


Acute Biomechanical Effects of Cardiac Contractility Modulation in Living Myocardial Slices from End-Stage Heart Failure Patients

 , , , , , ,
, , , , , ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Slice Preparation
2.2. Slice Cultivation
2.3. CCM Stimulation
2.4. Functional Refractory Period
2.5. Force-Frequency Relationship
2.6. Contractile Measurements
2.7. Statistical Analysis
3. Results
3.1. LMS Characteristics
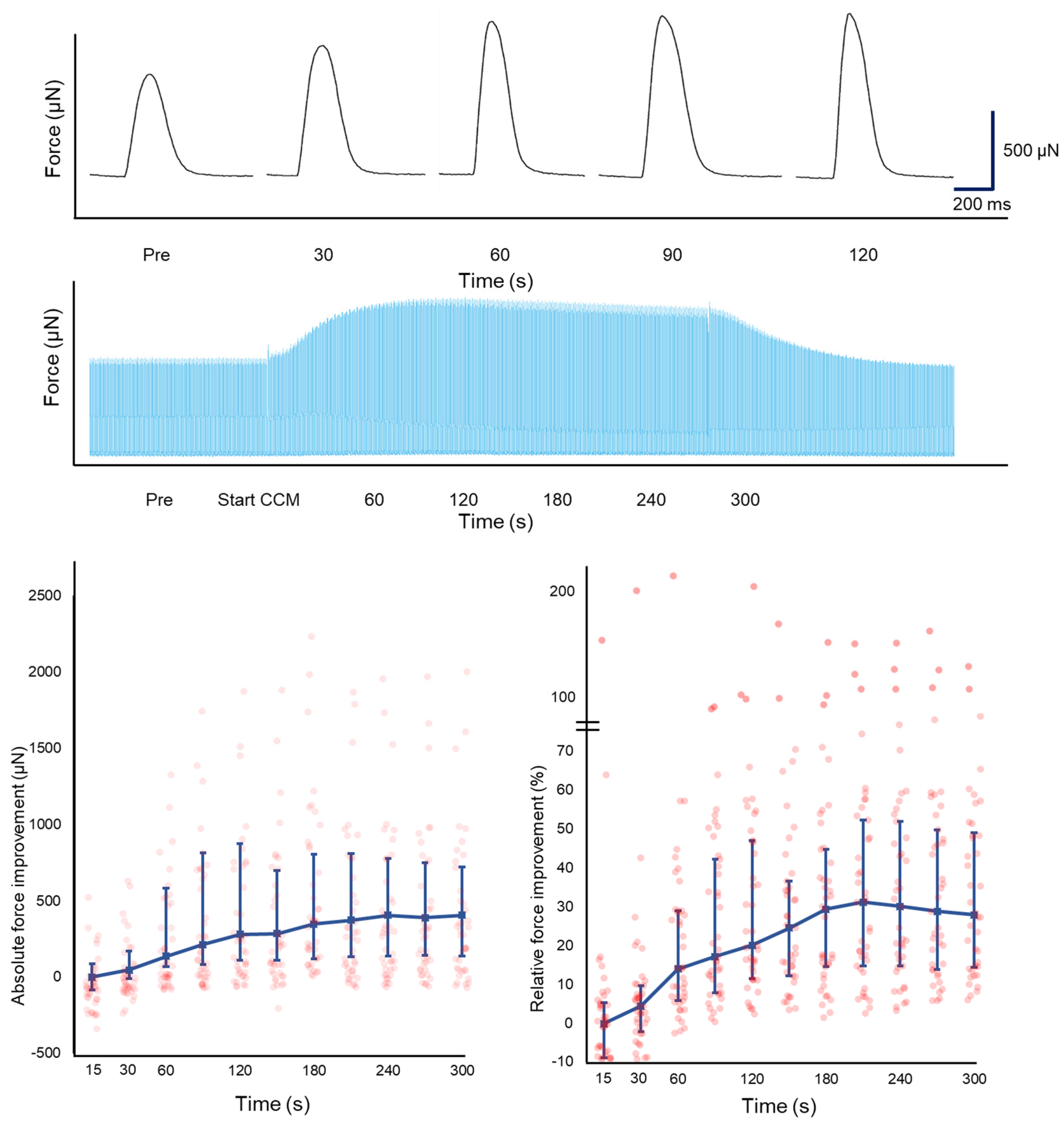
3.2. Biomechanical Effects of CCM on Contractility
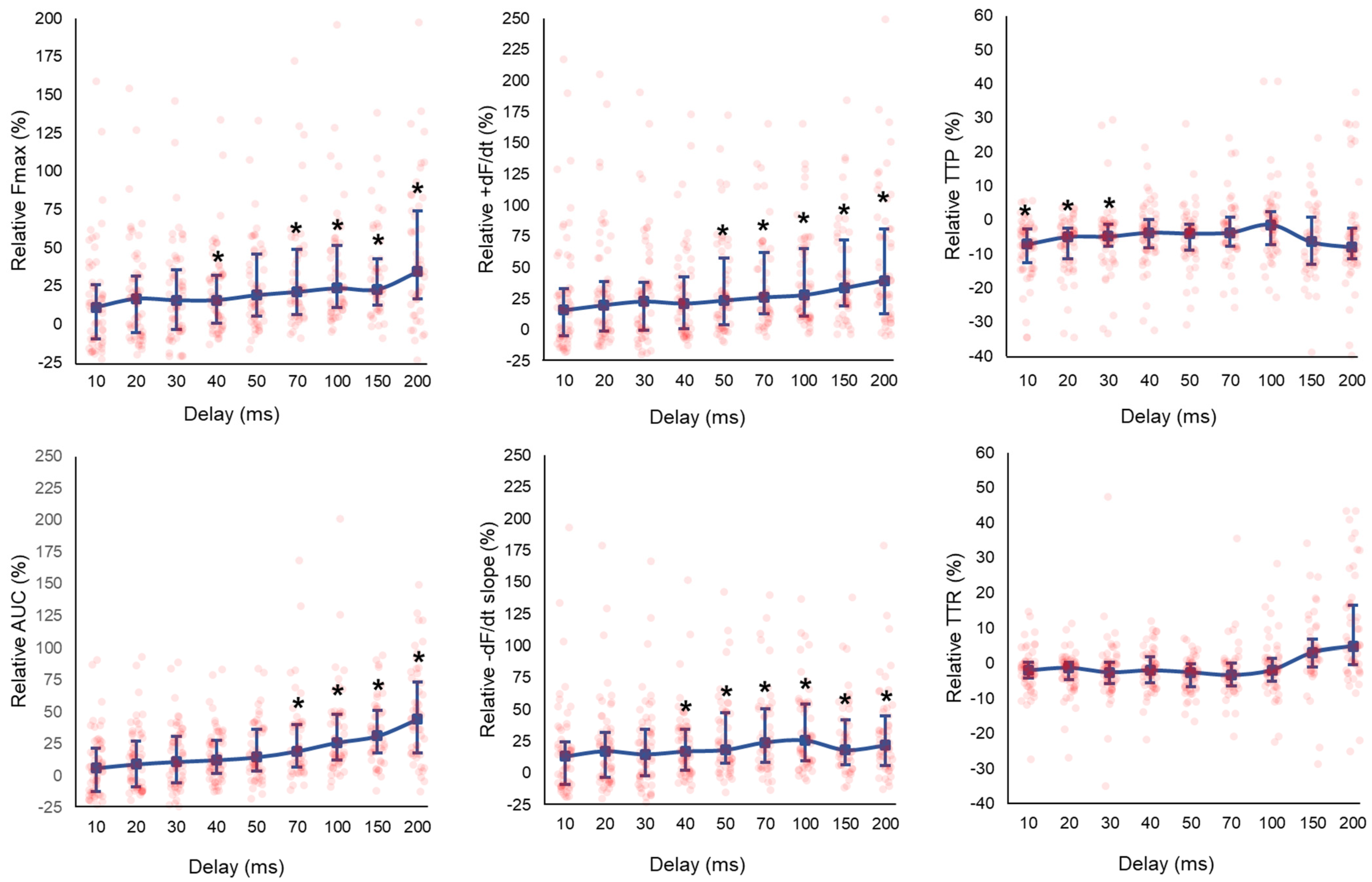
3.3. Effect of CCM Stimulation Delay
3.4. Effect of CCM Stimulation Duration
3.5. Effect of CCM Stimulation Amplitude
3.6. Force-Frequency Relationship
4. Discussion
4.1. Key Findings
4.2. Effect of CCM on the Biomechanical Profile of HF-LMS
4.3. Individual Response of LMS to CCM Stimulation
4.4. CCM and the Force Frequency Relationship in Failing Myocardium
4.5. Clinical Perspective
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giallauria, F.; Cuomo, G.; Parlato, A.; Raval, N.Y.; Kuschyk, J.; Coats, A.J.S. A comprehensive individual patient data meta-analysis of the effects of cardiac contractility modulation on functional capacity and heart failure-related quality of life. ESC Heart Fail. 2020, 7, 2922–2932. [Google Scholar] [CrossRef]
- Abraham, W.T.; Kuck, K.-H.; Goldsmith, R.L.; Lindenfeld, J.; Reddy, V.Y.; Carson, P.E.; Mann, D.L.; Saville, B.; Parise, H.; Chan, R.; et al. A Randomized Controlled Trial to Evaluate the Safety and Efficacy of Cardiac Contractility Modulation. JACC Heart Fail. 2018, 6, 874–883. [Google Scholar] [CrossRef]
- Yu, C.M.; Chan, J.Y.; Zhang, Q.; Yip, G.W.; Lam, Y.Y.; Chan, A.; Burkhoff, D.; Lee, P.W.; Fung, J.W. Impact of cardiac contractility modulation on left ventricular global and regional function and remodeling. JACC Cardiovasc. Imaging 2009, 2, 1341–1349. [Google Scholar] [CrossRef]
- Brunckhorst, C.B.; Shemer, I.; Mika, Y.; Ben-Haim, S.A.; Burkhoff, D. Cardiac contractility modulation by non-excitatory currents: Studies in isolated cardiac muscle. Eur. J. Heart Fail. 2005, 8, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Tschöpe, C.; Kherad, B.; Klein, O.; Lipp, A.; Blaschke, F.; Gutterman, D.; Burkhoff, D.; Hamdani, N.; Spillmann, F.; Van Linthout, S. Cardiac contractility modulation: Mechanisms of action in heart failure with reduced ejection fraction and beyond. Eur. J. Heart Fail. 2019, 21, 14–22. [Google Scholar] [CrossRef]
- Zhang, Q.; Chan, Y.-S.; Liang, Y.-J.; Fang, F.; Lam, Y.-Y.; Chan, C.-P.; Lee, A.P.-W.; Chan, K.C.-Y.; Wu, E.B.; Yu, C.-M. Comparison of left ventricular reverse remodeling induced by cardiac contractility modulation and cardiac resynchronization therapy in heart failure patients with different QRS durations. Int. J. Cardiol. 2013, 167, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Pipilas, D.C.; Hanley, A.; Singh, J.P.; Mela, T. Cardiac Contractility Modulation for Heart Failure: Current and Future Directions. J. Soc. Cardiovasc. Angiogr. Interv. 2023, 2, 101176. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Riccardi, M.; Sammartino, A.M.; Adamo, M.; Inciardi, R.M.; Lombardi, C.M.; Pugliese, N.R.; Tomasoni, D.; Vizzardi, E.; Metra, M.; Coats, A.J.S.; et al. Cardiac contractility modulation: An effective treatment strategy for heart failure beyond reduced left ventricular ejection fraction? Heart Fail. Rev. 2023, 28, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Feaster, T.K.; Feric, N.; Pallotta, I.; Narkar, A.; Casciola, M.; Graziano, M.P.; Aschar-Sobbi, R.; Blinova, K. Acute effects of cardiac contractility modulation stimulation in conventional 2D and 3D human induced pluripotent stem cell-derived cardiomyocyte models. Front. Physiol. 2022, 13, 1023563. [Google Scholar] [CrossRef]
- Narkar, A.; Feaster, T.K.; Casciola, M.; Blinova, K. Human in vitro neurocardiac coculture (ivNCC) assay development for evaluating cardiac contractility modulation. Physiol. Rep. 2022, 10, e15498. [Google Scholar] [CrossRef] [PubMed]
- Amesz, J.H.; Langmuur, S.J.; Bierhuizen, M.F.; de Groot, N.M.; Manintveld, O.C.; Taverne, Y.J. Omecamtiv mecarbil in precision-cut living heart failure slices: A story of a double-edged sword. J. Mol. Cell. Cardiol. Plus 2023, 5, 100040. [Google Scholar] [CrossRef]
- Fischer, C.; Milting, H.; Fein, E.; Reiser, E.; Lu, K.; Seidel, T.; Schinner, C.; Schwarzmayr, T.; Schramm, R.; Tomasi, R.; et al. Long-term functional and structural preservation of precision-cut human myocardium under continuous electromechanical stimulation in vitro. Nat. Commun. 2019, 10, 117. [Google Scholar] [CrossRef]
- Abu-Khousa, M.; Fiegle, D.J.; Sommer, S.T.; Minabari, G.; Milting, H.; Heim, C.; Weyand, M.; Tomasi, R.; Dendorfer, A.; Volk, T.; et al. The Degree of t-System Remodeling Predicts Negative Force-Frequency Relationship and Prolonged Relaxation Time in Failing Human Myocardium. Front. Physiol. 2020, 11, 182. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in linear mixed effects models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef]
- Morita, H.; Suzuki, G.; Haddad, W.; Mika, Y.; Tanhehco, E.J.; Sharov, V.G.; Goldstein, S.; Ben-Haim, S.; Sabbah, H.N. Cardiac contractility modulation with nonexcitatory electric signals improves left ventricular function in dogs with chronic heart failure. J. Card. Fail. 2003, 9, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Pappone, C.; Rosanio, S.; Burkhoff, D.; Mika, Y.; Vicedomini, G.; Augello, G.; Shemer, I.; Prutchi, D.; Haddad, W.; Aviv, R.; et al. Cardiac contractility modulation by electric currents applied during the refractory period in patients with heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am. J. Cardiol. 2002, 90, 1307–1313. [Google Scholar] [CrossRef] [PubMed]
- Pitoulis, F.G.; Nunez-Toldra, R.; Xiao, K.; Kit-Anan, W.; Mitzka, S.; Jabbour, R.J.; Harding, S.E.; Perbellini, F.; Thum, T.; de Tombe, P.P.; et al. Remodelling of adult cardiac tissue subjected to physiological and pathological mechanical load in vitro. Cardiovasc. Res. 2022, 118, 814–827. [Google Scholar] [CrossRef]
- Pitoulis, F.G.; Smith, J.J.; Pamias-Lopez, B.; de Tombe, P.P.; Hayman, D.; Terracciano, C.M. MyoLoop: Design, development and validation of a standalone bioreactor for pathophysiological electromechanical in vitro cardiac studies. Exp. Physiol. 2024, 109, 405–415. [Google Scholar] [CrossRef]
- Pitoulis, F.G.; Hasan, W.; Papadaki, M.; Clavere, N.G.; Perbellini, F.; Harding, S.E.; Kirk, J.A.; Boateng, S.Y.; de Tombe, P.P.; Terracciano, C.M. Intact myocardial preparations reveal intrinsic transmural heterogeneity in cardiac mechanics. J. Mol. Cell. Cardiol. 2020, 141, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Wood, E.H.; Heppner, R.L.; Weidmann, S. Inotropic effects of electric currents. I. Positive and negative effects of constant electric currents or current pulses applied during cardiac action potentials. II. Hypotheses: Calcium movements, excitation-contraction coupling and inotropic effects. Circ. Res. 1969, 24, 409–445. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.E. Cardiac Muscle; The Heart as a Pump and Function of the Heart Valves. In Guyton and Hall Textbook of Medical Phsyiology; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Pieske, B.; Trost, S.; Schütt, K.; Minami, K.; Just, H.; Hasenfuss, G. Influence of Forskolin on the force-frequency behavior in nonfailing and end-stage failing human myocardium. Basic Res. Cardiol. 1998, 93, s066–s075. [Google Scholar] [CrossRef]
- Hashimoto, K.; Perez, N.G.; Kusuoka, H.; Baker, D.L.; Periasamy, M.; Marbán, E. Frequency-dependent changes in calcium cycling and contractile activation in SERCA2a transgenic mice. Basic Res. Cardiol. 2000, 95, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Members, W.C. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. J. Card. Fail. 2022, 28, e1–e167. [Google Scholar]
- van Doorn, E.C.H.; Amesz, J.H.; Sadeghi, A.H.; de Groot, N.M.S.; Manintveld, O.C.; Taverne, Y.J.H.J. Preclinical Models of Cardiac Disease: A Comprehensive Overview for Clinical Scientists. Cardiovasc. Eng. Technol. 2024, 15, 232–249. [Google Scholar] [CrossRef] [PubMed]
- Watson, S.A.; Terracciano, C.M.; Perbellini, F. Myocardial Slices: An Intermediate Complexity Platform for Translational Cardiovascular Research. Cardiovasc. Drugs Ther. 2019, 33, 239–244. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | N = 7 |
|---|---|
| Age, years | 39 ± 18.5 |
| Male, n (%) | 3 (43) |
| Etiology of heart failure | |
| Ischemic cardiomyopathy, n | 3 |
| Dilated cardiomyopathy, n | 3 |
| Chemotherapy induced, n | 2 |
| Myocarditis, n | 1 |
| Arrhythmogenic cardiomyopathy, n | 1 |
| Surgery | |
| LVAD implantation, n | 2 |
| Cardiac transplantation, n | 5 |
| LVAD in situ, n | 1 |
| Baseline | CCM | p-Value | |
|---|---|---|---|
| Fmax (µN) | 1066 (529–2128) | 1229 (587–2658) | 0.050 * |
| CD (ms) | 450 (396–485) | 429 (377–482) | 0.297 |
| CD50 (ms) | 223 (210–256) | 217 (199–246) | 0.056 |
| –dF/dt (µN/s) | −6461 (−13,355–−3020) | −6968 (−16,660–−3692) | 0.043 * |
| +dF/dt (µN/s) | 8148 (4109–16,488) | 10145 (5086–22,260) | 0.050 * |
| AUC (µN.s) | 243 (129–464) | 297 (151–562) | 0.053 |
| TTP (ms) | 166 (152–187) | 160 (142–185) | 0.357 |
| TTR (ms) | 270 (230–305) | 268 (221–303) | 0.388 |
| Baseline | CCM | p-Value | |
|---|---|---|---|
| Fmax (µN) | 1066 (626–2113) | 1324 (801–2738) | 0.030 * |
| CD (ms) | 441 (393–485) | 411 (370–474) | 0.163 |
| CD50 (ms) | 224 (216–252) | 217 (202–242) | 0.043 * |
| –dF/dt (µN/s) | −6461 (−13,183–−3828) | −7914 (−16,915–−4505) | 0.028 * |
| +dF/dt (µN/s) | 8880 (5419–16,282) | 11275 (6629–24,770) | 0.027 * |
| AUC (µN.s) | 243 (156–461) | 306 (192–582) | 0.040 * |
| TTP (ms) | 166 (154–186) | 159 (142–173) | 0.209 |
| TTR (ms) | 267 (228–301) | 260 (220–281) | 0.272 |
| Patient etiology | Baseline (µN) | CCM (µN) | % | LMS (n) |
|---|---|---|---|---|
| Ischemic cardiomyopathy | 1411 (1042–2113) | 2376 (1239–2918) | 68.4 | 20 |
| Ischemic cardiomyopathy | 582 (405–863) | 786 (532–1113) | 35.2 | 5 |
| Myocarditis-induced dilated cardiomyopathy | 1103 (204–1485) | 1164 (317–1928) | 12.3 | 5 |
| Arrhythmogenic cardiomyopathy | 2668 (1247–4071) | 2927 (1267–4202) | 9.7 | 15 |
| Ischemic cardiomyopathy | 1103 (624–2167) | 1164 (629–2002) | 5.5 | 8 |
| Chemo-induced dilated cardiomyopathy | 267 (161–384) | 266 (143–454) | −0.3 | 11 |
| Chemo-induced dilated cardiomyopathy | 2267 (1652–2880) | 2172 (1671–2671) | −4.2 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bierhuizen, M.F.A.; Amesz, J.H.; Langmuur, S.J.J.; Lam, B.; Knops, P.; Veen, K.M.; Manintveld, O.C.; Kluin, J.; de Groot, N.M.S.; Taverne, Y.J.H.J. Acute Biomechanical Effects of Cardiac Contractility Modulation in Living Myocardial Slices from End-Stage Heart Failure Patients. Bioengineering 2025, 12, 174. https://doi.org/10.3390/bioengineering12020174
Bierhuizen MFA, Amesz JH, Langmuur SJJ, Lam B, Knops P, Veen KM, Manintveld OC, Kluin J, de Groot NMS, Taverne YJHJ. Acute Biomechanical Effects of Cardiac Contractility Modulation in Living Myocardial Slices from End-Stage Heart Failure Patients. Bioengineering. 2025; 12(2):174. https://doi.org/10.3390/bioengineering12020174
Chicago/Turabian StyleBierhuizen, Mark F. A., Jorik H. Amesz, Sanne J. J. Langmuur, Bobby Lam, Paul Knops, Kevin M. Veen, Olivier C. Manintveld, Jolanda Kluin, Natasja M. S. de Groot, and Yannick J. H. J. Taverne. 2025. "Acute Biomechanical Effects of Cardiac Contractility Modulation in Living Myocardial Slices from End-Stage Heart Failure Patients" Bioengineering 12, no. 2: 174. https://doi.org/10.3390/bioengineering12020174
APA StyleBierhuizen, M. F. A., Amesz, J. H., Langmuur, S. J. J., Lam, B., Knops, P., Veen, K. M., Manintveld, O. C., Kluin, J., de Groot, N. M. S., & Taverne, Y. J. H. J. (2025). Acute Biomechanical Effects of Cardiac Contractility Modulation in Living Myocardial Slices from End-Stage Heart Failure Patients. Bioengineering, 12(2), 174. https://doi.org/10.3390/bioengineering12020174