Visualization of Myocardial Strain Pattern Uniqueness with Respect to Activation Time and Contractility: A Computational Study


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
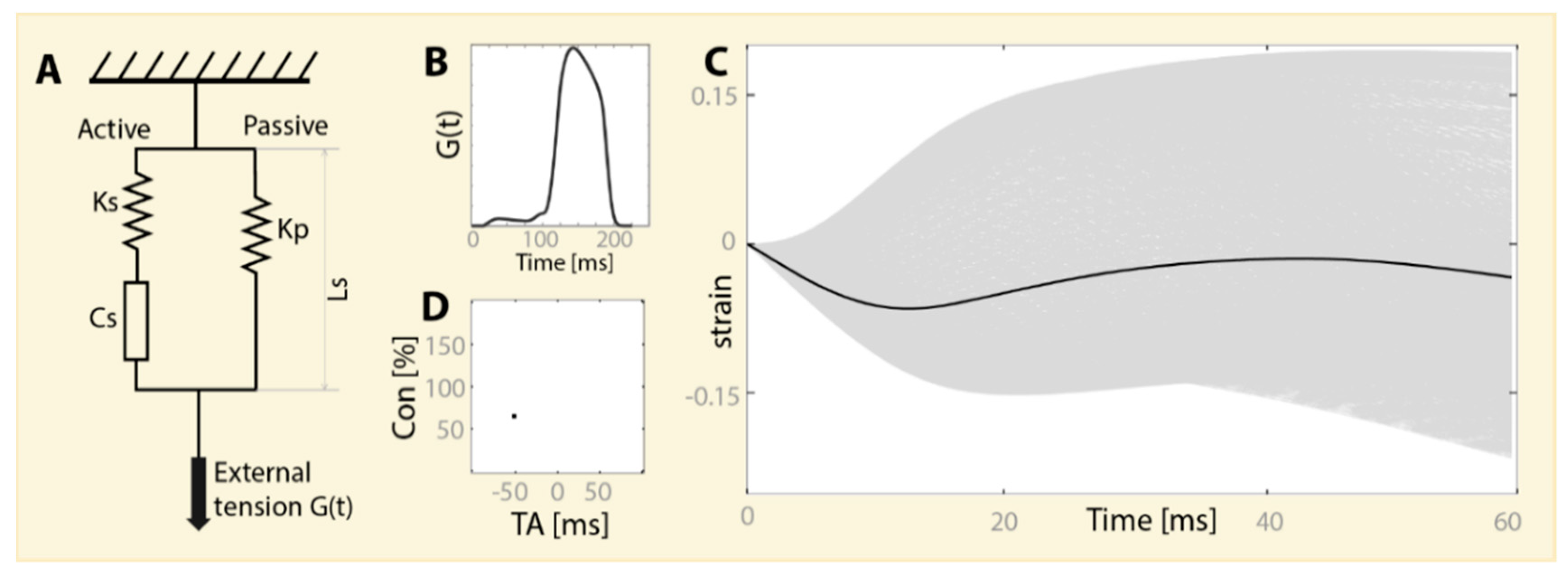
2.1. Parameter Space
2.2. Synthetic Measurement Space
2.3. Visualization of the Cohort in the Parameter Space
3. Results
- Each image is composed of one blob (connected component);
- Each blob has a distinctively different shape, size, and eccentricity.
4. Discussion
Funding
Conflicts of Interest
References
- Smiseth, O.A.; Torp, H.; Opdahl, A.; Haugaa, K.H.; Urheim, S. Myocardial strain imaging: how useful is it in clinical decision making? Eur. Heart J. 2016, 37, 1196–1207. [Google Scholar] [CrossRef] [PubMed]
- Collier, P.; Phelan, D.; Klein, A. A Test in Context: Myocardial strain measured by speckle-tracking echocardiography. J. Am. Coll. Cardiol. 2017, 69, 1043–1056. [Google Scholar] [CrossRef] [PubMed]
- Geyer, H.; Caracciolo, G.; Abe, H.; Wilansky, S.; Carerj, S.; Gentile, F.; Nesser, H.-J.; Khandheria, B.; Narula, J.; Sengupta, P.P. Assessment of myocardial mechanics using speckle tracking echocardiography: Fundamentals and clinical applications. J. Am. Soc. Echocardiogr. 2010, 23, 351–369. [Google Scholar] [CrossRef] [PubMed]
- Park, J.J.; Park, J.-B.; Park, J.-H.; Cho, G.-Y. Global longitudinal strain to predict mortality in patients with acute heart failure. J. Am. Coll. Cardiol. 2018, 71, 1947–1957. [Google Scholar] [CrossRef] [PubMed]
- Jasaityte, R.; Heyde, B.; D’hooge, J. Current state of three-dimensional myocardial strain estimation using echocardiography. J. Am. Soc. Echocardiogr 2013, 26, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Huang, X.; Ma, J.; Huang, J.; Fan, Y.; Li, H.; Qiu, J.; Zhang, H.; Huang, W. Value of three-dimensional strain parameters for predicting left ventricular remodeling after ST-elevation myocardial infarction. Int. J. Cardiovasc. Imag. 2017, 33, 663–673. [Google Scholar] [CrossRef]
- Krishnamurthy, A.; Villongco, C.T.; Chuang, J.; Frank, L.R.; Nigam, V.; Belezzuoli, E.; Stark, P.; Krummen, D.E.; Narayan, S.; Omens, J.H.; et al. Patient-specific models of cardiac biomechanics. J. Comput. Phys. 2013, 244, 4–21. [Google Scholar] [CrossRef]
- Bradley, C.; Bowery, A.; Britten, R.; Budelmann, V.; Camara, O.; Christie, R.; Cookson, A.; Frangi, A.F.; Gamage, T.B.; Heidlauf, T.; et al. OpenCMISS: A multi-physics & multi-scale computational infrastructure for the VPH/Physiome project. Progr. Biophys. Mol. Biol. 2011, 107, 32–47. [Google Scholar]
- Broomé, M.; Donker, D.W. Patient-Specific eal-time cardiovascular simulation as clinical decision support in intensive care medicine. In Annual Update in Intensive Care and Emergency Medicine 2017; Vincent, J.L., Ed.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 459–475. [Google Scholar]
- Chabiniok, R.; Moireau, P.; Lesault, P.-F.; Rahmouni, A.; Deux, J.-F.; Chapelle, D. Estimation of tissue contractility from cardiac cine-MRI using a biomechanical heart model. Biomech. Model. Mechanobiol. 2012, 11, 609–630. [Google Scholar] [CrossRef]
- Pironet, A.; Desaive, T.; Dauby, P.C.; Chase, J.G.; Docherty, P.D. Parameter identification methods in a model of the cardiovascular system. IFAC-PapersOnLine 2015, 48, 366–371. [Google Scholar] [CrossRef]
- Chabiniok, R.; Wang, V.Y.; Hadjicharalambous, M.; Asner, L.; Lee, J.; Sermesant, M.; Kuhl, E.; Young, A.A.; Moireau, P.; Nash, M.P.; et al. Multiphysics and multiscale modelling, data–model fusion and integration of organ physiology in the clinic: ventricular cardiac mechanics. Interface Focus 2016, 6, 20150083. [Google Scholar] [CrossRef] [PubMed]
- Sermesant, M.; Moireau, P.; Camara, O.; Sainte-Marie, J.; Andriantsimiavona, R.; Cimrman, R.; Hill, D.L.G.; Chapelle, D.; Razavi, R. Cardiac function estimation from MRI using a heart model and data assimilation: Advances and difficulties. Med. Image Anal. 2006, 10, 642–656. [Google Scholar] [CrossRef] [PubMed]
- Steinman, D.A.; Migliavacca, F. Editorial: Special issue on verification, validation, and uncertainty quantification of cardiovascular models: Towards effective VVUQ for translating cardiovascular modelling to clinical utility. Cardiovasc. Eng. Technol. 2018, 9, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Trayanova, N.A. Whole-heart modeling. Circ. Res. 2011, 108, 113–128. [Google Scholar] [CrossRef] [PubMed]
- Le Rolle, V.; Hernández, A.I.; Richard, P.-Y.; Donal, E.; Carrault, G. Model-based analysis of myocardial strain data acquired by tissue Doppler imaging. Artif. Intell. Med. 2008, 44, 201–219. [Google Scholar] [CrossRef]
- Dhamala, J.; Arevalo, H.J.; Sapp, J.; Horácek, B.M.; Wu, K.C.; Trayanova, N.A.; Wang, L. Quantifying the uncertainty in model parameters using Gaussian process-based Markov chain Monte Carlo in cardiac electrophysiology. Med. Image Anal. 2018, 48, 43–57. [Google Scholar] [CrossRef]
- Chapelle, D.; Fragu, M.; Mallet, V.; Moireau, P. Fundamental principles of data assimilation underlying the Verdandi library: applications to biophysical model personalization within euHeart. Med. Biol. Eng. Comput. 2013, 51, 1221–1233. [Google Scholar] [CrossRef]
- Eck, V.G.; Donders, W.P.; Sturdy, J.; Feinberg, J.; Delhaas, T.; Hellevik, L.R.; Huberts, W. A guide to uncertainty quantification and sensitivity analysis for cardiovascular applications. Int. J. Numer. Methods Biomed. Eng. 2016, 32, e02755. [Google Scholar] [CrossRef]
- Donekal, S.; Ambale-Venkatesh, B.; Berkowitz, S.; Wu, C.O.; Choi, E.Y.; Fernandes, V.; Yan, R.; Harouni, A.A.; Bluemke, D.A.; Lima, J.A.C. Inter-study reproducibility of cardiovascular magnetic resonance tagging. J. Cardiovasc. Magn. Resonance 2013, 15, 37. [Google Scholar] [CrossRef]
- Farsalinos, K.E.; Daraban, A.M.; Ünlü, S.; Thomas, J.D.; Badano, L.P.; Voigt, J.-U. Head-to-Head comparison of global longitudinal strain measurements among nine different vendors. J. Am. Soc. Echocardiogr. 2015, 28, 1171–1181. e2. [Google Scholar] [CrossRef]
- Zaniboni, M.; Riva, I.; Cacciani, F.; Groppi, M. How different two almost identical action potentials can be: A model study on cardiac repolarization. Math. Biosci. 2010, 228, 56–70. [Google Scholar] [CrossRef] [PubMed]
- Edelman, G.M.; Gally, J.A. Degeneracy and complexity in biological systems. Proc. Natl. Acad. Sci. USA 2001, 98, 13763–13768. [Google Scholar] [CrossRef] [PubMed]
- Gutenkunst, R.N.; Waterfall, J.J.; Casey, F.P.; Brown, K.S.; Myers, C.R.; Sethna, J.P. Universally sloppy parameter sensitivities in systems biology models. PLoS Comput. Biol. 2007, 3, e189. [Google Scholar] [CrossRef] [PubMed]
- Kirn, B.; Walmsley, J.; Lumens, J. Uniqueness of local myocardial strain patterns with respect to activation time and contractility of the failing heart: a computational study. BioMed. Eng. OnLine 2018, 17, 182. [Google Scholar] [CrossRef] [PubMed]
- Arts, T.; Delhaas, T.; Bovendeerd, P.; Verbeek, X.; Prinzen, F.W. Adaptation to mechanical load determines shape and properties of heart and circulation: the CircAdapt model. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, H1943–H1954. [Google Scholar] [CrossRef] [PubMed]
- Walmsley, J.; Arts, T.; Derval, N.; Bordachar, P.; Cochet, H.; Ploux, S.; Prinzen, F.W.; Delhaas, T.; Lumens, J. Fast Simulation of mechanical heterogeneity in the electrically asynchronous heart using the multiPatch module. PLoS Comput. Biol. 2015, 11, e1004284. [Google Scholar] [CrossRef] [PubMed]
- Eynard, D.; Kovnatsky, A.; Bronstein, M.M.; Glashoff, K.; Bronstein, A.M. Multimodal manifold analysis by simultaneous diagonalization of laplacians. IEEE Trans. Pattern Anal. Mach. Intell. 2015, 37, 2505–2517. [Google Scholar] [CrossRef] [PubMed]



© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kirn, B. Visualization of Myocardial Strain Pattern Uniqueness with Respect to Activation Time and Contractility: A Computational Study. Data 2019, 4, 79. https://doi.org/10.3390/data4020079
Kirn B. Visualization of Myocardial Strain Pattern Uniqueness with Respect to Activation Time and Contractility: A Computational Study. Data. 2019; 4(2):79. https://doi.org/10.3390/data4020079
Chicago/Turabian StyleKirn, Borut. 2019. "Visualization of Myocardial Strain Pattern Uniqueness with Respect to Activation Time and Contractility: A Computational Study" Data 4, no. 2: 79. https://doi.org/10.3390/data4020079
APA StyleKirn, B. (2019). Visualization of Myocardial Strain Pattern Uniqueness with Respect to Activation Time and Contractility: A Computational Study. Data, 4(2), 79. https://doi.org/10.3390/data4020079