Esophageal varices due to a probable arteriovenous communication in a dog. J. Vet. Intern. Med. 2007, 21, 1392–1395. [Google Scholar] [CrossRef] [PubMed]
- Specchi, S.; d’Anjou, M.A.; Carmel, E.N.; Bertolini, G. Computed tomographic characteristics of collateral venous pathways in dogs with caudal vena cava obstruction. Vet. Radiol. Ultrasound 2014, 55, 531–538. [Google Scholar] [CrossRef] [PubMed]




















© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertolini, G. Anomalies of the Portal Venous System in Dogs and Cats as Seen on Multidetector-Row Computed Tomography: An Overview and Systematization Proposal. Vet. Sci. 2019, 6, 10. https://doi.org/10.3390/vetsci6010010
Bertolini G. Anomalies of the Portal Venous System in Dogs and Cats as Seen on Multidetector-Row Computed Tomography: An Overview and Systematization Proposal. Veterinary Sciences. 2019; 6(1):10. https://doi.org/10.3390/vetsci6010010
Chicago/Turabian StyleBertolini, Giovanna. 2019. "Anomalies of the Portal Venous System in Dogs and Cats as Seen on Multidetector-Row Computed Tomography: An Overview and Systematization Proposal" Veterinary Sciences 6, no. 1: 10. https://doi.org/10.3390/vetsci6010010
APA StyleBertolini, G. (2019). Anomalies of the Portal Venous System in Dogs and Cats as Seen on Multidetector-Row Computed Tomography: An Overview and Systematization Proposal. Veterinary Sciences, 6(1), 10. https://doi.org/10.3390/vetsci6010010