1. Introduction
Periapical radiography remains a fundamental diagnostic tool for assessing marginal bone levels around dental implants, primarily due to its cost-effectiveness, accessibility, and ease of use in routine clinical settings [
1,
2]. Although periapical radiographs are limited in providing only the mesial and distal aspects of implants [
3], they are regarded as sufficient for monitoring longitudinal changes in peri-implant bone levels [
4,
5], Moreover, periapical radiograph plays a critical role in the early detection of peri-implantitis and in evaluating progressive bone loss around implants [
2]. However, periapical radiographs inherently involve projecting three-dimensional structures onto a two-dimensional plane, which introduces potential geometric distortion [
6]. This limitation can result in the clinically significant underestimation of marginal bone loss [
7,
8,
9].
Image distortion of periapical radiographs typically arises from two principal causes: improper angulation of the X-ray tube head and misalignment of the digital sensor (film) [
1,
10]. Even relatively modest vertical or horizontal deviations, particularly those exceeding 10 degrees from the ideal projection, have been shown to compromise the accuracy and reliability of radiographic measurements [
11,
12,
13,
14]. Suboptimal image quality and examiner variability may further influence measurement consistency [
15,
16].
Previous studies have predominantly investigated the effects of projection error on detecting marginal bone levels or peri-implant osseous defects [
14]. However, with increasing interest in the role of restoration contour on peri-implant tissue health, attention has shifted toward more detailed morphological parameters, particularly the transmucosal configuration of implant restorations [
17,
18,
19]. Katafuchi et al. reported that an emergence angle exceeding 30°, as measured on periapical radiographs, was significantly associated with a higher prevalence of peri-implantitis [
20]. Furthermore, convex emergence profiles have been linked to a greater incidence of peri-implantitis than straight or concave profiles [
20,
21].
To better assess these morphological risks, Han et al. introduced the concept of the profile angle, a more refined metric designed to evaluate the three-dimensional geometry of CAD-CAM customized abutments [
22]. Unlike prefabricated abutments, CAD-CAM abutments feature highly individualized, free-form configurations that pose challenges for accurate assessment using two-dimensional radiographs. The profile angle is measured by dividing the transmucosal area into three distance ranges from the implant–abutment junction (0–1 mm, 1–2 mm, and 2–3 mm) and calculating the angle between the implant’s long axis and the outer contour of the abutment within each distance range. Studies have shown that the profile angle is more predictive of marginal bone loss than the traditional emergence angle [
22,
23].
Despite its potential clinical relevance, measuring the profile angle from periapical radiographs presents methodological challenges. While the implant has a standardized geometry that may allow partial correction for angulation error, CAD-CAM abutments lack uniformity. CAD-CAM abutments are especially vulnerable to image distortion resulting from even minor tube head or sensor misalignment [
24,
25,
26,
27]. Since most current assessments of profile angle rely on two-dimensional radiography, it is essential to evaluate how changes in projection geometry affect the accuracy of these measurements, particularly in the context of CAD-CAM restorations where transmucosal configuration varies considerably.
No study has assessed the impact of vertical and horizontal tube head angulation or digital sensor rotation on profile angle measurements. Moreover, the influence of implant position relative to the center of the edentulous ridge, whether buccally or lingually offset, on the magnitude of radiographic distortion remains unclear. The current study aimed to investigate how variations in X-ray tube head angulation and sensor alignment affect the accuracy of profile angle measurements in CAD-CAM abutments. An additional comparison was performed on whether implant positioning within the residual ridge contributes to distortion in periapical radiographs.
2. Materials and Methods
A mandibular acrylic resin model (PRO2002-UL-HD-FEM-28; Nissin Dental, Kyoto, Japan) was used as a base model. The right and the second first molars were removed, and the empty areas were recontoured using modeling wax (Pinnacle Modeling Wax; Dentsply Sirona, Bensheim, Germany). The model was scanned using an intraoral scanner (TRIOS3; 3Shape, Copenhagen, Denmark), and the STL file was printed using a polyjet 3D printer (J5 DentaJet; Stratasys, Minnetonka, MN, USA) to fabricate a master model. To evaluate the effect of implant positioning on profile angle distortion, five implant locations were designated based on the bucco-lingual position of the screw access channel (SAC):
Group Cent: SAC at the occlusal fossa.
Group B10: SAC 1.0 mm buccally off from a central position.
Group B15: SAC 1.5 mm buccally off from a central position.
Group L10: SAC 1.0 mm lingually off from a central position.
Group L15: SAC 1.5 mm lingually off from a central position.
All implants were planned using digital implant planning software (Implant Studio1.7.83.0; 3Shape), and full-guided surgical templates were fabricated to ensure precise placement. A single master model was used with interchangeable implant removable dies, allowing consistent comparison of radiographic distortion across different implant positions.
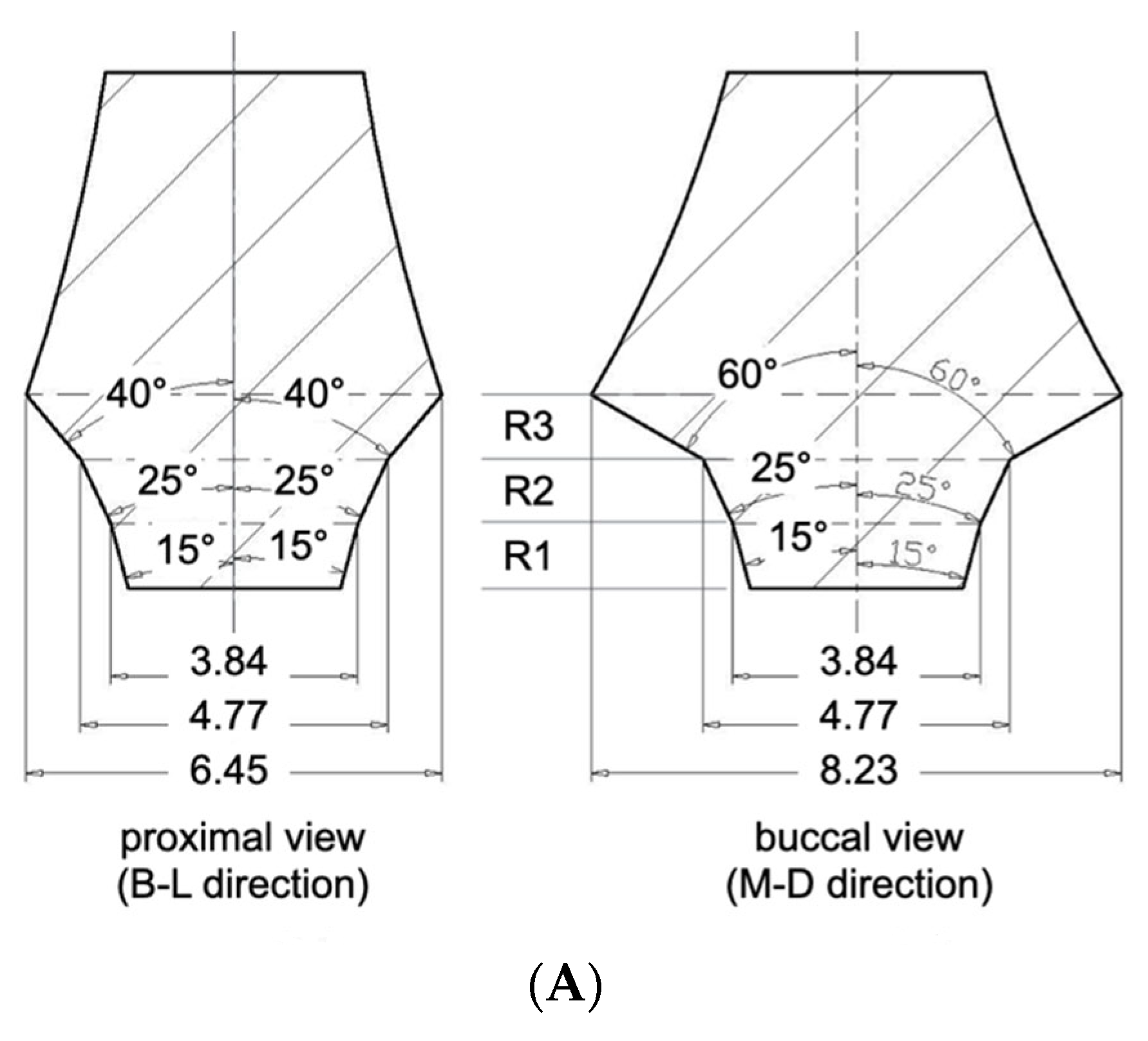
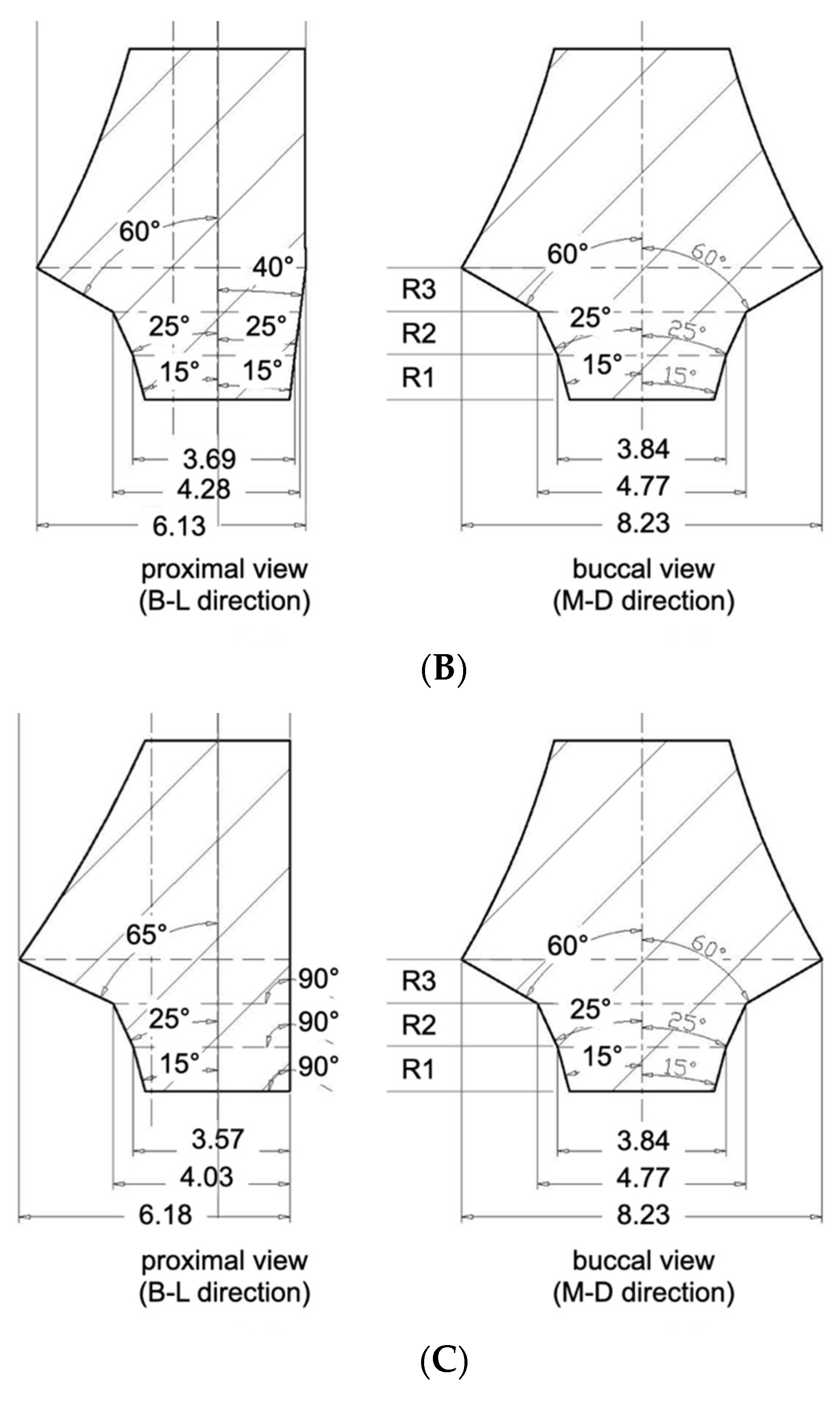
Three CAD-CAM abutments were designed to represent identical profile angle characteristics from the buccal or lingual aspect. The profile angles were uniformly set to 15° in the 0–1 mm distance range (R1), 25° in the 1–2 mm range (R2), and 60° in the 2–3 mm range (R3) above the implant–abutment junction (IAJ). This standardization allowed for controlled comparisons by eliminating variability in the bucco-lingual emergence profile. In contrast, the abutment designs differed in the mesio-distal direction due to varying degrees of asymmetry based on the horizontal offset of the SAC:
S-Type (Symmetrical Abutment): designed for Group Cent, it featured a symmetrical profile in both the mesio-distal and bucco-lingual planes. In the mesio-distal view, the profile angles were 15°, 25°, and 40° in R1, R2, and R3, respectively (
Figure 1A).
A10-Type (Asymmetrical 1.0 mm Offset): designed for Groups B10 and L10, presented asymmetry only in the mesio-distal plane. On the offset side (i.e., the direction of SAC displacement), the profile angles were 15°, 25°, and 60° in R1, R2, and R3. The opposite side featured a uniformly flattened profile angle of 7° across all three distance ranges (
Figure 1B).
A15-Type (Asymmetrical 1.5 mm Offset): designed for Groups B15 and L15, exhibited the most pronounced asymmetry. The profile angles were 15°, 25°, 65° at the offset side, while the opposite side was designed with a fully vertical contour, featuring 0° in all three ranges (
Figure 1C).
By keeping the bucco-lingual profile constant and only changing its shape when viewed from the mesio-distal direction (i.e., the proximal view), this design allowed us to investigate how different X-ray projection angles affect the measurement of profile angles depending on both the abutment contour and the implant′s position.
The right second premolar and second molar in the master model were prepared to receive full veneer ceramic crowns. The model was scanned using an intraoral scanner (TRIOS3; 3Shape), and full veneer restorations were designed using dental CAD software (CEREC inLab20; Dentsply Sirona). The crowns were then milled using a 3-axis milling machine (CEREC MC X; Dentsply Sirona) from lithium disilicate blocks (IPS e.max CAD; Ivoclar Vivadent, Schaan, Liechtenstein) and cemented using resin modified glass ionomer cement (RelyX Luting; 3M, Saint Paul, MN, USA) (
Figure 2).
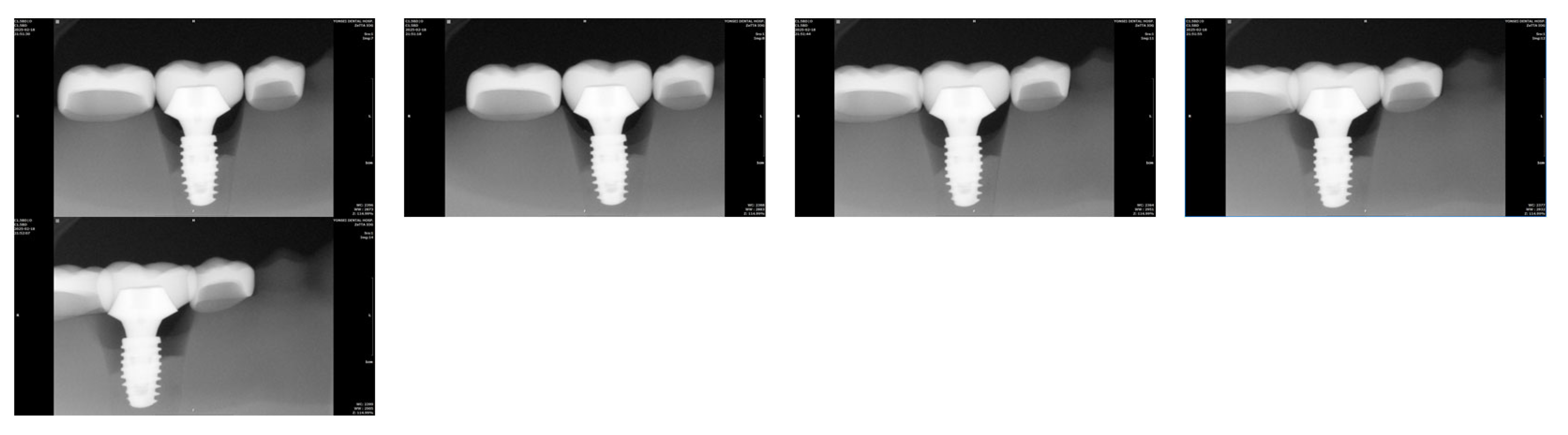
Each interchangeable implant die with its corresponding abutment was then sequentially positioned into the master model′s implant recipient site. Implant-supported crowns were fabricated following the same design and milling protocol used for the adjacent crowns. This process was repeated for all five implant dies, resulting in five implant-supported restorations, each corresponding to one of the experimental groups (
Figure 3).
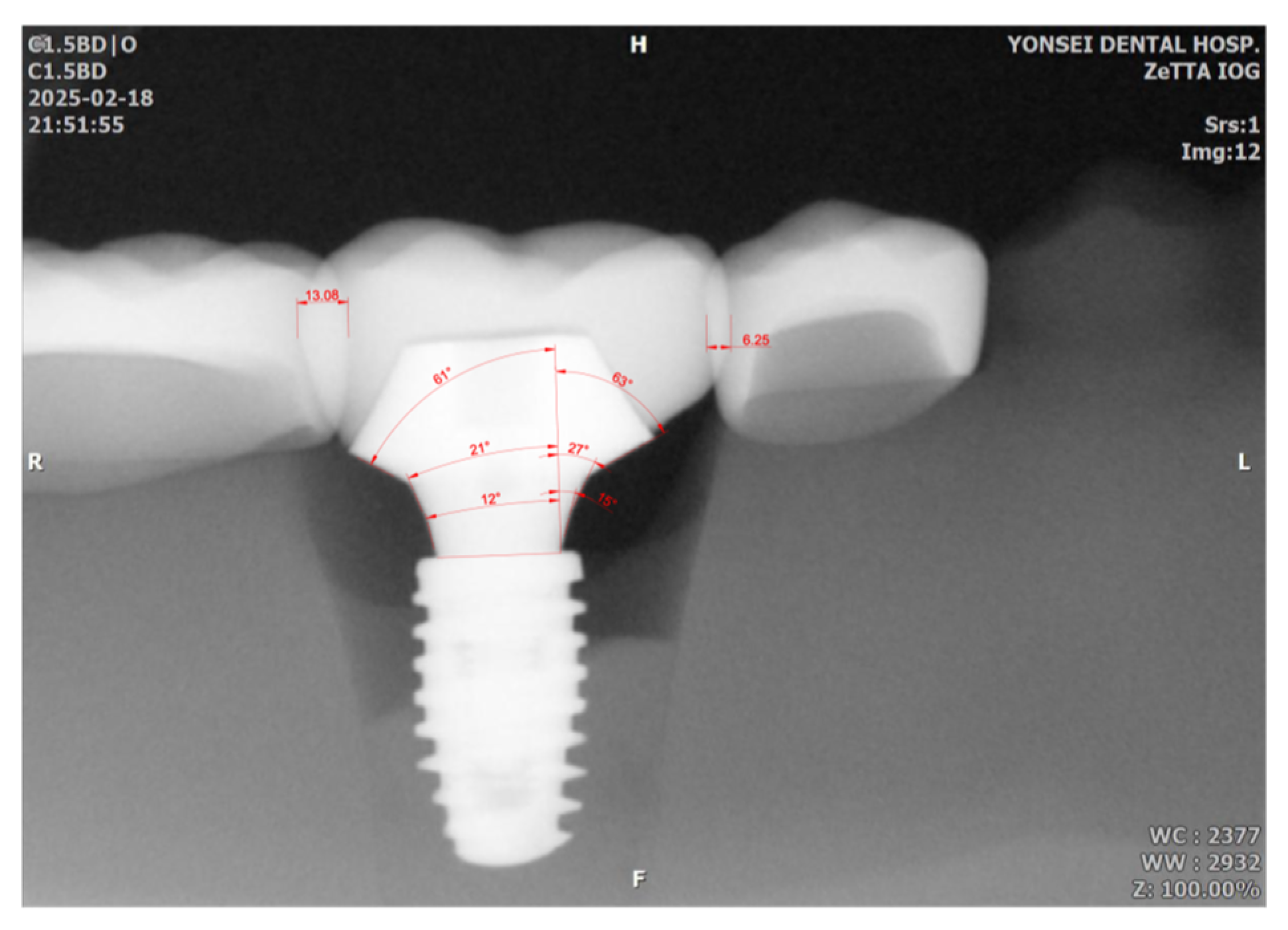
Radiographic imaging was performed with an intraoral X-ray device (ProXTM; Planmeca, Charlotte, NC, USA) and a CMOS digital sensor (RVG 6200; Carestream, Atlanta, GA, USA) under standardized conditions (70 kV, 1.12 mAs). Three experimental variables were tested: (1) Vertical tube head angulation: 0°, 5°, 10°, 15°, and 20° downward, with the digital sensor fixed parallel to the implant axis. (2) Horizontal digital sensor rotation: 0°, 5°, 10°, 15°, and 20° medial rotation, with the tube head fixed perpendicular to the implant. (3) Horizontal tube head angulation: 0°, 5°, 10°, 15°, and 20° mesial and distal rotations, with the digital sensor fixed.
Using CAD software (AutoCAD for MAC 2025 V.58.M.214; Autodesk Inc., San Francisco, CA, USA), interthread distances (between the second and third mesial threads), the amount of proximal overlap between adjacent restorations, and profile angles (mesial and distal aspects) were measured. Using CAD software (Meshmixer11.5.474; Autodesk Inc.), reference profile angles were obtained from the original STL abutment files. A calibrated examiner acquired each radiograph twice, and the mean value was used for analysis. As a pilot study with tightly controlled conditions and geometries, a single representative value per condition was analyzed descriptively. The focus was identifying distortion trends and absolute deviations rather than conducting inferential statistical comparisons.
4. Discussion
Periapical radiographs are widely employed in implant dentistry to evaluate peri-implant marginal bone levels and, more recently, the transmucosal contours of CAD-CAM customized abutments [
2,
9,
12]. However, these radiographs inherently project three-dimensional anatomical structures into two-dimensional images, making them susceptible to geometric distortion that may compromise the accuracy of radiographic assessments [
6]. This study explored how deviations in X-ray tube head projection angles and digital sensor alignment affect the reliability of profile angle, a parameter increasingly utilized to evaluate the biological relationship between abutment contour and peri-implant tissue response.
Our findings demonstrated that vertical and horizontal projection errors can significantly distort profile angle measurements. Among the variables investigated, horizontal tube head angulation exerted the most substantial influence, introducing asymmetrical distortion that either exaggerated or underestimated mesial and distal profile angles depending on the direction of rotation. Vertical angulation beyond 15° led to a consistent underestimation of the measured profile angles.
Few studies have directly evaluated the impact of sensor malalignment on radiographic image distortion. Preus et al. reported that positioning a digital sensor at a 30° angle relative to the long axis of teeth in dry human mandibles led to significant elongation of object images, even when the X-ray tube was aligned correctly [
28]. The current study showed that such rotation caused markedly greater distortion in interthread distances than vertical tube head deviations. Therefore, it is suggested that even minor sensor misalignment, often overlooked during paralleling techniques in clinical situations, can introduce significant image distortion. Thus, clinicians should exercise heightened caution in preventing sensor misalignment, as it may impact radiographic accuracy more than vertical angulation of the X-ray tube.
Another unique contribution of this study is the inclusion of implant positional offset within the residual ridge, which has not been addressed in prior literature. Even without projection angle deviations, 1.5 mm buccally off-center implants showed greater interthread distance elongation than lingually positioned implants. As projection angle deviation increased, distortion became more pronounced in buccally placed implants. At a vertical angulation of 20°, Group B15 exhibited nearly 40% interthread elongation, compared to only 7.9% in Group L15. Similarly, horizontal sensor rotation led to severe distortion in off-center groups, often exceeding acceptable thresholds or rendering measurement infeasible. This discrepancy is likely due to X-rays′ geometric divergence: when the implant is positioned closer to the X-ray source (e.g., buccally), the distortion increases because of the shorter source-to-object distance. Given that the distance from implant to sensor remains constant, these magnification effects become more pronounced. To mitigate this, increasing the distance between the X-ray tube head and the patient may help reduce beam divergence and minimize geometric distortion, particularly for buccally placed implants.
Based on the findings of this study, a set of clinically applicable guidelines can be proposed, radiographs exhibiting more than 10% interthread distance elongation or more than 10% crown overlap with adjacent teeth should be considered potentially inaccurate and retaken. These two thresholds can serve as practical indicators of vertical and horizontal projection error, respectively. This is especially relevant for buccally positioned implants, which appear more susceptible to distortion due to their proximity to the X-ray source. In such cases, clinicians may consider increasing the tube-to-object distance or using enhanced positioning protocols to maintain image fidelity.
Although this is a pilot study, it establishes critical trends, future studies with larger sample sizes and statistical analysis are warranted to validate these findings. A limitation of this pilot study is that the vertical angulation of the radiation tube was applied only in the positive direction. Previous studies have reported that when vertical angulation was increased in both positive and negative directions, greater linear distortion was observed in the negative direction at the same degree of rotation [
14,
29]. This aspect should be taken into consideration in the main study based on this pilot investigation. Further, in vivo studies, including patient-specific anatomical variations and comparisons with three-dimensional imaging modalities (e.g., CBCT with metal artifact reduction), would further strengthen the clinical relevance of profile angle assessments. Moreover, developing automated or AI-assisted tools for radiographic analysis may enhance standardization and reduce examiner-dependent variability, ultimately enabling a more robust evaluation of implant prosthesis design about peri-implant tissue health.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}