
Measuring Geographic Atrophy Area Using Column-Based Machine Learning Software on Spectral-Domain Optical Coherence Tomography versus Fundus Auto Fluorescence

 , , , ,
, , , ,
Abstract

1. Background
2. Methods
2.1. Study Design, Patient Selection, and Data Collection
2.2. FAF Image Acquisition
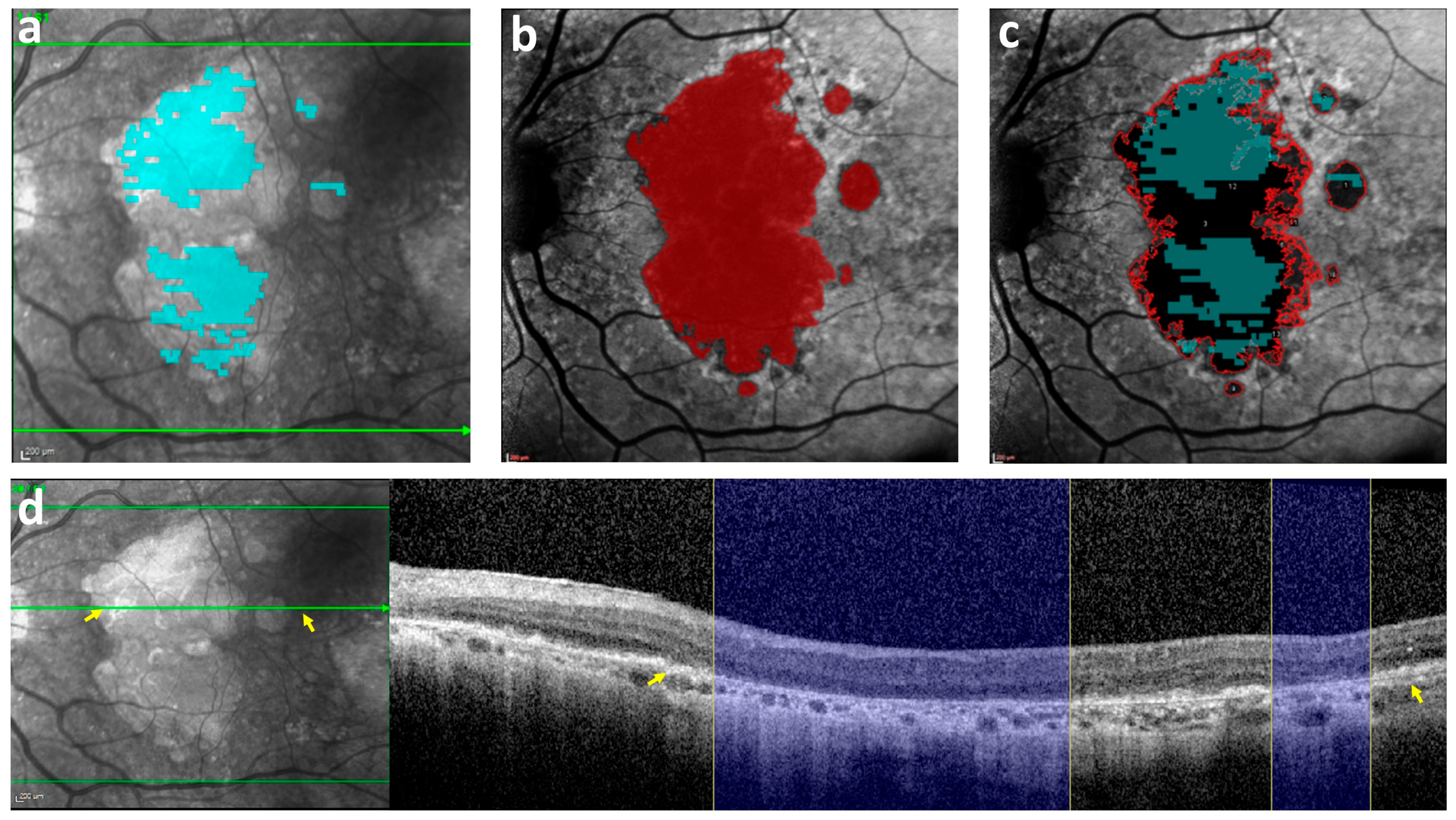
2.3. FAF Image Analysis and Semi-Automated Annotation
2.4. OCT Image Acquisition
2.5. OCT Image Analysis and Semi-Automated Annotation
2.6. Measured Parameters
2.7. Study Outcomes
2.8. Statistical Analysis
2.9. Subgroup Analysis
3. Results
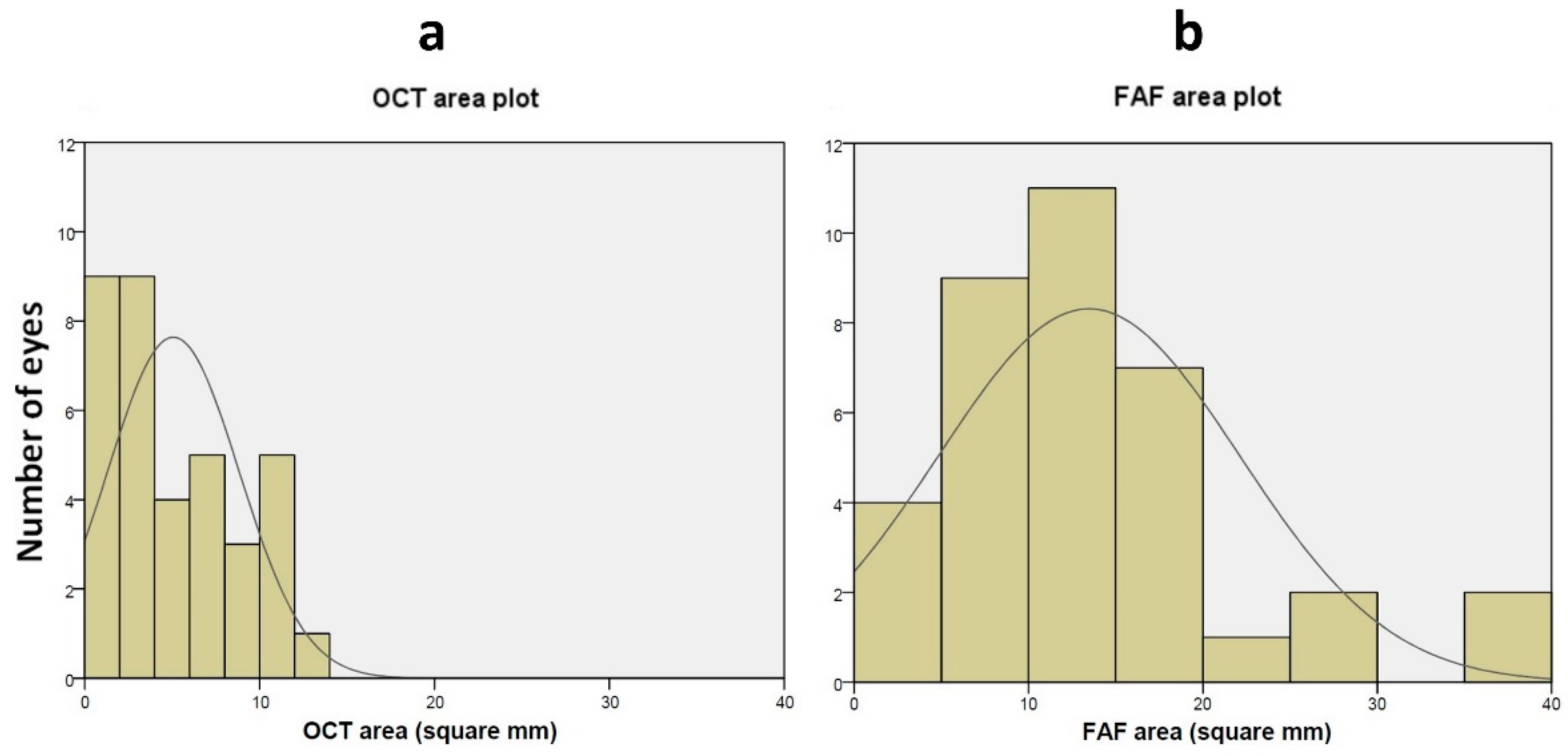
3.1. GA Outcome Measures
3.2. Correlation between the OCT Shape Descriptors and the Difference in GA Area Measured between FAF and OCT
3.3. Correlation between the FAF Shape Descriptors and the Difference in GA Area Measured between FAF and OCT
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khan, H.; Aziz, A.A.; Sulahria, H.; Khan, H.; Ahmed, A.; Choudhry, N.; Narayanan, R.; Danzig, C.; Khanani, A.M. Emerging Treatment Options for Geographic Atrophy (GA) Secondary to Age-Related Macular Degeneration. Clin. Ophthalmol. 2023, 17, 321–327. [Google Scholar] [CrossRef]
- Sadda, S.R.; Guymer, R.; Holz, F.G.; Schmitz-Valckenberg, S.; Curcio, C.A.; Bird, A.C.; Blodi, B.A.; Bottoni, F.; Chakravarthy, U.; Chew, E.Y.; et al. Consensus Definition for Atrophy Associated with Age-Related Macular Degeneration on OCT: Classification of Atrophy Report 3. Ophthalmology 2018, 125, 537–548. [Google Scholar] [CrossRef]
- Fleckenstein, M.; Mitchell, P.; Freund, K.B.; Sadda, S.V.; Holz, F.G.; Brittain, C.; Henry, E.C.; Ferrara, D. The Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration. Ophthalmology 2018, 125, 369–390. [Google Scholar] [CrossRef] [PubMed]
- Holz, F.G.; Sadda, S.R.; Staurenghi, G.; Lindner, M.; Bird, A.C.; Blodi, B.A.; Bottoni, F.; Chakravarthy, U.; Chew, E.Y.; Csaky, K.; et al. Imaging Protocols in Clinical Studies in Advanced Age-Related Macular Degeneration. Ophthalmology 2017, 124, 464–478. [Google Scholar] [CrossRef]
- Schmitz-Valckenberg, S.; Pfau, M.; Fleckenstein, M.; Staurenghi, G.; Sparrow, J.R.; Bindewald-Wittich, A.; Spaide, R.F.; Wolf, S.; Sadda, S.R.; Holz, F.G. Fundus Autofluorescence Imaging. Prog. Retin. Eye Res. 2021, 81, 100893. [Google Scholar] [CrossRef]
- Guymer, R.H. Geographic Atrophy Trials: Turning the Ship around May Not Be That Easy. Ophthalmol. Retin. 2018, 2, 515–517. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, G.J.; Westby, K.; Csaky, K.G.; Monés, J.; Pearlman, J.A.; Patel, S.S.; Joondeph, B.C.; Randolph, J.; Masonson, H.; Rezaei, K.A. C5 Inhibitor Avacincaptad Pegol for Geographic Atrophy Due to Age-Related Macular Degeneration: A Randomized Pivotal Phase 2/3 Trial. Ophthalmology 2021, 128, 576–586. [Google Scholar] [CrossRef]
- Bindewald, A.; Bird, A.C.; Dandekar, S.S.; Dolar-Szczasny, J.; Dreybaupt, J.; Fitzke, F.W.; Einbock, W.; Holz, F.G.; Jorzik, J.J.; Keilhauer, C.; et al. Classification of Fundus Autofluorescence Patterns in Early Age-Related Macular Disease. Investig. Ophthalmol. Vis. Sci. 2005, 46, 3309–3314. [Google Scholar] [CrossRef] [PubMed]
- Cleland, S.C.; Konda, S.M.; Danis, R.P.; Huang, Y.; Myers, D.J.; Blodi, B.A.; Domalpally, A. Quantification of Geographic Atrophy Using Spectral Domain OCT in Age-Related Macular Degeneration. Ophthalmol. Retin. 2021, 5, 41–48. [Google Scholar] [CrossRef]
- Velaga, S.B.; Nittala, M.G.; Hariri, A.; Sadda, S.R. Correlation between Fundus Autofluorescence and En Face OCT Measurements of Geographic Atrophy. Ophthalmol. Retin. 2022, 6, 676–683. [Google Scholar] [CrossRef]
- Ji, Z.; Chen, Q.; Niu, S.; Leng, T.; Rubin, D.L. Beyond Retinal Layers: A Deep Voting Model for Automated Geographic Atrophy Segmentation in SD-OCT Images. Transl. Vis. Sci. Technol. 2018, 7, 1. [Google Scholar] [CrossRef]
- Xu, R.; Niu, S.; Chen, Q.; Ji, Z.; Rubin, D.; Chen, Y. Automated Geographic Atrophy Segmentation for SD-OCT Images Based on Two-Stage Learning Model. Comput. Biol. Med. 2019, 105, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Keenan, T.D.; Dharssi, S.; Peng, Y.; Chen, Q.; Agrón, E.; Wong, W.T.; Lu, Z.; Chew, E.Y. A Deep Learning Approach for Automated Detection of Geographic Atrophy from Color Fundus Photographs. Ophthalmology 2019, 126, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.J.; Izatt, J.A.; O’Connell, R.V.; Winter, K.P.; Toth, C.A.; Farsiu, S. Validated Automatic Segmentation of AMD Pathology Including Drusen and Geographic Atrophy in SD-OCT Images. Investig. Ophthalmol. Vis. Sci. 2012, 53, 53–61. [Google Scholar] [CrossRef]
- Hu, Z.; Wang, Z.; Sadda, S. Automated Segmentation of Geographic Atrophy Using Deep Convolutional Neural Networks. In Proceedings of the Medical Imaging 2018: Computer-Aided Diagnosis, Houston, TX, USA, 10–15 February 2018. [Google Scholar]
- Panthier, C.; Querques, G.; Puche, N.; Le Tien, V.; Garavito, R.B.; Béchet, S.; Massamba, N.; Souied, E.H. Evaluation of Semiautomated Measurement of Geographic Atrophy in Age-Related Macular Degeneration by Fundus Autofluorescence in Clinical Setting. Retina 2014, 34, 576–582. [Google Scholar] [CrossRef]
- Szeskin, A.; Yehuda, R.; Shmueli, O.; Levy, J.; Joskowicz, L. A Column-Based Deep Learning Method for the Detection and Quantification of Atrophy Associated with AMD in OCT Scans. Med. Image Anal. 2021, 72, 102130. [Google Scholar] [CrossRef]
- Mahmoudzadeh, R.; Salabati, M.; Khan, M.A.; Garg, S.J.; Hsu, J. Manual versus Semi-Automated Measurement of Geographic Atrophy Area in Eyes with Age-Related Macular Degeneration. Transl. Vis. Sci. Technol. 2021, 10, 33. [Google Scholar] [CrossRef] [PubMed]
- Yehoshua, Z.; Rosenfeld, P.J.; Gregori, G.; Feuer, W.J.; Falcão, M.; Lujan, B.J.; Puliafito, C. Progression of Geographic Atrophy in Age-Related Macular Degeneration Imaged with Spectral Domain Optical Coherence Tomography. Ophthalmology 2011, 118, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Alagorie, A.R.; Nassisi, M.; Verma, A.; Nittala, M.; Corradetti, G.; Velaga, S.; Sadda, S.R. Relationship between Proximity of Choriocapillaris Flow Deficits and Enlargement Rate of Geographic Atrophy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 995–1003. [Google Scholar] [CrossRef]
- Sayegh, R.G.; Simader, C.; Scheschy, U.; Montuoro, A.; Kiss, C.; Sacu, S.; Kreil, D.P.; Prnte, C.; Schmidt-Erfurth, U. A Systematic Comparison of Spectral-Domain Optical Coherence Tomography and Fundus Autofluorescence in Patients with Geographic Atrophy. Ophthalmology 2011, 118, 1844–1851. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, O.; Yehuda, R.; Szeskin, A.; Joskowicz, L.; Levy, J. Progression of CRORA (Complete RPE and Outer Retinal Atrophy) in Dry Age-Related Macular Degeneration Measured Using SD-OCT. Transl. Vis. Sci. Technol. 2022, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Carass, A.; Roy, S.; Gherman, A.; Reinhold, J.C.; Jesson, A.; Arbel, T.; Maier, O.; Handels, H.; Ghafoorian, M.; Platel, B.; et al. Evaluating White Matter Lesion Segmentations with Refined Sørensen-Dice Analysis. Sci. Rep. 2020, 10, 8242. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.L.; Sun, M.; Khetpal, S.; Grossetta Nardini, H.K.; Del Priore, L.V. Topographic Variation of the Growth Rate of Geographic Atrophy in Nonexudative Age-Related Macular Degeneration: A Systematic Review and Meta-Analysis. Investig. Ophthalmol. Vis. Sci. 2020, 61, 2. [Google Scholar]
- Pfau, M.; Lindner, M.; Goerdt, L.; Thiele, S.; Nadal, J.; Schmid, M.; Schmitz-Valckenberg, S.; Sadda, S.R.; Holz, F.G.; Fleckenstein, M. Prognostic Value of Shape-Descriptive Factors for the Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration. Retina 2019, 39, 1527–1540. [Google Scholar] [CrossRef] [PubMed]
- Liefers, B.; Colijn, J.M.; González-Gonzalo, C.; Verzijden, T.; Wang, J.J.; Joachim, N.; Mitchell, P.; Hoyng, C.B.; van Ginneken, B.; Klaver, C.C.W.; et al. A Deep Learning Model for Segmentation of Geographic Atrophy to Study Its Long-Term Natural History. Ophthalmology 2020, 127, 1086–1096. [Google Scholar] [CrossRef]
- Sayegh, R.G.; Sacu, S.; Dunavölgyi, R.; Kroh, M.E.; Roberts, P.; Mitsch, C.; Montuoro, A.; Ehrenmüller, M.; Schmidt-Erfurth, U. Geographic Atrophy and Foveal-Sparing Changes Related to Visual Acuity in Patients with Dry Age-Related Macular Degeneration Over Time. Am. J. Ophthalmol. 2017, 179, 118–128. [Google Scholar] [CrossRef]
- Shen, L.L.; Sun, M.; Grossetta Nardini, H.K.; Del Priore, L.V. Progression of Unifocal versus Multifocal Geographic Atrophy in Age-Related Macular Degeneration: A Systematic Review and Meta-Analysis. Ophthalmol. Retin. 2020, 4, 899–910. [Google Scholar]
- Zanzottera, E.C.; Ach, T.; Huisingh, C.; Messinger, J.D.; Freund, K.B.; Curcio, C.A. Visualizing Retinal Pigment Epithelium Phenotypes in the Transition to Atrophy in Neovascular Age-Related Macular Degeneration. Retina 2016, 36 (Suppl. 1), S26–S39. [Google Scholar] [CrossRef] [PubMed]
- Rudolf, M.; Vogt, S.D.; Curcio, C.A.; Huisingh, C.; McGwin, G.; Wagner, A.; Grisanti, S.; Read, R.W. Histologic Basis of Variations in Retinal Pigment Epithelium Autofluorescence in Eyes with Geographic Atrophy. Ophthalmology 2013, 120, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.L.; Sun, M.; Ahluwalia, A.; Young, B.K.; Park, M.M.; Del Priore, L.V. Geographic Atrophy Growth Is Strongly Related to Lesion Perimeter: Unifying Effects of Lesion Area, Number, and Circularity on Growth. Ophthalmol. Retin. 2021, 5, 868–878. [Google Scholar] [CrossRef]
- Schmitz-Valckenberg, S.; Sahel, J.A.; Danis, R.; Fleckenstein, M.; Jaffe, G.J.; Wolf, S.; Pruente, C.; Holz, F.G. Natural History of Geographic Atrophy Progression Secondary to Age-Related Macular Degeneration (Geographic Atrophy Progression Study). Ophthalmology 2016, 123, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.L.; Sun, M.; Ahluwalia, A.; Park, M.M.; Young, B.K.; Del Priore, L.V. Local Progression Kinetics of Geographic Atrophy Depends upon the Border Location. Investig. Ophthalmol. Vis. Sci. 2021, 62, 28. [Google Scholar] [CrossRef] [PubMed]
- Keenan, T.D.; Agrón, E.; Domalpally, A.; Clemons, T.E.; van Asten, F.; Wong, W.T.; Danis, R.G.; Sadda, S.V.; Rosenfeld, P.J.; Klein, M.L.; et al. Progression of Geographic Atrophy in Age-Related Macular Degeneration: AREDS2 Report Number 16. Ophthalmology 2018, 125, 1913–1928. [Google Scholar] [CrossRef]
- Liao, D.S.; Grossi, F.V.; El Mehdi, D.; Gerber, M.R.; Brown, D.M.; Heier, J.S.; Wykoff, C.C.; Singerman, L.J.; Abraham, P.; Grassmann, F.; et al. Complement C3 Inhibitor Pegcetacoplan for Geographic Atrophy Secondary to Age-Related Macular Degeneration: A Randomized Phase 2 Trial. Ophthalmology 2020, 127, 186–195. [Google Scholar] [CrossRef]
- Wu, Z.; Pfau, M.; Blodi, B.A.; Holz, F.G.; Jaffe, G.J.; Liakopoulos, S.; Sadda, S.R.; Staurenghi, G.; Bjelopera, E.; Brown, T.; et al. OCT Signs of Early Atrophy in Age-Related Macular Degeneration: Interreader Agreement: Classification of Atrophy Meetings Report 6. Ophthalmol. Retin. 2022, 6, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Chandra, S.; Rasheed, R.; Sen, P.; Menon, D.; Sivaprasad, S. Inter-Rater Reliability for Diagnosis of Geographic Atrophy Using Spectral Domain OCT in Age-Related Macular Degeneration. Eye 2022, 36, 392–397. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| p-Value | FAF | OCT | Factor |
|---|---|---|---|
| (n = 36 Eyes) | (n = 36 Eyes) | ||
| <0.0001 | 13.47 ± 8.64 | 4.74 ± 3.80 | Total lesion area (mm2) |
| (0.24; 37.98) | (0.15; 13.23) | ||
| 0.002 | 42.36 ± 22.31 | 33.38 ± 19.74 | Perimeter (mm) |
| (2.93; 97.17) | (1.63; 77.44) | ||
| 0.001 | 4.54 ± 3.37 | 8.53 ± 6.17 | 1 Focality |
| (1.00; 15.00) | (1.00; 31.00) | ||
| <0.0001 | 0.34 ± 0.18 | 0.49 ± 0.14 | 2 Circularity |
| (0.10; 1.15) | (0.07; 0.75) | ||
| <0.0001 | 1.43 ± 1.04 | 0.31 ± 0.39 | Minimum distance from center (mm) |
| (0; 3.62) | (0; 1.89) | ||
| 0.002 | 1.18 ± 1.62 | 0.31 ± 0.71 | Minimum lesion Feret (mm) |
| (0.03; 5.22) | (0.05; 3.55) | ||
| <0.0001 | 4.70 ± 1.59 | 2.81 ± 1.48 | Maximum lesion Feret (mm) |
| (0.74; 8.14) | (0.52; 6.77) |
| Univariate Regression Analysis | ||
|---|---|---|
| Variable | 1 r | p-Value |
| Total lesion area (mm2) | 0.408 | 0.007 |
| Perimeter (mm) | 0.68 | <0.0001 |
| 2 Focality | 0.58 | <0.0001 |
| 3 Circularity | 0.05 | 0.391 |
| Minimum distance from center (mm) | 0.12 | 0.250 |
| Minimum lesion Feret (mm) | −0.22 | 0.102 |
| Maximum lesion Feret (mm) | 0.35 | 0.018 |
| Multivariate Regression Analysis | ||
| Variable | Estimated β | p-Value |
| Total lesion area (mm2) | −0.15 | 0.66 |
| Perimeter (mm) | 0.31 | <0.0001 |
| Focality | 0.07 | 0.77 |
| Maximum lesion Feret (mm) | −1.63 | 0.047 |
| Adjusted r2 | 0.52 | |
| Univariate Regression Analysis | ||
|---|---|---|
| Variable | 1 r | p-Value |
| Total lesion area (mm2) | 0.92 | <0.0001 |
| Perimeter (mm) | 0.74 | <0.0001 |
| 2 Focality | 0.32 | 0.09 |
| 3 Circularity | −0.12 | 0.25 |
| Minimum distance from center (mm) | −0.44 | 0.004 |
| Minimum lesion Feret (mm) | 0.11 | 0.48 |
| Maximum lesion Feret (mm) | 0.87 | <0.0001 |
| Multivariate Regression Analysis | ||
| Variable | Estimated β | p-Value |
| Total lesion area (mm2) | 0.67 | <0.0001 |
| Perimeter (mm) | 0.31 | 0.34 |
| Minimum distance from center (mm) | 0.07 | 0.13 |
| Maximum lesion Feret (mm) | −1.63 | 0.62 |
| Adjusted r2 | 0.83 | |
| p-Value | FAF | OCT | Factor |
|---|---|---|---|
| (n = 9 Eyes) | (n = 9 Eyes) | ||
| 0.001 | 9.85 ± 5.08 | 3.35 ± 3.18 | Total lesion area (mm2) |
| (2.65; 16.73) | (0.57; 10.38) | ||
| 0.51 | 42.36 ± 22.31 | 37.13 ± 24.33 | Perimeter (mm) |
| (16.16; 52.58) | (8.68; 84.93) | ||
| 0.01 | 4.11 ± 2.93 | 13.00 ± 7.92 | 1 Focality |
| (1.00; 8.50) | (5.00; 26.00) | ||
| 0.04 | 0.36 ± 0.15 | 0.49 ± 0.08 | 2 Circularity |
| (0.12; 0.67) | (0.38; 0.59) | ||
| 0.08 | 1.20 ± 1.09 | 0.40 ± 0.30 | Minimum distance from center (mm) |
| (0.11; 3.62) | (0; 0.99) | ||
| 0.06 | 1.35 ± 1.78 | 0.08 ± 0.03 | Minimum lesion Feret (mm) |
| (0.03; 4.62) | (0.05; 0.14) | ||
| <0.0001 | 3.97 ± 1.00 | 2.23 ± 1.10 | Maximum lesion Feret (mm) |
| (2.03; 5.17) | (0.80; 4.23) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shmueli, O.; Szeskin, A.; Benhamou, I.; Joskowicz, L.; Shwartz, Y.; Levy, J. Measuring Geographic Atrophy Area Using Column-Based Machine Learning Software on Spectral-Domain Optical Coherence Tomography versus Fundus Auto Fluorescence. Bioengineering 2024, 11, 849. https://doi.org/10.3390/bioengineering11080849
Shmueli O, Szeskin A, Benhamou I, Joskowicz L, Shwartz Y, Levy J. Measuring Geographic Atrophy Area Using Column-Based Machine Learning Software on Spectral-Domain Optical Coherence Tomography versus Fundus Auto Fluorescence. Bioengineering. 2024; 11(8):849. https://doi.org/10.3390/bioengineering11080849
Chicago/Turabian StyleShmueli, Or, Adi Szeskin, Ilan Benhamou, Leo Joskowicz, Yahel Shwartz, and Jaime Levy. 2024. "Measuring Geographic Atrophy Area Using Column-Based Machine Learning Software on Spectral-Domain Optical Coherence Tomography versus Fundus Auto Fluorescence" Bioengineering 11, no. 8: 849. https://doi.org/10.3390/bioengineering11080849
APA StyleShmueli, O., Szeskin, A., Benhamou, I., Joskowicz, L., Shwartz, Y., & Levy, J. (2024). Measuring Geographic Atrophy Area Using Column-Based Machine Learning Software on Spectral-Domain Optical Coherence Tomography versus Fundus Auto Fluorescence. Bioengineering, 11(8), 849. https://doi.org/10.3390/bioengineering11080849