The Treatment of Acute Diaphyseal Long-bones Fractures with Orthobiologics and Pharmacological Interventions for Bone Healing Enhancement: A Systematic Review of Clinical Evidence

 ,
,  ,
,
Abstract
1. Introduction
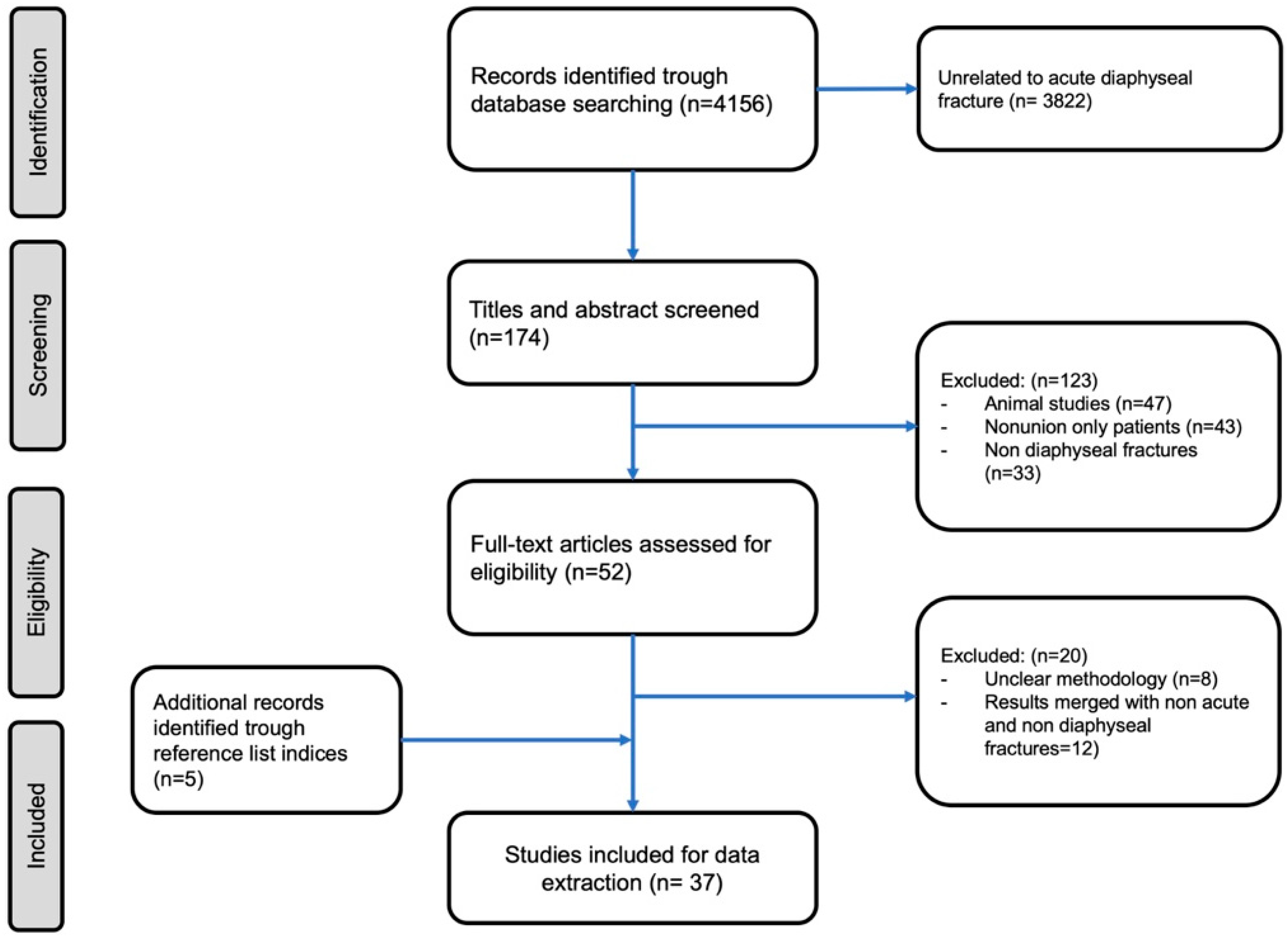
2. Materials and Methods
3. Results
3.1. Autologous Bone grafting (Autograft)
3.2. Allogenic Bone grafting (Allograft)
3.3. Bone Substitutes
3.4. Growth Factors and Peptides
3.5. Cell Therapies
3.6. Systemic Pharmacological Therapy
3.6.1. Bisphosphonates
3.6.2. Denosumab
3.6.3. Strontium Ranelate
3.6.4. Parathormone Analogues
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mills, L.A.; Aitken, S.A.; Simpson, A.H.R.W. The risk of non-union per fracture: Current myths and revised figures from a population of over 4 million adults. Acta Orthop. 2017, 88, 434–439. [Google Scholar] [CrossRef]
- Nandra, R.; Grover, L.; Porter, K. Fracture non-union epidemiology and treatment. Trauma 2016, 18, 3–11. [Google Scholar] [CrossRef]
- Massari, L.; Benazzo, F.; Falez, F.; Cadossi, R.; Perugia, D.; Pietrogrande, L.; Aloj, D.C.; Capone, A.; D’Arienzo, M.; Cadossi, M.; et al. Can Clinical and Surgical Parameters Be Combined to Predict How Long It Will Take a Tibia Fracture to Heal? A Prospective Multicentre Observational Study: The FRACTING Study. BioMed Res. Int. 2018, 2018, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Marongiu, G.; Dolci, A.; Verona, M.; Capone, A. The biology and treatment of acute long-bones diaphyseal fractures: Overview of the current options for bone healing enhancement. Bone Rep. 2020, 12, 100249. [Google Scholar] [CrossRef] [PubMed]
- Calcei, J.G.; Rodeo, S.A. Orthobiologics for Bone Healing. Clin. Sports Med. 2019, 38, 79–95. [Google Scholar] [CrossRef]
- Miska, M.; Findeisen, S.; Tanner, M.; Biglari, B.; Studier-Fischer, S.; Grützner, P.A.; Moghaddam, A.; Schmidmaier, G. Treatment of nonunions in fractures of the humeral shaft according to the Diamond Concept. Bone Joint J. 2016, 98, 81–87. [Google Scholar] [CrossRef]
- Andrzejowski, P.; Giannoudis, P.V. The ‘diamond concept’ for long bone non-union management. J. Orthop. Traumatol. 2019, 20, 21. [Google Scholar] [CrossRef]
- Capone, A.; Orgiano, F.; Pianu, F.; Planta, M. Orthopaedic surgeons’ strategies in pharmacological treatment of fragility fractures. Clin. Cases Miner. Bone Metab. 2014, 11, 105–109. [Google Scholar] [CrossRef]
- Brandi, M.L. Drugs for bone healing. Expert Opin. Investig. Drugs. 2012, 21, 1169–1176. [Google Scholar] [CrossRef]
- Marongiu, G.; Mastio, M.; Capone, A. Current options to surgical treatment in osteoporotic fractures. Aging Clin. Exp. Res. 2013, 25, 15–17. [Google Scholar] [CrossRef]
- Marongiu, G.; Capone, A. Atypical periprosthetic acetabular fracture in long-term alendronate therapy. Clin. Cases Miner. Bone Metab. 2016, 13, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Capone, A.; Peri, M.; Mastio, M. Surgical treatment of acetabular fractures in the elderly: A systematic review of the results. EFORT Open Rev. 2017, 2, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Kashayi-Chowdojirao, S.; Vallurupalli, A.; Chilakamarri, V.K.; Patnala, C.; Chodavarapu, L.M.; Kancherla, N.R.; Syed, A.H.K. Role of autologous non-vascularised intramedullary fibular strut graft in humeral shaft nonunions following failed plating. J. Clin. Orthop. Trauma 2017, 8, S21–S30. [Google Scholar] [CrossRef] [PubMed]
- Azi, M.L.; Aprato, A.; Santi, I.; Kfuri, M.; Masse, A.; Joeris, A. Autologous bone graft in the treatment of post-traumatic bone defects: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2016, 17, 465. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.L.; Bucholz, R.W.; Bosse, M.J.; Mirza, S.K.; Lyon, T.R.; Webb, L.X.; Pollak, A.N.; Golden, J.D.; Valentin-Opran, A. Recombinant Human BMP-2 and Allograft Compared with Autogenous Bone Graft for Reconstruction of Diaphyseal Tibial Fractures with Cortical Defects. J. Bone Joint Surg. 2006, 88, 1431–1441. [Google Scholar] [CrossRef]
- Major Extremity Trauma Research Consortium. A Randomized Controlled Trial Comparing rhBMP-2/Absorbable Collagen Sponge Versus Autograft for the Treatment of Tibia Fractures With Critical Size Defects. J. Orthop. Trauma 2019, 33, 384–391. [Google Scholar] [CrossRef]
- Zhen, P.; Liu, X.-Y.; Lu, H.; Li, X.-S. Fixation and reconstruction of severe tibial shaft fractures with vascularized fibular grafting. Arch. Orthop. Trauma Surg. 2011, 131, 93–99. [Google Scholar] [CrossRef]
- Sen, M.K.; Miclau, T. Autologous iliac crest bone graft: Should it still be the gold standard for treating nonunions? Injury 2007, 38, S75–S80. [Google Scholar] [CrossRef]
- Cox, G.; Jones, E.; McGonagle, D.; Giannoudis, P.V. Reamer-irrigator-aspirator indications and clinical results: A systematic review. Int. Orthop. 2011, 35, 951–956. [Google Scholar] [CrossRef]
- Streubel, P.N.; Desai, P.; Suk, M. Comparison of RIA and conventional reamed nailing for treatment of femur shaft fractures. Injury 2010, 41, S51–S56. [Google Scholar] [CrossRef]
- Cobbs, K.F. RIA use in a community orthopedic trauma practice: Applying technology, respecting biology. Injury 2010, 41, S78–S84. [Google Scholar] [CrossRef]
- McCall, T.A.; Brokaw, D.S.; Jelen, B.A.; Scheid, D.K.; Scharfenberger, A.V.; Maar, D.C.; Green, J.M.; Shipps, M.R.; Stone, M.B.; Musapatika, D.; et al. Treatment of Large Segmental Bone Defects with Reamer-Irrigator-Aspirator Bone Graft: Technique and Case Series. Orthop. Clin. N. Am. 2010, 41, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Belthur, M.V.; Conway, J.D.; Jindal, G.; Ranade, A.; Herzenberg, J.E. Bone Graft Harvest Using a New Intramedullary System. Clin. Orthop. Relat. Res. 2008, 466, 2973–2980. [Google Scholar] [CrossRef] [PubMed]
- Oryan, A.; Alidadi, S.; Moshiri, A.; Maffulli, N. Bone regenerative medicine: Classic options, novel strategies, and future directions. J. Orthop. Surg. Res. 2014, 9, 18. [Google Scholar] [CrossRef]
- Gogus, A.; Ozturk, C.; Tezer, M.; Çamurdan, K.; Hamzaoglu, A. “Sandwich technique” in the surgical treatment of primary complex fractures of the femur and humerus. Int. Orthop. 2007, 31, 87–92. [Google Scholar] [CrossRef][Green Version]
- Wu, H.; Yan, S.; Wu, L.; He, R.; Wang, X.; Dai, X. Combined use of extensively porous coated femoral components with onlay cortical strut allografts in revision of Vancouver B2 and B3 periprosthetic femoral fractures. Chin. Med. J. 2009, 122, 2612–2615. [Google Scholar]
- Capone, A. Periprosthetic fractures: Epidemiology and current treatment. Clin. Cases Miner. Bone Metab. 2017, 14, 189. [Google Scholar] [CrossRef]
- Tomás Hernández, J.; Holck, K. Periprosthetic femoral fractures: When I use strut grafts and why? Injury 2015, 46, S43–S46. [Google Scholar] [CrossRef]
- Khashan, M.; Amar, E.; Drexler, M.; Chechik, O.; Cohen, Z.; Steinberg, E.L. Superior outcome of strut allograft-augmented plate fixation for the treatment of periprosthetic fractures around a stable femoral stem. Injury 2013, 44, 1556–1560. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Mansukhani, S.A.; Kim, J.-S.; Park, J.-W. Use of Locking Plate and Strut Onlay Allografts for Periprosthetic Fracture Around Well-Fixed Femoral Components. J. Arthroplast. 2017, 32, 166–170. [Google Scholar] [CrossRef]
- Smith, P.J.; Lihou, M.G. Prediction of remission induction in childhood acute myeloid leukemia. Aust. N. Z. J. Med. 1986, 16, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Font-Vizcarra, L.; Fernández-Valencia, J.A.; Gallart, X.; Segur, J.M.; Prat, S.; Riba, J. Cortical Strut Allograft as an Adjunct to Plate Fixation for Periprosthetic Fractures of the Femur. HIP Int. 2010, 20, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.S.; Duncan, C.P.; Berry, D.J.; Lewallen, D.G.; Gross, A.E.; Chandler, H.P. Periprosthetic Femoral Fractures Around Well-Fixed Implants. J. Bone Joint Surg.-Am. Vol. 2002, 84, 945–950. [Google Scholar] [CrossRef]
- Salvi, M.; Caputo, F.; Piu, G.; Sanna, M.; Sanna, C.; Marongiu, G. The loss of extension test (LOE test): A new clinical sign for the anterior cruciate ligament insufficient knee. J. Orthop. Traumatol. 2013, 14, 185–191. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Capone, A.; Bienati, F.; Torchia, S.; Podda, D.; Marongiu, G. Short stem total hip arthroplasty for osteonecrosis of the femoral head in patients 60 years or younger: A 3- to 10-year follow-up study. BMC Musculoskelet. Disord. 2017, 18, 301. [Google Scholar] [CrossRef]
- Li, D.; Hu, Q.; Kang, P.; Yang, J.; Zhou, Z.; Shen, B.; Pei, F. Reconstructed the bone stock after femoral bone loss in Vancouver B3 periprosthetic femoral fractures using cortical strut allograft and impacted cancellous allograft. Int. Orthop. 2018, 42, 2787–2795. [Google Scholar] [CrossRef]
- Moore, R.E.; Baldwin, K.; Austin, M.S.; Mehta, S. A Systematic Review of Open Reduction and Internal Fixation of Periprosthetic Femur Fractures With or Without Allograft Strut, Cerclage, and Locked Plates. J. Arthroplast. 2014, 29, 872–876. [Google Scholar] [CrossRef]
- Urist, M.R.; Dowell, T.A.; Hay, P.H.; Strates, B.S. Inductive substrates for bone formation. Clin. Orthop. Relat. Res. 1968, 59, 59–96. [Google Scholar] [CrossRef]
- Boyce, T.; Edwards, J.; Scarborough, N. Allograft Bone. Orthop. Clin. N. Am. 1999, 30, 571–581. [Google Scholar] [CrossRef]
- Verona, M.; Marongiu, G.; Cardoni, G.; Piras, N.; Frigau, L.; Capone, A. Arthroscopically assisted reduction and internal fixation (ARIF) versus open reduction and internal fixation (ORIF) for lateral tibial plateau fractures: A comparative retrospective study. J. Orthop. Surg. Res. 2019, 14, 155. [Google Scholar] [CrossRef]
- Lindsey, R.W.; Sadasivian, K.K.; Wood, G.W.; Stubbs, H.A.; Block, J.E. Grafting Long Bone Fractures With Demineralized Bone Matrix Putty Enriched With Bone Marrow: Pilot Findings. Orthopedics 2006, 29, 939–941. [Google Scholar] [CrossRef] [PubMed]
- Kulachote, N.; Sa-ngasoongsong, P.; Sirisreetreerux, N.; Chanplakorn, P.; Fuangfa, P.; Suphachatwong, C.; Wajanavisit, W. Demineralized Bone Matrix Add-On for Acceleration of Bone Healing in Atypical Subtrochanteric Femoral Fracture: A Consecutive Case-Control Study. BioMed Res. Int. 2016, 2016, 4061539. [Google Scholar] [CrossRef] [PubMed]
- Van der Stok, J.; Hartholt, K.A.; Schoenmakers, D.A.L.; Arts, J.J.C. The available evidence on demineralised bone matrix in trauma and orthopaedic surgery. Bone Joint Res. 2017, 6, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Doria, C.; Balsano, M.; Spiga, M.; Mosele, G.R.; Puddu, L.; Caggiari, G. Tibioplasty, a new technique in the management of tibial plateau fracture: A multicentric experience review. J. Orthop. 2017, 14, 176–181. [Google Scholar] [CrossRef]
- Ayoub, M.A.; El-Rosasy, M.A. Hybrid grafting of post-traumatic bone defects using β-tricalcium phosphate and demineralized bone matrix. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 663–670. [Google Scholar] [CrossRef]
- Chapman, M.W.; Bucholz, R.; Cornell, C. Treatment of Acute Fractures with a Collagen-Calcium Phosphate Graft Material. A Randomized Clinical Trial. J. Bone Joint Surg. 1997, 79, 495–502. [Google Scholar] [CrossRef]
- Civinini, R.; Capone, A.; Carulli, C.; Matassi, F.; Nistri, L.; Innocenti, M. The kinetics of remodeling of a calcium sulfate/calcium phosphate bioceramic. J. Mater. Sci. Mater. Med. 2017, 28, 137. [Google Scholar] [CrossRef]
- Sun, J.; Hao, S.; Sun, R.; Yang, Y. Treatment of high-energy tibial shaft fractures with internal fixation and early prophylactic NovaBone grafting. Orthop. Surg. 2009, 1, 17–21. [Google Scholar] [CrossRef]
- Cho, T.-J.; Gerstenfeld, L.C.; Einhorn, T.A. Differential Temporal Expression of Members of the Transforming Growth Factor β Superfamily During Murine Fracture Healing. J. Bone Miner. Res. 2002, 17, 513–520. [Google Scholar] [CrossRef]
- Dimitriou, R.; Dahabreh, Z.; Katsoulis, E.; Matthews, S.J.; Branfoot, T.; Giannoudis, P.V. Application of recombinant BMP-7 on persistent upper and lower limb non-unions. Injury 2005, 36, S51–S59. [Google Scholar] [CrossRef]
- Calori, G.M.; Colombo, M.; Bucci, M.; Mazza, E.L.; Fadigati, P.; Mazzola, S. Clinical effectiveness of Osigraft in long-bones non-unions. Injury 2015, 46, S55–S64. [Google Scholar] [CrossRef]
- Yu, Y.Y.; Lieu, S.; Lu, C.; Colnot, C. Bone morphogenetic protein 2 stimulates endochondral ossification by regulating periosteal cell fate during bone repair. Bone 2010, 47, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, H.; Oka, H.; Jingushi, S.; Izumi, T.; Fukunaga, M.; Sato, K.; Matsushita, T.; Nakamura, K. A local application of recombinant human fibroblast growth factor 2 for tibial shaft fractures: A randomized, placebo-controlled trial. J. Bone Miner. Res. 2010, 25, 2735–2743. [Google Scholar] [CrossRef] [PubMed]
- Swiontkowski, M.F.; Aro, H.T.; Donell, S.; Esterhai, J.L.; Goulet, J.; Jones, A.; Kregor, P.J.; Nordsletten, L.; Paiement, G.; Patel, A. Recombinant Human Bone Morphogenetic Protein-2 in Open Tibial Fractures. J. Bone Joint Surg. 2006, 88, 1258–1265. [Google Scholar] [CrossRef] [PubMed]
- Ristiniemi, J.; Flinkkilä, T.; Hyvönen, P.; Lakovaara, M.; Pakarinen, H.; Jalovaara, P. RhBMP-7 accelerates the healing in distal tibial fractures treated by external fixation. J. Bone Joint Surg. Br. Vol. 2007, 89, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Govender, S.; Csimma, C.; Genant, H.K.; Valentin-Opran, A. Recombinant Human Bone Morphogenetic Protein-2 for Treatment of Open Tibial Fractures. J. Bone Joint Surg.-Am. Vol. 2002, 84, 2123–2134. [Google Scholar] [CrossRef]
- Aro, H.T.; Govender, S.; Patel, A.D.; Hernigou, P.; Perera de Gregorio, A.; Popescu, G.I.; Golden, J.D.; Christensen, J.; Valentin, A. Recombinant Human Bone Morphogenetic Protein-2: A Randomized Trial in Open Tibial Fractures Treated with Reamed Nail Fixation. J. Bone Joint Surg.-Am. Vol. 2011, 93, 801–808. [Google Scholar] [CrossRef]
- Lyon, T.; Scheele, W.; Bhandari, M.; Koval, K.J. Efficacy and Safety of Recombinant Human Bone Matrix for Closed Tibial Diaphyseal Fracture. J. Bone Joint Surg. Am. 2013, 95, 2088–2097. [Google Scholar] [CrossRef]
- Calori, G.M.; Tagliabue, L.; Gala, L.; D’Imporzano, M.; Peretti, G.; Albisetti, W. Application of rhBMP-7 and platelet-rich plasma in the treatment of long bone non-unions. Injury 2008, 39, 1391–1402. [Google Scholar] [CrossRef]
- Kanakaris, N.K.; Calori, G.M.; Verdonk, R.; Burssens, P.; De Biase, P.; Capanna, R.; Vangosa, L.B.; Cherubino, P.; Baldo, F.; Ristiniemi, J. Application of BMP-7 to tibial non-unions: A 3-year multicenter experience. Injury 2008, 39, S83–S90. [Google Scholar] [CrossRef]
- Klenke, F.M.; Siebenrock, K.A. Osteology in Orthopedics—Bone Repair, Bone Grafts and Bone Graft Substitutes. In Reference Module in Biomedical Sciences; Elsevier: Amsterdam, The Netherlands, 2016; pp. 1–15. [Google Scholar]
- Barcak, E.A.; Beebe, M.J. Bone Morphogenetic Protein. Orthop. Clin. N. Am. 2017, 48, 301–309. [Google Scholar] [CrossRef]
- Guo, W.; Gorlick, R.; Ladanyi, M.; Meyers, P.A.; Huvos, A.G.; Bertino, J.R.; Healey, J.H. Expression of bone morphogenetic proteins and receptors in sarcomas. Clin. Orthop. Relat. Res. 1999, 365, 175–183. [Google Scholar] [CrossRef]
- Kim, P.H.; Leopold, S.S. Gustilo-Anderson Classification. Clin. Orthop. Relat. Res. 2012, 470, 3270–3274. [Google Scholar] [CrossRef]
- Hernigou, P.; Mathieu, G.; Poignard, A.; Manicom, O.; Beaujean, F.; Rouard, H. Percutaneous Autologous Bone-Marrow Grafting for Nonunions: Surgical Technique. JBJS Essent. Surg. Tech. 2006, 88, 322–327. [Google Scholar] [CrossRef]
- Liebergall, M.; Schroeder, J.; Mosheiff, R.; Gazit, Z.; Yoram, Z.; Rasooly, L.; Daskal, A.; Khoury, A.; Weil, Y.; Beyth, S. Stem Cell–based Therapy for Prevention of Delayed Fracture Union: A Randomized and Prospective Preliminary Study. Mol. Ther. 2013, 21, 1631–1638. [Google Scholar] [CrossRef]
- Schottel, P.C.; Warner, S.J. Role of Bone Marrow Aspirate in Orthopedic Trauma. Orthop. Clin. N. Am. 2017, 48, 311–321. [Google Scholar] [CrossRef]
- Jäger, M.; Herten, M.; Fochtmann, U.; Fischer, J.; Hernigou, P.; Zilkens, C.; Hendrich, C.; Krauspe, R. Bridging the gap: Bone marrow aspiration concentrate reduces autologous bone grafting in osseous defects. J. Orthop. Res. 2011, 29, 173–180. [Google Scholar] [CrossRef]
- Le Nail, L.-R.; Stanovici, J.; Fournier, J.; Splingard, M.; Domenech, J.; Rosset, P. Percutaneous grafting with bone marrow autologous concentrate for open tibia fractures: Analysis of forty three cases and literature review. Int. Orthop. 2014, 38, 1845–1853. [Google Scholar] [CrossRef]
- Desai, P.; Hasan, S.M.; Zambrana, L.; Hegde, V.; Saleh, A.; Cohn, M.R.; Lane, J.M. Bone Mesenchymal Stem Cells with Growth Factors Successfully Treat Nonunions and Delayed Unions. HSS J. 2015, 11, 104–111. [Google Scholar] [CrossRef]
- Goel, A.; Sangwan, S.S.; Siwach, R.C.; Ali, A.M. Percutaneous bone marrow grafting for the treatment of tibial non-union. Injury 2005, 36, 203–206. [Google Scholar] [CrossRef]
- Oh, J.H.; Kim, W.; Park, K.U.; Roh, Y.H. Comparison of the Cellular Composition and Cytokine-Release Kinetics of Various Platelet-Rich Plasma Preparations. Am. J. Sports Med. 2015, 43, 3062–3070. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Rohilla, R.; Gawande, J.; Kumar Sehgal, P. To evaluate the role of platelet-rich plasma in healing of acute diaphyseal fractures of the femur. Chin. J. Traumatol. 2017, 20, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, R.; Kumar, V.; Garg, B.; Singh, R.; Jain, V.; Coshic, P.; Chatterjee, K. Role of autologous platelet-rich plasma in treatment of long-bone nonunions: A prospective study. Musculoskelet. Surg. 2015, 99, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Duramaz, A.; Ursavaş, H.T.; Bilgili, M.G.; Bayrak, A.; Bayram, B.; Avkan, M.C. Platelet-rich plasma versus exchange intramedullary nailing in treatment of long bone oligotrophic nonunions. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 131–137. [Google Scholar] [CrossRef]
- Wang, D.; Rodeo, S.A. Platelet-Rich Plasma in Orthopaedic Surgery. JBJS Rev. 2017, 5, e7. [Google Scholar] [CrossRef]
- Tarantino, U.; Capone, A.; Planta, M.; D’Arienzo, M.; Letizia Mauro, G.; Impagliazzo, A.; Formica, A.; Pallotta, F.; Patella, V.; Spinarelli, A.; et al. The incidence of hip, forearm, humeral, ankle, and vertebral fragility fractures in Italy: Results from a 3-year multicenter study. Arthritis Res. Ther. 2010, 12, R226. [Google Scholar] [CrossRef]
- Marongiu, G.; Congia, S.; Verona, M.; Lombardo, M.; Podda, D.; Capone, A. The impact of magnetic resonance imaging in the diagnostic and classification process of osteoporotic vertebral fractures. Injury 2018, 49, S26–S31. [Google Scholar] [CrossRef]
- Cheng, C.; Shoback, D. Mechanisms Underlying Normal Fracture Healing and Risk Factors for Delayed Healing. Curr. Osteoporos. Rep. 2019, 17, 36–47. [Google Scholar] [CrossRef]
- Capone, A.; Podda, D.; Ennas, F.; Iesu, C.; Casciu, L.; Civinini, R. Hyperbaric Oxygen Therapy for Transient Bone Marrow Oedema Syndrome of the Hip. HIP Int. 2011, 21, 211–216. [Google Scholar] [CrossRef]
- Fu, L.; Tang, T.; Hao, Y.; Dai, K. Long-term effects of alendronate on fracture healing and bone remodeling of femoral shaft in ovariectomized rats. Acta Pharmacol. Sin. 2013, 34, 387–392. [Google Scholar] [CrossRef]
- Congia, S.; Palmas, A.; Marongiu, G.; Capone, A. Is antegrade nailing a proper option in 2- and 3-part proximal humeral fractures? Musculoskelet. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Colón-Emeric, C.; Nordsletten, L.; Olson, S.; Major, N.; Boonen, S.; Haentjens, P.; Mesenbrink, P.; Magaziner, J.; Adachi, J.; Lyles, K.W.; et al. Association between timing of zoledronic acid infusion and hip fracture healing. Osteoporos. Int. 2011, 22, 2329–2336. [Google Scholar] [CrossRef] [PubMed]
- Moroni, A.; Faldini, C.; Hoang-Kim, A.; Pegreffi, F.; Giannini, S. Alendronate Improves Screw Fixation in Osteoporotic Bone. J. Bone Joint Surg. 2007, 89, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Hegde, V.; Jo, J.E.; Andreopoulou, P.; Lane, J.M. Effect of osteoporosis medications on fracture healing. Osteoporos. Int. 2016, 27, 861–871. [Google Scholar] [CrossRef] [PubMed]
- Adami, S.; Libanati, C.; Boonen, S.; Cummings, S.R.; Ho, P.-R.; Wang, A.; Siris, E.; Lane, J.M. Denosumab Treatment in Postmenopausal Women with Osteoporosis Does Not Interfere with Fracture-Healing. J. Bone Joint Surg.-Am. Vol. 2012, 94, 2113–2119. [Google Scholar] [CrossRef] [PubMed]
- Marie, P.J.; Ammann, P.; Boivin, G.; Rey, C. Mechanisms of Action and Therapeutic Potential of Strontium in Bone. Calcif. Tissue Int. 2001, 69, 121–129. [Google Scholar] [CrossRef]
- Alegre, D.N.; Ribeiro, C.; Sousa, C.; Correia, J.; Silva, L.; de Almeida, L. Possible benefits of strontium ranelate in complicated long bone fractures. Rheumatol. Int. 2012, 32, 439–443. [Google Scholar] [CrossRef]
- Negri, A.L.; Spivacow, F.R. Healing of subtrochanteric atypical fractures after strontium ranelate treatment. Clin. Cases Min. Bone Metab. 2012, 9, 166–169. [Google Scholar]
- Capone, A.; Franco, E.; Daniele, P. Periprosthetic femoral fractures: Risk factors and current options to treatment. Aging Clin. Exp. Res. 2011, 23, 33–35. [Google Scholar]
- Díez-Pérez, A.; Marin, F.; Eriksen, E.F.; Kendler, D.L.; Krege, J.H.; Delgado-Rodríguez, M. Effects of teriparatide on hip and upper limb fractures in patients with osteoporosis: A systematic review and meta-analysis. Bone 2019, 120, 1–8. [Google Scholar] [CrossRef]
- Nakajima, A.; Shimoji, N.; Shiomi, K.; Shimizu, S.; Moriya, H.; Einhorn, T.A.; Yamazaki, M. Mechanisms for the Enhancement of Fracture Healing in Rats Treated With Intermittent Low-Dose Human Parathyroid Hormone (1-34). J. Bone Min. Res. 2002, 17, 2038–2047. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, T.; Nakajima, A.; Shiomi, K.; Moriya, H.; Einhorn, T.A.; Yamazaki, M. Effects of low-dose, intermittent treatment with recombinant human parathyroid hormone (1–34) on chondrogenesis in a model of experimental fracture healing. Bone 2005, 37, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Ota, M.; Takahata, M.; Shimizu, T.; Momma, D.; Hamano, H.; Hiratsuka, S.; Amizuka, N.; Hasegawa, T.; Iwasaki, N. Optimal administration frequency and dose of teriparatide for acceleration of biomechanical healing of long-bone fracture in a mouse model. J. Bone Min. Metab. 2019, 37, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Aspenberg, P.; Genant, H.K.; Johansson, T.; Nino, A.J.; See, K.; Krohn, K.; García-Hernández, P.A.; Recknor, C.P.; Einhorn, T.; Dalsky, G.P.; et al. Teriparatide for acceleration of fracture repair in humans: A prospective, randomized, double-blind study of 102 postmenopausal women with distal radial fractures. J. Bone Min. Res. 2010, 25, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Peichl, P.; Holzer, L.A.; Maier, R.; Holzer, G. Parathyroid Hormone 1-84 Accelerates Fracture-Healing in Pubic Bones of Elderly Osteoporotic Women. J. Bone Joint Surg.-Am. Vol. 2011, 93, 1583–1587. [Google Scholar] [CrossRef] [PubMed]
- Im, G.-I.; Lee, S.-H. Effect of Teriparatide on Healing of Atypical Femoral Fractures: A Systemic Review. J. Bone Metab. 2015, 22, 183. [Google Scholar] [CrossRef]
- Miyakoshi, N.; Aizawa, T.; Sasaki, S.; Ando, S.; Maekawa, S.; Aonuma, H.; Tsuchie, H.; Sasaki, H.; Kasukawa, Y.; Shimada, Y. Healing of bisphosphonate-associated atypical femoral fractures in patients with osteoporosis: A comparison between treatment with and without teriparatide. J. Bone Miner. Metab. 2015, 33, 553–559. [Google Scholar] [CrossRef]
- Watts, N.B.; Aggers, D.; McCarthy, E.F.; Savage, T.; Martinez, S.; Patterson, R.; Carrithers, E.; Miller, P. Responses to Treatment With Teriparatide in Patients With Atypical Femur Fractures Previously Treated With Bisphosphonates. J. Bone Miner. Res. 2017, 32, 1027–1033. [Google Scholar] [CrossRef]
- Chiang, C.Y.; Zebaze, R.M.D.; Ghasem-Zadeh, A.; Iuliano-Burns, S.; Hardidge, A.; Seeman, E. Teriparatide improves bone quality and healing of atypical femoral fractures associated with bisphosphonate therapy. Bone 2013, 52, 360–365. [Google Scholar] [CrossRef]
- Greenspan, S.L.; Vujevich, K.; Britton, C.; Herradura, A.; Gruen, G.; Tarkin, I.; Siska, P.; Hamlin, B.; Perera, S. Teriparatide for treatment of patients with bisphosphonate-associated atypical fracture of the femur. Osteoporos. Int. 2018, 29, 501–506. [Google Scholar] [CrossRef]
- Shimada, Y.; Ishikawa, T.; Endo, J.; Katsuragi, J.; Kotani, T.; Kiuchi, H.; Kuniyoshi, K.; Ohtori, S. Treatment of Atypical Ulnar Fractures Associated with Long-Term Bisphosphonate Therapy for Osteoporosis: Autogenous Bone Graft with Internal Fixation. Case Rep. Orthop. 2017, 2017, 8602573. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Miyakoshi, N.; Kasukawa, Y.; Sato, T.; Kubota, H.; Sasaki, H.; Mizutani, T.; Shimada, Y. Treatment of Atypical Fracture of the Ulnar Diaphysis by Open Reduction and Internal Fixation with Teriparatide. Case Rep. Orthop. 2019, 2019, 9103412. [Google Scholar] [CrossRef] [PubMed]
- Papaiordanidou, M.; Billot, M.; Varray, A.; Martin, A. Neuromuscular Fatigue Is Not Different between Constant and Variable Frequency Stimulation. PLoS ONE 2014, 9, e84740. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-K.; Kim, J.T.; Kim, K.-C.; Ha, Y.-C.; Koo, K.-H. Conservative Treatment for Minimally Displaced Type B Periprosthetic Femoral Fractures. J. Arthroplast. 2017, 32, 3529–3532. [Google Scholar] [CrossRef] [PubMed]
- Miura, T.; Kijima, H.; Tani, T.; Ebina, T.; Miyakoshi, N.; Shimada, Y. Two Cases of Periprosthetic Atypical Femoral Fractures in Patients on Long-Term Bisphosphonate Treatment. Case Rep. Surg. 2019, 2019, 9845320. [Google Scholar] [CrossRef]
- Tanaka, S.; Fukui, T.; Oe, K.; Matsumoto, T.; Matsushita, T.; Hayashi, S.; Kawamoto, T.; Kuroda, R.; Niikura, T. A Periprosthetic Femoral Fracture with Characteristics of Atypical Femoral Fracture. Case Rep. Orthop. 2019, 2019, 1275369. [Google Scholar] [CrossRef]
- Lee, J.Y.Y.; Soh, T.; Howe TSen Koh, J.S.B.; Kwek, E.B.K.; Chua, D.T.C. Bisphosphonate-associated peri-implant fractures: A new clinical entity? Acta Orthop. 2015, 86, 622–626. [Google Scholar] [CrossRef]
- Niikura, T.; Lee, S.Y.; Sakai, Y.; Kuroda, R.; Kurosaka, M. Rare non-traumatic periprosthetic femoral fracture with features of an atypical femoral fracture: A case report. J. Med. Case Rep. 2015, 9, 103. [Google Scholar] [CrossRef]
- Cross, M.B.; Nam, D.; van der Meulen, M.C.H.; Bostrom, M.P.G. A rare case of a bisphosphonate-induced peri-prosthetic femoral fracture. J. Bone Joint Surg. Br. Vol. 2012, 94, 994–997. [Google Scholar] [CrossRef]
- Ramani, A.; Wagner, R. Periprosthetic Femoral Stress Fracture After Bisphosphonate Treatment Resulting in Nonunion Successfully Treated with Teriparatide. JBJS Case Connect. 2016, 6, e37. [Google Scholar] [CrossRef]
- Curtin, B.M.; Fehring, T.K. Bisphosphonate fractures as a cause of painful total hip arthroplasty. Orthopedics 2011, 34, e939–e944. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Tanaka, C.; Tada, H.; Kanoe, H.; Shirai, T. Radiographic features of teriparatide-induced healing of femoral fractures. Bone Rep. 2015, 3, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, G.; Ferraro, S.; Zitiello, M.; Bonacci, E.; Garro, L.; Surace, M.F.; D’angelo, E.; De, G.M. Shoulder periprosthetic fracture in elderly patient: A minimally invasive osteosynthesis and “off-label” treatment with teriparatide. A case report and literature review. J. Biol. Regul. Homeost. Agents 2019, 33, 57–62. [Google Scholar] [PubMed]


{kind=link}
| Osteogenicity | Osteoconductivity | Osteoinductivity | |
|---|---|---|---|
| Autograft | ++++ | ++++ | ++++ |
| Allograft | - | +++ | + |
| Demineralized Bone Matrix (DBM) | - | ++ | + |
| Calcium phosphate Hydroxyapatite | - | + | - |
| Bioactive glass | - | ++ | - |
| Bone Morphogenetic Proteins (BMPs) | - | - | +++ |
| Platelet rich plasma (PRP) | + | - | ++ |
| Bone marrow aspirate concentrate (BMAC) | +++ | - | ++ |
| Topic | n. of Patients Included |
|---|---|
| Bone graft (15–17,25,26,29–33) | 205 |
| Bone substitutes (41,42,45,46,48) | 331 |
| Growth factors (53,55–58) | 615 |
| Cell therapies (66,69,73) | 69 |
| Pharmacological therapy (97)**(98–105,107–114) | 110 |
| Type | Subtype | Clinical Evidence | Quality of Evidence |
|---|---|---|---|
| Autologous bone graft (ABG) | Cortical graft | Both vascularized and non-vascularized cortical graft showed effectiveness in tibia and humeral shaft fractures when associated to Open Reduction and Internal Fixation (ORIF). Vascularized ABG represent the treatment of choice for open tibia fractures with bone defect. High incidence of donor-site morbidities (i.e., iliac crest) | Strong |
| RIA | Evidence suggest no effect in improvement of healing in acute fracture. | Moderate | |
| Allogenic bone graft (Allograft) | Cortical graft | Cortical allograft showed effectiveness in complex femoral and humeral shaft fractures when associated to ORIF. Represent a reliably solution in the treatment of periprosthetic femoral fractures. High rates of infection | Moderate |
| Bone substitutes | Demineralized bone matrix (DBM) | Case series support the use in acute fracture of humerus, tibia and femur and atypical femoral fractures | Weak |
| Calcium phosphate, β-tricalcium phosphate | Unclear benefit on fracture healing. Useful as scaffolds combined to DBM, growth factors and cell therapies | Weak | |
| Calcium phosphate ceramics | 1 RCT showed that ceramics provide union rates similar to cortical autograft in acute long bones fractures. Lower rates of infection compared to autografts. In 1 RCT, Bioglass showed better healing rates for high-energy tibial shaft fractures, compared to the control group. | Moderate |
| Type | Subtype | Clinical Evidence | Quality of Evidence |
|---|---|---|---|
| Growth factors | BMP-2, BMP-7 | rhBMP-2 for treating open tibia fractures, (a Gustilo type 3) The rhBMP-7 is limited to treating tibia shaft non-unions. Potential local (heterotopic ossification) and systemic complications (carcinogenesis, renal and hepatic failure) | Strong |
| rhFGF | Case series suggested benefit in tibial shaft fractures. | Weak | |
| Cell therapies | Autologous bone marrow aspirate concentrate (BMAC) | Case series reported unclear benefit in bone healing of acute open tibia fracture. | Weak |
| Platelet rich plasma (PRP) | Conflicting evidence. 1 RCT showed shorter healing time in tibial fractures + ORIF. 1 RCT showed no difference in femoral subtrochanteric fractures + IMN | Moderate |
| Agent | Class | Clinical Evidence | Quality of Evidence |
|---|---|---|---|
| Calcium/vitamin D | Supplemental | Potential activity of increasing bone mineral density at fracture site | Weak |
| Bisphosphonates | Antiresorptive | Unclear evidence suggests inhibition of healing. Unclear if there are benefits in augmenting healing. Improve BMD at fracture site when administrated 2 weeks after fracture. Improve fixation at bone implant interface | Weak |
| Denosumab | Antiresorptive | Does not affect negatively bone healing Not clear if enhance bone healing | Weak |
| Strontium ranelate | Anabolic | Case reports shown favor on fracture healing. Augment callus resistance and volume. Reports showed enhancement in union after delayed union or non-union. | Weak |
| Teriparatide | Anabolic | Reduction of healing time in long bone fractures and improved implant stabilization. Moderate evidence for enhanced bone healing of delayed unions, non-unions, atypical femoral fractures and periprosthetic femoral fractures | Moderate |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marongiu, G.; Contini, A.; Cozzi Lepri, A.; Donadu, M.; Verona, M.; Capone, A. The Treatment of Acute Diaphyseal Long-bones Fractures with Orthobiologics and Pharmacological Interventions for Bone Healing Enhancement: A Systematic Review of Clinical Evidence. Bioengineering 2020, 7, 22. https://doi.org/10.3390/bioengineering7010022
Marongiu G, Contini A, Cozzi Lepri A, Donadu M, Verona M, Capone A. The Treatment of Acute Diaphyseal Long-bones Fractures with Orthobiologics and Pharmacological Interventions for Bone Healing Enhancement: A Systematic Review of Clinical Evidence. Bioengineering. 2020; 7(1):22. https://doi.org/10.3390/bioengineering7010022
Chicago/Turabian StyleMarongiu, Giuseppe, Andrea Contini, Andrea Cozzi Lepri, Matthew Donadu, Marco Verona, and Antonio Capone. 2020. "The Treatment of Acute Diaphyseal Long-bones Fractures with Orthobiologics and Pharmacological Interventions for Bone Healing Enhancement: A Systematic Review of Clinical Evidence" Bioengineering 7, no. 1: 22. https://doi.org/10.3390/bioengineering7010022
APA StyleMarongiu, G., Contini, A., Cozzi Lepri, A., Donadu, M., Verona, M., & Capone, A. (2020). The Treatment of Acute Diaphyseal Long-bones Fractures with Orthobiologics and Pharmacological Interventions for Bone Healing Enhancement: A Systematic Review of Clinical Evidence. Bioengineering, 7(1), 22. https://doi.org/10.3390/bioengineering7010022