
Use of Ozone in Veterinary Dentistry as an Alternative to Conventional Antibiotics and Antiseptics


 ,
,  and
and 
Abstract
Simple Summary
Abstract
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
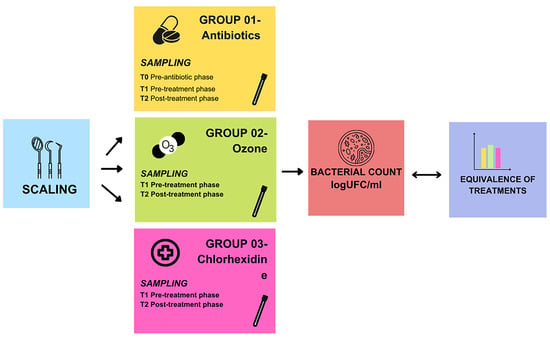
2.2. Patient Preparation and Sampling
- -
- Group 1:
- -
- Group 2:
- -
- Group 3:
2.3. Mesophilic Bacterial Count Determination
- -
- represents the number of colonies recorded for each dilution.
- -
- V is the volume in milliliters (mL) of sterile physiological solution in which the bacteriological swab has been immersed.
- -
- denotes the number of dilutions.
- -
- represents the dilution factor corresponding to the first dilution.
2.4. Statistical Analysis
3. Results and Discussions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wallis, C.; Holcombe, L.J. A review of the frequency and impact of periodontal disease in dogs. J. Small Anim. Pract. 2020, 61, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-P.; Chang, S.-H.; Tang, C.-Y.; Liou, M.-L.; Tsai, S.-J.J.; Lin, Y.-L. Composition Analysis and Feature Selection of the Oral Microbiota Associated with Periodontal Disease. BioMed Res. Int. 2018, 2018, 3130607. [Google Scholar] [CrossRef] [PubMed]
- Santibáñez, R.; Rodríguez-Salas, C.; Flores-Yáñez, C.; Garrido, D.; Thomson, P. Assessment of Changes in the Oral Microbiome That Occur in Dogs with Periodontal Disease. Vet. Sci. 2021, 8, 291. [Google Scholar] [CrossRef] [PubMed]
- Logan, E.I. Dietary influences on periodontal health in dogs and cats. Vet. Clin. N. Am. Small Anim. Pract. 2006, 36, 1385–1401. [Google Scholar] [CrossRef] [PubMed]
- Yamaki, S.; Tachibana, M.; Hachimura, H.; Ogawa, M.; Kanegae, S.; Amimoto, H.; Shimizu, T.; Watanabe, K.; Watarai, M.; Amimoto, A. The association between gingivitis and oral spirochetes in young cats and dogs. PLoS ONE 2023, 18, e0281126. [Google Scholar] [CrossRef] [PubMed]
- Liccardo, D.; Cannavo, A. Periodontal Disease: A Risk Factor for Diabetes and Cardiovascular Disease. Int. J. Mol. Sci. 2019, 20, 1414. [Google Scholar] [CrossRef] [PubMed]
- Robbins, S.N.; Goggs, R.; Lhermie, G.; Lalonde-Paul, D.F.; Menard, J. Antimicrobial Prescribing Practices in Small Animal Emergency and Critical Care. Front. Vet. Sci. 2020, 7, 110. [Google Scholar] [CrossRef] [PubMed]
- Manzillo, V.F.; Peruzy, M.F.; Gizzarelli, M.; Izzo, B.; Sarnelli, P.; Carrella, A.; Vinciguerra, G.; Chirollo, C.; Fayala, N.E.H.B.; Balestrino, I.; et al. Examining the Veterinary Electronic Antimicrobial Prescriptions for Dogs and Cats in the Campania Region, Italy: Corrective Strategies Are Imperative. Animals 2023, 13, 2869. [Google Scholar] [CrossRef]
- Oppelaar, M.C.; Zijtveld, C.; Kuipers, S.; Oever, J.T.; Honings, J.; Weijs, W.; Wertheim, H.F.L. Evaluation of Prolonged vs Short Courses of Antibiotic Prophylaxis Following Ear, Nose, Throat, and Oral and Maxillofacial Surgery: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head. Neck Surg. 2019, 145, 610–616. [Google Scholar] [CrossRef]
- Välkki, K.J.; Thomson, K.H.; Grönthal, T.S.C.; Junnila, J.J.T.; Rantala, M.H.J.; Laitinen-Vapaavuori, O.M.; Mölsä, S.H. Antimicrobial prophylaxis is considered sufficient to preserve an acceptable surgical site infection rate in clean orthopaedic and neurosurgeries in dogs. Acta Vet. Scand. 2020, 62, 53. [Google Scholar] [CrossRef]
- Buonavoglia, A.; Leone, P.; Solimando, A.G.; Fasano, R.; Malerba, E.; Prete, M.; Corrente, M.; Prati, C.; Vacca, A.; Racanelli, V. Antibiotics or No Antibiotics, That Is the Question: An Update on Efficient and Effective Use of Antibiotics in Dental Practice. Antibiotics 2021, 10, 550. [Google Scholar] [CrossRef] [PubMed]
- Weese, J.S.; Battersby, I.; Morrison, J.; Spofford, N.; Soltero-Rivera, M. Antimicrobial use practices in canine and feline dental procedures performed in primary care veterinary practices in the United States. PLoS ONE 2023, 18, e0295070. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, P.B.; Brennan, M.T.; Kent, M.L.; Norton, H.J.; Weinrib, D.A. Impact of amoxicillin prophylaxis on the incidence, nature, and duration of bacteremia in children after intubation and dental procedures. Circulation 2004, 109, 2878–2884. [Google Scholar] [CrossRef] [PubMed]
- Kern, I.; Bartmann, C.P.; Verspohl, J.; Rohde, J.; Bienert-Zeit, A. Bacteremia before, during and after tooth extraction in horses in the absence of antimicrobial administration. Equine Vet. J. 2017, 49, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Ruparell, A.; Inui, T.; Staunton, R.; Wallis, C.; Deusch, O.; Holcombe, L.J. The canine oral microbiome: Variation in bacterial populations across different niches. BMC Microbiol. 2020, 20, 42. [Google Scholar] [CrossRef] [PubMed]
- Niemiec, B.A.; Gawor, J.; Tang, S.; Prem, A.; Krumbeck, J.A. The bacteriome of the oral cavity in healthy dogs and dogs with periodontal disease. Am. J. Vet. Res. 2021, 83, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Bellows, J.; Berg, M.L. AAHA Dental Care Guidelines for Dogs and Cats. J. Am. Anim. Hosp. Assoc. 2019, 55, 49–69. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, E.; Dominguez, C. Mechanisms underlying chlorhexidine-induced cytotoxicity. Toxicol. In Vitro 2001, 15, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Löe, H.; Schiøtt, C.R. The effect of mouthrinses and topical application of chlorhexidine on the development of dental plaque and gingivitis in man. J. Periodontal Res. 1970, 5, 79–83. [Google Scholar] [CrossRef]
- Sasser, L. Endodontic Disinfection for Orthograde Root Canal Treatment in Veterinary Dentistry. J. Vet. Dent. 2020, 37, 35–40. [Google Scholar] [CrossRef]
- Vianna, M.E.; Gomes, B.P.; Berber, V.B.; Zaia, A.A.; Ferraz, C.C.R.; de Souza-Filho, F.J. In vitro evaluation of the antimicrobial activity of chlorhexidine and sodium hypochlorite. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 97, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Huth, K.C.; Quirling, M.; Lenzke, S.; Paschos, E.; Kamereck, K.; Brand, K.; Hickel, R.; Ilie, N. Effectiveness of ozone against periodontal pathogenic microorganisms. Eur. J. Oral Sci. 2011, 119, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Sciorsci, R.; Lillo, E.; Occhiogrosso, L.; Rizzo, A. Ozone therapy in veterinary medicine: A review. Res. Vet. Sci. 2020, 130, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Gavazza, A.; Marchegiani, A.; Rossi, G.; Franzini, M.; Spaterna, A.; Mangiaterra, S.; Cerquetella, M. Ozone Therapy as a Possible Option in COVID-19 Management. Front. Public Health 2020, 258, 417. [Google Scholar] [CrossRef] [PubMed]
- Sciorsci, R.L.; Rizzo, A.; Piccinno, M.; Lillo, E.; Carbonari, A.; Jirillo, F. Antimicrobial Resistance and Current Alternatives in Veterinary Practice: A Review. Curr. Pharm. Des. 2023, 29, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Sadatullah, S.; Mohamed, N.H.; Razak, F.A. The antimicrobial effect of 0.1 ppm ozonated water on 24-hour plaque microorganisms in situ. Braz. Oral Res. 2012, 26, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Anumula, L.; Kumar, K.V. Antibacterial activity of fresh prepared ozonated water and chlorexidine on Mutans Streptococcus when used as an oral rinse—A randomised clinical study. J. Clin. Diagn. Res. 2017, 11, ZC05–ZC08. [Google Scholar] [CrossRef]
- Kaur, A.; Bhavikatti, S.K. Efficacy of ozonised water and 0.2% Chlorhexidine gluconate in the management of chronic periodontitis when used as an irrigant in conjugation with Phase 1 Therapy. J. Contemp. Dent. Pract. 2019, 20, 318–323. [Google Scholar] [PubMed]
- Zanardi, I.; Borrelli, E.; Valacchi, G.; Travagli, V.; Bocci, V. Ozone: A Multifaceted Molecule with Unexpected Therapeutic Activity. Curr. Med. Chem. 2016, 23, 304–314. [Google Scholar] [CrossRef]
- Park, J.-S.; Sung, B.-J.; Yoon, K.-S.; Jeong, C.-S. The bactericidal effect of an ionizer under low concentration of ozone. BMC Microbiol. 2016, 16, 173. [Google Scholar] [CrossRef]
- Huth, K.C.; Jakob, F.M.; Saugel, B.; Cappello, C.; Paschos, E.; Hollweck, R.; Hickel, R.; Brand, K. Effect of ozone on oral cells compared with established antimicrobials. Eur. J. Oral. Sci. 2006, 114, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Al-Omiri, M.K.; Alhijawi, M.; AlZarea, B.K.; Hassan, R.S.A.; Lynch, E. Ozone treatment of recurrent aphthous stomatitis: A double blinded study. Sci. Rep. 2016, 6, 27772. [Google Scholar] [CrossRef] [PubMed]
- Yiğitarslan, K.; Özcan, C.; Cetintav, B. Thermographic Examination of the Gingiva of 16 Dogs. J. Vet. Dent. 2023, 40, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Zacher, A.; Marretta, S.M. Diagnosis and Management of Furcation Lesions in Dogs—A Review. J. Vet. Dent. 2022, 39, 151–172. [Google Scholar] [CrossRef] [PubMed]
- Bocci, V. Scientific and medical aspects of ozone therapy. State of the art. Arch. Med. Res. 2006, 37, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Bocci, V. Ossigeno Ozono Terapia: Comprensione dei Meccanismi di Azione e Possibilità Terapeutiche; CEA: Milan, Italy, 2000. [Google Scholar]
- ISO 7932: 2004; Microbiology of Food and Animal Feeding Stuffs—Horizontal Method for the Enumeration of Presumptive Bacillus Cereus—Colony-Count Technique at 30 Degrees C. ISO: Geneva, Switzerland, 2004.
- Dalmaso, G.; Bini, M. Qualification of high recovery, flocked swabs as compared to traditional rayon swabs for microbiological environmental monitoring of surfaces. PDA J. Pharm. Sci. Technol. 2008, 62, 191–199. [Google Scholar] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; The R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Harvey, C.E. Management of periodontal disease: Understanding the options. Vet. Clin. N. Am. Small Anim. Pract. 2005, 35, 819–836. [Google Scholar] [CrossRef] [PubMed]
- Blazevich, M.; Miles, C. The Presence of Bacteremia in 13 Dogs Undergoing Oral Surgery Without the Use of Antibiotic Therapy. J. Vet. Dent. 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Fossum, T.W. Small Animal Surgery; Mosby Elsevier: St. Louis, MO, USA, 2007; pp. 93–95. [Google Scholar]
- Elliott, D.R.; Wilson, M.; Buckley, C.M.F.; Spratt, D.A. Aggregative Behavior of Bacteria Isolated from Canine Dental Plaque. Appl. Environ. Microbiol. 2006, 72, 5211–5217. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dahlén, G.; Charalampakis, G.; Abrahamsson, I.; Bengtsson, L.; Falsen, E. Predominant bacterial species in subgingival plaque in dogs. J. Periodontal Res. 2012, 47, 354–364. [Google Scholar] [CrossRef]
- Lawler, B.; Sambrook, P.J. Antibiotic prophylaxis for dentoalveolar surgery: Is it indicated? Aust. Dent. J. 2005, 50 (Suppl. S2), S54–S59. [Google Scholar] [CrossRef]
- Qiu, W.; Zhou, Y.; Li, Z.; Huang, T.; Xiao, Y.; Cheng, L.; Peng, X.; Zhang, L.; Ren, B. Application of Antibiotics/Antimicrobial Agents on Dental Caries. BioMed Res. Int. 2020, 2020, 5658212. [Google Scholar] [CrossRef]
- Eick, S.; Tigan, M. Effect of ozone on periodontopathogenic species—An in vitro study. Clin. Oral Investig. 2012, 16, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Ahmedi, J.; Ahmedi, E. Efficiency of gaseous ozone in reducing the development of dry socket following surgical third molar extraction. Eur. J. Dent. 2016, 10, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Ebensberger, U.; Pohl, Y. PCNA-expression of cementoblasts and fibroblasts on the root surface after extraoral rinsing for decontamination. Dent. Traumatol. 2002, 18, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Cline, N.V.; Layman, D.L. The effects of chlorhexidine on the attachment and growth of cultured human periodontal cells. J. Periodontol. 1992, 63, 598–602. [Google Scholar] [CrossRef]
- Liu, J.X.; Werner, J. Cytotoxicity evaluation of chlorhexidine gluconate on human fibroblasts, myoblasts, and osteoblasts. J. Bone Jt. Infect. 2018, 3, 165–172. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melanie, P.; Niola, C.; Plataroti, I.; Mancini, S.; Fratini, F. Use of Ozone in Veterinary Dentistry as an Alternative to Conventional Antibiotics and Antiseptics. Vet. Sci. 2024, 11, 163. https://doi.org/10.3390/vetsci11040163
Melanie P, Niola C, Plataroti I, Mancini S, Fratini F. Use of Ozone in Veterinary Dentistry as an Alternative to Conventional Antibiotics and Antiseptics. Veterinary Sciences. 2024; 11(4):163. https://doi.org/10.3390/vetsci11040163
Chicago/Turabian StyleMelanie, Pierre, Carlotta Niola, Ilaria Plataroti, Simone Mancini, and Filippo Fratini. 2024. "Use of Ozone in Veterinary Dentistry as an Alternative to Conventional Antibiotics and Antiseptics" Veterinary Sciences 11, no. 4: 163. https://doi.org/10.3390/vetsci11040163
APA StyleMelanie, P., Niola, C., Plataroti, I., Mancini, S., & Fratini, F. (2024). Use of Ozone in Veterinary Dentistry as an Alternative to Conventional Antibiotics and Antiseptics. Veterinary Sciences, 11(4), 163. https://doi.org/10.3390/vetsci11040163