
Risk Factors Associated with Mortality in Hospitalized Patients with COVID-19 during the Omicron Wave in Brazil

 ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Inclusion Criteria
- Population: inpatients over 18 years old, obtained from the SIVEP-Gripe database records [23], testing positive for COVID-19.
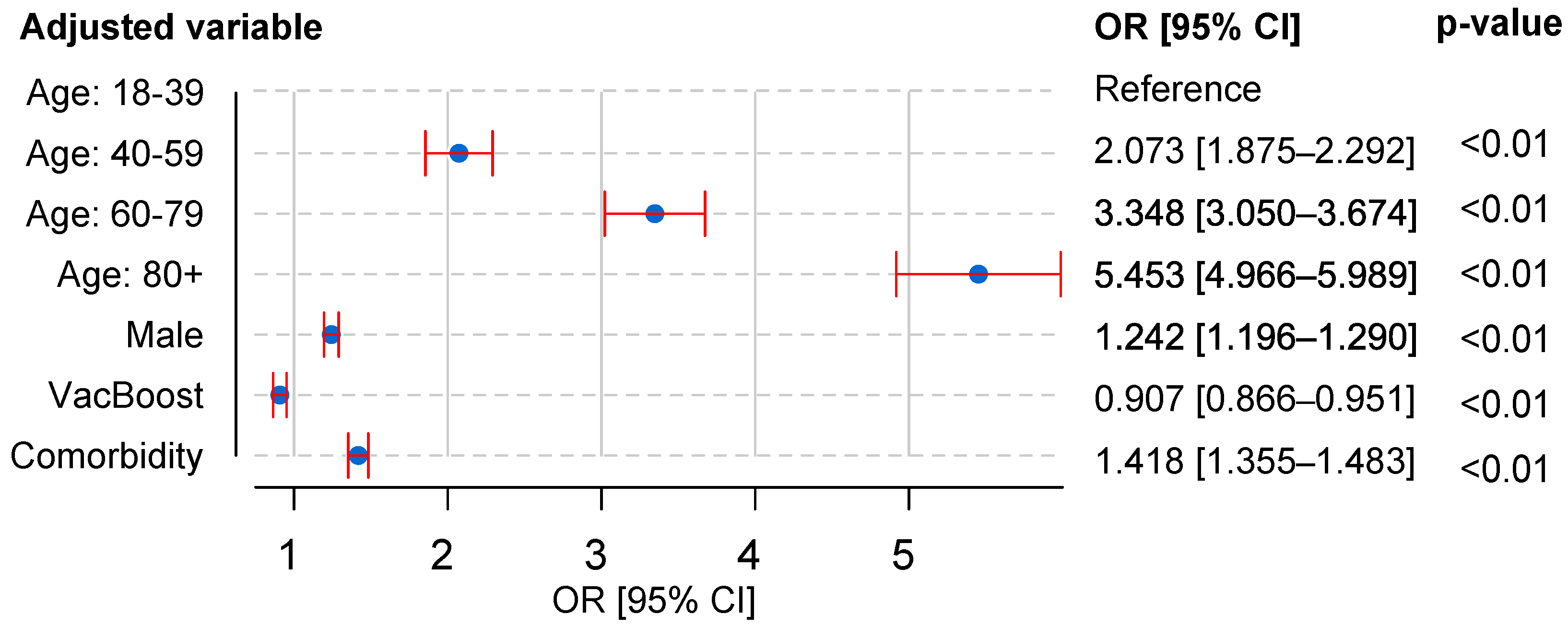
- Risk factors: gender (M), age (40–59 years; 60–79 years; and 80 years or older), incomplete vaccination (i.e., without the third dose of vaccine), and comorbidities (as previously listed).
- Analysis period: 1 February to 31 March 2022.
2.3. Exclusion Criteria
2.4. Statistical Analysis
- Hospitalized patients aged 40–59 years, aged 60–79 years, and 80 years or older.
- Male hospitalized patients.
- Those with at least one comorbid condition.
- Those with an incomplete vaccination status.
2.5. Computing Platform and Programming Language
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Moreira, R.d.S. COVID-19: Unidades de terapia intensiva, ventiladores mecânicos e perfis latentes de mortalidade associados à letalidade no Brasil. Cadernos de Saúde Pública 2020, 36, e00080020. [Google Scholar] [CrossRef] [PubMed]
- Lima, E.E.; Vilela, E.A.; Peralta, A.; Rocha, M.; Queiroz, B.L.; Gonzaga, M.R.; Piscoya-Díaz, M.; Martinez-Folgar, K.; García-Guerrero, V.M.; Freire, F.H. Investigating regional excess mortality during 2020 COVID-19 pandemic in selected Latin American countries. Genus 2021, 77, 1–20. [Google Scholar] [CrossRef]
- Almeida, F. Exploring the impact of COVID-19 on the sustainability of health critical care systems in South America. Int. J. Health Policy Manag. 2021, 10, 462. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tracking SARS-CoV-2 Variants. 2022. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants (accessed on 10 June 2022).
- Gu, H.; Krishnan, P.; Ng, D.Y.; Chang, L.D.; Liu, G.Y.; Cheng, S.S.; Hui, M.M.; Fan, M.C.; Wan, J.H.; Lau, L.H.; et al. Probable transmission of SARS-CoV-2 omicron variant in quarantine hotel, Hong Kong, China, November 2021. Emerg. Infect. Dis. 2022, 28, 460. [Google Scholar] [CrossRef]
- Elliott, P.; Bodinier, B.; Eales, O.; Wang, H.; Haw, D.; Elliott, J.; Whitaker, M.; Jonnerby, J.; Tang, D.; Walters, C.E.; et al. Rapid increase in Omicron infections in England during December 2021: REACT-1 study. Science 2022, 375, 1406–1411. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, N.; Ghani, A.; Cori, A.; Hogan, A.; Hinsley, W.; Volz, E. Report 49: Growth, Population Distribution and Immune Escape of Omicron in England; Imperial College London: London, UK, 2021. [Google Scholar]
- Tian, D.; Sun, Y.; Xu, H.; Ye, Q. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J. Med. Virol. 2022, 94, 2376–2383. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.S.; Müller, G.C.; Campos, F.E.M.; Borges, M.E.; de Almeida, G.B.; Poloni, S.; Simon, L.M.; Bagattini, Â.M.; da Rosa, M.Q.M.; Filho, J.A.F.D.F.; et al. Modelagem do Impacto Estimado da Vacinação de Crianças de 5–11 anos Contra a COVID-19 no Brasil. 2022. Available online: https://sbim.org.br/images/files/modelagem-vacinacao-criancas-15fev2022.pdf (accessed on 13 June 2022).
- Secretaria Extraordinária de Enfrentamento à COVID-19. Report No: 65/2021-SECOVID/GAB/SECOVID/MS; Technical Report; Ministry of Health (Brazil): Brasília, Brazil, 2021. [Google Scholar]
- Hippisley-Cox, J.; Coupland, C.A.; Mehta, N.; Keogh, R.H.; Diaz-Ordaz, K.; Khunti, K.; Lyons, R.A.; Kee, F.; Sheikh, A.; Rahman, S.; et al. Risk prediction of covid-19 related death and hospital admission in adults after covid-19 vaccination: National prospective cohort study. BMJ 2021, 374, n2244. [Google Scholar] [CrossRef]
- Fang, H.; Liu, Q.; Xi, M.; Xiong, D.; He, J.; Luo, P.; Li, Z. Impact of comorbidities on clinical prognosis in 1280 patients with different types of COVID-19. J. Investig. Med. 2021, 69, 75–85. [Google Scholar] [CrossRef]
- Malik, J.A.; Ahmed, S.; Shinde, M.; Al-Marmash, M.H.S.; Alghamdi, S.; Hussain, A.; Anwar, S. The impact of COVID-19 on the comorbidities: A review of recent updates for combating it. Saudi J. Biol. Sci. 2022, 29, 3586–3599. [Google Scholar] [CrossRef] [PubMed]
- Henkens, M.; Raafs, A.; Verdonschot, J.; Linschoten, M.; van Smeden, M.; Wang, P.; van der Hooft, B.; Tieleman, R.; Janssen, M.; Ter Bekke, R.; et al. Age is the main determinant of COVID-19 related in-hospital mortality with minimal impact of pre-existing comorbidities, a retrospective cohort study. BMC Geriatr. 2022, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Endeshaw, Y.; Campbell, K. Advanced age, comorbidity and the risk of mortality in COVID-19 infection. J. Natl. Med. Assoc. 2022, 114, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.C.; Chang, W.W.; Lee, W.S. Analysis of an outbreak of COVID-19 (alpha-variant) with rapid progression to mortality in Taipei, Taiwan. J. Infect. 2022, 84, e33–e34. [Google Scholar] [CrossRef] [PubMed]
- Yek, C.; Warner, S.; Wiltz, J.L.; Sun, J.; Adjei, S.; Mancera, A.; Silk, B.J.; Gundlapalli, A.V.; Harris, A.M.; Boehmer, T.K.; et al. Risk factors for severe COVID-19 outcomes among persons aged ≥ 18 years who completed a primary COVID-19 vaccination series—465 health care facilities, United States, December 2020–October 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 19. [Google Scholar] [CrossRef] [PubMed]
- Gautret, P.; Hoang, V.T.; Jimeno, M.T.; Lagier, J.C.; Rossi, P.; Fournier, P.E.; Colson, P.; Raoult, D. The severity of the first 207 infections with the SARS-CoV-2 Omicron BA. 2 variant, in Marseille, France, December 2021–February 2022. J. Med. Virol. 2022, 94, 3494–3497. [Google Scholar] [CrossRef] [PubMed]
- Modes, M.E.; Directo, M.P.; Melgar, M.; Johnson, L.R.; Yang, H.; Chaudhary, P.; Bartolini, S.; Kho, N.; Noble, P.W.; Isonaka, S.; et al. Clinical characteristics and outcomes among adults hospitalized with laboratory-confirmed SARS-CoV-2 infection during periods of B. 1.617. 2 (Delta) and B. 1.1. 529 (Omicron) variant predominance—One hospital, California, July 15–September 23, 2021, and December 21, 2021–January 27, 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 217. [Google Scholar]
- Sheikh, A.; Kerr, S.; Woolhouse, M.; McMenamin, J.; Robertson, C.; Simpson, C.R.; Millington, T.; Shi, T.; Agrawal, U.; Hameed, S.S.; et al. Severity of omicron variant of concern and effectiveness of vaccine boosters against symptomatic disease in Scotland (EAVE II): A national cohort study with nested test-negative design. Lancet Infect. Dis. 2022, 22, 959–966. [Google Scholar] [CrossRef]
- Bager, P.; Wohlfahrt, J.; Bhatt, S.; Stegger, M.; Legarth, R.; Møller, C.H.; Skov, R.L.; Valentiner-Branth, P.; Voldstedlund, M.; Fischer, T.K.; et al. Risk of hospitalisation associated with infection with SARS-CoV-2 omicron variant versus delta variant in Denmark: An observational cohort study. Lancet Infect. Dis. 2022, 21, 1507–1517. [Google Scholar] [CrossRef]
- Butt, A.A.; Dargham, S.R.; Tang, P.; Chemaitelly, H.; Hasan, M.R.; Coyle, P.V.; Kaleeckal, A.H.; Latif, A.N.; Loka, S.; Shaik, R.M.; et al. COVID-19 disease severity in persons infected with the Omicron variant compared with the Delta variant in Qatar. J. Glob. Health 2022, 12, 05032. [Google Scholar] [CrossRef]
- Ministry of Health (Brazil). Open DataSUS. SARS 2021 e 2022—Severe Acute Respiratory Syndrome Database. 2022. Available online: https://opendatasus.saude.gov.br/dataset/srag-2021-e-2022 (accessed on 24 June 2022).
- Ranzani, O.T.; Bastos, L.S.; Gelli, J.G.M.; Marchesi, J.F.; Baião, F.; Hamacher, S.; Bozza, F.A. Characterisation of the first 250,000 hospital admissions for COVID-19 in Brazil: A retrospective analysis of nationwide data. Lancet Respir. Med. 2021, 9, 407–418. [Google Scholar] [CrossRef]
- Oliveira, E.A.; Colosimo, E.A.; e Silva, A.C.S.; Mak, R.H.; Martelli, D.B.; Silva, L.R.; Martelli-Júnior, H.; Oliveira, M.C.L. Clinical characteristics and risk factors for death among hospitalised children and adolescents with COVID-19 in Brazil: An analysis of a nationwide database. Lancet Child Adolesc. Health 2021, 5, 559–568. [Google Scholar] [CrossRef]
- Marra, V.; Quartin, M. A Bayesian estimate of the early COVID-19 infection fatality ratio in Brazil based on a random seroprevalence survey. Int. J. Infect. Dis. 2021, 111, 190–195. [Google Scholar] [CrossRef]
- Gomez, J.M.D.; Du-Fay-de Lavallaz, J.M.; Fugar, S.; Sarau, A.; Simmons, J.A.; Clark, B.; Sanghani, R.M.; Aggarwal, N.T.; Williams, K.A.; Doukky, R.; et al. Sex differences in COVID-19 hospitalization and mortality. J. Women’s Health 2021, 30, 646–653. [Google Scholar] [CrossRef] [PubMed]
- La Vignera, S.; Cannarella, R.; Condorelli, R.A.; Torre, F.; Aversa, A.; Calogero, A.E. Sex-specific SARS-CoV-2 mortality: Among hormone-modulated ACE2 expression, risk of venous thromboembolism and hypovitaminosis D. Int. J. Mol. Sci. 2020, 21, 2948. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health (Brazil). Open DataSUS. SARS 2021 e 2022—National Vaccination Campaign against COVID-19. 2022. Available online: https://opendatasus.saude.gov.br/dataset/covid-19-vacinacao (accessed on 24 July 2022).
- Rahul, K.; Banyal, R.K.; Goswami, P. Analysis and processing aspects of data in big data applications. J. Discret. Math. Sci. Cryptogr. 2020, 23, 385–393. [Google Scholar] [CrossRef]
- Leme, J.V.; Casaca, W.; Colnago, M.; Dias, M.A. Towards Assessing the Electricity Demand in Brazil: Data-Driven Analysis and Ensemble Learning Models. Energies 2020, 13, 1407. [Google Scholar] [CrossRef]
- Thompson, E.J.; Williams, D.M.; Walker, A.J.; Mitchell, R.E.; Niedzwiedz, C.L.; Yang, T.C.; Huggins, C.F.; Kwong, A.S.; Silverwood, R.J.; Di Gessa, G.; et al. Long COVID burden and risk factors in 10 UK longitudinal studies and electronic health records. Nat. Commun. 2022, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Norton, E.C.; Dowd, B.E.; Maciejewski, M.L. Odds ratios—Current best practice and use. JAMA 2018, 320, 84–85. [Google Scholar] [CrossRef]
- Le, C.T.; Eberly, L.E. Introductory Biostatistics; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Seabold, S.; Perktold, J. Statsmodels: Econometric and statistical modeling with python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; Volume 57, pp. 10–25080. [Google Scholar]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; John Wiley and Sons: Hoboken, NJ, USA, 2000. [Google Scholar]
- Nafee, T.; Gibson, C.M.; Travis, R.; Yee, M.K.; Kerneis, M.; Chi, G.; AlKhalfan, F.; Hernandez, A.F.; Hull, R.D.; Cohen, A.T.; et al. Machine learning to predict venous thrombosis in acutely ill medical patients. Res. Pract. Thromb. Haemost. 2020, 4, 230–237. [Google Scholar] [CrossRef]
- Nieto-Codesido, I.; Calvo-Alvarez, U.; Diego, C.; Hammouri, Z.; Mallah, N.; Ginzo-Villamayor, M.J.; Salgado, F.J.; Carreira, J.M.; Rábade, C.; Barbeito, G.; et al. Risk factors of mortality in hospitalized patients with COVID-19 applying a machine learning algorithm. Open Respir. Arch. 2022, 4, 100162. [Google Scholar] [CrossRef]
- Soto, A.; Quiñones, D.; Azañero, J.; Chumpitaz, R.; Claros, J.; Salazar, L.; Rosales, O.; Nuñez, L.; Roca, D.; Alcantara, A. Mortality and associated risk factors in patients hospitalized due to COVID-19 in a Peruvian reference hospital. PLoS ONE 2022, 17, e0264789. [Google Scholar] [CrossRef]
- Liu, W.; Yang, C.; Liao, Y.G.; Wan, F.; Lin, L.; Huang, X.; Zhang, B.H.; Yuan, Y.; Zhang, P.; Zhang, X.J.; et al. Risk factors for COVID-19 progression and mortality in hospitalized patients without pre-existing comorbidities. J. Infect. Public Health 2022, 15, 13–20. [Google Scholar] [PubMed]
- Malafaia, G. Implicações da imunossenescência na vacinação de idosos. Braz. J. Geriatr. Gerontol. 2008, 11, 433–441. [Google Scholar] [CrossRef]
- Elghazaly, S.; El Sood, H.A.; Samy, S.; AbdelFatah, M.; Hassany, M.; Khader, Y.; Afifi, S.; Eid, A. The Impact of Comorbidities on COVID-19 Severity and Mortality in Egypt. Iproceedings 2022, 8, e36576. [Google Scholar] [CrossRef]
- Escobedo-de la Peña, J.; Rascón-Pacheco, R.A.; de Jesús Ascencio-Montiel, I.; González-Figueroa, E.; Fernández-Gárate, J.E.; Medina-Gómez, O.S.; Borja-Bustamante, P.; Santillán-Oropeza, J.A.; Borja-Aburto, V.H. Hypertension, diabetes and obesity, major risk factors for death in patients with COVID-19 in Mexico. Arch. Med. Res. 2021, 52, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Salinas-Aguirre, J.; Sánchez-García, C.; Rodríguez-Sanchez, R.; Rodríguez-Muñoz, L.; Díaz-Castaño, A.; Bernal-Gómez, R. Clinical characteristics and comorbidities associated with mortality in patients with COVID-19 in Coahuila (Mexico). Rev. Clínica Española (Engl. Ed.) 2022, 222, 288–292. [Google Scholar] [CrossRef]
- Çınar, F.; Ekinci, G. Investigation of the effect of comorbidity on mortality in patients with covid-19: A systematic review and meta-analysis. Biointerface Res. Appl. Chem. 2022, 12, 5579–5590. [Google Scholar]
- Biswas, M.; Rahaman, S.; Biswas, T.K.; Haque, Z.; Ibrahim, B. Association of sex, age, and comorbidities with mortality in COVID-19 patients: A systematic review and meta-analysis. Intervirology 2021, 64, 36–47. [Google Scholar] [CrossRef]
- Siddiqi, Z.; Fatima, J.; Bhatt, D.; Shukla, V.; Malik, M.; Ashfaq, A.; Masakputra, V.; Barbhuyan, A. Prevalence of Comorbidities in Survivors and Non-Survivors of Severe COVID-19 at a Dedicated COVID Care Centre. J. Assoc. Physicians India 2022, 70, 11–12. [Google Scholar]
- Louie, J.K.; Acosta, M.; Samuel, M.C.; Schechter, R.; Vugia, D.J.; Harriman, K.; Matyas, B.T. A novel risk factor for a novel virus: Obesity and 2009 pandemic influenza A (H1N1). Clin. Infect. Dis. 2011, 52, 301–312. [Google Scholar] [CrossRef]
- Dietz, W.; Santos-Burgoa, C. Obesity and its implications for COVID-19 mortality. Obesity 2020, 28, 1005. [Google Scholar] [CrossRef]
- Du, Y.; Zhou, N.; Zha, W.; Lv, Y. Hypertension is a clinically important risk factor for critical illness and mortality in COVID-19: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Swamy, S.; Koch, C.A.; Hannah-Shmouni, F.; Schiffrin, E.L.; Klubo-Gwiezdzinska, J.; Gubbi, S. Hypertension and COVID-19: Updates from the era of vaccines and variants. J. Clin. Transl. Endocrinol. 2022, 27, 100285. [Google Scholar] [CrossRef] [PubMed]
- de Jesus, M.A.S.; Hojo-Souza, N.S.; de Moraes, T.R.; Guidoni, D.L.; Souza, F.S.H. Profile of Brazilian inpatients with COVID-19 vaccine breakthrough infection and risk factors for unfavorable outcome. Pan Am. J. Public Health 2022, 46. [Google Scholar] [CrossRef] [PubMed]
- Tazerji, S.S.; Shahabinejad, F.; Tokasi, M.; Rad, M.A.; Khan, M.S.; Safdar, M.; Filipiak, K.J.; Szarpak, L.; Dzieciatkowski, T.; Jurgiel, J.; et al. Global data analysis and risk factors associated with morbidity and mortality of COVID-19. Gene Rep. 2022, 26, 101505. [Google Scholar] [CrossRef] [PubMed]
- Collie, S.; Champion, J.; Moultrie, H.; Bekker, L.G.; Gray, G. Effectiveness of BNT162b2 vaccine against omicron variant in South Africa. N. Engl. J. Med. 2022, 386, 494–496. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Huang, L.; Ye, G.; Geng, Q.; Ikeogu, N.; Harris, M.; Dileepan, G.; Burrack, K.; Du, L.; Frosch, A.; et al. Vaccine booster efficiently inhibits entry of SARS-CoV-2 omicron variant. Cell. Mol. Immunol. 2022, 19, 445–446. [Google Scholar] [CrossRef]
- Smid, M.; Berec, L.; Majek, O.; Pavlik, T.; Jarkovsky, J.; Pribylova, L.; Weiner, J.; Barusova, T.; Trnka, J. Protection by vaccines and previous infection against the Omicron variant of SARS-CoV-2. J. Infect. Dis. 2022, 226, 1385–1390. [Google Scholar] [CrossRef]
- Buchan, S.A.; Chung, H.; Brown, K.A.; Austin, P.C.; Fell, D.B.; Gubbay, J.B.; Nasreen, S.; Schwartz, K.L.; Sundaram, M.E.; Tadrous, M.; et al. Estimated Effectiveness of COVID-19 Vaccines Against Omicron or Delta Symptomatic Infection and Severe Outcomes. JAMA Netw. Open 2022, 5, e2232760. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. Covid-19 vaccine effectiveness against the Omicron (B. 1.1. 529) variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Brasen, C.L.; Christensen, H.; Olsen, D.A.; Kahns, S.; Andersen, R.F.; Madsen, J.B.; Lassen, A.; Kierkegaard, H.; Jensen, A.; Sydenham, T.V.; et al. Daily monitoring of viral load measured as SARS-CoV-2 antigen and RNA in blood, IL-6, CRP and complement C3d predicts outcome in patients hospitalized with COVID-19. Clin. Chem. Lab. Med. (CCLM) 2021, 59, 1988–1997. [Google Scholar] [CrossRef]
- Lo, T.; Usman, H.; Sikdar, K.C.; Strong, D.; James, S.; Ross, J.; Saxinger, L.M. Risk factors for COVID-19 hospitalization or death during the first Omicron surge in adults: A large population-based case-control study. medRxiv 2022. [Google Scholar] [CrossRef]
- Jassat, W.; Karim, S.A.; Ozougwu, L.; Welch, R.; Mudara, C.; Masha, M.; Rousseau, P.; Wolmarans, M.; Selikow, A.; Govender, N.; et al. Trends in cases, hospitalisation and mortality related to the Omicron BA. 4/BA. 5 sub-variants in South Africa. medRxiv 2022. [Google Scholar] [CrossRef]
- Nafilyan, V.; Ward, I.L.; Robertson, C.; Sheikh, A. Evaluation of risk factors for postbooster Omicron COVID-19 deaths in England. JAMA Netw. Open 2022, 5, e2233446. [Google Scholar] [CrossRef] [PubMed]
- Brazil Civil Registry Office. Brazil Civil Registry Platform. 2022. Available online: https://transparencia.registrocivil.org.br/especial-covid (accessed on 2 October 2022).
- Baqui, P.; Marra, V.; Alaa, A.M.; Bica, I.; Ercole, A.; van Der Schaar, M. Comparing COVID-19 risk factors in Brazil using machine learning: The importance of socioeconomic, demographic and structural factors. Sci. Rep. 2021, 11, 15591. [Google Scholar] [CrossRef]
- Amaral, F.; Casaca, W.; Oishi, C.M.; Cuminato, J.A. Towards Providing Effective Data-Driven Responses to Predict the COVID-19 in São Paulo and Brazil. Sensors 2021, 21, 540. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | COVID-19 Hospitalizations | COVID-19 Deaths | Lethality | ||
|---|---|---|---|---|---|
| ( = 50,896) | ( = 17,640) | 0.35 | |||
| Sex | |||||
| Male | 26,388 | 51.85% | 9713 | 55.06% | 0.37 |
| Female | 24,508 | 48.15% | 7927 | 44.94% | 0.32 |
| Age, years | |||||
| Mean age ± SD | 68.71 ± 18.14 | 74.29 ± 15.23 | - | ||
| 18–39 | 4562 | 8.96% | 577 | 3.27% | 0.13 |
| 40–59 | 8999 | 17.68% | 2206 | 12.51% | 0.25 |
| 60–79 | 20,971 | 41.20% | 7326 | 41.53% | 0.35 |
| ≥80 | 16,364 | 32.15% | 7531 | 42.69% | 0.46 |
| Number of comorbidities | |||||
| 0 | 21,009 | 41.28% | 6193 | 35.11% | 0.29 |
| 1 | 16,721 | 32.85% | 6010 | 34.07% | 0.36 |
| 2 | 10,055 | 19.76% | 4013 | 22.75% | 0.40 |
| 3 | 2694 | 5.29% | 1222 | 6.93% | 0.45 |
| ≥4 | 417 | 0.82% | 202 | 1.14% | 0.48 |
| Vaccine doses | |||||
| 0–2 doses | 40,657 | 79.88% | 13,921 | 78.92% | 0.34 |
| ≥3 doses | 10,239 | 20.12% | 3,719 | 21.08% | 0.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colnago, M.; Benvenuto, G.A.; Casaca, W.; Negri, R.G.; Fernandes, E.G.; Cuminato, J.A. Risk Factors Associated with Mortality in Hospitalized Patients with COVID-19 during the Omicron Wave in Brazil. Bioengineering 2022, 9, 584. https://doi.org/10.3390/bioengineering9100584
Colnago M, Benvenuto GA, Casaca W, Negri RG, Fernandes EG, Cuminato JA. Risk Factors Associated with Mortality in Hospitalized Patients with COVID-19 during the Omicron Wave in Brazil. Bioengineering. 2022; 9(10):584. https://doi.org/10.3390/bioengineering9100584
Chicago/Turabian StyleColnago, Marilaine, Giovana A. Benvenuto, Wallace Casaca, Rogério G. Negri, Eder G. Fernandes, and José A. Cuminato. 2022. "Risk Factors Associated with Mortality in Hospitalized Patients with COVID-19 during the Omicron Wave in Brazil" Bioengineering 9, no. 10: 584. https://doi.org/10.3390/bioengineering9100584
APA StyleColnago, M., Benvenuto, G. A., Casaca, W., Negri, R. G., Fernandes, E. G., & Cuminato, J. A. (2022). Risk Factors Associated with Mortality in Hospitalized Patients with COVID-19 during the Omicron Wave in Brazil. Bioengineering, 9(10), 584. https://doi.org/10.3390/bioengineering9100584