
Lumbar Intervertebral Disc Herniation: Annular Closure Devices and Key Design Requirements

 ,
,  and
and 
Abstract
1. Introduction
1.1. Background
1.2. The Importance of Annular Closure
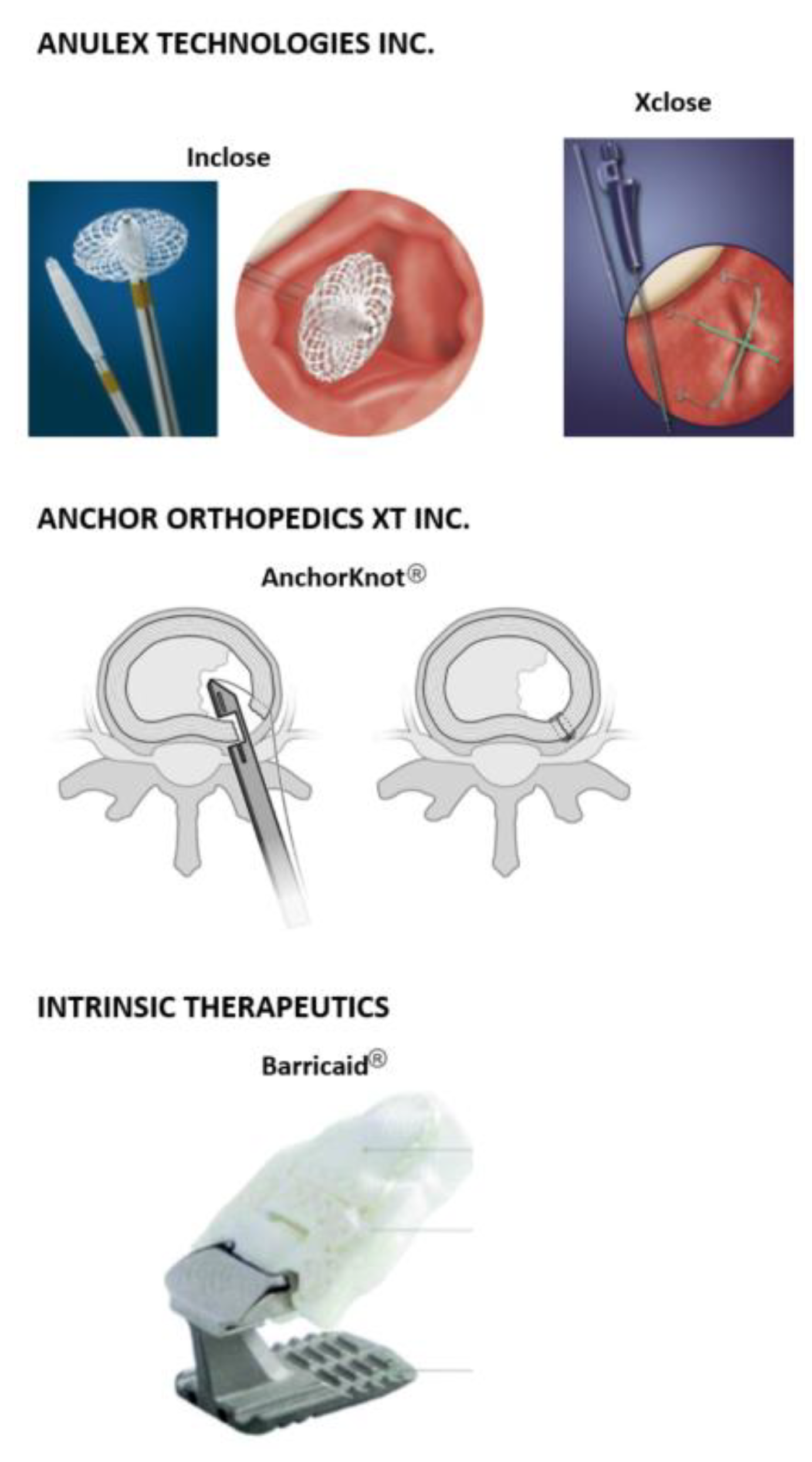
1.3. Commercial Annular Closure Devices
1.3.1. Inclose and Xclose Systems
1.3.2. AnchorKnot® Tissue Approximation Kit
1.3.3. Barricaid® Annular Closure Device
2. Design Requirements for an Annular Closure Device
2.1. Previous Efforts at Developing an Annular Repair/Regeneration Strategy
2.2. Aims and Scope
2.3. Key Requirements for an Annular Repair Strategy
2.3.1. Mechanical Requirements
2.3.2. Biological Requirements
2.3.3. Material Requirements
2.4. Preclinical Testing
2.5. Considerations for Clinical Translation
2.5.1. Sterilization
2.5.2. Delivery and Attachment
2.5.3. Postoperative Imaging
- “MRI Safe—an item that poses no known hazards resulting from exposure to any MR environment. MR Safe items are composed of materials that are electrically nonconductive, non-metallic, and nonmagnetic.
- MR Conditional—an item with demonstrated safety in the MR environment within defined conditions.
- MR Unsafe—an item which poses unacceptable risks to the patient, medical staff, or other persons within the MR environment.”
2.5.4. Same Level Symptomatic Reherniation
2.5.5. Device Loosening, Failure, and Safe Removal
2.5.6. Pain Score Improvement
2.6. Current Testing Standards
3. Conclusions and Recommendations
Author Contributions
Funding
Conflicts of Interest
Appendix A. Design Specification for an Annular Repair Strategy
- Range of motion must be restored in all six degrees of freedom (flexion–extension, lateral bending, and axial rotation) within an acceptable range. In vivo flexion (6°–13°), extension (1°–5°), lateral bending (2.9°–11°), and axial rotation (2°–3°) must be maintained within acceptable ranges.
- Withstands in vivo intradiscal pressure during daily life activities (see Table 2 for reference values).
- Allows nutrient supply to rest of tissue to continue—minimizes disruption of the blood supply in the outer annulus, and does not cause significant damage or lesions to the endplates that will compromise nutrient supply [78].
- Maintains pH range within 6.4 and 7.4.
- Reduces inflammatory cytokine excretion.
- Prevents tissue innervation.
- Minimizes endplate lesions—preservation of the endplates is crucial, particularly the caudal (bottom) endplate.
- Temperature range of 37 ± 2 °C (physiological temperature)Life in service (see 2.6 Current testing standards).
- 10 years (1 × 107 loading cycles).
- Barricaid® (Intrinsic Therapeutics, Woburn, MA, USA).
- AnchorKnot® Tissue Approximation Kit (Anchor Orthopedics XT Inc., Mississauga, ON, USA)
- Fills an annular defect size after discectomy likely to be within 8–10 × 6 mm (width × height) (based on Barricaid® size range).
- Biocompatible.
- Non-cytotoxic.
- Must have similar mechanical properties to native AF.
- Must be resistant to degradation.
- BS EN ISO 10993 Biological evaluation of medical devices, Parts 1–20.
- ASTM F981-04(2016) Standard Practice for Assessment of Compatibility of Biomaterials for Surgical Implants with Respect to Effect of Materials on Muscle and Insertion into Bone.
- ASTM F1983-14 Standard Practice for Assessment of Selected Tissue Effects of Absorbable Biomaterials for Implant Applications.
- BS ISO 18192-2:2010 Implants for surgery. Wear of total intervertebral spinal disc prostheses. Nucleus replacements.
- BS ISO 18192-3:2017 Implants for surgery. Wear of total intervertebral spinal disc prostheses. Impingement-wear testing and corresponding environmental conditions for test of lumbar prostheses under adverse kinematic conditions.
- BS ISO 18192-1:2011+A1:2018 Implants for surgery. Wear of total intervertebral spinal disc prostheses. Loading and displacement parameters for wear testing and corresponding environmental conditions for test.
- ASTM F1717-18 Standard Test Methods for Spinal Implant Constructs in a Vertebrectomy Model.
- ASTM F2789-10(2015) Standard Guide for Mechanical and Functional Characterization of Nucleus Devices.
- ASTM F2346-18 Standard Test Methods for Static and Dynamic Characterization of Spinal Artificial Discs.
- ASTM F2423-11(2016) Standard Guide for Functional, Kinematic, and Wear Assessment of Total Disc Prostheses.
- ASTM F3295-18 Standard Guide for Impingement Testing of Total Disc Prostheses.
- ASTM F732-17 Standard Test Method for Wear Testing of Polymeric Materials Used in Total Joint Prostheses.
- ASTM F2900-11 Standard Guide for Characterization of Hydrogels used in Regenerative Medicine.
- ASTM F3142-16 Standard Guide for Evaluation of in vitro Release of Biomolecules from Biomaterials Scaffolds for TEMPs.
- ASTM F2150-19 Standard Guide for Characterization and Testing of Biomaterial Scaffolds Used in Regenerative Medicine and Tissue-Engineered Medical Products.
- ASTM F2052-15 Standard Test Method for Measurement of Magnetically Induced Displacement Force on Medical Devices in the Magnetic Resonance Environment.
- ASTM F3224-17 Standard Test Method for Evaluating Growth of Engineered Cartilage Tissue using Magnetic Resonance Imaging.
- The device must be safely delivered or implanted during a microdiscectomy or minimally invasive procedure.
- The device must be safely attached to the tissue and must remain in place.
- The device shall not fail if patient requirements are met, the device is properly implanted, and the patient follows postoperative care.
- The device should allow for safe removal at any time.
- The device must maintain adequate mechanical properties after sterilization.
- The device is MRI safe or MRI conditional.
- A VAS pain score decrease of at least 20mm in a 100mm scale and/or ODI score decrease of at least 15 points is considered a success.
References
- GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar] [CrossRef]
- Urban, J. Disc biochemistry in relation to function. In The Lumbar Spine; Wiesel, S.W., Weinstein, J.N., Herkowitz, H.N., Dvorak, J., Bell, G., Eds.; Saunders: Philadelphia, PA, USA, 1996; pp. 271–280. [Google Scholar]
- Humzah, M.D.; Soames, R.W. Human intervertebral disc: Structure and function. Anat. Rec. 1988, 220, 337–356. [Google Scholar] [CrossRef]
- Cassidy, J.J.; Hiltner, A.; Baer, E. Hierarchical structure of the intervertebral disc. Connect. Tissue Res. 1989, 23, 75–88. [Google Scholar] [CrossRef]
- Marchand, F.; Ahmed, A.M. Investigation of the laminate structure of lumbar disc anulus fibrosus. Spine 1990, 15, 402–410. [Google Scholar] [CrossRef]
- Smith, L.J.; Nerurkar, N.L.; Choi, K.S.; Harfe, B.D.; Elliott, D.M. Degeneration and regeneration of the intervertebral disc: Lessons from development. Dis. Models Mech. 2011, 4, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, C.W.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic Resonance Classification of Lumbar Intervertebral Disc Degeneration. Spine 2001, 26, 1873–1878. [Google Scholar] [CrossRef]
- Griffith, J.F.; Wang, Y.-X.; Antonio, G.E.; Choi, K.C.; Yu, A.; Ahuja, A.T.; Leung, P.C. Modified Pfirrmann Grading System for Lumbar Intervertebral Disc Degeneration. Spine 2007, 32, E708–E712. [Google Scholar] [CrossRef]
- Amin, R.M.; Andrade, N.S.; Neuman, B.J. Lumbar Disc Herniation. Curr. Rev. Musculoskelet. Med. 2017, 10, 507–516. [Google Scholar] [CrossRef]
- Suthar, P.; Patel, R.; Mehta, C.; Patel, N. MRI evaluation of lumbar disc degenerative disease. J. Clin. Diagn. Res. 2015, 9, TC04-9. [Google Scholar] [CrossRef]
- Fardon, D.F.; Williams, A.L.; Dohring, E.J.; Murtagh, F.R.; Rothman, S.L.G.; Sze, G.K. Lumbar disc nomenclature: Version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Spine J. 2014, 14, 2525–2545. [Google Scholar] [CrossRef]
- Jordan, J.; Konstantinou, K.; O’dowd, J. Herniated lumbar disc. BMJ Clin. Evid. 2009, 2009, 1118. [Google Scholar] [PubMed]
- Omidi-Kashani, F.; Hejrati, H.; Ariamanesh, S. Ten important tips in treating a patient with lumbar disc herniation. Asian Spine J. 2016, 10, 955–963. [Google Scholar] [CrossRef] [PubMed][Green Version]
- National Guideline Centre (UK). Low Back Pain and Sciatica in Over 16s: Assessment and Management. National Institute for Health and Care Excellence (NICE), November 2016. Available online: https://www.nice.org.uk/guidance/ng59 (accessed on 22 November 2021).
- Lee, C.K.; Goel, V.K. Artificial disc prosthesis: Design concepts and criteria. Spine J. 2004, 4, S209–S218. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.G.; Helgeson, M.D.; Vaccaro, A.R. Spinal Motion Restoration Devices for the Degenerative Disc. In The Intervertebral Disc; Springer: Vienna, Austria, 2014; pp. 225–246. [Google Scholar]
- Satoh, I.; Yonenobu, K.; Hosono, N.; Ohwada, T.; Fuji, T.; Yoshikawa, H. Indication of posterior lumbar interbody fusion for lumbar disc herniation. J. Spinal Disord. Technol. 2006, 19, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Randolph, G.B.; Scioscia, T.N.; Wang, J.C. Lumbar Total Disc Arthroplasty: State of the Data. Semin. Spine Surg. 2006, 18, 61–71. [Google Scholar] [CrossRef]
- Cakir, B.; Richter, M.; Käfer, W.; Puhl, W.; Schmidt, R. The impact of total lumbar disc replacement on segmental and total lumbar lordosis. Clin. Biomech. 2005, 20, 357–364. [Google Scholar] [CrossRef]
- Blamoutier, A. Surgical discectomy for lumbar disc herniation: Surgical techniques. Orthop. Traumatol. Surg. Res. 2013, 99, S187–S196. [Google Scholar] [CrossRef]
- Katayama, Y.; Matsuyama, Y.; Yoshihara, H.; Sakai, Y.; Nakamura, H.; Nakashima, S.; Ito, Z.; Ishiguro, N. Comparison of surgical outcomes between macro discectomy and micro discectomy for lumbar disc herniation: A prospective randomized study with surgery performed by the same spine surgeon. J. Spinal Disord. Technol. 2006, 19, 344–347. [Google Scholar] [CrossRef]
- Goel, V.K.; Goyal, S.; Clark, C.; Nishiyama, K.; Nye, T. Kinematics of the whole lumbar spine. Effect of discectomy. Spine 1985, 10, 543–554. [Google Scholar] [CrossRef]
- Strenge, K.B.; DiPaola, C.P.; Miller, L.E.; Hill, C.P.; Whitmore, R.G. Multicenter study of lumbar discectomy with Barricaid annular closure device for prevention of lumbar disc reherniation in US patients. Medicine 2019, 98, e16953. [Google Scholar] [CrossRef]
- Miller, L.E.; McGirt, M.J.; Garfin, S.R.; Bono, C.M. Association of Annular Defect Width After Lumbar Discectomy With Risk of Symptom Recurrence and Reoperation: Systematic Review and Meta-analysis of Comparative Studies. Spine 2018, 43, E308–E315. [Google Scholar] [CrossRef] [PubMed]
- Heuer, F.; Ulrich, S.; Claes, L.; Wilke, H.-J. Biomechanical evaluation of conventional anulus fibrosus closure methods required for nucleus replacement. Laboratory investigation. J. Neurosurg. Spine 2008, 9, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.A.; Stefanakis, M.; Dolan, P. Healing of a painful intervertebral disc should not be confused with reversing disc degeneration: Implications for physical therapies for discogenic back pain. Clin. Biomech. 2010, 25, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Marcolongo, M.; Sarkar, S.; Ganesh, N. Trends in materials for spine surgery. In Comprehensive Biomaterials; Paul, D., Ed.; Elsevier: Oxford, UK, 2011. [Google Scholar]
- Koepsell, L.; Zhang, L.; Neufeld, D.; Fong, H.; Deng, Y. Electrospun Nanofibrous Polycaprolactone Scaffolds for Tissue Engineering of Annulus Fibrosus. Macromol. Biosci. 2011, 11, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, J.; Diwan, A.D.; Tipper, J.L. Advanced Strategies for the Regeneration of Lumbar Disc Annulus Fibrosus. Int. J. Mol. Sci. 2020, 21, 4889. [Google Scholar] [CrossRef]
- Bailey, A.; Messer, J.; Griffith, S.L.; Anular Repair Clinical Study Group. Prospective, randomized controlled study of repairing the anulus fibrosus after lumbar discectomy: A single surgeon’s experience. Spine J. 2010, 10, 127S. [Google Scholar] [CrossRef]
- Bateman, A.H.; Balkovec, C.; Akens, M.K.; Chan, A.H.W.; Harrison, R.D.; Oakden, W.; Yee, A.J.M.; McGill, S.M. Closure of the annulus fibrosus of the intervertebral disc using a novel suture application device-in vivo porcine and ex vivo biomechanical evaluation. Spine J. 2016, 16, 889–895. [Google Scholar] [CrossRef]
- Qi, L.; Li, M.; Si, H.; Wang, L.; Jiang, Y.; Zhang, S.; Li, L. The clinical application of ‘jetting suture’ technique in annular repair under microendoscopic discectomy: A prospective single-cohort observational study. Medicine 2016, 95, e4503. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, A.; Wales, L.; Houfburg, R.; Durfee, W.K.; Griffith, S.L.; Bentley, I. Optimizing the effectiveness of a mechanical suture-based anulus fibrosus repair construct in an acute failure laboratory simulation. J. Spinal Disord. Technol. 2013, 26, 393–399. [Google Scholar] [CrossRef]
- Chiang, Y.-F.; Chiang, C.-J.; Yang, C.-H.; Zhong, Z.-C.; Chen, C.-S.; Cheng, C.-K.; Tsuang, Y.-H. Retaining intradiscal pressure after annulotomy by different annular suture techniques, and their biomechanical evaluations. Clin. Biomech. 2012, 27, 241–248. [Google Scholar] [CrossRef]
- Chiang, C.-J.; Cheng, C.-K.; Sun, J.-S.; Liao, C.-J.; Wang, Y.-H.; Tsuang, Y.-H. The effect of a new anular repair after discectomy in intervertebral disc degeneration: An experimental study using a porcine spine model. Spine 2011, 36, 761–769. [Google Scholar] [CrossRef]
- Anulex Technologies, Inc. Xclose Tissue Repair System, Model XC-200-01, Premarket filed with FDA. 2009. Available online: https://fda.report/PMN/K091432 (accessed on 20 November 2021).
- Ahlgren, B.D.; Lui, W.; Herkowitz, H.N.; Panjabi, M.M.; Guiboux, J.P. Effect of anular repair on the healing strength of the intervertebral disc: A sheep model. Spine 2000, 25, 2165–2170. [Google Scholar] [CrossRef]
- Anulex Technologies, Inc. 501(K) Summary of Safety and Effectiveness: Inclose Surgical Mesh System. 2005. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf5/k050969.pdf (accessed on 22 November 2021).
- Grunert, P.; Borde, B.H.; Hudson, K.D.; Macielak, M.R.; Bonassar, L.J.; Härtl, R. Annular repair using high density collagen gel: In vivo outcome in a rodent spine model. Spine J. 2013, 13, 51S. [Google Scholar] [CrossRef]
- Likhitpanichkul, M.; Dreischarf, M.; Illien-Junger, S.; Walter, B.; Nukaga, T.; Long, R.; Sakai, D.; Hecht, A.; Iatridis, J. Fibrin-genipin adhesive hydrogel for annulus fibrosus repair: Performance evaluation with large animal organ culture, in situ biomechanics, and in vivo degradation tests. Eur. Cell. Mater. 2014, 28, 25–28. [Google Scholar] [CrossRef]
- Guterl, C.C.; Torre, O.M.; Purmessur, D.; Dave, K.; Likhitpanichkul, M.; Hecht, A.C.; Nicoll, S.B.; Iatridis, J.C. Characterization of Mechanics and Cytocompatibility of Fibrin-Genipin Annulus Fibrosus Sealant with the Addition of Cell Adhesion Molecules. Tissue Eng. Part A 2014, 20, 2536–2545. [Google Scholar] [CrossRef] [PubMed]
- Vergroesen, P.-P.A.; Bochyn Ska, A.I.; Emanuel, K.S.; Sharifi, S.; Kingma, I.; Grijpma, D.W.; Smit, T.H. A biodegradable glue for annulus closure: Evaluation of strength and endurance. Spine 2015, 40, 622–628. [Google Scholar] [CrossRef]
- Grunert, P.; Borde, B.H.; Towne, S.B.; Moriguchi, Y.; Hudson, K.D.; Bonassar, L.J.; Härtl, R. Riboflavin crosslinked high-density collagen gel for the repair of annular defects in intervertebral discs: An in vivo study. Acta Biomater. 2015, 26, 215–224. [Google Scholar] [CrossRef]
- Likhitpanichkul, M.; Kim, Y.; Torre, O.M.; See, E.; Kazezian, Z.; Pandit, A.; Hecht, A.C.; Iatridis, J.C. Fibrin-genipin annulus fibrosus sealant as a delivery system for anti-TNFα drug. Spine J. 2015, 15, 2045–2054. [Google Scholar] [CrossRef]
- Kang, R.; Li, H.; Lysdahl, H.; Svend Le, D.Q.; Chen, M.; Xie, L. Cody Bünger Cyanoacrylate medical glue application in intervertebral disc annulus defect repair: Mechanical and biocompatible evaluation. J. Biomed. Mater. Res. Part B Appl. Biomater. 2017, 105, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Cruz, M.A.; McAnany, S.; Gupta, N.; Long, R.G.; Nasser, P.; Eglin, D.; Hecht, A.C.; Illien-Junger, S.; Iatridis, J.C. Structural and Chemical Modification to Improve Adhesive and Material Properties of Fibrin-Genipin for Repair of Annulus Fibrosus Defects in Intervertebral Disks. J. Biomech. Eng. 2017, 139, 0845011–0845017. [Google Scholar] [CrossRef]
- Chik, T.; Ma, X.; Choy, T.; Li, Y.; Diao, H.; Teng, W.; Han, S.; Cheung, K.; Chan, B. Photochemically crosslinked collagen annulus plug: A potential solution solving the leakage problem of cell-based therapies for disc degeneration. Acta Biomater. 2013, 9, 8128–8139. [Google Scholar] [CrossRef]
- Bron, J.L.; van der Veen, A.J.; Helder, M.N.; van Royen, B.J.; Smit, T.H. Biomechanical and in vivo evaluation of experimental closure devices of the annulus fibrosus designed for a goat nucleus replacement model. Eur. Spine J. 2010, 19, 1347–1355. [Google Scholar] [CrossRef] [PubMed]
- Ledet, E.H.; Jeshuran, W.; Glennon, J.C.; Shaffrey, C.; De Deyne, P.; Belden, C.; Kallakury, B.; Carl, A.L. Small intestinal submucosa for anular defect closure: Long-term response in an in vivo sheep model. Spine 2009, 34, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.; Araghi, A.; Blumenthal, S.; Huffmon, G.V.; Anular Repair Clinical Study Group. Prospective, multicenter, randomized, controlled study of anular repair in lumbar discectomy: Two-year follow-up. Spine 2013, 38, 1161–1169. [Google Scholar] [CrossRef]
- Martens, F.; Lesage, G.; Muir, J.M.; Stieber, J.R. Implantation of a bone-anchored annular closure device in conjunction with tubular minimally invasive discectomy for lumbar disc herniation: A retrospective study. BMC Musculoskelet. Disord. 2018, 19, 269. [Google Scholar] [CrossRef]
- Choy, W.J.; Phan, K.; Diwan, A.D.; Ong, C.S.; Mobbs, R.J. Annular closure device for disc herniation: Meta-analysis of clinical outcome and complications. BMC Musculoskelet. Disord. 2018, 19, 290. [Google Scholar] [CrossRef]
- Ardeshiri, A.; Miller, L.E.; Synowitz, M.; Jadik, S. Surgical Experience and Complications in 50 Patients Treated with an Anular Closure Device Following Lumbar Discectomy. Orthop. Surg. 2019, 11, 431–437. [Google Scholar] [CrossRef]
- Krutko, A.V.; Baykov, E.S.; Sadovoy, M.A. Reoperation after microdiscectomy of lumbar herniation: Case report. Int. J. Surg. Case Rep. 2016, 24, 119–123. [Google Scholar] [CrossRef][Green Version]
- Intrinsic Therapeutics. Instructions for Use Barricaid® Anular Closure Device (ACD). Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160050D.pdf (accessed on 20 November 2021).
- Lange, N.; Meyer, B.; Shiban, E. Symptomatic annulus-repair-device loosening due to a low-grade infection. Acta Neurochir. 2018, 160, 199–203. [Google Scholar] [CrossRef]
- Guterl, C.; See, E.; Blanquer, S.; Pandit, A.; Ferguson, S.; Benneker, L.; Grijpma, D.; Sakai, D.; Eglin, D.; Alini, M.; et al. Challenges and strategies in the repair of ruptured annulus fibrosus. Eur. Cell. Mater. 2012, 25, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Chamoli, U.; Umali, J.; Kleuskens, M.W.A.; Chepurin, D.; Diwan, A.D. Morphological characteristics of the kangaroo lumbar intervertebral discs and comparison with other animal models used in spine research. Eur. Spine J. 2019, 29, 652–662. [Google Scholar] [CrossRef]
- Adams, M.A.; Lama, P.; Zehra, U.; Dolan, P. Why do some intervertebral discs degenerate, when others (in the same spine) do not? Clin. Anat. 2015, 28, 195–204. [Google Scholar] [CrossRef]
- Bron, J.L.; Helder, M.N.; Meisel, H.-J.; van Royen, B.J.; Smit, T.H. Repair, regenerative and supportive therapies of the annulus fibrosus: Achievements and challenges. Eur. SPINE J. 2009, 18, 301–313. [Google Scholar] [CrossRef]
- Hastreiter, D.; Ozuna, R.M.; Spector, M. Regional variations in certain cellular characteristics in human lumbar intervertebral discs, including the presence of α-smooth muscle actin. J. Orthop. Res. 2001, 19, 597–604. [Google Scholar] [CrossRef]
- Salzmann, S.N.; Plais, N.; Shue, J.; Girardi, F.P. Lumbar disc replacement surgery-successes and obstacles to widespread adoption. Curr. Rev. Musculoskelet. Med. 2017, 10, 153–159. [Google Scholar] [CrossRef]
- Schnake, K.J.; Putzier, M.; Haas, N.P.; Kandziora, F. Mechanical concepts for disc regeneration. Eur. Spine J. 2006, 15, 3. [Google Scholar] [CrossRef]
- Tavakoli, J. Tissue Engineering of the Intervertebral Disc’s Annulus Fibrosus: A Scaffold-Based Review Study. Tissue Eng. Regen. Med. 2017, 14, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Melrose, J.; Smith, S.M.; Little, C.B.; Moore, R.J.; Vernon-Roberts, B.; Fraser, R.D. Recent advances in annular pathobiology provide insights into rim-lesion mediated intervertebral disc degeneration and potential new approaches to annular repair strategies. Eur. Spine J. 2008, 17, 1131–1148. [Google Scholar] [CrossRef]
- Zhang, Y.; Chee, A.; Thonar, E.J.-M.A.; An, H.S. Intervertebral Disk Repair by Protein, Gene, or Cell Injection: A Framework for Rehabilitation-Focused Biologics in the Spine. PM&R 2011, 3, S88–S94. [Google Scholar]
- Moriguchi, Y.; Alimi, M.; Khair, T.; Manolarakis, G.; Berlin, C.; Bonassar, L.J.; Härtl, R. Biological Treatment Approaches for Degenerative Disk Disease: A Literature Review of in Vivo Animal and Clinical Data. Glob. Spine J. 2016, 6, 497–518. [Google Scholar] [CrossRef] [PubMed]
- Benneker, L.M.; Anderson, G.; Iatridis, J.S.; Sakai, D.; Härtl, R.; Ito, K.; Grad, S. Cell therapy for intervertebral disc repair: Advancing cell therapy from bench to clinics. Eur. Cells Mater. 2014, 27, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Bowles, R.D.; Setton, L.A. Biomaterials for intervertebral disc regeneration and repair. Biomaterials 2017, 129, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Buckley, C.T.; Hoyland, J.A.; Fujii, K.; Pandit, A.; Iatridis, J.C.; Grad, S. Critical aspects and challenges for intervertebral disc repair and regeneration-Harnessing advances in tissue engineering. JOR Spine 2018, 1, e1029. [Google Scholar] [CrossRef] [PubMed]
- Long, R.G.; Torre, O.M.; Hom, W.W.; Assael, D.J.; Iatridis, J.C. Design Requirements for Annulus Fibrosus Repair: Review of Forces, Displacements, and Material Properties of the Intervertebral Disk and a Summary of Candidate Hydrogels for Repair. J. Biomech. Eng. 2016, 138, 021007. [Google Scholar] [CrossRef] [PubMed]
- Goodman Campbell Brain and Spine. Spine Anatomy. Available online: https://www.goodmancampbell.com/spine-anatomy (accessed on 30 May 2018).
- Baldit, A. PMicromechanics of the Intervertebral Disk. In Multiscale Biomechanics Part 3; Ganghoffer, J.F., Ed.; Elsevier Ltd.: Amsterdam, The Netherlands, 2018; Chapter 11; pp. 455–467. ISBN 978-78548-208-3. [Google Scholar] [CrossRef]
- Vergroesen, P.-P.; Kingma, I.; Emanuel, K.; Hoogendoorn, R.; Welting, T.; van Royen, B.; van Dieën, J.; Smit, T. Mechanics and biology in intervertebral disc degeneration: A vicious circle. Osteoarthr. Cartil. 2015, 23, 1057–1070. [Google Scholar] [CrossRef]
- Bach, K.; Ford, J.; Foley, R.; Januszewski, J.; Murtagh, R.; Decker, S.; Uribe, J.S. Morphometric Analysis of Lumbar Intervertebral Disc Height: An Imaging Study. World Neurosurg. 2019, 124, e106–e118. [Google Scholar] [CrossRef] [PubMed]
- Grunhagen, T.; Wilde, G.; Soukane, D.M.; Shirazi-Adl, S.A.; Urban, J. Nutrient Supply and Intervertebral Disc Metabolism. J. Bone Jt. Surg. 2006, 88, 30. [Google Scholar]
- Grunhagen, T.; Shirazi-Adl, A.; Fairbank, J.C.T.; Urban, J.P.G. Intervertebral Disk Nutrition: A Review of Factors Influencing Concentrations of Nutrients and Metabolites. Orthop. Clin. N. Am. 2011, 42, 465–477. [Google Scholar] [CrossRef]
- Yin, S.; Du, H.; Zhao, W.; Ma, S.; Zhang, M.; Guan, M.; Liu, M. Inhibition of both endplate nutritional pathways results in intervertebral disc degeneration in a goat model. J. Orthop. Surg. Res. 2019, 14, 138. [Google Scholar] [CrossRef]
- Martins, D.E.; De Medeiros, V.P.; Wajchenberg, M.; Paredes-Gamero, E.J.; Lima, M.; Reginato, R.D.; Nader, H.; Puertas, E.B.; Faloppa, F. Changes in human intervertebral disc biochemical composition and bony end plates between middle and old age. PLoS ONE 2018, 13, e0203932. [Google Scholar] [CrossRef]
- Sanginov, A.J.; Krutko, A.V.; Baykov, E.S.; Lutsik, A.A. Outcomes of surgical treatment of lumbar disk herniation using an annular closure device. Coluna/ Columna 2018, 17, 188–194. [Google Scholar] [CrossRef]
- Gilbert, H.T.J.; Hodson, N.; Baird, P.; Richardson, S.M.; Hoyland, J.A. Acidic pH promotes intervertebral disc degeneration: Acid-sensing ion channel -3 as a potential therapeutic target. Sci. Rep. 2016, 6, 37360. [Google Scholar] [CrossRef]
- Akgun, B.; Ozturk, S.; Cakin, H.; Kaplan, M. Migration of fragments into the spinal canal after intervertebral polyethylene glycol implantation: An extremely rare adverse effect. J. Neurosurg. Spine 2014, 21, 614–616. [Google Scholar] [CrossRef]
- Daly, C.; Ghosh, P.; Jenkin, G.; Oehme, D.; Goldschlager, T. A Review of Animal Models of Intervertebral Disc Degeneration: Pathophysiology, Regeneration, and Translation to the Clinic. BioMed Res. Int. 2016, 2016, 5952165. [Google Scholar] [CrossRef]
- Newell, N.; Little, J.P.; Christou, A.; Adams, M.A.M.; Adam, C.J.; Masouros, S.D.S.D. Biomechanics of the human intervertebral disc: A review of testing techniques and results. J. Mech. Behav. Biomed. Mater. 2016, 69, 420–434. [Google Scholar] [CrossRef]
- Goel, V.K.; Monroe, B.T.; Gilbertson, L.G.; Brinckmann, P. Interlaminar shear stresses and laminae separation in a disc: Finite element analysis of the l3-l4 motion segment subjected to axial compressive loads. Spine 1995, 20, 689–698. [Google Scholar] [CrossRef]
- Eberlein, R.; Holzapfel, G.A.; Schulze-Bauer, C.A.J. An anisotropic model for annulus tissue and enhanced finite element analyses of intact lumbar disc bodies. Comput. Methods Biomech. Biomed. Engin. 2001, 4, 209–229. [Google Scholar] [CrossRef]
- Qasim, M.; Natarajan, R.N.; An, H.S.; Andersson, G.B.J. Initiation and progression of mechanical damage in the intervertebral disc under cyclic loading using continuum damage mechanics methodology: A finite element study. J. Biomech. 2012, 45, 1934–1940. [Google Scholar] [CrossRef] [PubMed]
- Shahraki, N.M.; Fatemi, A.; Agarwal, A.; Goel, V.K. Prediction of clinically relevant initiation and progression of tears within annulus fibrosus. J. Orthop. Res. 2017, 35, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Moroni, L.; Lambers, F.M.; Wilson, W.; van Donkelaar, C.C.; de Wijn, J.R.; Huiskes, R.; and van Blitterswijk, C.A. Finite Element Analysis of Meniscal Anatomical 3D Scaffolds: Implications for Tissue Engineering. Open Biomed. Eng. J. 2007, 1, 23–34. [Google Scholar] [CrossRef]
- Lacroix, D.; Planell, J.A.; Prendergast, P.J. Computer-aided design and finite-element modelling of biomaterial scaffolds for bone tissue engineering. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2009, 367, 1993–2009. [Google Scholar] [CrossRef] [PubMed]
- Galante, R.; Pinto, T.J.A.; Colaço, R.; Serro, A.P. Sterilization of hydrogels for biomedical applications: A review. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 106, 2472–2492. [Google Scholar] [CrossRef]
- Lu, H.H.; Thomopoulos, S. Functional Attachment of Soft Tissues to Bone: Development, Healing, and Tissue Engineering. Annu. Rev. Biomed. Eng. 2013, 15, 201–226. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.M.; Costa, F.; Tralhão, A.; Marques, H.; Cardim, N.; Adragão, P. MRI-conditional pacemakers: Current perspectives. In Medical Devices: Evidence and Research; Dove Medical Press Ltd.: Auckland, New Zealand, 2014; Volume 7, pp. 115–124. [Google Scholar] [CrossRef]
- ASTM F2052-15, Standard Test Method for Measurement of Magnetically Induced Displacement Force on Medical Devices in the Magnetic Resonance Environment; ASTM International: West Conshohocken, PA, USA, 2015.
- Zhu, J.; Marchant, R.E. Design properties of hydrogel tissue-engineering scaffolds. Expert Rev. Med. Devices 2011, 8, 607–626. [Google Scholar] [CrossRef] [PubMed]
- Drazin, D.; Ugiliweneza, B.; Al-Khouja, L.; Yang, D.; Johnson, P.; Kim, T.; Boakye, M. Treatment of Recurrent Disc Herniation: A Systematic Review. Cureus 2016, 8, e622. [Google Scholar] [CrossRef] [PubMed]
- Martens, F.; Vajkoczy, P.; Jadik, S.; Hegewald, A.; Stieber, J.; Hes, R. Patients at the Highest Risk for Reherniation Following Lumbar Discectomy in a Multicenter Randomized Controlled Trial. JBJS Open Access 2018, 3, e0037. [Google Scholar] [CrossRef] [PubMed]
- Abdu, R.W.; Abdu, W.A.; Pearson, A.M.; Zhao, W.; Lurie, J.D.; Weinstein, J.N. Reoperation for Recurrent Intervertebral Disc Herniation in the Spine Patient Outcomes Research Trial. Spine 2017, 42, 1106–1114. [Google Scholar] [CrossRef]
- Kienzler, J.C.; Klassen, P.D.; Miller, L.E.; Assaker, R.; Heidecke, V.; Frohlich, S.; Thome, C.; Annular Closure RCT Study Group. Three-year results from a randomized trial of lumbar discectomy with annulus fibrosus occlusion in patients at high risk for reherniation. Acta Neurochir. 2019, 161, 1389–1396. [Google Scholar] [CrossRef]
- Haefeli, M.; Elfering, A. Pain assessment. Eur. Spine J. 2006, 15, S17–S24. [Google Scholar] [CrossRef] [PubMed]
- BS ISO 18192-2:2010, Implants for Surgery—Wear of Total Intervertebral Spinal Disc Prostheses; Nucleus Replacements; British Standards Institution: London, UK, 2010.
- BS ISO 18192-3:2017, Implants for Surgery. Wear of Total Intervertebral Spinal Disc Prostheses; Impingement-Wear Testing and Corresponding Environmental Conditions for Test of Lumbar Prostheses under Adverse Kinematic Conditions; British Standards Institution: London, UK, 2017.
- BS ISO 18192-1:2011+A1:2018, Implants for Surgery. Wear of Total Intervertebral Spinal Disc Prostheses; Loading and Displacement Parameters for Wear Testing and Corresponding Environmental Conditions for Test; British Standards Institution: London, UK, 2011.
- ASTM F1717-18, Standard Test Methods for Spinal Implant Constructs in a Vertebrectomy Model; ASTM International: West Conshohocken, PA, USA, 2018.
- ASTM F2789-10, Standard Guide for Mechanical and Functional Characterization of Nucleus Devices; ASTM International: West Conshohocken, PA, USA, 2015.
- ASTM F2346-18, Standard Test Methods for Static and Dynamic Characterization of Spinal Artificial Discs; ASTM International: West Conshohocken, PA, USA, 2018.
- ASTM F2423-11, Standard Guide for Functional, Kinematic, and Wear Assessment of Total Disc Prostheses; ASTM International: West Conshohocken, PA, USA, 2016.
- ASTM F3295-18, Standard Guide for Impingement Testing of Total Disc Prostheses; ASTM International: West Conshohocken, PA, USA, 2018.
- BS EN ISO 10993, Biological Evaluation of Medical Devices Parts 1–20; British Standards Institution: London, UK, 2009–2021.
- ASTM F981-04, Standard Practice for Assessment of Compatibility of Biomaterials for Surgical Implants with Respect to Effect of Materials on Muscle and Insertion into Bone; ASTM International: West Conshohocken, PA, USA, 2016.
- ASTM F1983-14, Standard Practice for Assessment of Selected Tissue Effects of Absorbable Biomaterials for Implant Applications; ASTM International: West Conshohocken, PA, USA, 2014.
- ASTM F3142-16, Standard Guide for Evaluation of in vitro Release of Biomolecules from Biomaterials Scaffolds for TEMPs; ASTM International: West Conshohocken, PA, USA, 2016.
- ASTM F2150-19, Standard Guide for Characterization and Testing of Biomaterial Scaffolds Used in Regenerative Medicine and Tissue-Engineered Medical Products 1; ASTM International: West Conshohocken, PA, USA, 2019.
- ASTM F3224-17, Standard Test Method for Evaluating Growth of Engineered Cartilage Tissue Using Magnetic Resonance Imaging 1; ASTM International: West Conshohocken, PA, USA, 2017.



{kind=link}
{kind=link}
| Design Criteria for Hydrogel-Based Repair Strategies | Recommended Design Parameters | |
|---|---|---|
| Parameter | Recommended Value | |
| Device adhesion testing | IVD pressure, after implantation | 1.5 MPa |
| Similar biomaterial properties to native tissue | IVD pressure, maximal | 2.3 MPa |
| Tensile modulus, axial | 0.5–1 MPa | |
| Biocompatibility and cytotoxicity | Compressive/tensile strain | 28%/65% |
| Biomaterial degradation rate | Axial stiffness of restored IVD | 1.5–2 kN/mm |
| Biomechanics evaluation | Torsional stiffness of restored IVD | 3.2 Nm/deg |
| Reherniation risk | Tensile modulus, circumferential | 11–29 MPa |
| Aggregate modulus | 0.4–6 MPa | |
| Shear modulus | 0.1–0.28 MPa | |
| Range of Motion | ||||
|---|---|---|---|---|
| Mean angle (degrees) | ||||
| Flexion | 6°–13° | |||
| Extension | 1°–5° | |||
| Lateral bending | 2.9°–11° | |||
| Axial rotation | 2°–3° | |||
| Intradiscal Pressure | ||||
| Mean (MPa) | Maximum (MPa) | |||
| Prone | 0.22 | 0.41 | ||
| Sitting | 0.75 | 1.50 | ||
| Standing | 0.59 | 1.07 | ||
| IVD Height (mm) | ||||
| Anterior | Posterior | |||
| Male | Female | Male | Female | |
| L1-L2 | 7.48 ± 1.5 | 5.92 ± 1.2 | 4.91 ± 1.2 | 4.34 ± 0.9 |
| L2-L3 | 8.54 ± 1.5 | 7.15 ± 1.5 | 5.65 ± 1.4 | 5.11 ± 1 |
| L3-L4 | 9.58 ± 1.7 | 8.08 ± 1.4 | 6.02 ± 1.4 | 5.57 ± 1.2 |
| L4-L5 | 10.89 ± 2.1 | 9.76 ± 1.9 | 6.11 ± 1.3 | 5.97 ± 1.4 |
| L5-S1 | 11.8 ± 2.6 | 11.22 ± 2.5 | 5.24 ± 1.4 | 5.2 ± 1.4 |
| Category | Standard | Scope |
|---|---|---|
| Mechanical | BS ISO 18192-2:2010: Implants for surgery. Wear of total intervertebral spinal disc prostheses. Nucleus replacements [101] |
|
| BS ISO 18192-3:2017: Implants for surgery. Wear of total intervertebral spinal disc prostheses. Impingement-wear testing and corresponding environmental conditions for test of lumbar prostheses under adverse kinematic conditions [102] |
| |
| BS ISO 18192-1:2011+A1:2018: Implants for surgery. Wear of total intervertebral spinal disc prostheses. Loading and displacement parameters for wear testing and corresponding environmental conditions for test [103] |
| |
| Mechanical (continued) | ASTM F1717-18: Standard Test Methods For Spinal Implant Constructs In A Vertebrectomy Model [104] |
|
| ASTM F2789-10(2015): Standard Guide for Mechanical and Functional Characterization of Nucleus Devices [105] |
| |
| ASTM F2346-18: Standard Test Methods for Static and Dynamic Characterization of Spinal Artificial Discs [106] |
| |
| ASTM F2423-11(2016): Standard Guide for Functional, Kinematic, and Wear Assessment of Total Disc Prostheses [107] |
| |
| Mechanical (continued) | ASTM F3295-18: Standard Guide for Impingement Testing of Total Disc Prostheses [108] |
|
| Biological | BS EN ISO 10993: Biological evaluation of medical devices, Parts 1–20 [109] |
|
| ASTM F981-04(2016): Standard Practice for Assessment of Compatibility of Biomaterials for Surgical Implants with Respect to Effect of Materials on Muscle and Insertion into Bone [110] |
| |
| Biological (continued) | ASTM F1983-14: Standard Practice for Assessment of Selected Tissue Effects of Absorbable Biomaterials for Implant Applications [111] |
|
| Materials | ASTM F3142-16: Standard Guide for Evaluation of in vitro Release of Biomolecules from Biomaterials Scaffolds for Tissue-Engineered Medical Products (TEMPs) [112] |
|
| ASTM F2150-19: Standard Guide for Characterization and Testing of Biomaterial Scaffolds Used in Regenerative Medicine and Tissue-Engineered Medical Products [113] |
| |
| Imaging | ASTM F2052-15: Standard Test Method for Measurement of Magnetically Induced Displacement Force on Medical Devices in the Magnetic Resonance Environment [94] |
|
| ASTM F3224-17: Standard Test Method for Evaluating Growth of Engineered Cartilage Tissue using Magnetic Resonance Imaging [114] |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guardado, A.A.; Baker, A.; Weightman, A.; Hoyland, J.A.; Cooper, G. Lumbar Intervertebral Disc Herniation: Annular Closure Devices and Key Design Requirements. Bioengineering 2022, 9, 47. https://doi.org/10.3390/bioengineering9020047
Guardado AA, Baker A, Weightman A, Hoyland JA, Cooper G. Lumbar Intervertebral Disc Herniation: Annular Closure Devices and Key Design Requirements. Bioengineering. 2022; 9(2):47. https://doi.org/10.3390/bioengineering9020047
Chicago/Turabian StyleGuardado, Alexandra Alcántara, Alexander Baker, Andrew Weightman, Judith A. Hoyland, and Glen Cooper. 2022. "Lumbar Intervertebral Disc Herniation: Annular Closure Devices and Key Design Requirements" Bioengineering 9, no. 2: 47. https://doi.org/10.3390/bioengineering9020047
APA StyleGuardado, A. A., Baker, A., Weightman, A., Hoyland, J. A., & Cooper, G. (2022). Lumbar Intervertebral Disc Herniation: Annular Closure Devices and Key Design Requirements. Bioengineering, 9(2), 47. https://doi.org/10.3390/bioengineering9020047