
Congenital Partial Colonic Agenesis in Dogs and Cats: Clinical, Biological, Diagnostic Imaging, Endoscopic and Histopathologic Characterization, a Retrospective Study

Abstract
:Simple Summary
Abstract
1. Introduction
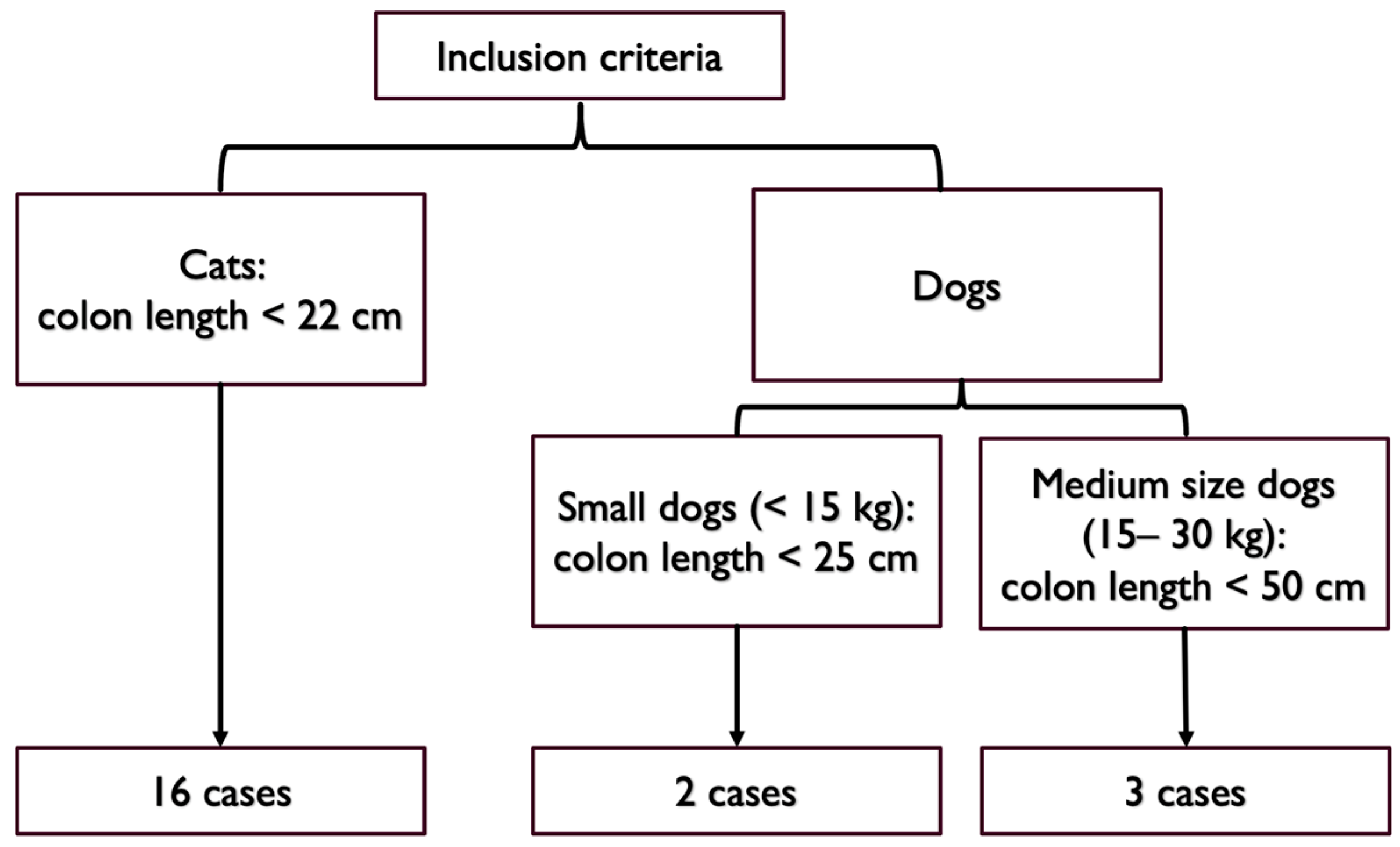
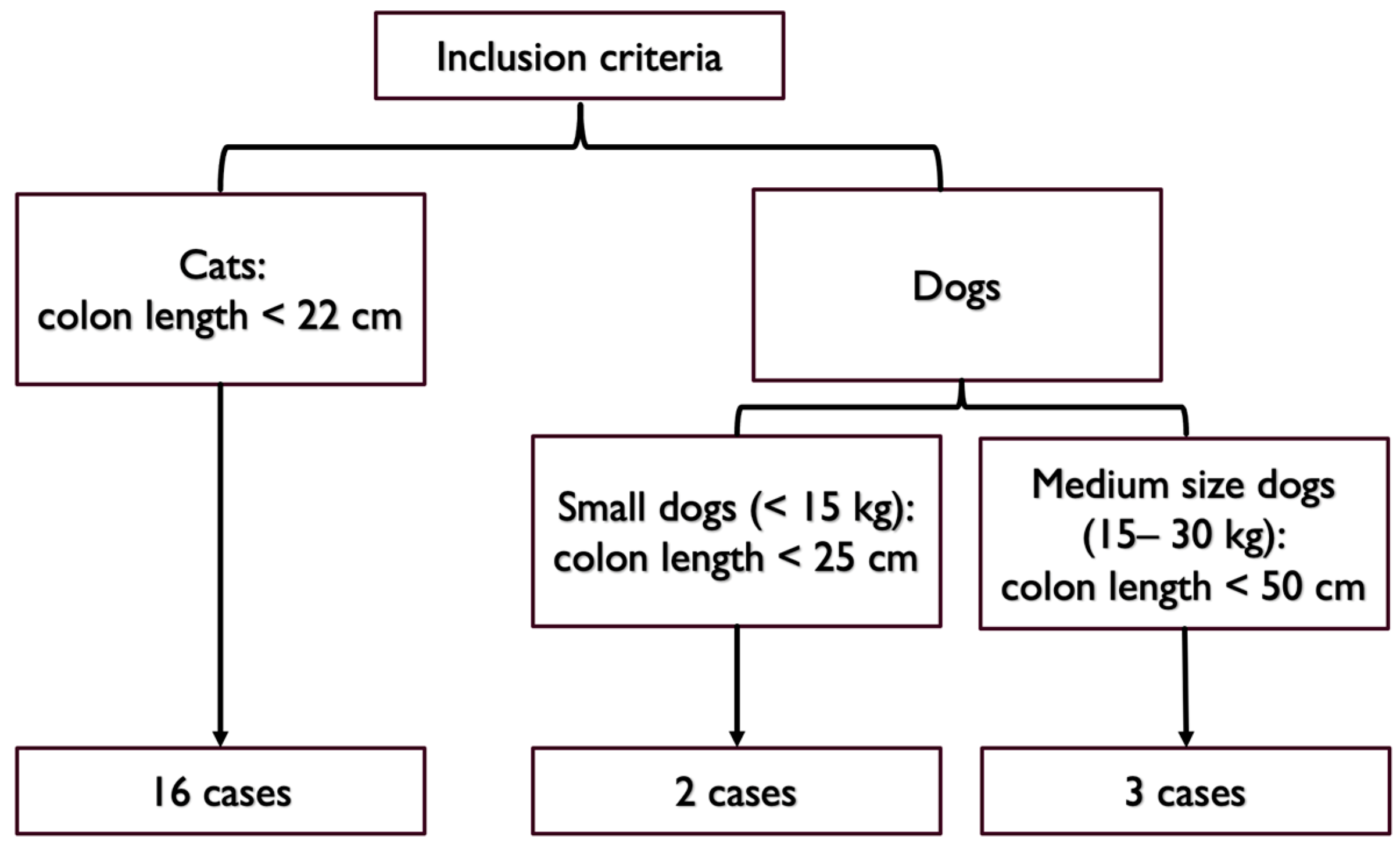
2. Materials and Methods
3. Results
3.1. Epidemiological and Clinical Data
3.2. Diagnostic Tests
3.2.1. Hematochemical Analysis
3.2.2. Abdominal Ultrasound
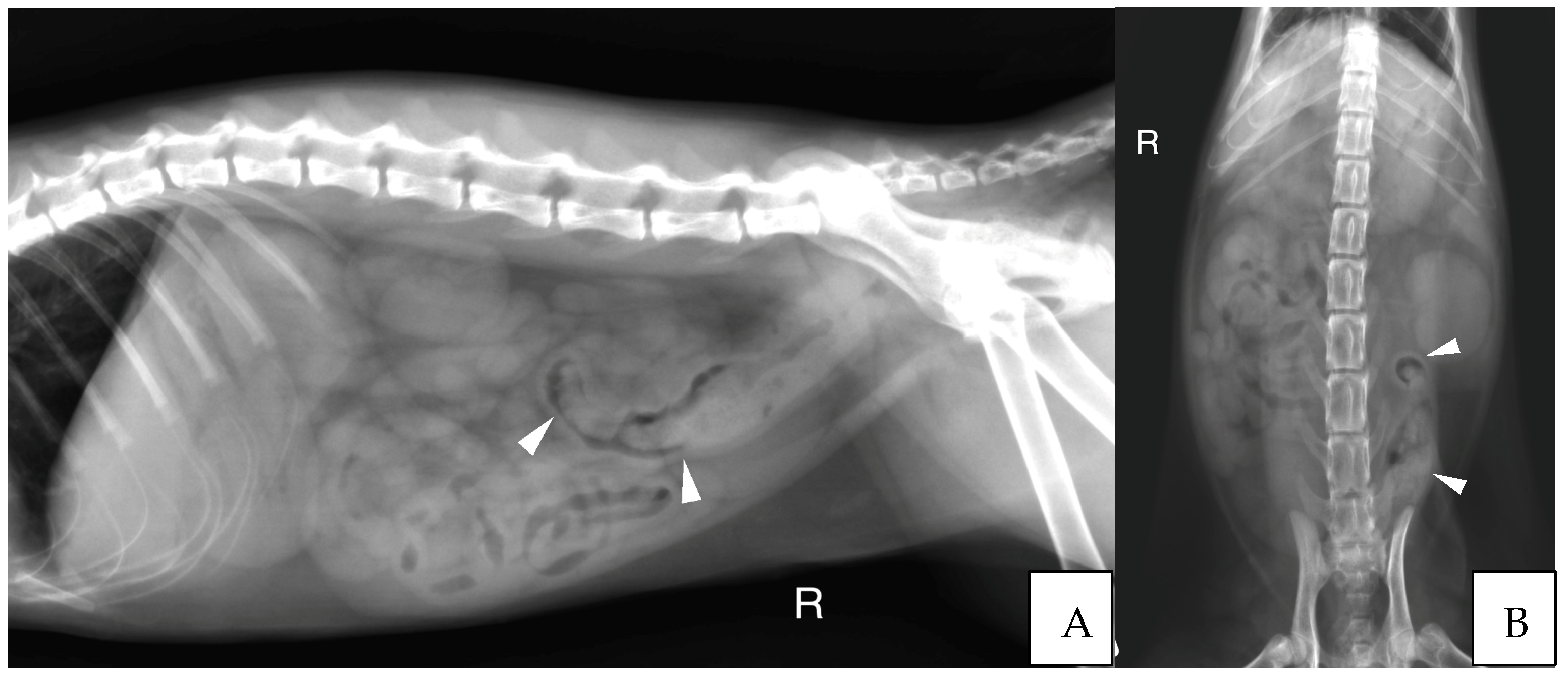
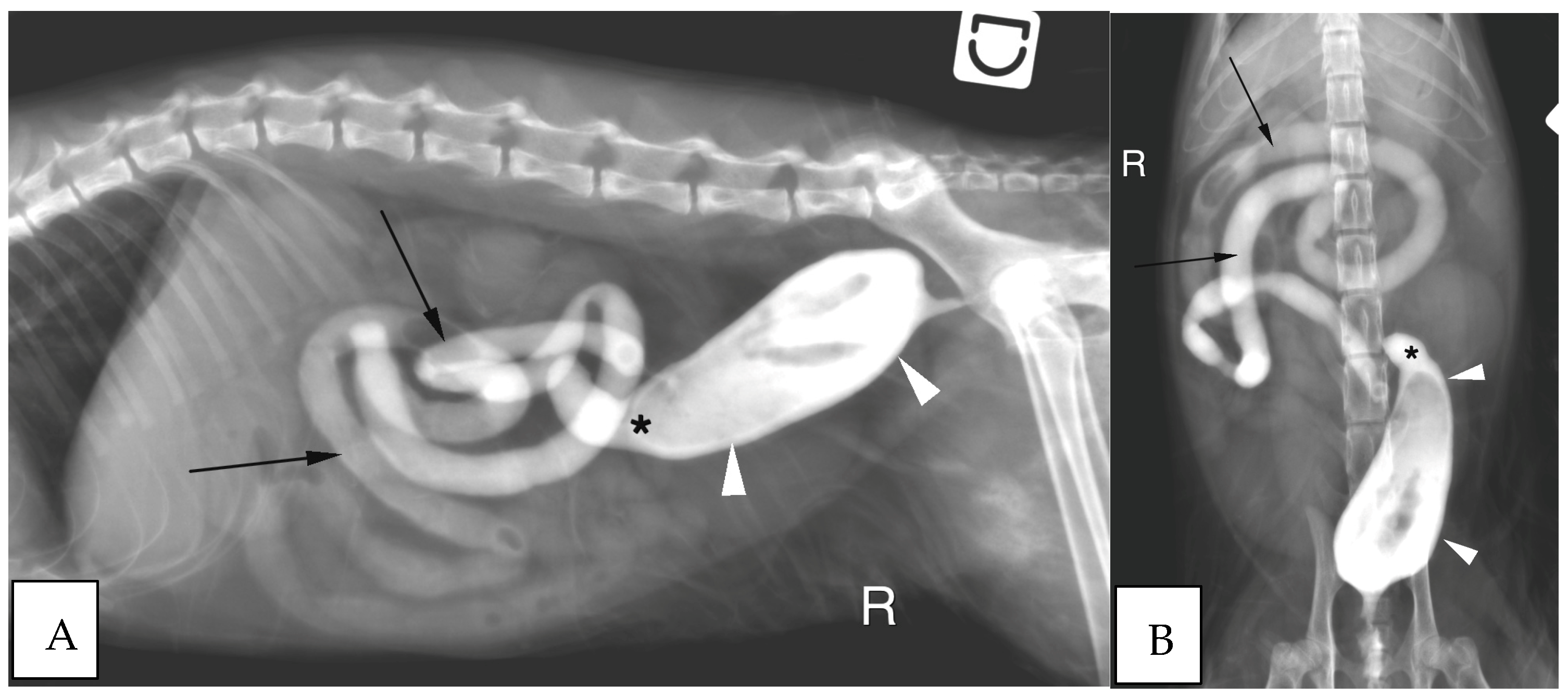
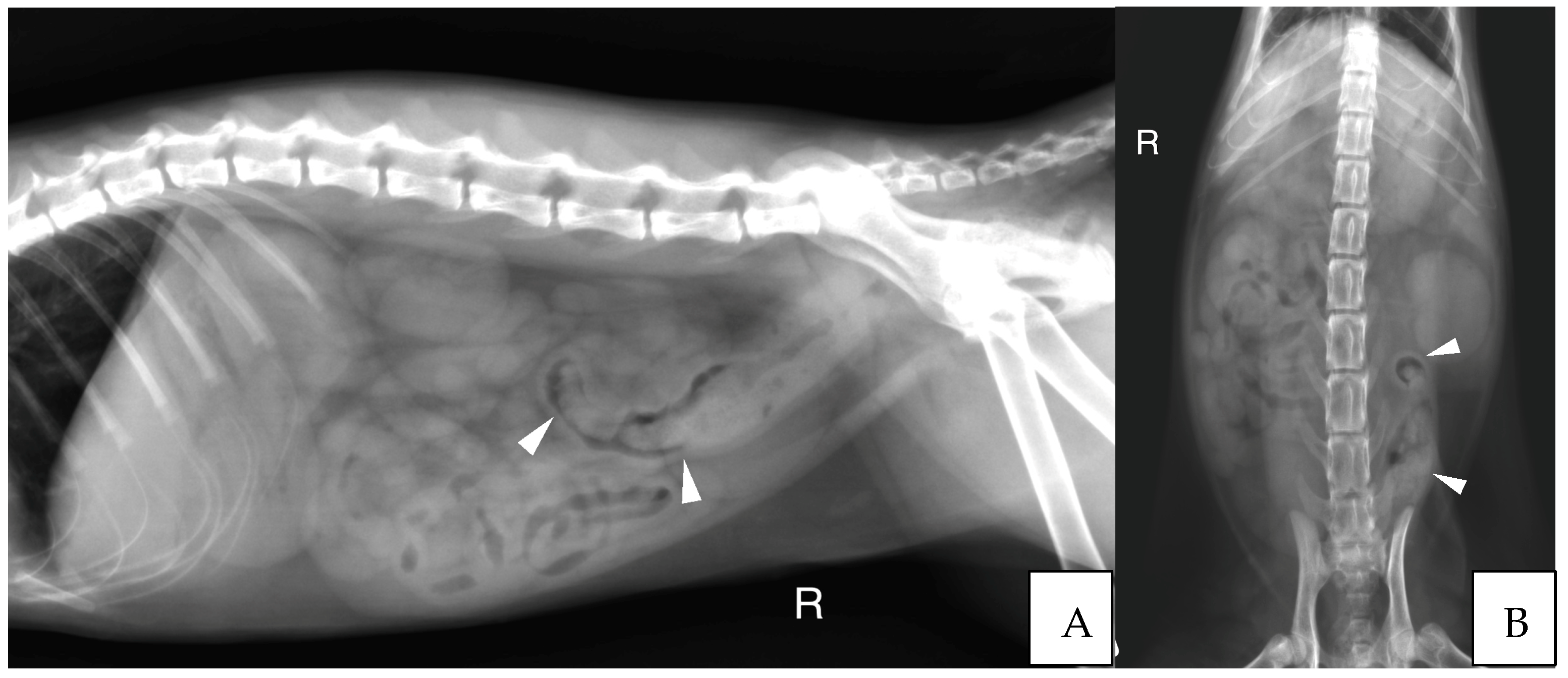
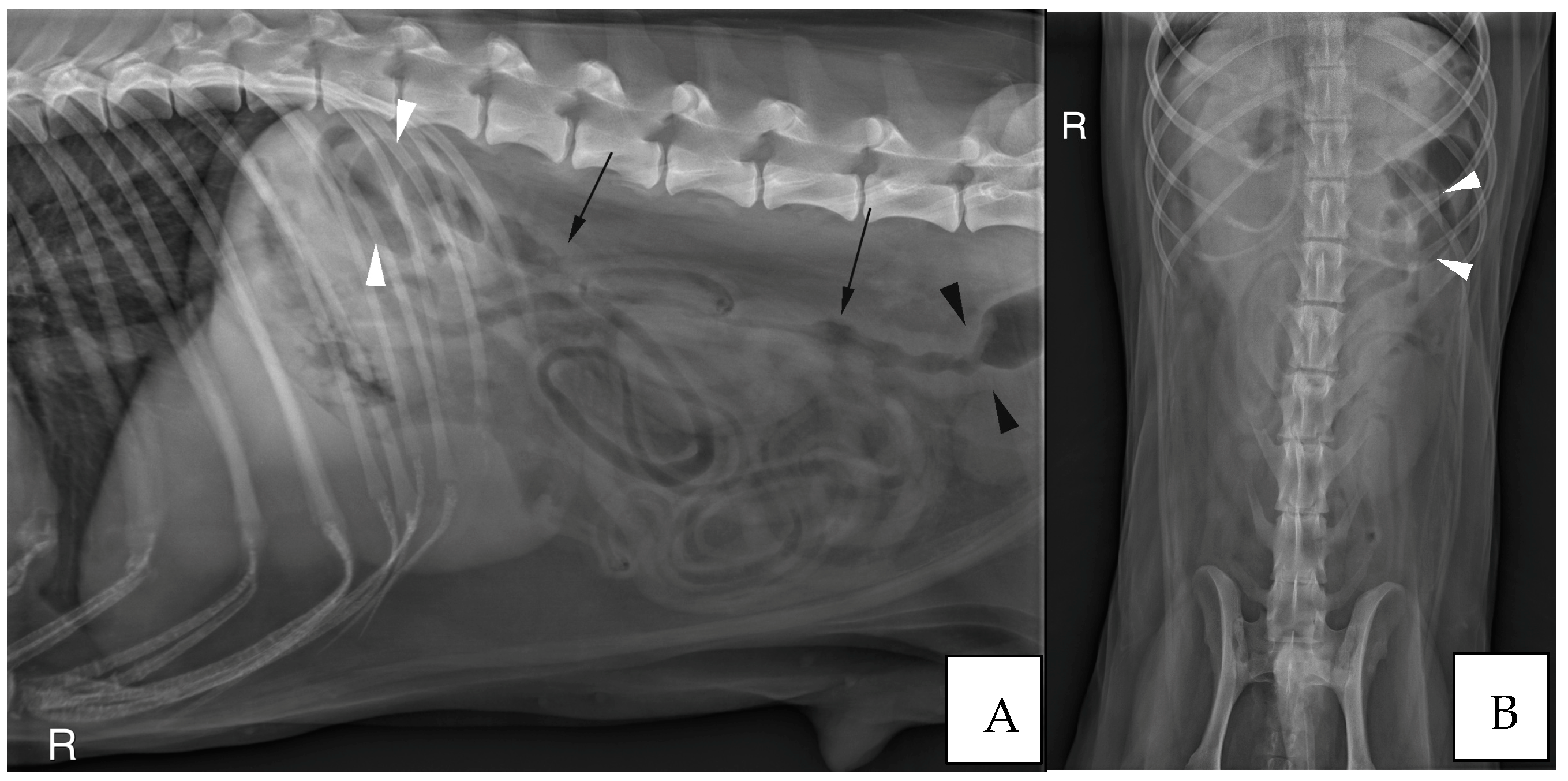
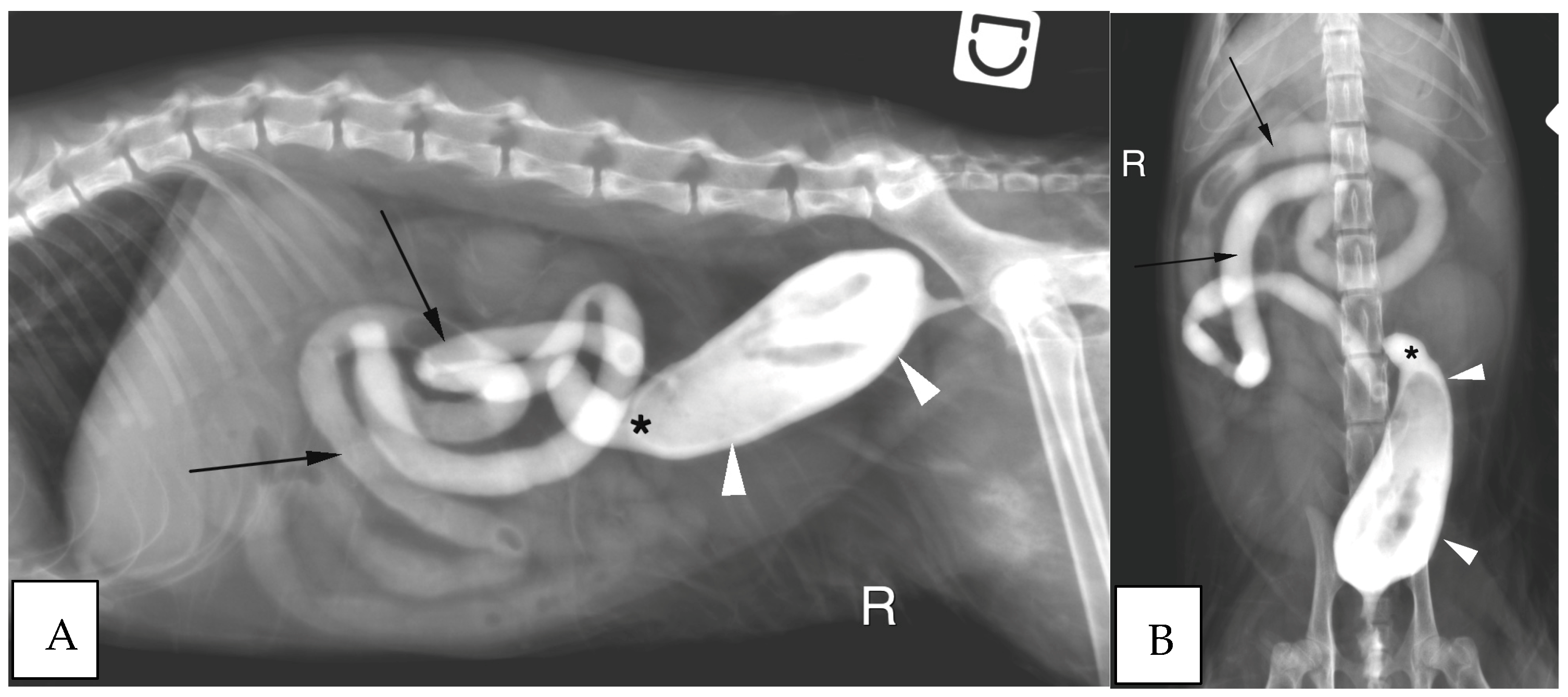
3.2.3. Abdominal Radiographs
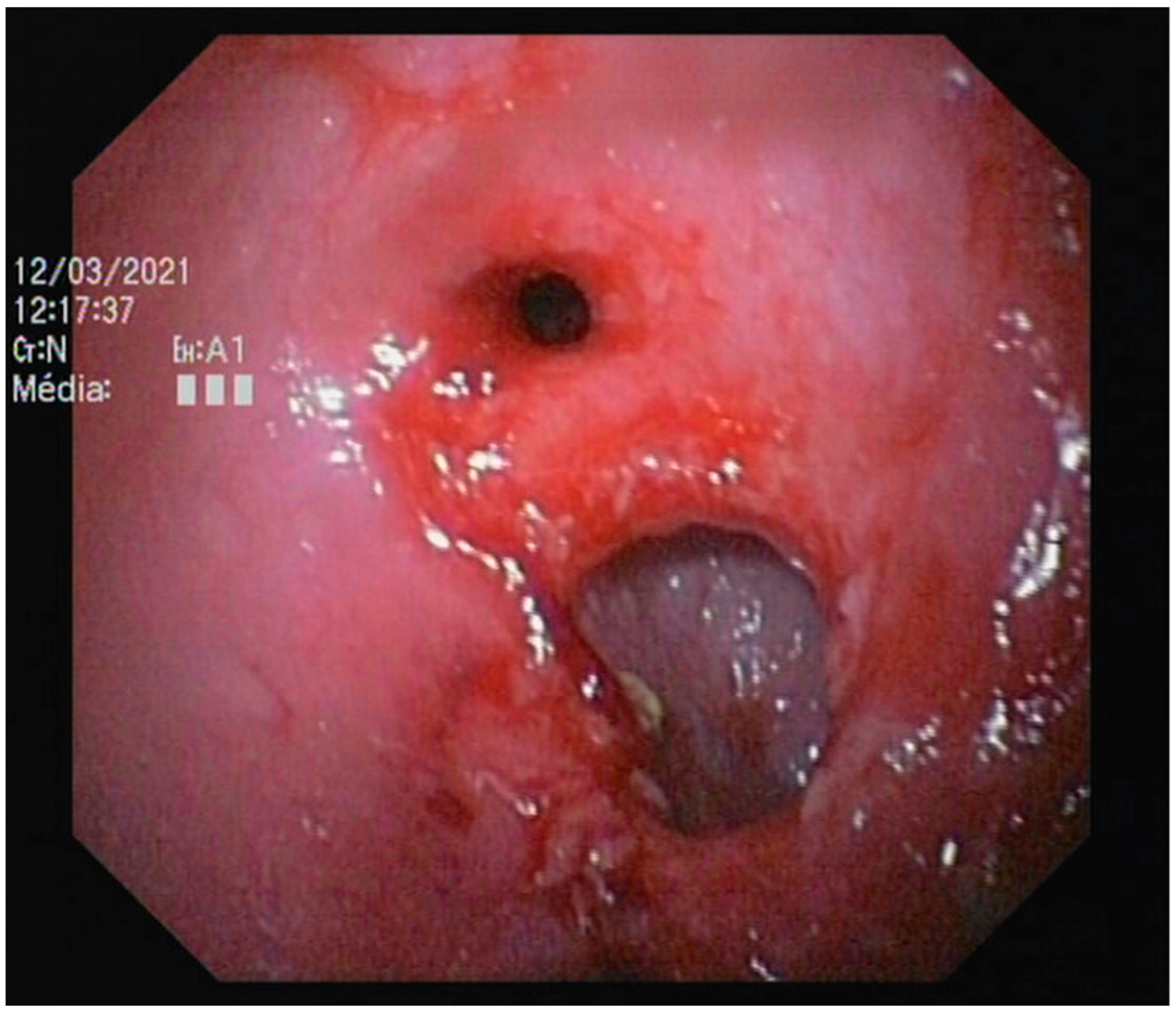
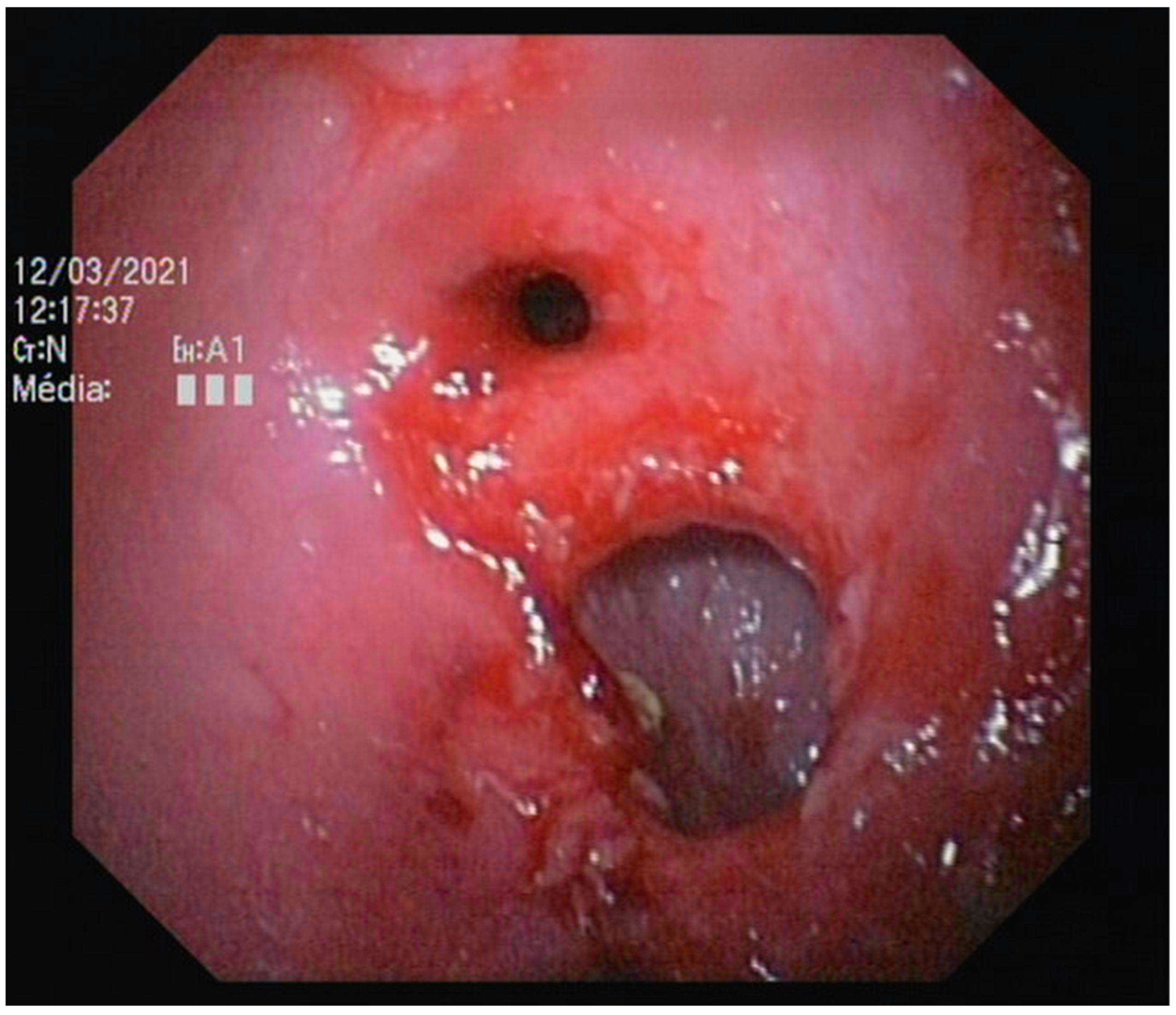
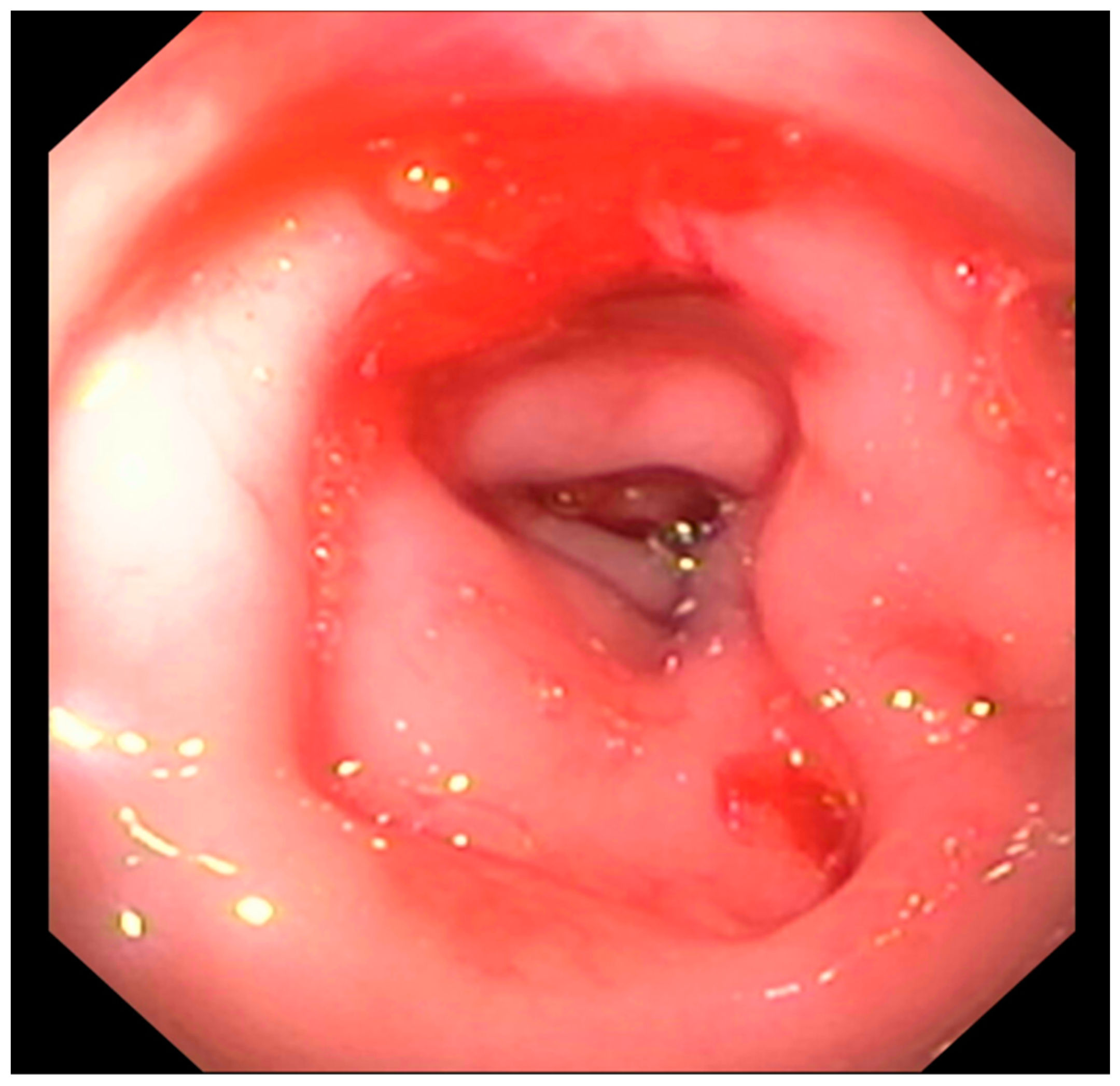
3.2.4. Endoscopic Findings
3.2.5. Histology
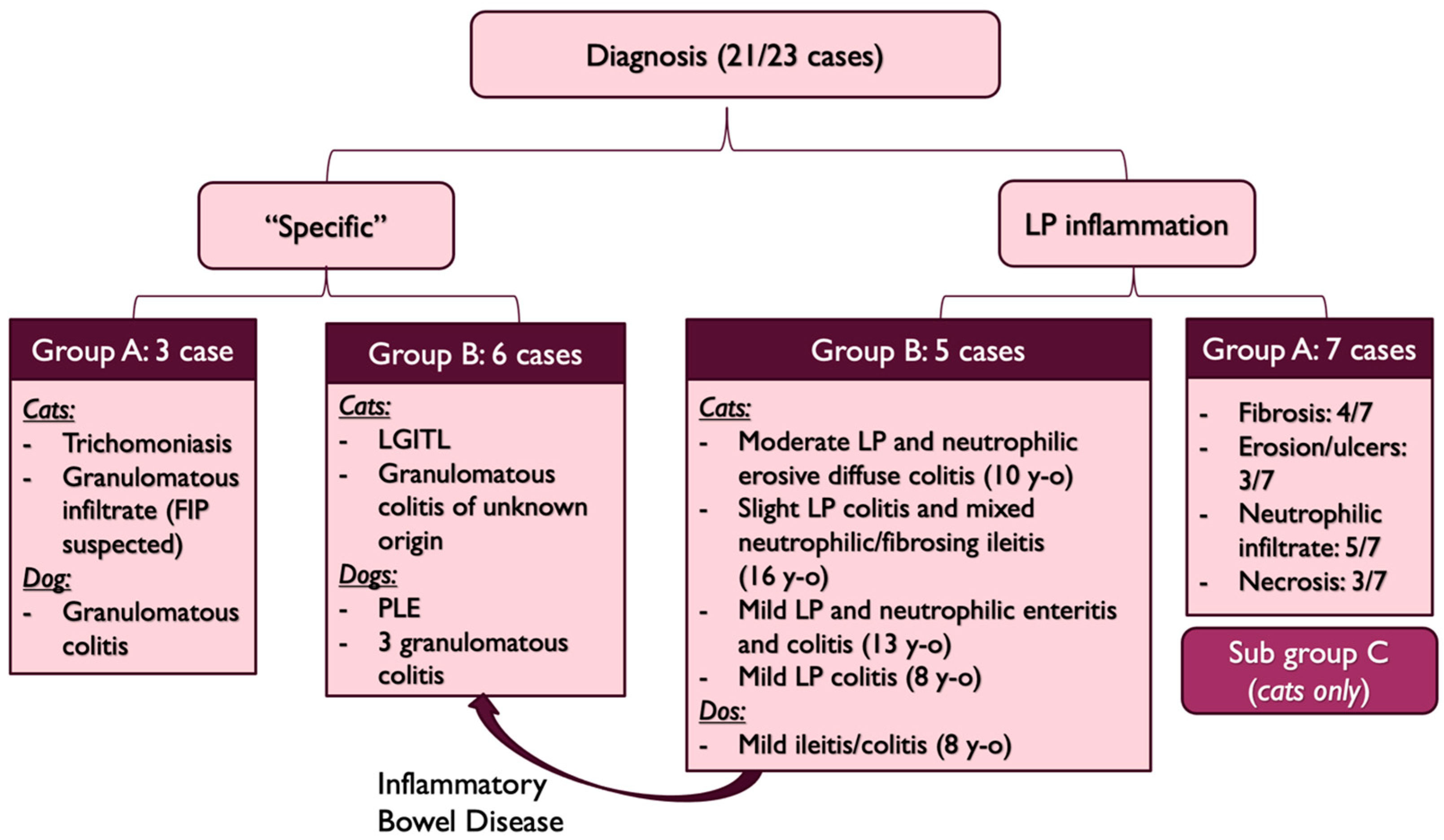
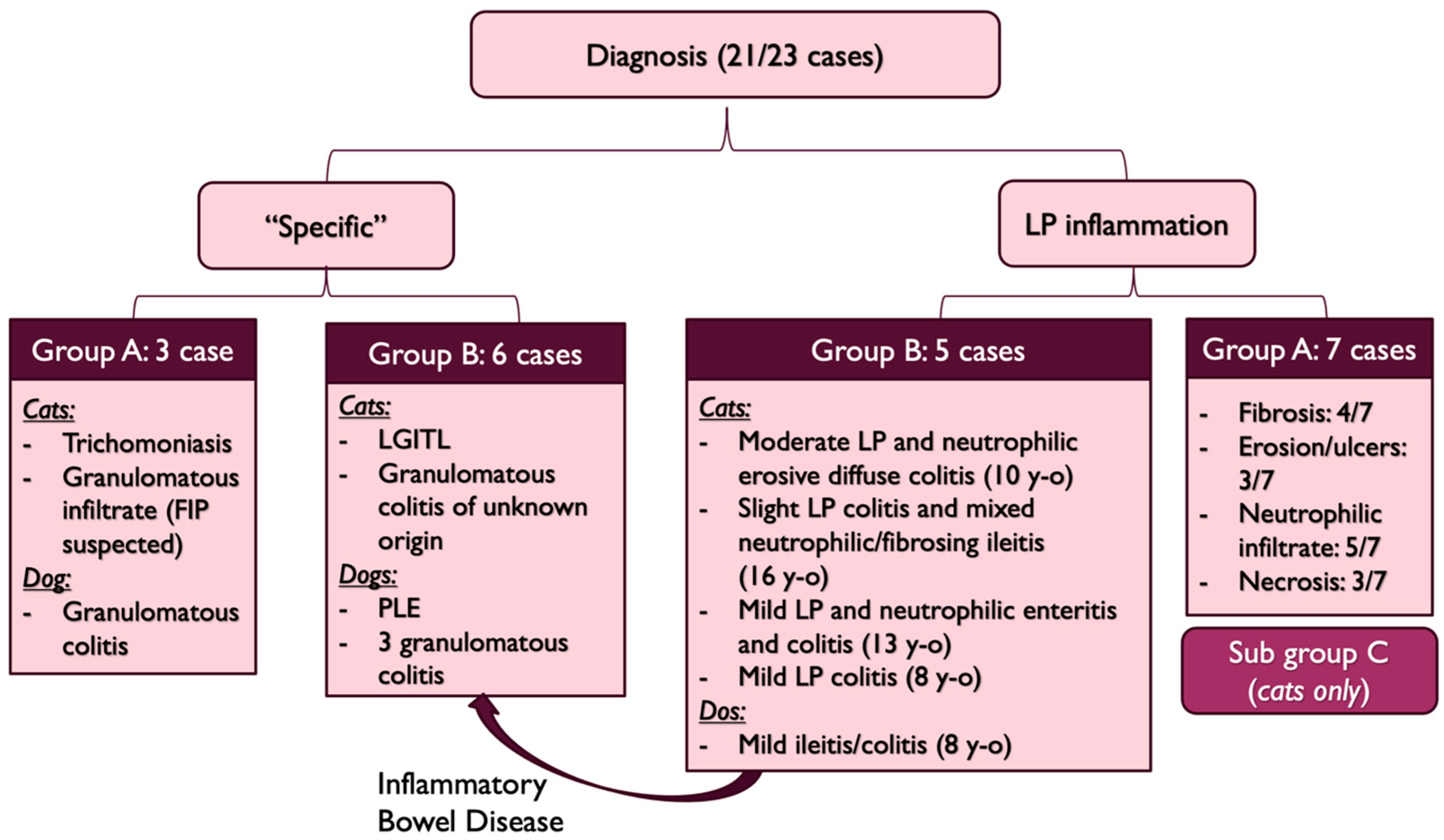
3.2.6. Diagnosis
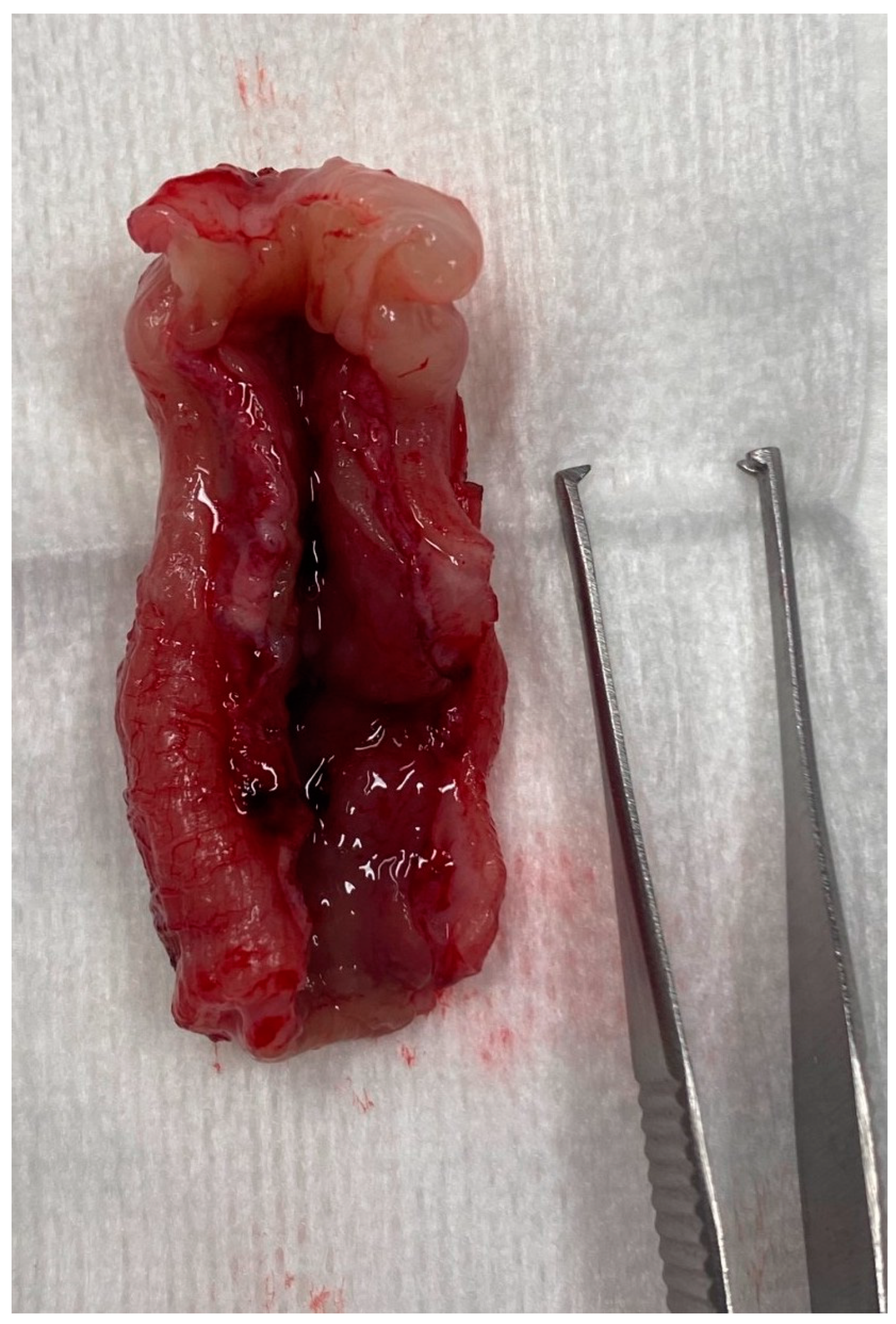
3.2.7. Management and Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Evans, H.E.; De Lahunta, A. The digestive apparatus and abdomen—Chapter 7. In Miller’s Anatomy of the Dog, 4th ed.; Elsevier Saunders: St. Louis, Missouri, USA, 2013; pp. 322–327. [Google Scholar]
- Washabau, R. Chapter 58—Large Intestine. In Canine and Feline Gastroenterology; Elsevier: St. Louis, Missouri, USA, 2013; pp. 729–777. [Google Scholar]
- Fruehwald, C.; Ellison, G. Successful Surgical Correction of Congenital Colonic Duplication and Anogenital Cleft in a Cat. J. Am. Anim. Hosp. Assoc. 2020, 56, 170–174. [Google Scholar] [CrossRef]
- Lecoindre, A.; Saade, D.; Barthez, P.; Cadoré, J.L. Congenital duodenocolic fistula in a dog. J. Small Anim. Pract. 2018, 59, 311–314. [Google Scholar] [CrossRef]
- Van der Gaag, I.; Tibboel, D. Intestinal atresia and stenosis in animals: A report of 34 cases. Vet. Pathol. 1980, 17, 565–574. [Google Scholar] [CrossRef] [PubMed]
- de Battisti, A.; Harran, N.; Chanoit, G.; Warren-Smith, C. Use of negative contrast computed tomography for diagnosis of a colonic duplication in a dog. J. Small Anim. Pract. 2013, 54, 547–550. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.J. Chapter 277: Diseases of the Large Intestine. In Textbook of Veterinary Internal Medicine, 8th ed.; Elsevier Health Sciences: St. Louis, Missouri, USA, 2016; pp. 1565–1592. [Google Scholar]
- Kararli, T.T. Comparison of the gastrointestinal anatomy, physiology, and biochemistry of humans and commonly used laboratory animals. Biopharm. Drug Dispos. 1995, 16, 351–380. [Google Scholar] [CrossRef]
- Sturgess, C.; Canfield, P.; Gruffydd-Jones, T.; Stokes, C. A gross and microscopical morphometric evaluation of feline large intestinal anatomy. J. Comp. Pathol. 2001, 124, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.B.; Rodriguez, A.; Colquhoun, J.K.; Stämpfli, H. Congenital colonic malformation (“short colon”) in a 4-month-old standardbred foal. Can. Vet. J. 2007, 48, 420–422. [Google Scholar]
- Fluke, M.H.; Hawkins, E.C.; Elliott, G.S.; Blevins, W.E. Short colon in two cats and a dog. J. Am. Vet. Med. Assoc. 1989, 195, 87–90. [Google Scholar]
- Schlesinger, D.P.; Philibert, D.; Breur, G.J. Agenesis of the cecum and the ascending and transverse colon in a 12-yer-old cat. Can. Vet. J. 1992, 33, 544–546. [Google Scholar] [PubMed]
- Deschamps, C.; Humbert, D.; Zentek, J.; Denis, S.; Priymenko, N.; Apper, E.; Blanquet-Diot, S. From Chihuahua to Saint-Bernard: How did digestion and microbiota evolve with dog sizes. Int. J. Biol. Sci. 2022, 18, 5086–5102. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.P.; Biourge, V.C.; Nguyen, P.G. Digestive sensitivity varies according to size of dogs: A review. J. Anim. Physiol. Anim. Nutr. 2017, 101, 1–9. [Google Scholar] [CrossRef]
- Penninck, D.; D’anjou, M.-A. Gastrointestinal tract chapter. In Atlas of Small Animal Ultrasonography, 2nd ed.; John Wiley and Sons Ltd.: Ames, IA, USA, 2015; pp. 259–308. [Google Scholar]
- Di Donato, P.; Penninck, D.; Pietra, M.; Cipone, M.; Diana, A. Ultrasonographic measurement of the relative thickness of intestinal wall layers in clinically healthy cats. J. Feline Med. Surg. 2014, 16, 333–339. [Google Scholar] [CrossRef]
- Gladwin, N.E.; Penninck, D.G.; Webster, C.R.L. Ultrasonographic evaluation of the thickness of the wall layers in the intestinal tract of dogs. Am. J. Vet. Res. 2014, 75, 349–353. [Google Scholar] [CrossRef]
- Group TWIGS; Washabau, R.J.; Day, M.J.; Willard, M.D.; Hall, E.J.; Jergens, A.E.; Mansell, J.; Minami, T.; Bilzer, T.W. Endoscopic, Biopsy, and Histopathologic Guidelines for the Evaluation of Gastrointestinal Inflammation in Companion Animals. J. Vet. Intern. Med. 2010, 24, 10–26. [Google Scholar]
- Xenoulis, P.; Zoran, D.; Fosgate, G.; Suchodolski, J.; Steiner, J. Feline Exocrine Pancreatic Insufficiency: A Retrospective Study of 150 Cases. J. Vet. Intern. Med. 2016, 30, 1790–1797. [Google Scholar] [CrossRef] [PubMed]
- Lamoureux, A.; Maurey, C.; Freiche, V. Treatment of inflammatory rectal strictures by digital bougienage: A retrospective study of nine cases. J. Small Anim. Pract. 2017, 58, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Brochard, C.; Siproudhis, L.; Wallenhorst, T.; Cuen, D.; D’Halluin, P.N.; Garros, A.; Bretagne, J.-F.; Bouguen, G. Anorectal stricture in 102 patients with Crohn’s disease: Natural history in the era of biologics. Aliment. Pharmacol. Ther. 2014, 40, 796–803. [Google Scholar] [CrossRef]
- Chang, C.-W.; Wong, J.-M.; Tung, C.-C.; Shih, I.-L.; Wang, H.-Y.; Wei, S.-C. Intestinal Stricture in Crohn’s Disease. Intest. Res. 2015, 13, 19–26. [Google Scholar] [CrossRef]
- Solitano, V.; Dal Buono, A.; Gabbiadini, R.; Wozny, M.; Repici, A.; Spinelli, A.; Vetrano, S.; Armuzzi, A. Fibro-Stenosing Crohn’s Disease: What Is New and What Is Next? J. Clin. Med. 2023, 12, 3052. [Google Scholar] [CrossRef]
- Hayashi, Y.; Nakase, H. The Molecular Mechanisms of Intestinal Inflammation and Fibrosis in Crohn’s Disease. Front. Physiol. 2022, 13, 845078. [Google Scholar] [CrossRef]
- Kouti, V.; Papazoglou, L.; Rallis, T. Short-Bowel Syndrome in Dogs and Cats. Compend. Contin. Educ. Pract. Vet. 2006, 28, 182–193. [Google Scholar]
- Vanderhoof, J.A.; Langnas, A.N.; Pinch, L.W.; Thompson, J.S.; Kaufman, S.S. Short bowel syndrome. J. Pediatr Gastroenterol. Nutr. 1992, 14, 359–370. [Google Scholar] [CrossRef]
- Jimba, Y.; Nagao, J.; Sumiyama, Y. Changes in Gastrointestinal Motility After Subtotal Colectomy in Dogs. Surg. Today 2002, 32, 1048–1057. [Google Scholar] [CrossRef]
- Clancy, C.S.; Jensen, K.A.; Van Wettere, A.J. Congenital Short-Bowel Syndrome in an Adult Dog. Vet. Pathol. 2018, 55, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Wakhlu, A.K.; Wakhlu, A.; Pandey, A.; Agarwal, R.; Tandon, R.K.; Kureel, S.N. Congenital short colon. World J. Surg. 1996, 20, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Chadha, R.; Khan, N.A. Congenital Pouch Colon. J. Indian Assoc. Pediatr. Surg 2017, 22, 69–78. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Species | Breed | Age (Months) | Sexes | Weight (kg) | Outdoor /Indoor | Deworming | Food Supplied | Vaccination Status |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Cat | Bengal | 16 | Female | 2.26 | Indoor | P + M | Hyperdigestible | Up to date |
| 2 | Cat | Savannah | 13 | Female | 2.3 | Indoor | F | Hydrolyzed | Up to date |
| 3 | Cat | Exotic Shorthair | 48 | Male | 3.2 | Indoor | None | Hyperdigestible | Up to date |
| 4 | Cat | DSH | 160 | Male | 4.2 | Outdoor | P + M | Hyperdigestible | Up to date |
| 5 | Cat | Bengal | 120 | Male | 3.6 | Indoor | P + M | Urinary diet | Up to date |
| 6 | Cat | DSH | 11 | Male | 2.2 | ? | ? | Home-made diet | ? |
| 7 | Cat | Persian | 120 | Male | 4.3 | Indoor | P + M | Hyperdigestible | Up to date |
| 8 | Cat | DSH | 12 | Male | 2.7 | Indoor | P + M | Hydrolyzed | Up to date |
| 9 | Cat | DSH | 130 | Male | 5.1 | Outdoor | P + M | ? | Up to date |
| 10 | Cat | Siberian | 12 | Male | 3.7 | ? | F | Conventional diet | Up to date |
| 11 | Cat | Scottish | 6.5 | Male | 2.3 | Indoor | ? | Hyperdigestible | Out of date |
| 12 | Cat | Chartreux | 192 | Male | 6.3 | Outdoor | P + M | Urinary diet | Up to date |
| 13 | Cat | Birman | 96 | Female | 2.25 | Indoor | P + M | Hydrolyzed | Up to date |
| 14 | Cat | Burmese | 156 | Female | 1.9 | Indoor | ? | Hyperdigestible | Up to date |
| 15 | Cat | Abyssinian | 81 | Female | 3.6 | Indoor | P + M | Hyperdigestible | Up to date |
| 16 | Cat | DSH | 103 | Female | 3.3 | Indoor | None | Conventional diet | Out of date |
| 17 | Cat | Bengal | 18 | Female | 2.6 | Outdoor | F | Hyperdigestible | Up to date |
| 18 | Dog | Collie | 96 | Male | 26.5 | Outdoor | ? | Home-made diet | Up to date |
| 19 | Dog | Boxer | 4 | Female | 15 | Outdoor | F | Conventional diet | Up to date |
| 20 | Dog | French Bulldog | 16 | Female | 9.7 | Outdoor | F | Hyperdigestible | Up to date |
| 21 | Dog | Whippet | 108 | Male | 10.8 | Outdoor | None | Urinary diet | Up to date |
| 22 | Dog | French bulldog | 60 | Female | 8.5 | Outdoor | P + M | Conventional diet | Up to date |
| 23 | Dog | Boxer | 52 | Female | 30.5 | Outdoor | P + M | Hyperdigestible | Up to date |
| Number | Stools (S, W, N, M) | Hematochezia (y/n) | Mucous (y/n) | Urgency to Defecate (y/n) | Dyschezia/ Tenesmus (y/n) | Appetite (N, P, D) | Weight Loss/Failure to Grow (y/n) | Increased Frequency of Defecation (y/n) | Vomiting (y/n) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | N | y | n | y | y | N | y | y | n |
| 2 | W | n | n | y | n | N | y | y | y |
| 3 | W | y | y | n | n | N | y | ? | y |
| 4 | M | y | n | n | n | N | n | n | n |
| 5 | M | y | n | n | n | N | n | y | y |
| 6 | W | y | n | ? | y | N | y | ? | y |
| 7 | S | y | y | n | n | N | n | y | n |
| 8 | M | y | n | y | y | P | y | y | n |
| 9 | N | n | n | n | n | D | n | n | y |
| 10 | S | n | y | n | y | N | n | y | n |
| 11 | W | y | y | y | y | N | n | y | n |
| 12 | M | n | n | n | n | D | y | n | n |
| 13 | M | n | n | n | n | N | y | y | y |
| 14 | W | n | n | n | n | N | y | n | y |
| 15 | W | n | n | n | n | N | n | y | n |
| 16 | W | n | n | y | n | N | n | y | n |
| 17 | W | n | n | y | n | N | y | y | n |
| 18 | W | y | n | n | n | N | y | y | n |
| 19 | S | y | y | y | y | N | n | ? | n |
| 20 | S | y | y | y | n | N | n | ? | n |
| 21 | S | n | n | n | n | D | n | y | n |
| 22 | W | n | n | n | n | D | y | n | y |
| 23 | S | y | n | n | n | N | n | n | n |
| Number | Stools (S, W, N, M) | Hematochezia (y/n) | Mucous (y/n) | Urgency to Defecate (y/n) | Dyschezia/ Tenesmus (y/n) | Appetite (N, P, D) | Weight Loss/Failure to Grow (y/n) | Increased Frequency of Defecation (y/n) | Vomiting (y/n) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | N | y | n | y | y | N | y | y | n |
| 2 | W | n | n | y | n | N | y | y | y |
| 3 | W | y | y | n | n | N | y | ? | y |
| 4 | M | y | n | n | n | N | n | n | n |
| 6 | W | y | n | ? | y | N | y | ? | y |
| 7 | S | y | y | n | n | N | n | y | n |
| 10 | S | n | y | n | y | N | n | y | n |
| 11 | W | y | y | y | y | N | n | y | n |
| 13 | M | n | n | n | n | N | y | y | y |
| 15 | W | n | n | n | n | N | n | y | n |
| 17 | W | n | n | y | n | N | y | y | n |
| 19 | S | y | y | y | y | N | n | ? | n |
| Percentage/12 cases | N: 8.3%; M: 16.6%; S: 25%; W: 50% | Yes: 58.3% | Yes: 41.6% | Yes: 41.6% | Yes: 41.6% | N: 100% | Yes: 50% | Yes: 66.6% | Yes: 33.3% |
| Number | Stools (S, W, N, M) | Hematochezia (y/n) | Mucous (y/n) | Urgency to Defecate (y/n) | Dyschezia/ Tenesmus (y/n) | Appetite (N, P, D) | Weight Loss/Failure to Grow (y/n) | Increased Frequency of Defecation (y/n) | Vomiting (y/n) |
|---|---|---|---|---|---|---|---|---|---|
| 5 | M | y | n | n | n | N | n | y | y |
| 8 | M | y | n | y | y | P | y | y | n |
| 9 | N | n | n | n | n | D | n | n | y |
| 12 | M | n | n | n | n | D | y | n | n |
| 14 | W | n | n | n | n | N | y | n | y |
| 16 | W | n | n | y | n | N | n | y | n |
| 18 | W | y | n | n | n | N | y | y | n |
| 20 | S | y | y | y | n | N | n | ? | n |
| 21 | S | n | n | n | n | D | n | y | n |
| 22 | W | n | n | n | n | D | y | n | y |
| 23 | S | y | n | n | n | N | n | n | n |
| Percentage/11 cases | N: 9%; M: 27%; S: 27%; W: 36% | Yes: 45% | Yes: 9% | Yes: 27% | Yes: 9% | N: 54%; D: 36%; P: 9% | Yes: 45.5% | Yes: 45.5% | Yes: 36% |
| Severity of Colonic Wall Thickening | Unremarkable | Mild | Moderate | Severe |
|---|---|---|---|---|
| Group A (/11 cases) | 3 | 3 | 4 | 1 |
| Group B (/8 cases) | 3 | 2 | 2 | 1 |
| Group A (10 Cases) | Group B (10 Cases) | ||||
|---|---|---|---|---|---|
| Endoscopic Findings | Number | Percentage (/20 Endoscopies) | Number | Percentage (/20 Endoscopies) | p Value (Chi-Squared Test) |
| Ileocolic junction abnormalities | 4 | 20% | 4 | 20% | 1 |
| Stenosis | 10 | 50% | 2 | 10% | <0.001 |
| Macroscopic erosion | 1 | 5% | 4 | 20% | <0.001 |
| Nonspecific mild to moderate colopathy | 5 | 25% | 3 | 15% | 0.077 |
| Unremarkable | 1 | 5% | 1 | 5% | 1 |
| Group A (9 Cases) | Group B (11 Cases) | |||
|---|---|---|---|---|
| Histological Findings | Number | Percentage (/20 Endoscopies) | Number | Percentage (/20 Endoscopies) |
| Mild-to-moderate LP infiltration | 6 | 30% | 10 | 50% |
| Marked LP infiltration | 2 | 10% | 1 | 5% |
| Neutrophilic infiltration | 5 | 25% | 4 | 20% |
| Fibrosis | 4 | 20% | 2 | 10% |
| Eosinophilic infiltration | 0 | 0% | 2 | 10% |
| Erosion/ulcers | 3 | 15% | 3 | 15% |
| Group | Case Number | Diagnosis | Treatment | Outcome |
|---|---|---|---|---|
| A | 1 | Subgroup C and stenosis (C) | Colectomy | Died in the post operative period |
| 2 | Subgroup C and stenosis (C) | Bougienage, amoxicillin/clavulanic acid 25 mg/kg q12h PO (Clavaseptin®), metronidazole 10 mg/kg q12h PO (Flagyl®), prednisolone 0.5 mg/kg/d PO (Microsolone®), probiotics (Fortiflora®), pancreatic enzymes supplementation 12 500 U/cat q12h PO (Eurobiol®), cobalamine 250 µg/cat once a week SC (Vitamine B12 Lavoisier®), diosmectite 0.75 g/kg q12h PO (Smecta®), hyperdigestible diet | Lost to follow-up | |
| 3 | Tritrichomonosis (C) | Ronidazole 30 mg/kg/d PO (pharmaceutical compounding) | Lost to follow-up | |
| 4 | Subgroup C and stenosis (C) | Metronidazole 14 mg/kg q12h PO (Metrobactin®), prednisolone 0.7 mg/kg/d PO (Microsolone®), hyperdigestible diet | Lost to follow-up | |
| 6 | Subgroup C and stenosis (C) | Colonic stent and bougienage, intra-rectal lidocaine 2% q12h (Titanoreine®), prednisolone 1 mg/kg/d PO (Microsolone®), metronidazole 11 mg/kg q12h PO (Eradia®), pancreatic enzymes 12,500 U/cat q12h PO (Eurobiol®), hyperdigestible diet, diosmectite 0.7 g/kg q12h PO (Smecta®) | Marked improvement | |
| 7 | Subgroup C with variable degree of LP inflammation (C) | Prendnisolone 0.5 mg/kg/d PO (Dermipred®) | Lost to follow up | |
| 10 | Short colon with stenosis. Granulomatous infiltrate (FIP suspected) (C) | Colectomy then prednisolone 1.5 mg/kg PO (Dermipred®), diosmectite PO if needed 1 g/kg q12h (Smecta®), metronidazole 19 mg/kg q12h PO (Metrobactin®) and GS 441524 SC | Mild improvement | |
| 11 | Subgroup C and stenosis (C) | Metronidazole 8 mg/kg & spiramycin 50,000 U/kg q12h PO (Stomorgyl PA®), Lactulose 0.5 mL/kg q12h PO (Laxatract®) and a/d food | Marked improvement | |
| 13 | Subgroup C and stenosis (C) | Metronidazole 7.5 mg/kg & spiramycin 45,000 U/kg q12h PO (Stomorgyl PA®), prednisolone 0.7 mg/kg/d PO (Microsolone®), hyperdigestible diet | Lost to follow-up | |
| 15 | Subgroup C and stenosis (C) | Prednisolone 0.75 mg/kg/d PO (Dermipred®), marbofloxacin 5 mg/kg PO (Marbocyl®), psyllium 2.5 g/cat PO (Fiberact®), hyperdigestible diet | Recent inclusion | |
| 17 | Subgroup C and stenosis (C) | Fiber enriched diet, metronidazole 9.6 mg/kg & spiramycin 58,000 U/kg q12h PO (Stomorgyl PA®), prednisolone 1 mg/kg/d PO (Dermipred®) | Recent inclusion | |
| 19 | Granulomatous colitis (D) | Marbofloxacin 4 mg/kg PO (Marbocyl®) | Improvement | |
| B | 5 | IBD (C) | Prednisolone 0.5 mg/kg PO (Dermipred®) and amoxicillin/clavulanic acid 14 mg/kg q12h (Clavaseptin®) PO | Lost to follow up |
| 8 | Granulomatous inflammation of unknown origin (C) | Prednisolonone 2 mg/kg/d PO (Dermipred®), diosmectite 1 g/kg q8h PO (Smecta®), TMPS 15 mg/kg q12h PO (Bactrim®) | Died within two weeks of hypovolemic shock | |
| 9 | LGITL in ileum (C) | Prednisolonone 2 mg/kg/d PO (Dermipred®), chlorambucil 20 mg/m2 every 2 weeks PO (Chloraminophene 2 mg®) | Marked improvement | |
| 12 | LP colitis (C) | Prednisolone 0.5 mg/kg PO (Microsolone®) and hyperdigestible diet | Marked improvement | |
| 14 | IBD with cholecystitis (C) | Marbofloxacin 5 mg/kg PO (Marbocyl®), amoxicillin/clavulanic acid 18 mg/kg q12h PO (Clavaspetin®), prednisolone 0.65 mg/kg/d PO (Microsolone®) after cholelithiasis removal. | Marked improvement | |
| 16 | IBD with stenotic areas (C) | Prednisolone 0.8 mg/kg PO (Dermipred®), marbofloxacin 3.1 mg/kg PO (Marbocyl®), psyllium 5g/cat PO (Fiberact ®), hyperdigestible diet | Recent inclusion | |
| 18 | IBD with stenotic areas (D) | Diosmectite 0.25 g/kg q12h PO (Smecta®), homemade eviction diet, probiotics PO (Fortiflora®), tylosine 20 mg/kg q12h PO (pharmaceutical compounding), prednisolone 0.5 mg/kg/d PO (Dermipred®). | Marked improvement. Colonic ADK diagnosed six months after | |
| 20 | Granulomatous colitis (D) | Enrofloxacin 7.4 mg/kg PO (Baytril®), fenebendazole 46 mg/kg PO (Panacur®), diosmectite 0.5 mg/kg q8h PO (Smecta®) | Died of septic shock after aspiration pneumonia | |
| 21 | Granulomatous colitis (D) | Marbofloxacin 4 mg/kg PO (Marbocyl®) | Marked improvement | |
| 22 | PLE (D) | Prednisolone 2 mg/kg/d PO (Dermipred®), cobalamine 55 µg/kg every other day PO (Cobalaplex®), ciclosporine 5 mg/kg/d PO (Atopica®), clopidogrel PO (Plavix®), metronidazole PO (Metrobactin®), ULF diet | Improvement with normal stools | |
| 23 | Granulomatous colitis (D) | Enrofloxacin 5 mg/kg PO (Baytril®), hyperdigestible diet, diosmectite 0.3 g/kg q8h PO (Smecta®) | Marked improvement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Remmel, P.; Gros, L.; Mortier, J.; Freiche, V. Congenital Partial Colonic Agenesis in Dogs and Cats: Clinical, Biological, Diagnostic Imaging, Endoscopic and Histopathologic Characterization, a Retrospective Study. Vet. Sci. 2023, 10, 577. https://doi.org/10.3390/vetsci10090577
Remmel P, Gros L, Mortier J, Freiche V. Congenital Partial Colonic Agenesis in Dogs and Cats: Clinical, Biological, Diagnostic Imaging, Endoscopic and Histopathologic Characterization, a Retrospective Study. Veterinary Sciences. 2023; 10(9):577. https://doi.org/10.3390/vetsci10090577
Chicago/Turabian StyleRemmel, Paul, Lucile Gros, Jérémy Mortier, and Valérie Freiche. 2023. "Congenital Partial Colonic Agenesis in Dogs and Cats: Clinical, Biological, Diagnostic Imaging, Endoscopic and Histopathologic Characterization, a Retrospective Study" Veterinary Sciences 10, no. 9: 577. https://doi.org/10.3390/vetsci10090577
APA StyleRemmel, P., Gros, L., Mortier, J., & Freiche, V. (2023). Congenital Partial Colonic Agenesis in Dogs and Cats: Clinical, Biological, Diagnostic Imaging, Endoscopic and Histopathologic Characterization, a Retrospective Study. Veterinary Sciences, 10(9), 577. https://doi.org/10.3390/vetsci10090577