Management of Cleft Palate in Puppies Using A Temporary Prosthesis: A Report of Three Cases

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Case Presentation
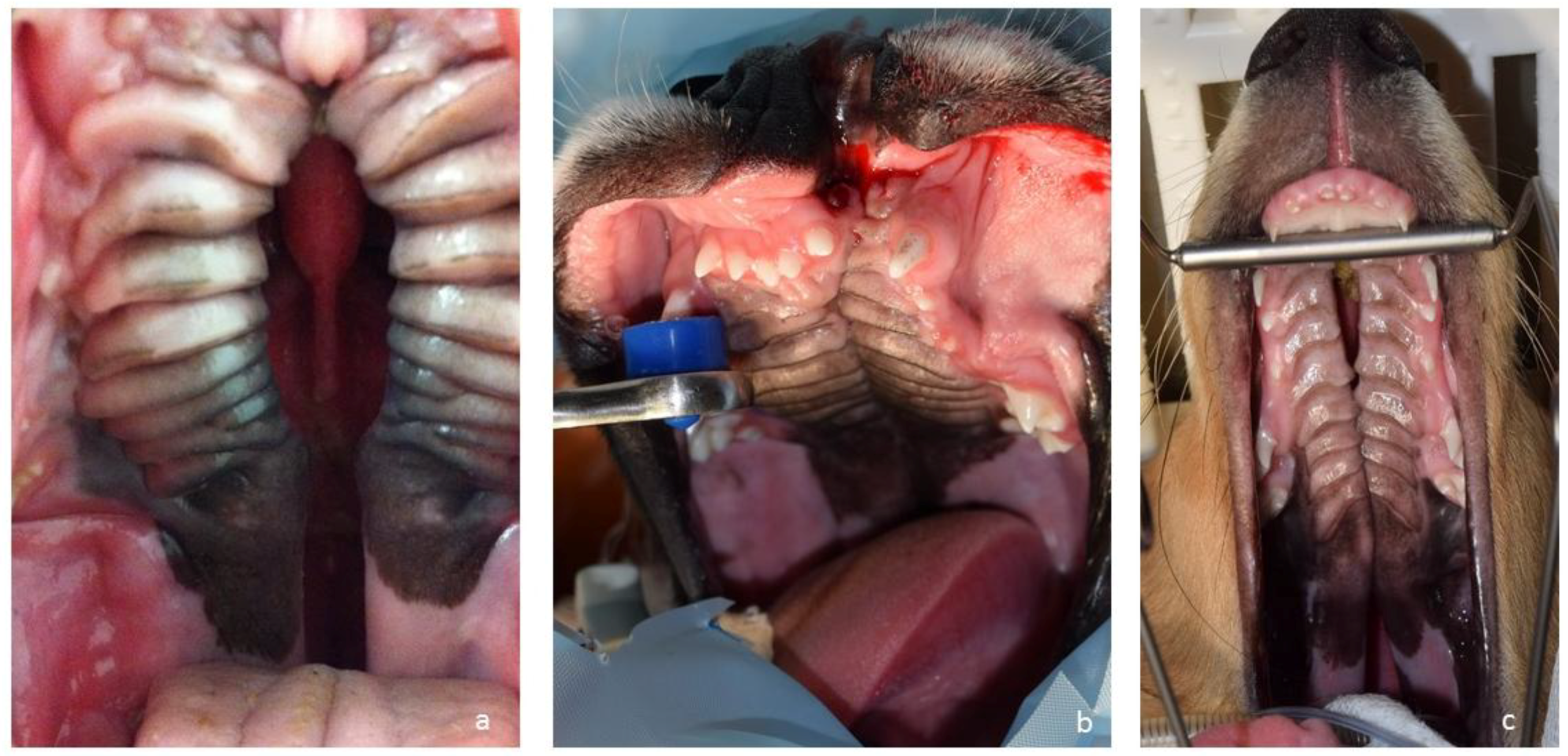
2.1. Cases
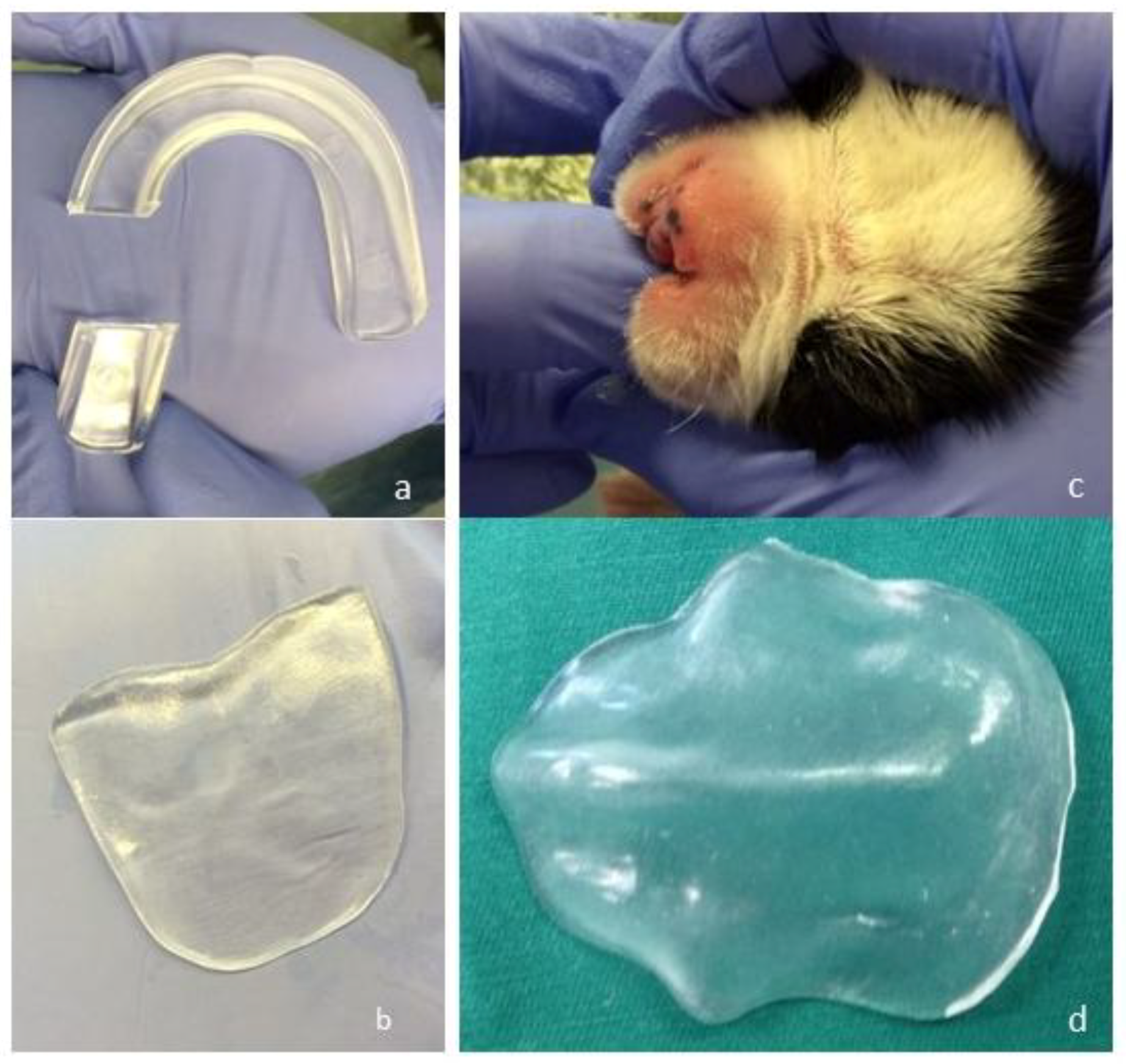
2.2. Customisation of A Palatal Prosthesis
2.3. Further Therapies
2.4. Development
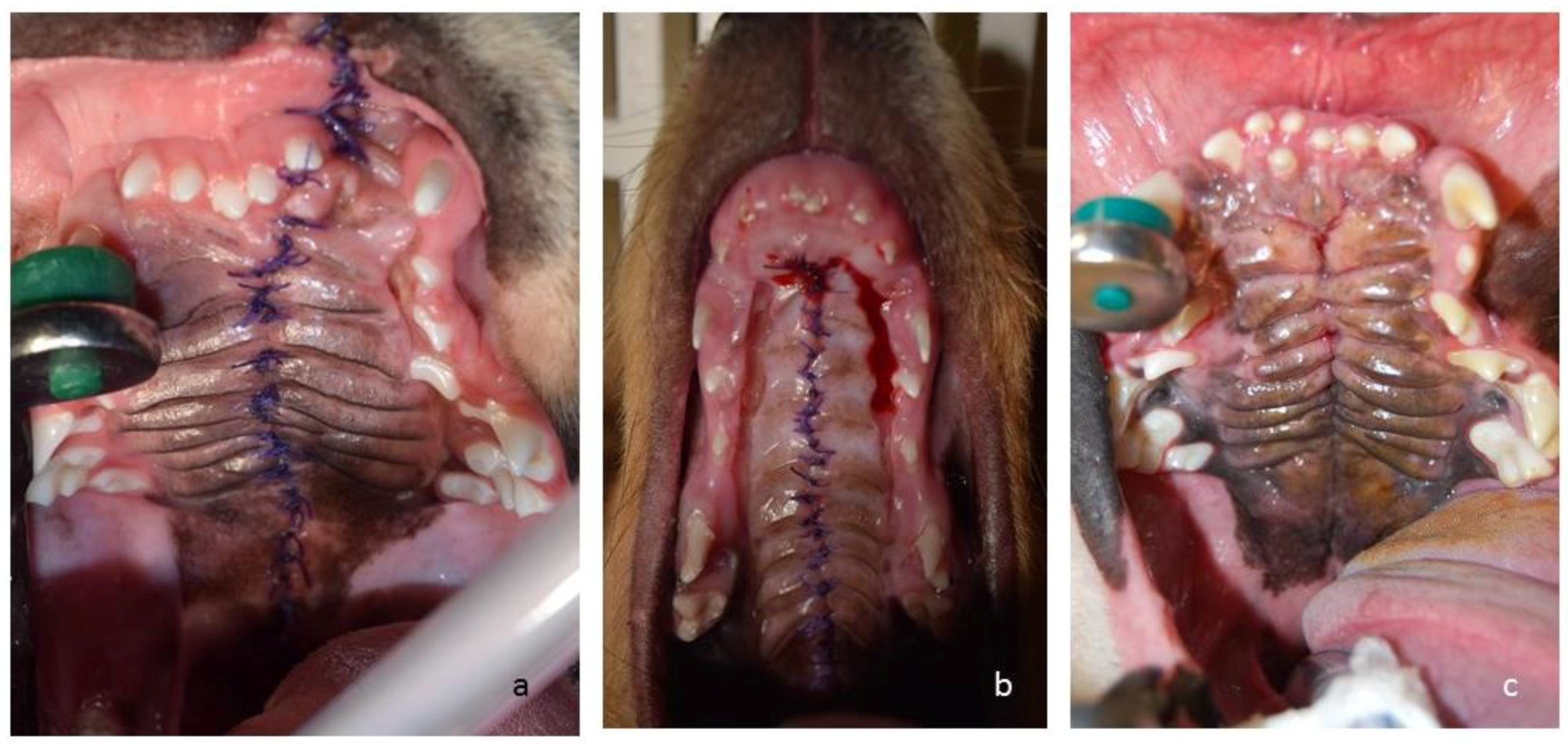
2.5. Outcomes and Follow-up
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hoskins, J.D. The Respiratory System. In Veterinary Pediatrics. Dogs and Cats from Birth to Six Months, 2nd ed.; Hoskins, J.D., Ed.; W.B. Saunders: Philadelphia, PA, USA, 1995; p. 73. ISBN 0721638872. [Google Scholar]
- Lee, J.I.; Kim, Y.S.; Kim, M.J.; Lee, J.; Choi, J.H.; Yeom, D.B.; Park, J.M.; Hong, S.H. Application of a temporary palatal prosthesis in a puppy suffering from cleft palate. J. Vet. Sci. 2006, 7, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Hedlund, C.S. Surgery of the oral cavity and oropharynx. In Small Animal Surgery, 2nd ed.; Fossum, T.W., Ed.; Mosby: St. Louis, MO, USA, 2002; pp. 274–306. ISBN 9781560535799. [Google Scholar]
- Martinez-Sanz, E.; Casado-Gomez, I.; Martin, C.; López-Gordillo, Y.; González, P.; Rodríguez-Bobada, C.; Paradas, I.; González-Meli, B.; Maldonado, E.; Maestro, C.; et al. A new technique for feeding dogs with a congenital cleft palate for surgical research. Lab. Anim. 2011, 45, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Fiani, N.; Verstraete, F.J.; Arzi, B. Reconstruction of congenital nose, cleft primary palate, and lip disorders. Vet. Clin. North Am. Small Anim. Pract. 2016, 46, 663–675. [Google Scholar] [CrossRef] [PubMed]
- Tolwani, R.; Hagan, C.; Runstadler, J.; Lyons, H.; Green, S.; Bouley, D.; Rodriguez, L.; Schendel, S.; Moseley, M.; Daunt, D.; et al. Magnetic resonance imaging and surgical repair of cleft palate in a four-week-old canine (Canis familiaris): An animal model for cleft palate repair. Contemp. Top. Lab. Anim. Sci. 2004, 43, 17–21. [Google Scholar] [PubMed]
- Peralta, S.; Fiani, N.; Kan-Rohrer, K.H.; Verstaete, F.J. Morphological evaluation of clefts of the lip, palate, or both in dog. Am. J. Vet. Res. 2017, 78, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Liao, Y.F. Hard palate-repair technique and facial growth in patients with cleft lip and palate: A systematic review. Br. J. Oral Maxillofac. Surg. 2013, 51, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Osuji, O. Preparation of feeding obturators for infants with cleft lip and palate. J. Clin. Pediatr. Dent. 1995, 19, 211–214. [Google Scholar] [PubMed]
- Agarwal, A.V.; Shafi, S. A feeding appliance for a newborn baby with cleft lip and palate. Natl. J. Maxillofac. Surg. 2010, 1, 91–93. [Google Scholar] [PubMed]
- Smith, M.M.; Rockhill, A.D. Prosthodontic appliance for repair of an oronasal fistula in a cat. J. Am. Vet. Med. Assoc. 1996, 9, 1410–1412. [Google Scholar]
- Hale, F.A.; Sylvestre, A.M.; Miller, C. The use of a prosthetic appliance to manage a large palatal defect in a dog. J. Vet. Dent. 1997, 14, 61–64. [Google Scholar] [PubMed]
- Yamamoto, S. The effects of food consistency on maxillary growth in rats. Eur. J. Orthod. 1996, 18, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Herfert, O. Fundamental investigations into problems related to cleft palate surgery. Br. J. Plast. Surg. 1958, 11, 97–105. [Google Scholar] [CrossRef]
- Bardach, J.; Kelly, K.M.; Salyer, K.E. A comparative-study of facial growth of facial growth following lip and palate repair performed in sequence and simultaneously-an experimental-study in beagles. Plast. Reconstr. Surg. 1993, 91, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Ophof, R.; Jaap, C.; Von Den Hoff, J.W.; Kuijpers-Jagtman, A. Histologic evaluation of skin-derived and collagen-based substrates implanted in palatal wound. Wound Repair Regen. 2004, 12, 528–538. [Google Scholar] [CrossRef] [PubMed]
- Bokemeyer, J.; Fehr, M.; Meyer-Lindenberg, A. Cleft palate repair using a collagen matrix (VetBiosist®). Tierarztl. Prax. Ausg. K Kleintiere Heimtiere 2009, 37, 173–178. [Google Scholar]
- Peralta, S.; Nemec, A.; Fiani, N.; Verstraete, F.J.M. Staged double-layer closure of palatal defects in 6 dogs. Vet. Surg. 2015, 44, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Nemec, A.; Daniaux, L.; Johnson, E.; Peralta, S.; Verstraete, F.J.M. Craniomaxillofacial abnormalities in dogs with congenital palatal defects: computed tomographic findings. Vet. Surg. 2015, 44, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Kemp, C.; Thiele, H.; Dankof, A.; Schmidt, G.; Lauster, C.; Fernahl, G.; Lauster, R. Cleft lip and/or palate with monogenic autosomal recessive transmission in Pyrenees shepherd dogs. Cleft Palate Craniofac. J. 2009, 46, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Bian, Z.; Torensma, R.; von den Hoff, J.W. Biological mechanisms in palatogenesis and cleft palate. J. Dent. Res. 2009, 88, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Moura, E.; Cirio, S.M.; Pimpao, C.T. Nonsyndromic cleft lip and palate in boxer dogs: Evidence of monogenic autosomal recessive inheritance. Cleft Palate Craniofac. J. 2012, 49, 759–760. [Google Scholar] [CrossRef] [PubMed]





© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conze, T.; Ritz, I.; Hospes, R.; Wehrend, A. Management of Cleft Palate in Puppies Using A Temporary Prosthesis: A Report of Three Cases. Vet. Sci. 2018, 5, 61. https://doi.org/10.3390/vetsci5030061
Conze T, Ritz I, Hospes R, Wehrend A. Management of Cleft Palate in Puppies Using A Temporary Prosthesis: A Report of Three Cases. Veterinary Sciences. 2018; 5(3):61. https://doi.org/10.3390/vetsci5030061
Chicago/Turabian StyleConze, Theresa, Isabelle Ritz, Rainer Hospes, and Axel Wehrend. 2018. "Management of Cleft Palate in Puppies Using A Temporary Prosthesis: A Report of Three Cases" Veterinary Sciences 5, no. 3: 61. https://doi.org/10.3390/vetsci5030061
APA StyleConze, T., Ritz, I., Hospes, R., & Wehrend, A. (2018). Management of Cleft Palate in Puppies Using A Temporary Prosthesis: A Report of Three Cases. Veterinary Sciences, 5(3), 61. https://doi.org/10.3390/vetsci5030061