

Assessment of Interference in CIEDs Exposed to Magnetic Fields at Power Frequencies: Induced Voltage Analysis and Measurement

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Effects of Factors
3.2. Validation of Formula-Based Approach
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CIED | Cardiac Implantable Electronic Device |
| PM | Pacemaker |
| ICD | Implantable Cardioverter Defibrillator |
| EMI | Electromagnetic Interference |
| MF | Magnetic Field |
| EF | Electric Field |
| IPG | Impulse Generator |
References
- Timmis, A.; Aboyans, V.; Vardas, P.; Townsend, N.; Torbica, A.; Kavousi, M.; Boriani, G.; Huculeci, R.; Kazakiewicz, D.; Scherr, D.; et al. European Society of Cardiology: The 2023 Atlas of Cardiovascular Disease Statistics. Eur. Heart J. 2024, 45, 4019–4062. [Google Scholar] [CrossRef] [PubMed]
- Modenese, A.; Gobba, F. Occupational Exposure to Electromagnetic Fields and Health Surveillance According to the European Directive 2013/35/EU. Int. J. Environ. Res. Public Health 2021, 18, 1730. [Google Scholar] [CrossRef] [PubMed]
- Mattei, E.; Censi, F.; Calcagnini, G.; Falsaperla, R. Workers with Cardiac AIMD Exposed to EMF: Methods and Case Studies for Risk Analysis in the Framework of the European Regulations. Int. J. Environ. Res. Public Health 2021, 18, 9709. [Google Scholar] [CrossRef] [PubMed]
- Hansson Mild, K.; Mattsson, M.-O.; Jeschke, P.; Israel, M.; Ivanova, M.; Shalamanova, T. Occupational Exposure to Electromagnetic Fields—Different from General Public Exposure and Laboratory Studies. Int. J. Environ. Res. Public Health 2023, 20, 6552. [Google Scholar] [CrossRef] [PubMed]
- Pirkkalainen, H.; Heiskanen, T.; Tonteri, J.; Elovaara, J.; Mika, P.; Korpinen, L. Measuring Occupational Exposure to Extremely Low-Frequency Electric Fields at 220 kV Substations. Radiat. Prot. Dosim. 2017, 176, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Directive 2013/35/EU of the European Parliament and of the Council on the Minimum Health and Safety Requirements Regarding the Exposure of Workers to the Risks Arising from Physical Agents (Electromagnetic Fields) (20th Individual Directive within the Meaning of Article 16(1) of Directive 89/391/EEC) and Repealing Directive 2004/40/EC; European Parliament and of the Council: Strasbourg, France, 2013; Volume 21.
- Guidelines for Limiting Exposure to Time-Varying Electric and Magnetic Fields (1 Hz to 100 kHz). Health Phys. 2010, 99, 818–836. [CrossRef] [PubMed]
- Zink, M.D.; Stunder, D.; Theiler, T.; Kraus, T.; Marx, N.; Napp, A. In Vivo Study of Electromagnetic Interference With Cardiac Contractility Modulation Devices at Power Frequency. J. Am. Heart Assoc. 2021, 10, e019171. [Google Scholar] [CrossRef] [PubMed]
- Tiikkaja, M.; Aro, A.L.; Alanko, T.; Lindholm, H.; Sistonen, H.; Hartikainen, J.E.K.; Toivonen, L.; Juutilainen, J.; Hietanen, M. Electromagnetic Interference with Cardiac Pacemakers and Implantable Cardioverter-Defibrillators from Low-Frequency Electromagnetic Fields In Vivo. EP Eur. 2013, 15, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Seckler, T.; Stunder, D.; Schikowsky, C.; Joosten, S.; Zink, M.D.; Kraus, T.; Marx, N.; Napp, A. Effect of Lead Position and Orientation on Electromagnetic Interference in Patients with Bipolar Cardiovascular Implantable Electronic Devices. Europace 2016, 19, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Beinart, R.; Nazarian, S. Effects of External Electrical and Magnetic Fields on Pacemakers and Defibrillators: From Engineering Principles to Clinical Practice. Circulation 2013, 128, 2799–2809. [Google Scholar] [CrossRef] [PubMed]
- Gercek, C.; Kourtiche, D.; Nadi, M.; Magne, I.; Schmitt, P.; Souques, M. Computation of Pacemakers Immunity to 50 Hz Electric Field: Induced Voltages 10 Times Greater in Unipolar Than in Bipolar Detection Mode. Bioengineering 2017, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Kourtiche, D.; Claudel, J.; Deschamps, F.; Magne, I.; Roth, P.; Schmitt, P.; Nadi, M. Interference Voltage Measurement and Analysis of Cardiac Implants Exposed to Electric Fields at Extremely Low Frequency. Biomed. Phys. Eng. Express 2024, 10, 045060. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M. Assessment for Occupational Hazards to Cardiac Implantable Electronic Devices Due to Electric Field Exposure at Power Frequency within the Framework of European Standards. Radioprotection. Available online: https://www.radioprotection.org/component/article?access=doi&doi=10.1051/radiopro/2024060 (accessed on 28 April 2025).
- EN 50527-2-2:2018; Procedure for the Assessment of the Exposure to Electromagnetic Fields of Workers Bearing Active Implantable Medical Devices—Part 2-2: Specific Assessment for Workers with Cardioverter Defibrillators (ICD). European Union: Brussels, Belgium, 2018.
- Marchal, C.; Nadi, M.; Tosser, A.J.; Roussey, C.; Gaulard, M.L. Dielectric Properties of Gelatine Phantoms Used for Simulations of Biological Tissues between 10 and 50 MHz. Int. J. Hyperth. 1989, 5, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Scholten, A.; Silny, J. The Interference Threshold of Unipolar Cardiac Pacemakers in Extremely Low Frequency Magnetic Fields. J. Med. Eng. Technol. 2001, 25, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Kourtiche, D.; Claudel, J.; Deschamps, F.; Magne, I.; Roth, P.; Schmitt, P.; Souques, M.; Nadi, M. Interference Thresholds for Active Implantable Cardiovascular Devices in Occupational Low-Frequency Electric and Magnetic Fields: A Numerical and In Vitro Study. Med. Eng. Phys. 2022, 104, 103799. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
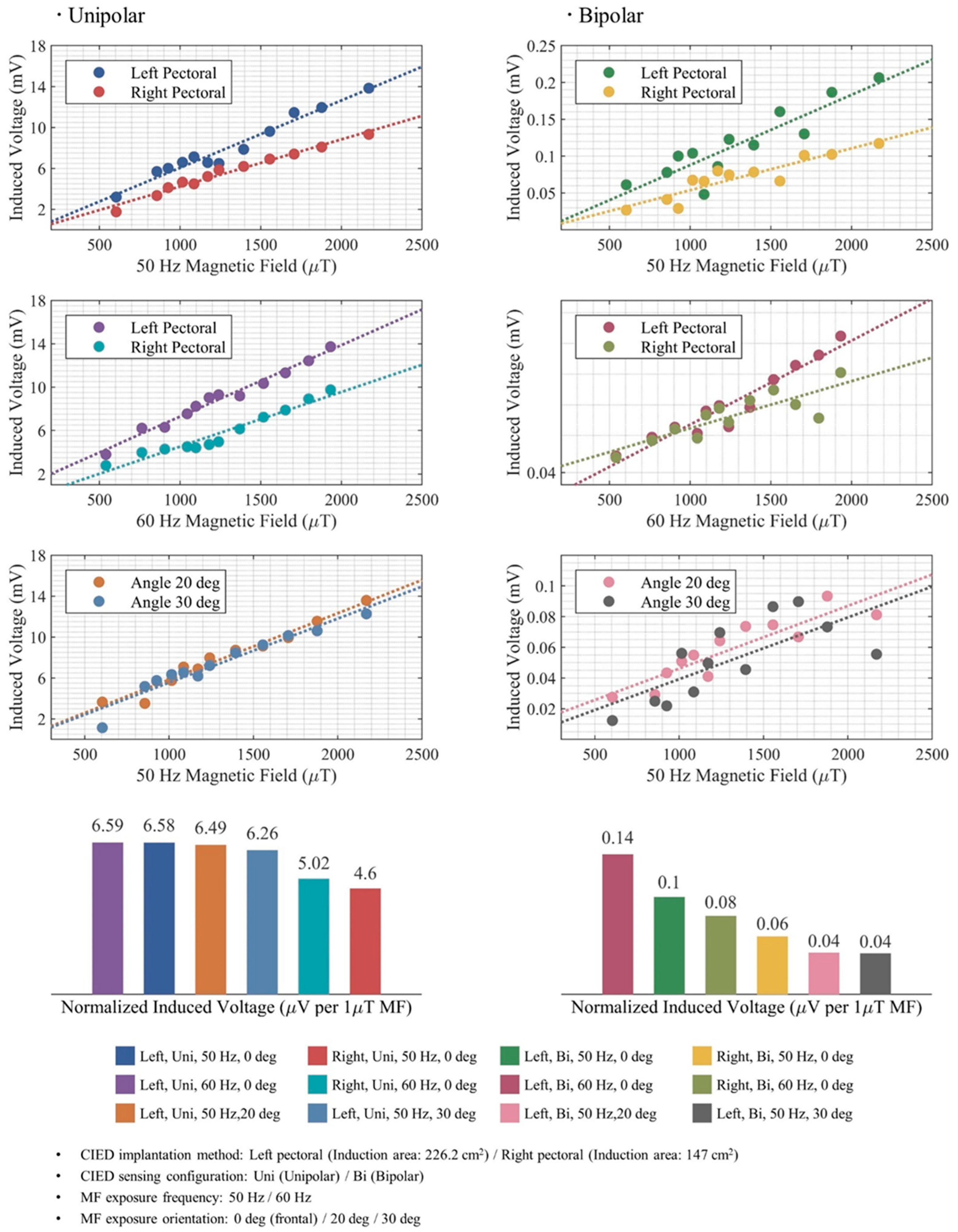
| Induction Area | Induced Voltage | ||||||
|---|---|---|---|---|---|---|---|
| Calculation | Simulation | Measurement | |||||
| Unipolar | Bipolar | Unipolar | Bipolar | Unipolar | Bipolar | Unipolar | Bipolar |
| cm2 | cm2 | μV | μV | μV | μV | μV | μV |
| 226.20 | 8.00 | 7.10 | 0.25 | 6.48 | 0.16 | 6.58 | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, M.; Kourtiche, D.; Claudel, J.; Roth, P.; Magne, I.; Deschamps, F.; Salvi, B. Assessment of Interference in CIEDs Exposed to Magnetic Fields at Power Frequencies: Induced Voltage Analysis and Measurement. Bioengineering 2025, 12, 677. https://doi.org/10.3390/bioengineering12070677
Zhou M, Kourtiche D, Claudel J, Roth P, Magne I, Deschamps F, Salvi B. Assessment of Interference in CIEDs Exposed to Magnetic Fields at Power Frequencies: Induced Voltage Analysis and Measurement. Bioengineering. 2025; 12(7):677. https://doi.org/10.3390/bioengineering12070677
Chicago/Turabian StyleZhou, Mengxi, Djilali Kourtiche, Julien Claudel, Patrice Roth, Isabelle Magne, François Deschamps, and Bruno Salvi. 2025. "Assessment of Interference in CIEDs Exposed to Magnetic Fields at Power Frequencies: Induced Voltage Analysis and Measurement" Bioengineering 12, no. 7: 677. https://doi.org/10.3390/bioengineering12070677
APA StyleZhou, M., Kourtiche, D., Claudel, J., Roth, P., Magne, I., Deschamps, F., & Salvi, B. (2025). Assessment of Interference in CIEDs Exposed to Magnetic Fields at Power Frequencies: Induced Voltage Analysis and Measurement. Bioengineering, 12(7), 677. https://doi.org/10.3390/bioengineering12070677