
Influence of Sagittal Lumbopelvic Morphotypes on the Range of Motion of Human Lumbar Spine: An In Vitro Cadaveric Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimen Preparation
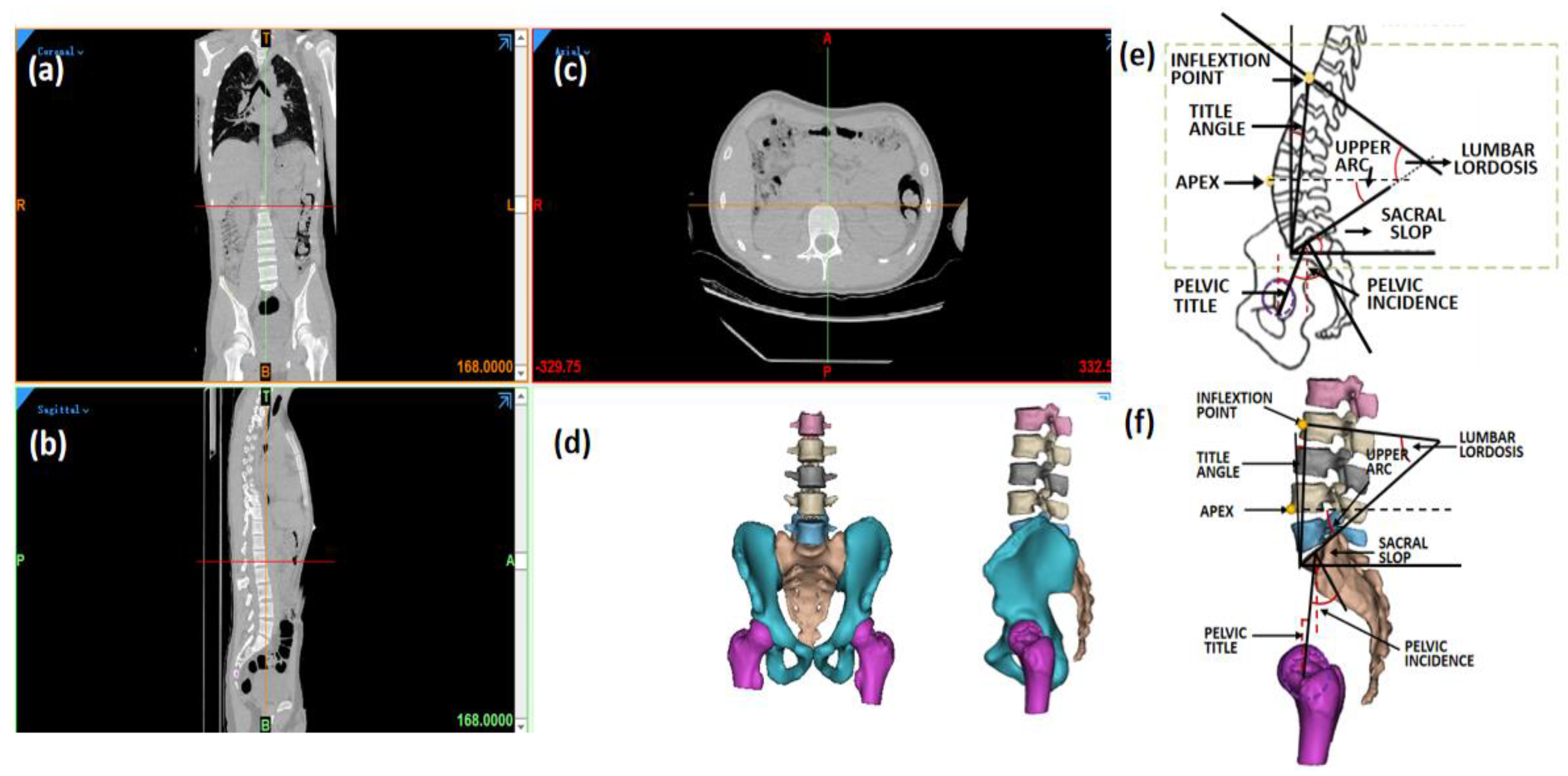
2.2. Sagittal Parameter Measurement
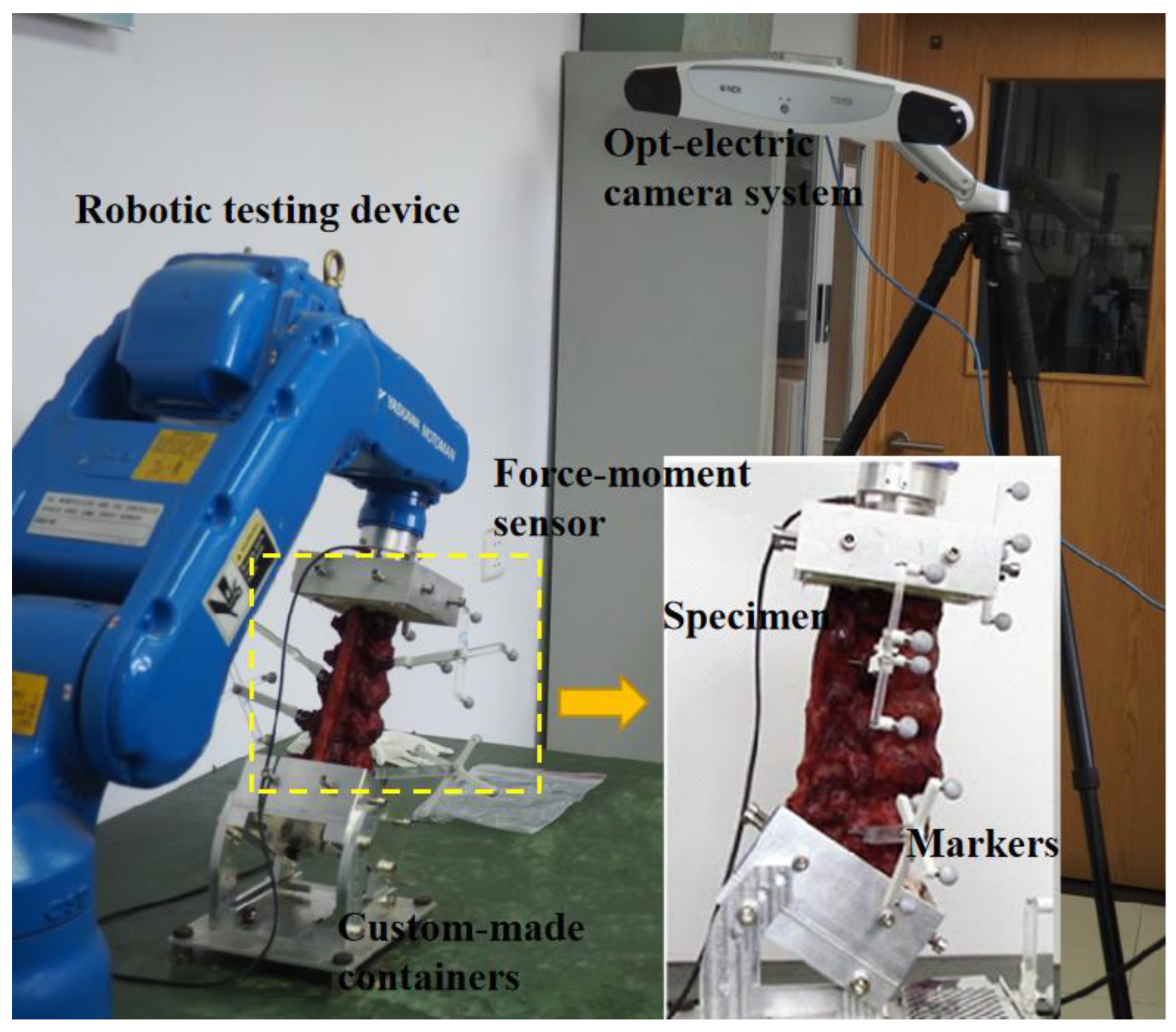
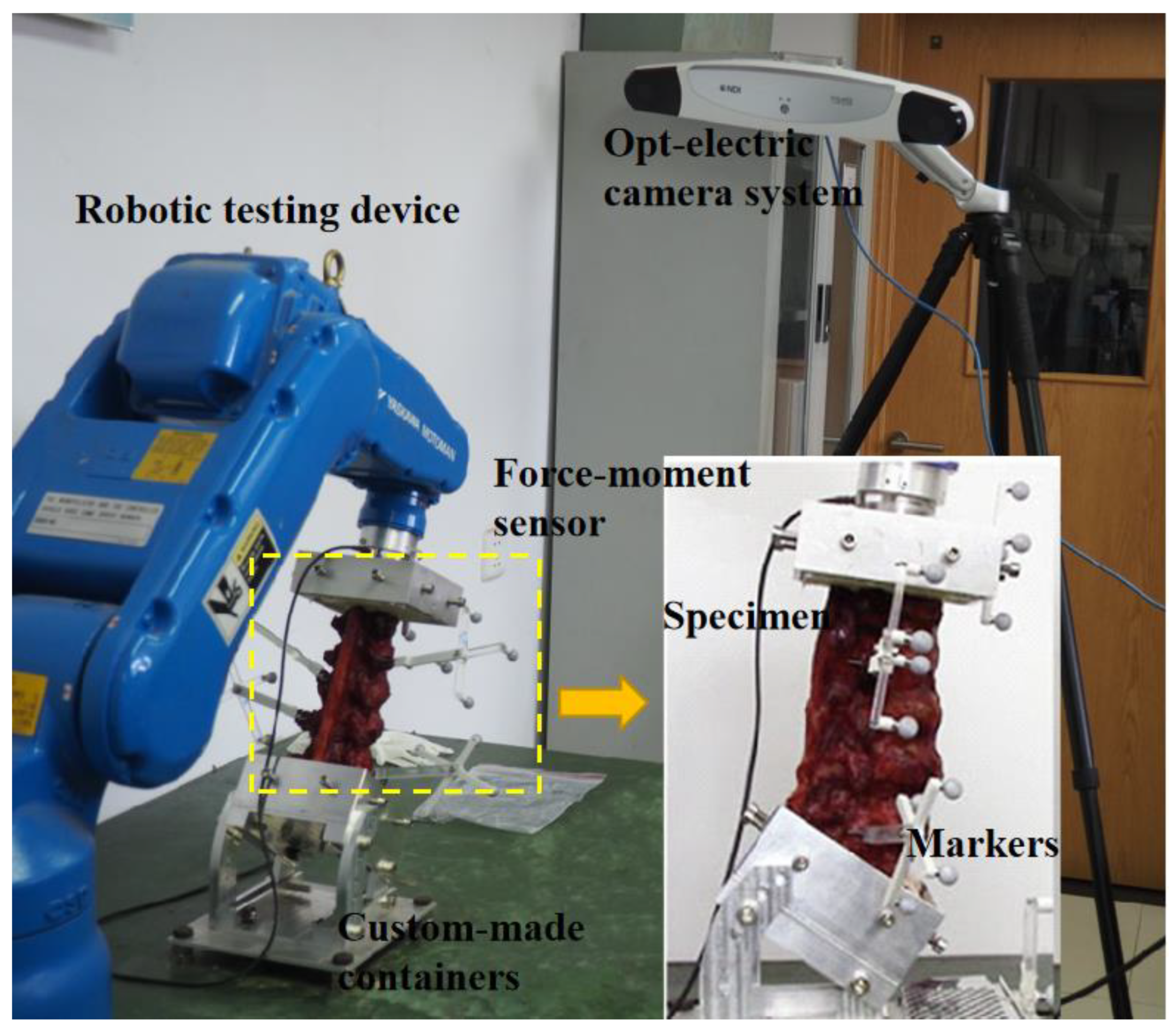
2.3. Testing Devices
2.4. Testing Protocol
2.5. Data Analysis
3. Results
3.1. Specimen Sagittal Parameters
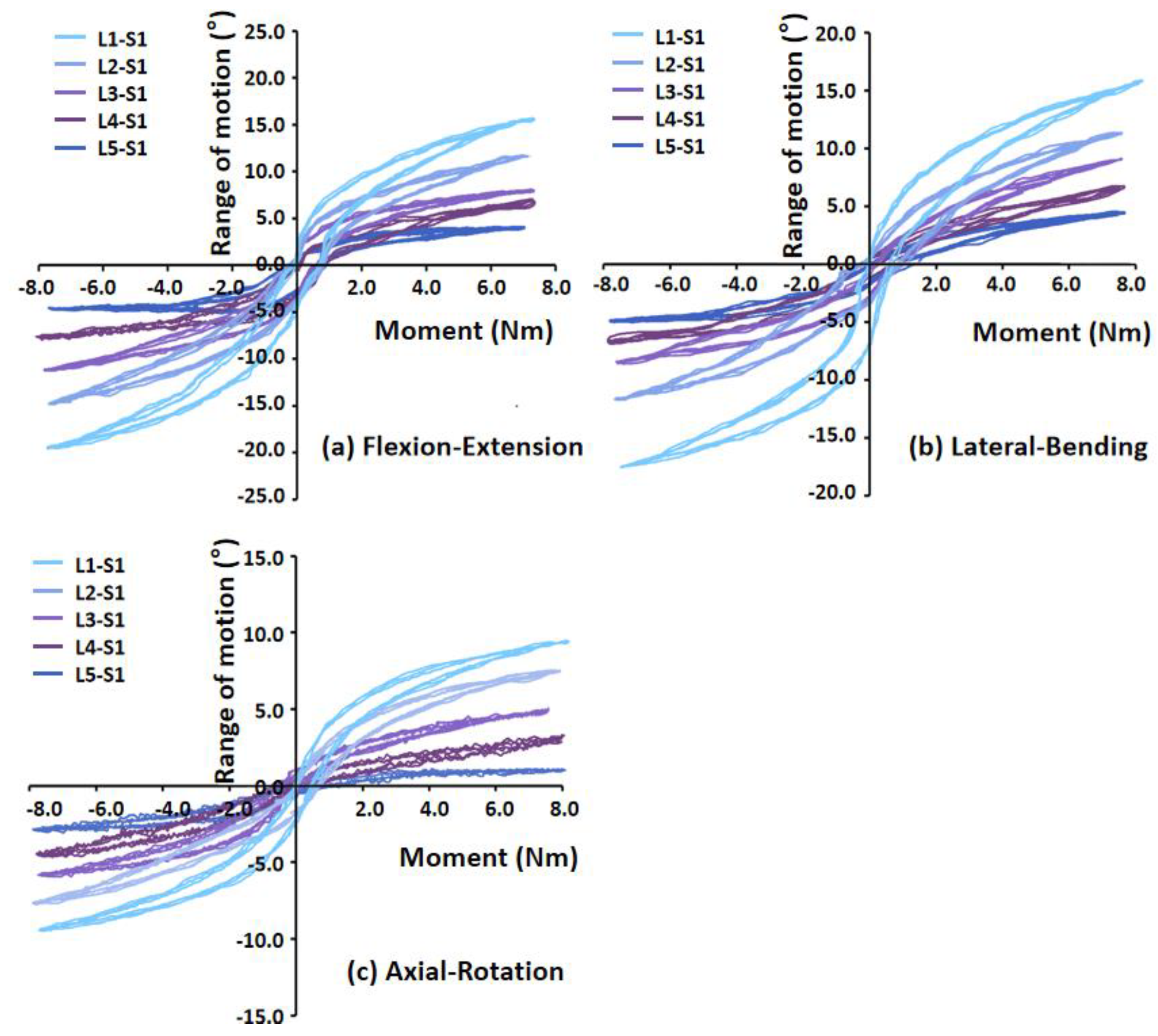
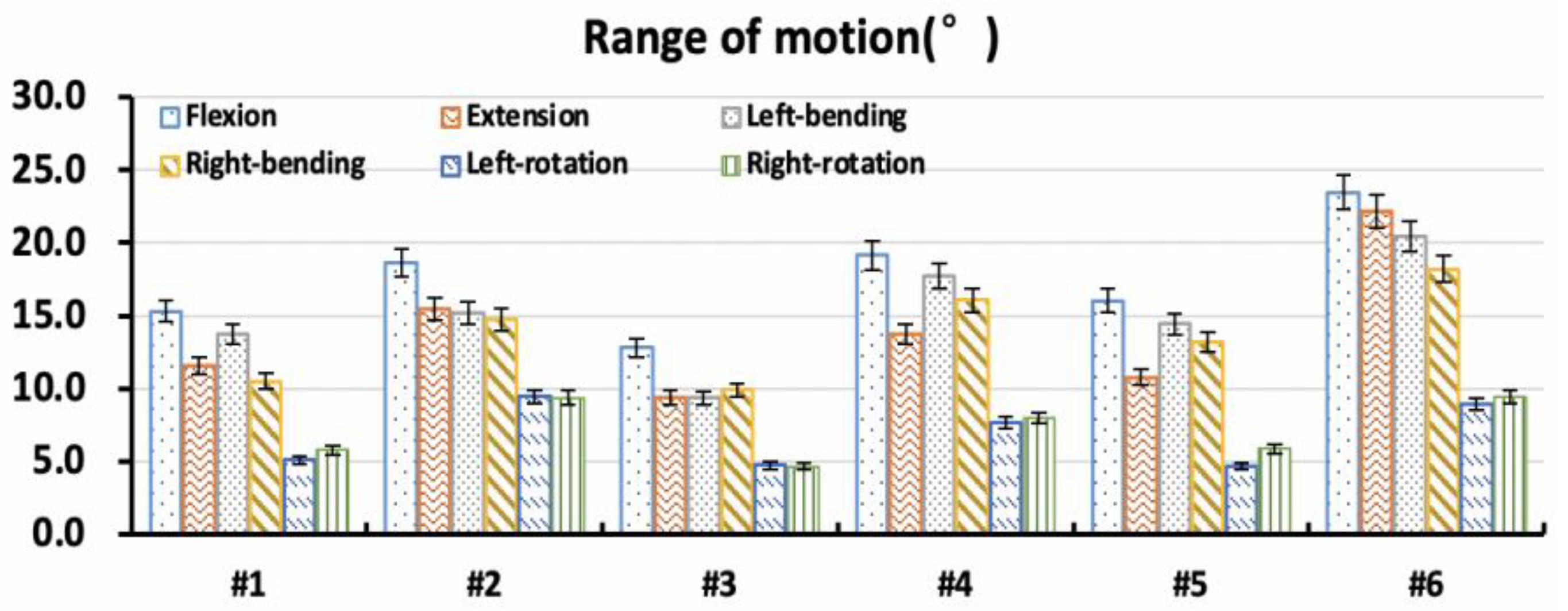
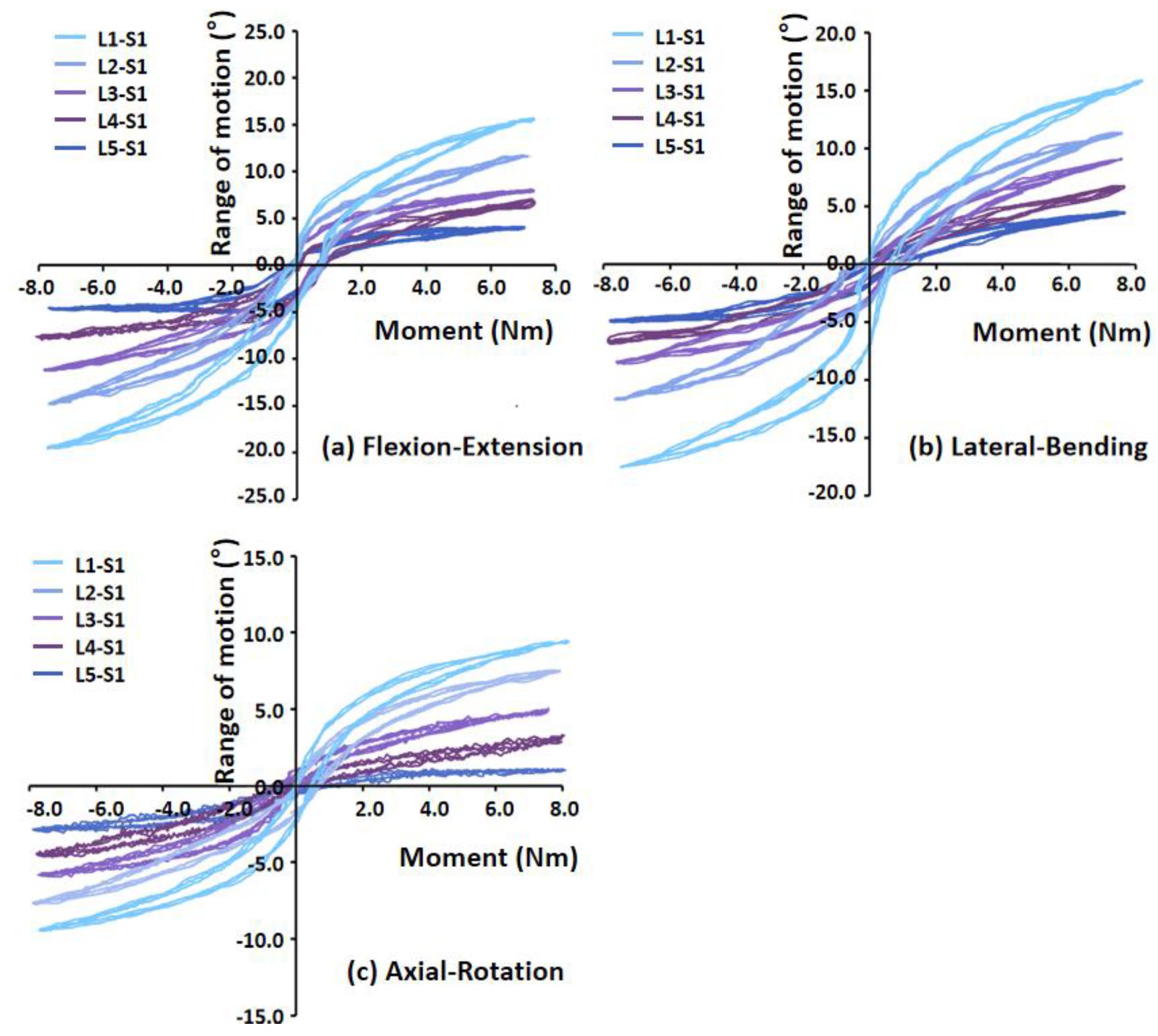
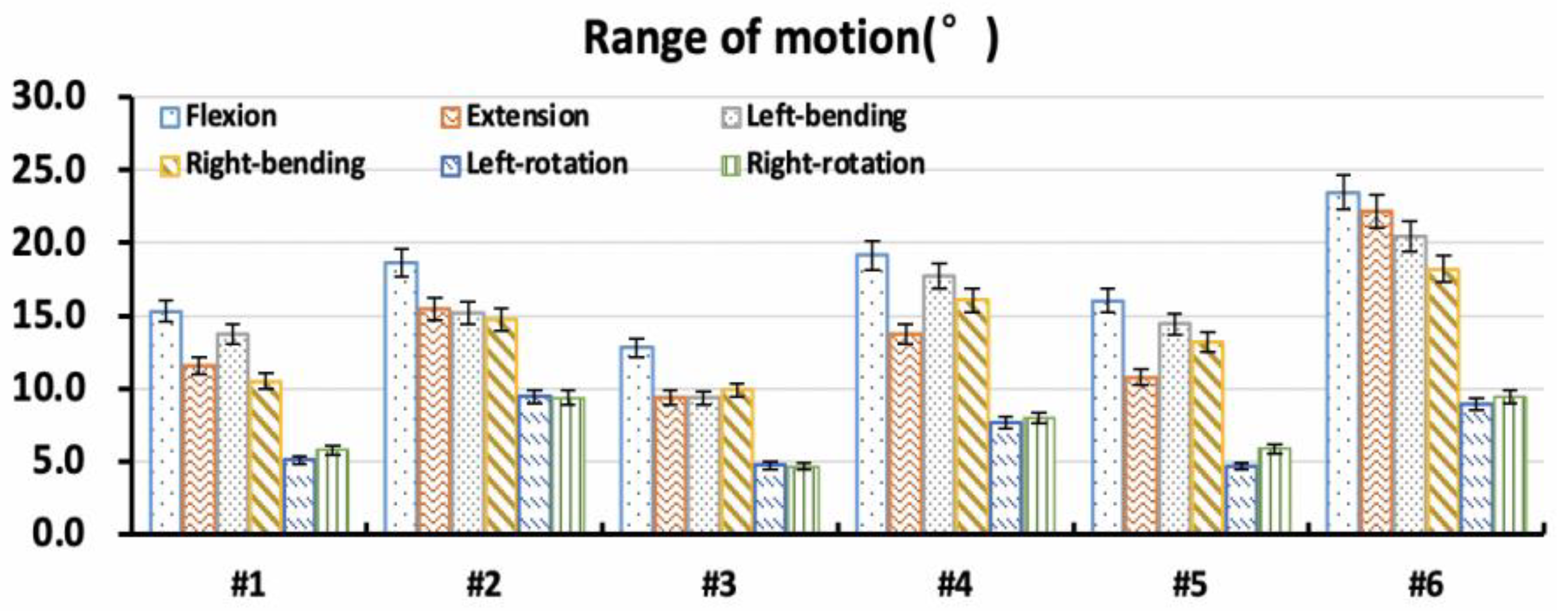
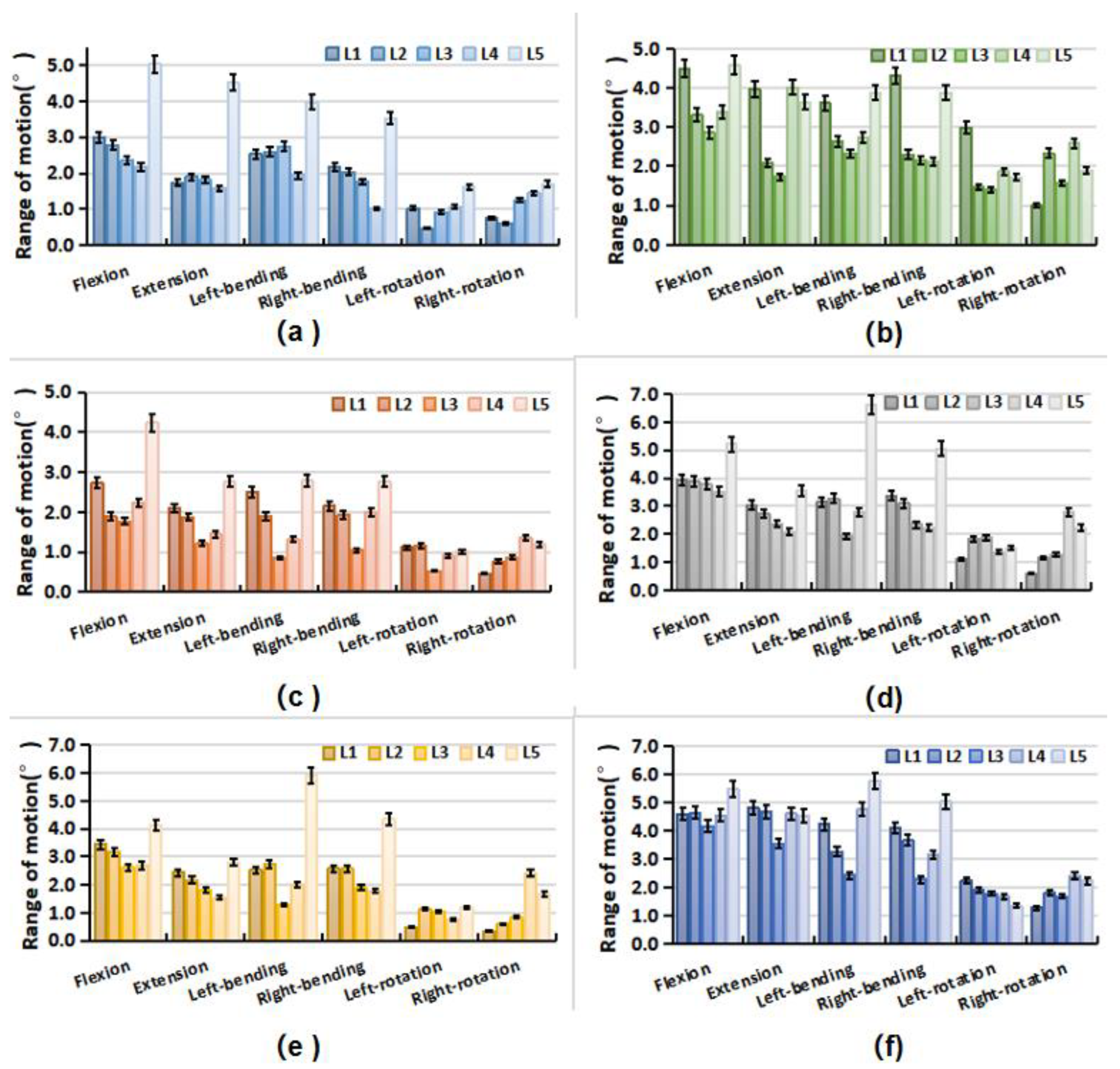
3.2. Intervertebral Rotations
3.3. Correlation Analysis
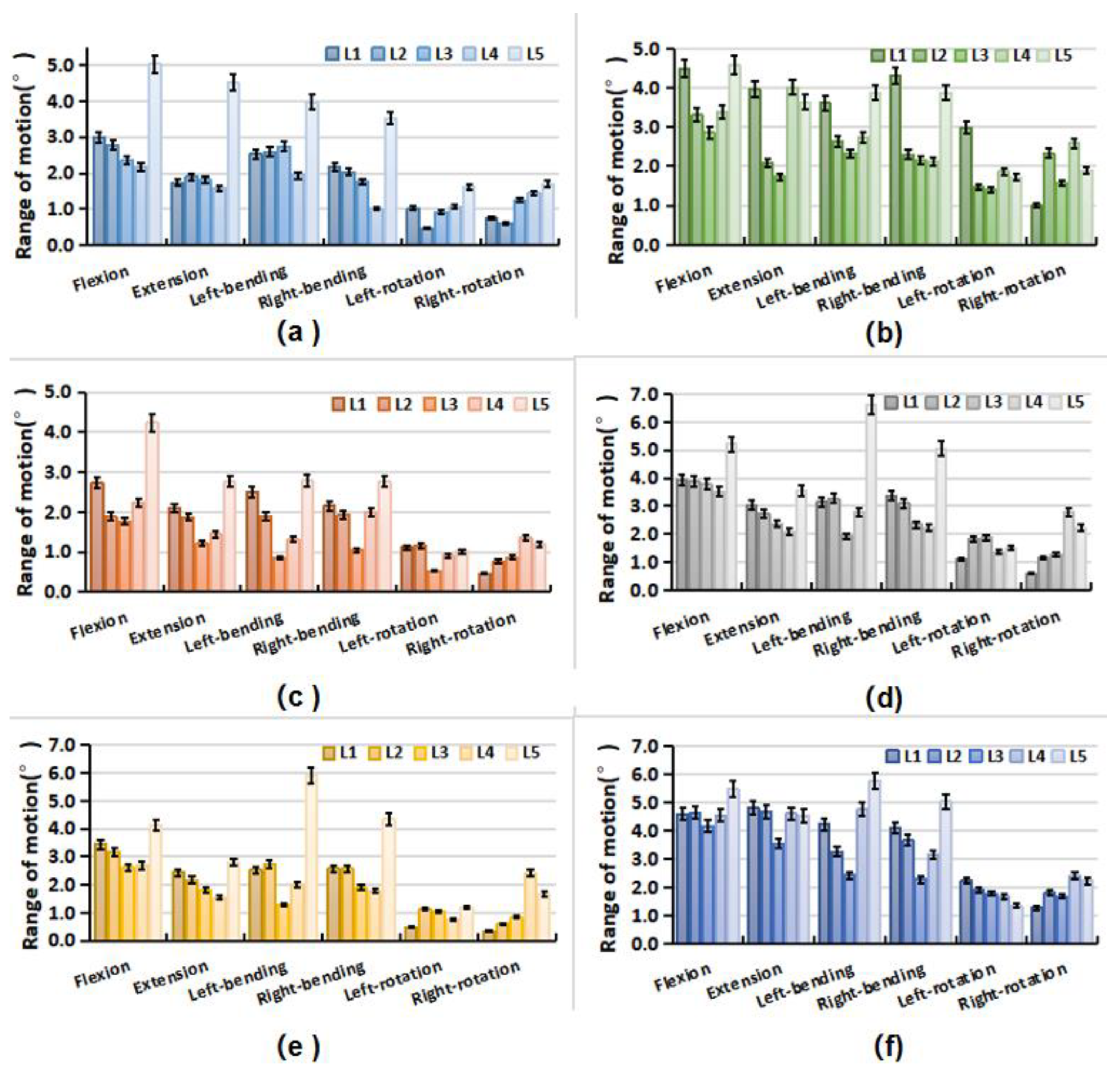
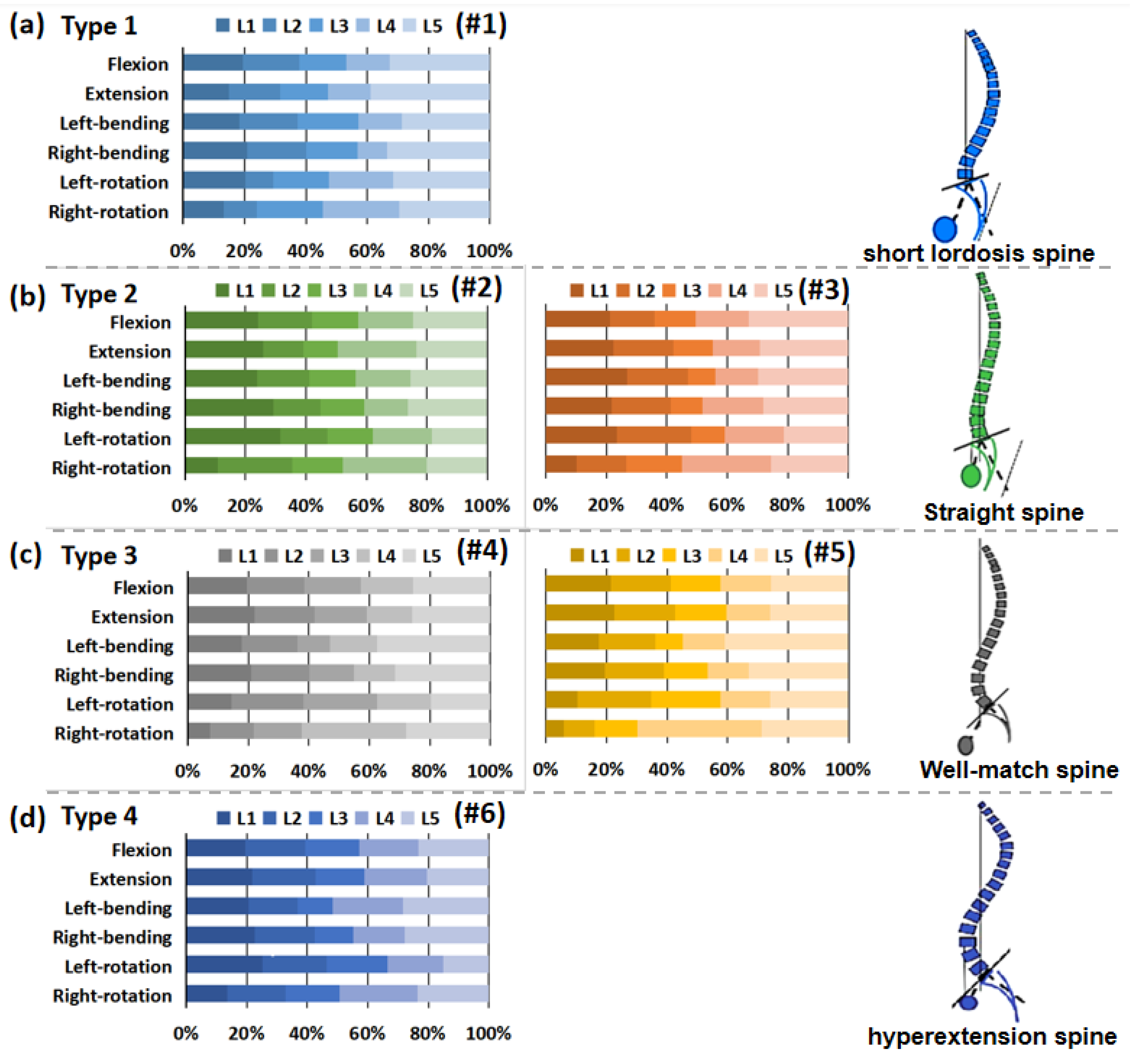
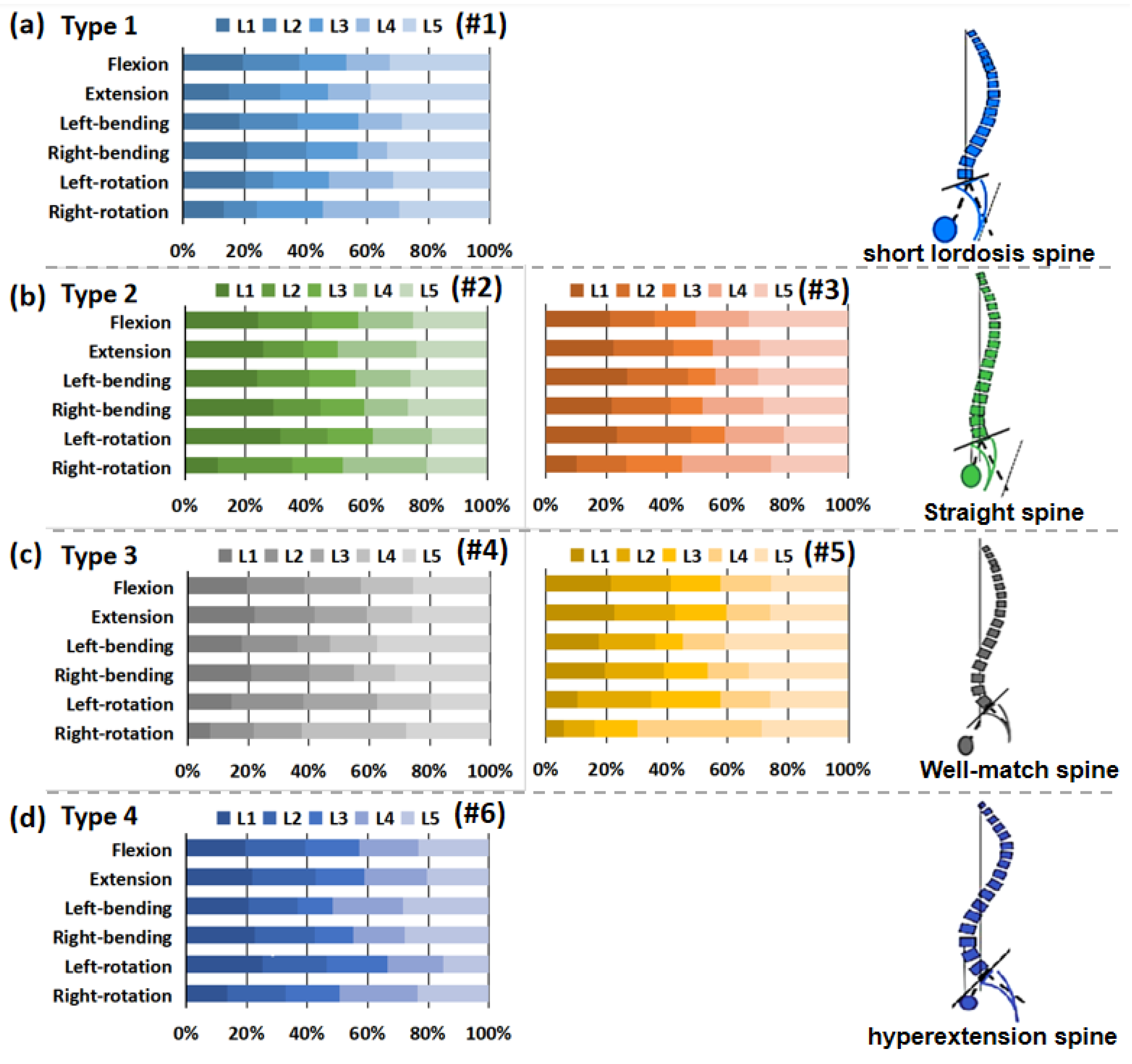
3.4. Intervertebral Rotation Distribution
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Skoyles, J.R. Human Balance, the Evolution of Bipedalism and Dysequilibrium Syndrome. Med. Hypotheses 2006, 66, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Bari, T.J.; Hansen, L.V.; Gehrchen, M. Surgical Correction of Adult Spinal Deformity in Accordance to the Roussouly Classification: Effect on Postoperative Mechanical Complications. Spine Deform. 2020, 8, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- Sebaaly, A.; Gehrchen, M.; Silvestre, C.; Kharrat, K.; Bari, T.J.; Kreichati, G.; Rizkallah, M.; Roussouly, P. Mechanical Complications in Adult Spinal Deformity and the Effect of Restoring the Spinal Shapes According to the Roussouly Classification: A Multicentric Study. Eur. Spine J. 2020, 29, 904–913. [Google Scholar] [CrossRef] [Green Version]
- Roussouly, P.; Gollogly, S.; Berthonnaud, E.; Dimnet, J. Classification of the Normal Variation in the Sagittal Alignment of the Human Lumbar Spine and Pelvis in the Standing Position. Spine 2005, 30, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Laouissat, F.; Sebaaly, A.; Gehrchen, M.; Roussouly, P. Classification of Normal Sagittal Spine Alignment: Refounding the Roussouly Classification. Eur. Spine J. 2018, 27, 2002–2011. [Google Scholar] [CrossRef] [PubMed]
- Sebaaly, A.; Riouallon, G.; Obeid, I.; Grobost, P.; Rizkallah, M.; Laouissat, F.; Charles, Y.P.; Roussouly, P. Proximal Junctional Kyphosis in Adult Scoliosis: Comparison of Four Radiological Predictor Models. Eur. Spine J. 2018, 27, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Hey, H.W.D.; Wong, G.C.; Chan, C.X.; Lau, L.L.; Kumar, N.; Thambiah, J.S.; Ruiz, J.N.; Liu, K.P.G.; Wong, H.K. Reproducibility of Sagittal Radiographic Parameters in Adolescent Idiopathic Scoliosis—A Guide to Reference Values Using Serial Imaging. Spine J. 2017, 17, 830–836. [Google Scholar] [CrossRef]
- Ferrero, E.; Vira, S.; Ames, C.P.; Kebaish, K.; Obeid, I.; O’Brien, M.F.; Gupta, M.C.; Boachie-Adjei, O.; Smith, J.S.; Mundis, G.M.; et al. Analysis of an Unexplored Group of Sagittal Deformity Patients: Low Pelvic Tilt despite Positive Sagittal Malalignment. Eur. Spine J. 2016, 25, 3568–3576. [Google Scholar] [CrossRef]
- Labelle, H.; Mac-Thiong, J.M.; Roussouly, P. Spino-Pelvic Sagittal Balance of Spondylolisthesis: A Review and Classification. Eur. Spine J. 2011, 20 (Suppl. S5), 641–646. [Google Scholar] [CrossRef] [Green Version]
- Galbusera, F.; Brayda-Bruno, M.; Costa, F.; Wilke, H.J. Numerical Evaluation of the Correlation between the Normal Variation in the Sagittal Alignment of the Lumbar Spine and the Spinal Loads. J. Orthop. Res. 2014, 32, 537–544. [Google Scholar] [CrossRef]
- Roussouly, P.; Pinheiro-Franco, J.L. Biomechanical Analysis of the Spino-Pelvic Organization and Adaptation in Pathology. Eur. Spine J. 2011, 20 (Suppl. S5), 609–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Huec, J.C.; Faundez, A.; Dominguez, D.; Hoffmeyer, P.; Aunoble, S. Evidence Showing the Relationship between Sagittal Balance and Clinical Outcomes in Surgical Treatment of Degenerative Spinal Diseases: A Literature Review. Int. Orthop. 2015, 39, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Wilke, H.-J.; Wenger, K.; Claes, L. Testing Criteria for Spinal Implants. Euro Spine J. 1998, 7, 148–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, C.; Lu, S.; Hai, Y.; Zang, L. Biomechanical Effect of Interspinous Dynamic Stabilization Adjacent to Single-Level Fusion on Range of Motion of the Transition Segment and the Adjacent Segment. Clin. Biomech. 2015, 30, 355–359. [Google Scholar] [CrossRef]
- Duval-Beaupère, G.; Schmidt, C.; Cosson, P. A Barycentremetric Study of the Sagittal Shape of Spine and Pelvis: The Conditions Required for an Economic Standing Position. Ann. Biomed. Eng. 1992, 20, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Panjabi, M.M.; Goel, V.; Oxland, T.; Takata, K.; Duranceau, J.; Krag, M.; Price, M. Human Lumbar Vertebrae: Quantitative Three-Dimensional Anatomy. Spine 1992, 17, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Cha, T.; Wang, W.; Guo, R.; Li, G. Investigation of Alterations in the Lumbar Disc Biomechanics at the Adjacent Segments After Spinal Fusion Using a Combined In Vivo and In Silico Approach. Ann. Biomed. Eng. 2020, 49, 601–616. [Google Scholar] [CrossRef]
- Wang, W.; Pei, B.; Pei, Y.; Shi, Z.; Kong, C.; Wu, X.; Wu, N.; Fan, Y.; Lu, S. Biomechanical Effects of Posterior Pedicle Fixation Techniques on the Adjacent Segment for the Treatment of Thoracolumbar Burst Fractures: A Biomechanical Analysis. Comput. Methods Biomech. Biomed. Engin. 2019, 22, 1083–1092. [Google Scholar] [CrossRef]
- Rohlmann, A.; Zander, T.; Schmidt, H.; Wilke, H.J.; Bergmann, G. Analysis of the Influence of Disc Degeneration on the Mechanical Behaviour of a Lumbar Motion Segment Using the Finite Element Method. J. Biomech. 2006, 39, 2484–2490. [Google Scholar] [CrossRef]
- Renner, S.M.; Natarajan, R.N.; Patwardhan, A.G.; Havey, R.M.; Voronov, L.I.; Guo, B.Y.; Andersson, G.B.J.; An, H.S. Novel Model to Analyze the Effect of a Large Compressive Follower Pre-Load on Range of Motions in a Lumbar Spine. J. Biomech. 2007, 40, 1326–1332. [Google Scholar] [CrossRef]
- Roussouly, P.; Nnadi, C. Sagittal Plane Deformity: An Overview of Interpretation and Management. Eur. Spine J. 2010, 19, 1824–1836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endo, K.; Suzuki, H.; Nishimura, H.; Tanaka, H.; Shishido, T.; Yamamoto, K. Characteristics of Sagittal Spino-Pelvic Alignment in Japanese Young Adults. Asian Spine J. 2014, 8, 599–604. [Google Scholar] [CrossRef] [Green Version]
- Gay, R.E.; Ilharreborde, B.; Zhao, K.; Zhao, C.; An, K.-N. Sagittal Plane Motion in the Human Lumbar Spine: Comparison of the in Vitro Quasistatic Neutral Zone and Dynamic Motion Parameters. Clin. Biomech. 2006, 21, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.A.; Roughley, P.J. What Is Intervertebral Disc Degeneration, and What Causes It? Spine 2006, 31, 2151–2161. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | 1 | 2 | 3 | 4 | 5 | 6 | Mean ± SD |
|---|---|---|---|---|---|---|---|
| Sex | Female | Male | Male | Female | Male | Female | -- |
| PI | 36.9 | 39.6 | 44.2 | 47.5 | 54.1 | 59.0 | 46.88 ± 7.74 |
| PT | 9.4 | 10.2 | 11.4 | 10.1 | 10.7 | 12.2 | 10.67 ± 0.92 |
| SS | 27.5 | 29.4 | 32.8 | 37.4 | 43.4 | 46.8 | 36.22 ± 7.06 |
| LL | 40.3 | 43.2 | 48.2 | 52.4 | 53.9 | 58.2 | 49.37 ± 6.18 |
| Apex | Upper L5 | Base L4 | Base L4 | Middle L4 | Middle L4 | Base L3 | -- |
| Upper arc | 14.0 | 13.9 | 15.4 | 14.8 | 14.7 | 16.6 | 14.90 ± 0.91 |
| LTA | −5.2 | −4.4 | −4.2 | −5.7 | −5.9 | −3.07 | −4.75 ± 0.97 |
| NVL | 4.3 | 4.6 | 4.9 | 5.0 | 4.8 | 5.0 | 4.77 ± 0.25 |
| Type | Type 1 | Type 2 | Type 2 | Type 3 | Type 3 | Type 4 | -- |
| Type | PI (°) | SS (°) | PT (°) | LL (°) | Apex | Upper Arc (°) | LTA (°) | NVL | |
|---|---|---|---|---|---|---|---|---|---|
| Flexion | 0.28 | 0.36 * | 0.63 * 7 | −0.15 | 0.51 * 4 | 0.33 * | 0.42 * | −0.14 | −0.06 |
| Extension | 0.19 | 0.34 * | 0.53 * | −0.04 | 0.67 * | 0.36 * | 0.41 * | 0.17 | 0.15 |
| Left-bending | 0.10 | −0.171 | 0.32* | −0.29 | −0.20 | 0.16 | 0.24 | −0.20 | −0.26 |
| Right-bending | 0.24 | 0.14 | 0.35* | 0.15 | −0.27 | 0.24 | 0.20 | 0.30 * | 0.27 |
| Left-rotation | 0.13 | −0.06 | 0.36* | −0.08 | −0.20 | 0.21 | −0.07 | 0.24 | 0.21 |
| Right-rotation | −0.04 | 0.19 | 0.28* | 0.12 | −0.07 | 0.13 | −0.06 | 0.13 | −0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Kong, C.; Pan, F.; Wang, W.; Wu, X.; Pei, B.; Lu, S. Influence of Sagittal Lumbopelvic Morphotypes on the Range of Motion of Human Lumbar Spine: An In Vitro Cadaveric Study. Bioengineering 2022, 9, 224. https://doi.org/10.3390/bioengineering9050224
Wang W, Kong C, Pan F, Wang W, Wu X, Pei B, Lu S. Influence of Sagittal Lumbopelvic Morphotypes on the Range of Motion of Human Lumbar Spine: An In Vitro Cadaveric Study. Bioengineering. 2022; 9(5):224. https://doi.org/10.3390/bioengineering9050224
Chicago/Turabian StyleWang, Wei, Chao Kong, Fumin Pan, Wei Wang, Xueqing Wu, Baoqing Pei, and Shibao Lu. 2022. "Influence of Sagittal Lumbopelvic Morphotypes on the Range of Motion of Human Lumbar Spine: An In Vitro Cadaveric Study" Bioengineering 9, no. 5: 224. https://doi.org/10.3390/bioengineering9050224
APA StyleWang, W., Kong, C., Pan, F., Wang, W., Wu, X., Pei, B., & Lu, S. (2022). Influence of Sagittal Lumbopelvic Morphotypes on the Range of Motion of Human Lumbar Spine: An In Vitro Cadaveric Study. Bioengineering, 9(5), 224. https://doi.org/10.3390/bioengineering9050224