

Automated Heart Rate Detection in Seismocardiograms Using Electrocardiogram-Based Algorithms—A Feasibility Study


Abstract

1. Introduction
- Signal preprocessing (this mainly implies filters and basic mathematical operations), which has signal samples (points) on the input and the output;
- Peak detection, which takes the signal samples and outputs the sequence of peak timestamps, a one-point pro heartbeat, which is then used to calculate HR and HRV parameters.
2. Materials and Methods
- In the first step, HR detection algorithms from ECG diagnostics were identified using a literature and software search.
- In the second step, the precision of these algorithms was tested using a test data set of ECG (gold standard) and SCG data collected in parallel to identify the best methods. The quality of the method is determined by the highest precision in determining the HR (lowest deviation from the gold standard).
- In the third step, the applicability and precision of the best algorithm are tested on real-life data in an experiment under resting conditions (sitting) and light activity (reading) interference.
2.1. Identification of ECG HR Algorithms and Implementation of Signal Preprocessing and Peak Detection Methods
2.1.1. Identification
2.1.2. Signal Preprocessing Pipelines
- to eliminate the low-frequency component with no morphological features below the HR;
- to eliminate high-frequency distortions induced by motion and other sources;
- to eliminate the 50 Hz magnetically induced interference, interference currents in the body, and interference currents in the electrode leads;
- in some cases, to eliminate substantial signal components not directly associated with the primary wave in the signal corresponding to the core fiducial point, usually R-peak (this applies to filters with a short bandpass zone).
2.1.3. Peak Detection Methods
2.2. Application of the Identified Algorithms to the Test Dataset
2.2.1. Evaluation Strategy
- the detected R-peaks on ECG were taken as ground truth;
- the first peak on SCG that hit the particular RR interval was treated as a true positive (TP), while every following peak in the interval was treated as a false positive (FP);
- each RR interval without any peaks on SCG hitting it is treated as a false-negative (FN).
2.2.2. Reference Dataset
2.3. Testing the Best Algorithm in a Real-Life Setting in Rest and Interfering Activity Conditions
2.3.1. Experiment
- 5 min seated, physical rest;
- 5 min seated, reading the book aloud without any additional physical activity.
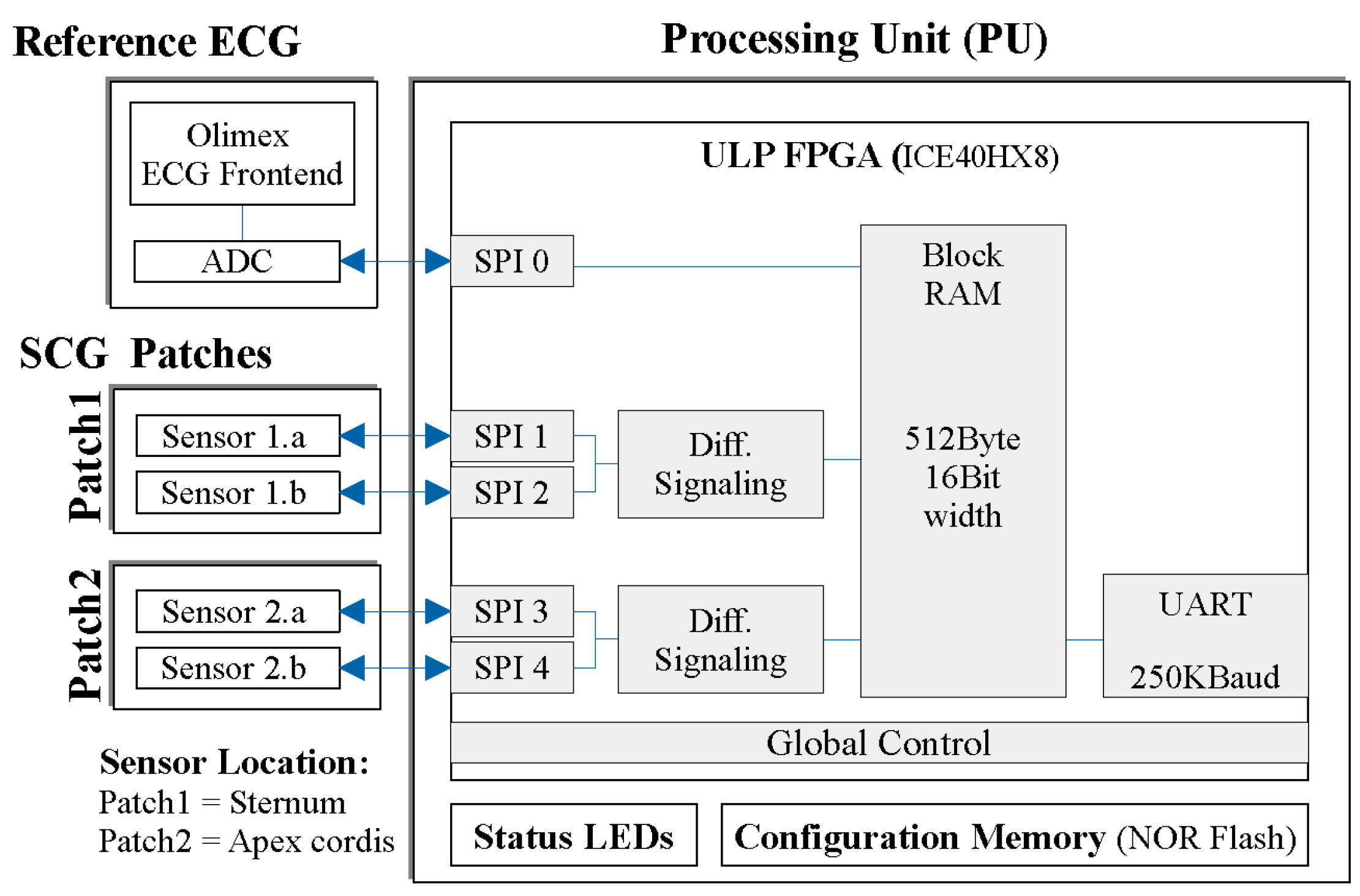
2.3.2. Sensor System
3. Results
3.1. Finding the Best Approach Using the CEBS Dataset
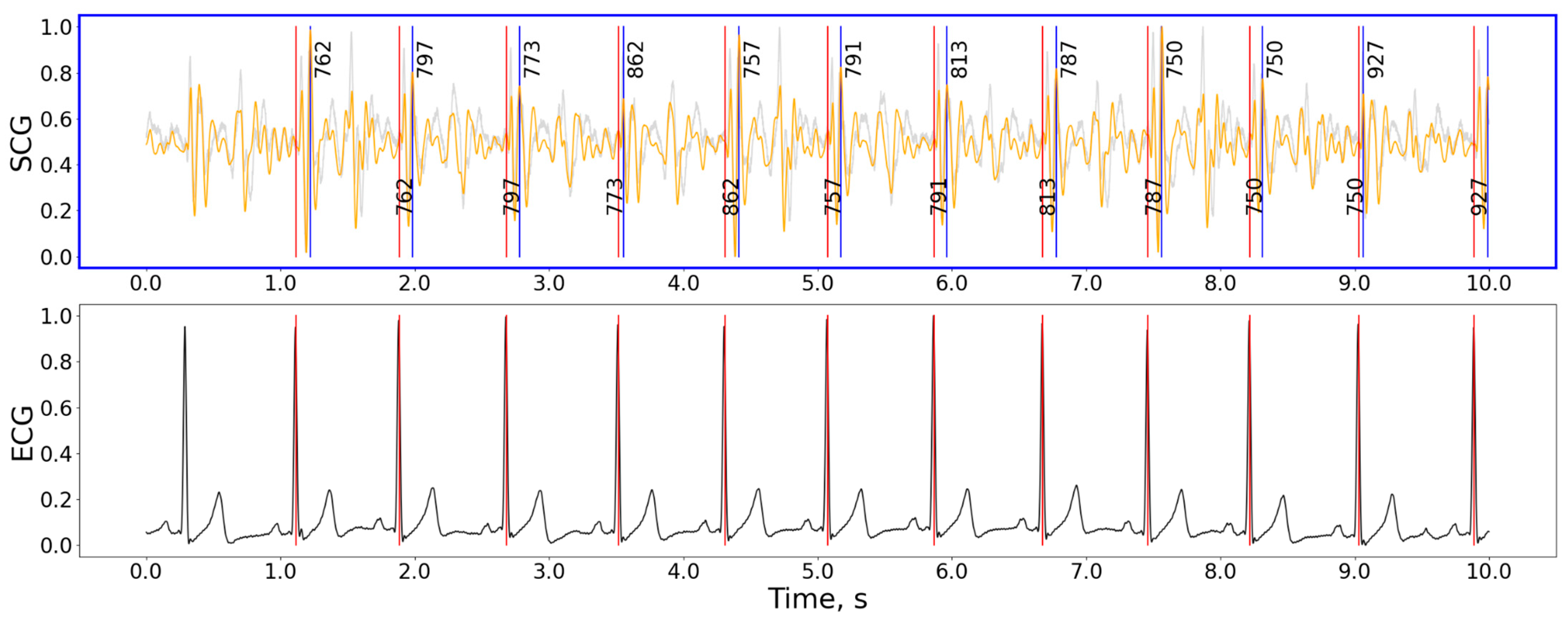
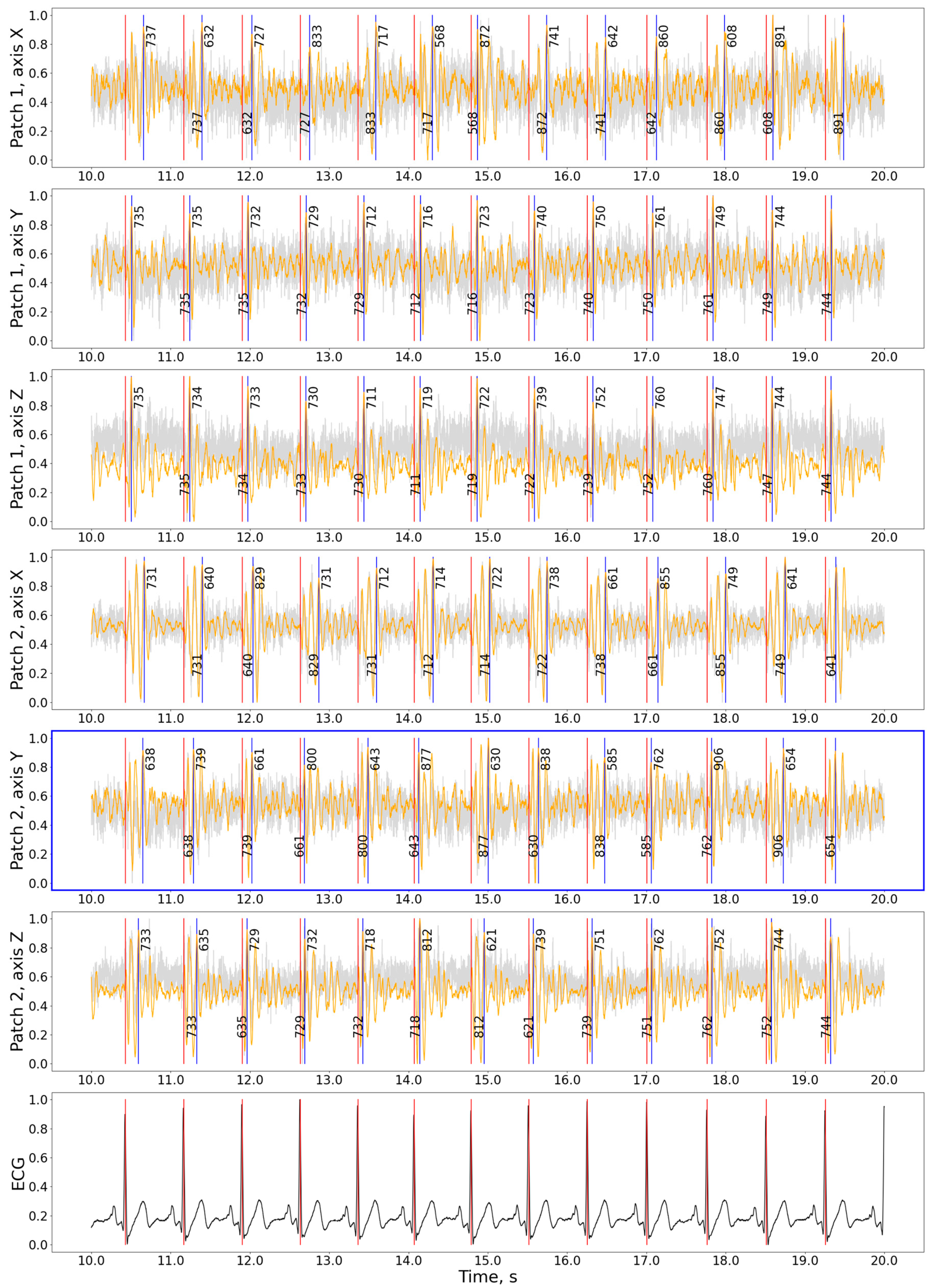
3.2. Testing the Approach on the Experimental Data
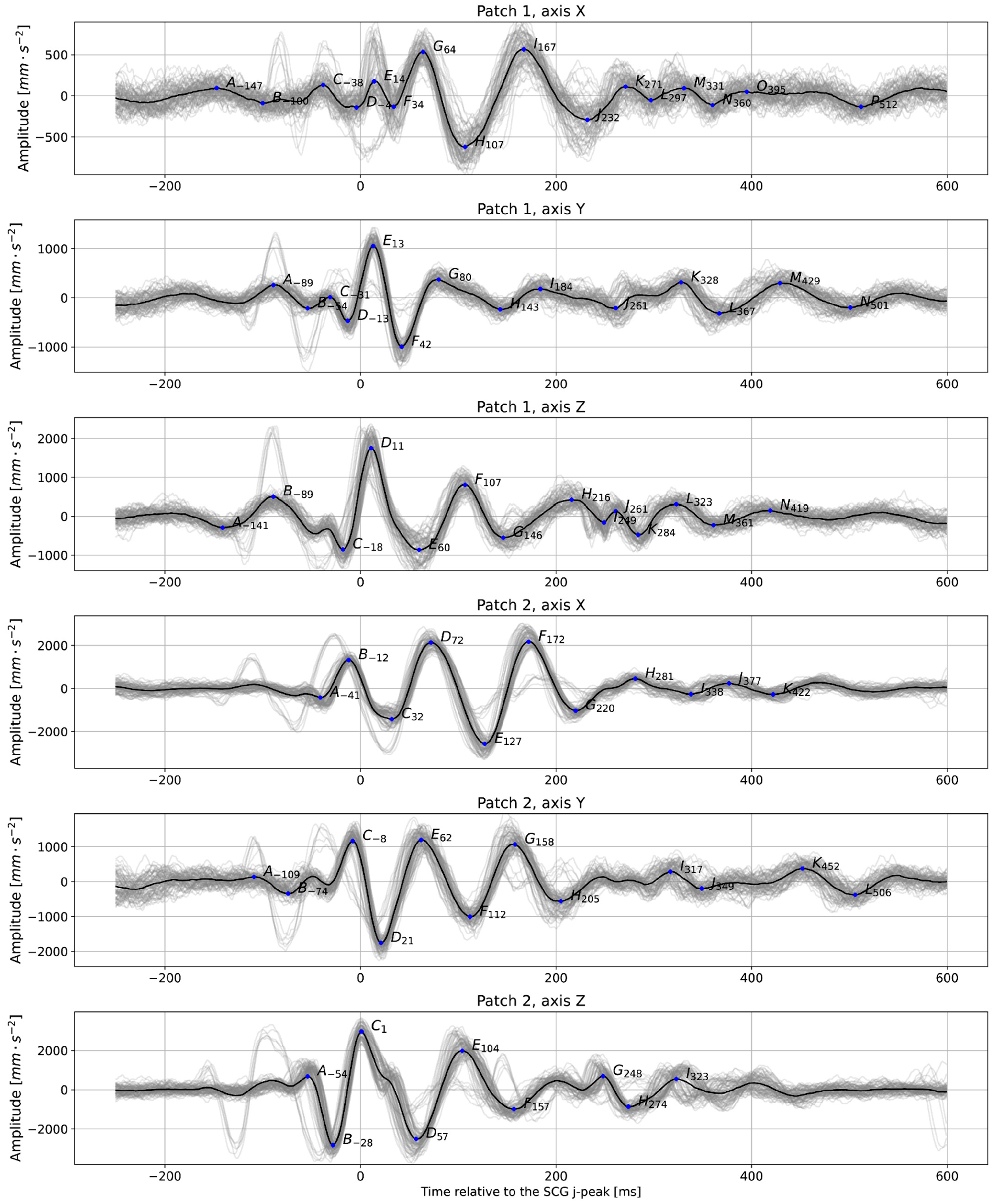
3.3. Analysis of Heartbeat Detection Precision
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Computer Code Availability Statement
References
- Cabanas, A.M.; Fuentes-Guajardo, M.; Latorre, K.; León, D.; Martín-Escudero, P. Skin Pigmentation Influence on Pulse Oximetry Accuracy: A Systematic Review and Bibliometric Analysis. Sensors 2022, 22, 3402. [Google Scholar] [CrossRef]
- Reece, J.D.; Bunn, J.A.; Choi, M.; Navalta, J.W. Assessing Heart Rate Using Consumer Technology Association Standards. Technologies 2021, 9, 46. [Google Scholar] [CrossRef]
- Kułach, A.; Dewerenda, M.; Majewski, M.; Lasek-Bal, A.; Gąsior, Z. 72 Hour Holter Monitoring, 7 Day Holter Monitoring, and 30 Day Intermittent Patient-Activated Heart Rhythm Recording in Detecting Arrhythmias in Cryptogenic Stroke Patients Free from Arrhythmia in a Screening 24 h Holter. Open Med. 2020, 15, 697–701. [Google Scholar] [CrossRef]
- Gordon, J.W. Certain Molar Movements of the Human Body Produced by the Circulation of the Blood. J. Anat. Physiol. 1877, 11, 533–536. [Google Scholar]
- Baevskii, R.M.; Egorov, A.D.; Kazarian, L.A. Seismocardiography. Kardiologiia 1964, 4, 87–89. [Google Scholar]
- Rai, D.; Thakkar, H.K.; Rajput, S.S.; Santamaria, J.; Bhatt, C.; Roca, F. A Comprehensive Review on Seismocardiogram: Current Advancements on Acquisition, Annotation, and Applications. Mathematics 2021, 9, 2243. [Google Scholar] [CrossRef]
- García-González, M.A.; Argelagós-Palau, A.; Fernández-Chimeno, M.; Ramos-Castro, J. A Comparison of Heartbeat Detectors for the Seismocardiogram. In Proceedings of the Computing in Cardiology, Zaragoza, Spain, 22–25 September 2013; pp. 461–464. [Google Scholar]
- Centracchio, J.; Parlato, S.; Esposito, D.; Bifulco, P.; Andreozzi, E. ECG-Free Heartbeat Detection in Seismocardiography Signals via Template Matching. Sensors 2023, 23, 4684. [Google Scholar] [CrossRef]
- Thakkar, H.K.; Sahoo, P.K. Towards Automatic and Fast Annotation of Seismocardiogram Signals Using Machine Learning. IEEE Sens. J. 2020, 20, 2578–2589. [Google Scholar] [CrossRef]
- Milena, Č.; Romano, C.; De Tommasi, F.; Carassiti, M.; Formica, D.; Schena, E.; Massaroni, C. Linear and Non-Linear Heart Rate Variability Indexes from Heart-Induced Mechanical Signals Recorded with a Skin-Interfaced IMU. Sensors 2023, 23, 1615. [Google Scholar] [CrossRef]
- Mafi, M. Signal Processing Methods for Heart Rate Detection Using the Seismocardiogram. Ph.D. Thesis, University of Saskatoon, Saskatoon, SK, Canada, 1 July 2016. [Google Scholar]
- Suresh, P.; Narayanan, N.; Pranav, C.V.; Vijayaraghavan, V. End-to-End Deep Learning for Reliable Cardiac Activity Monitoring Using Seismocardiograms. In Proceedings of the 2020 19th IEEE International Conference on Machine Learning and Applications (ICMLA), Virtual, 14–17 December 2020; pp. 1369–1375. [Google Scholar]
- Tapotee, M.I.; Saha, P.; Mahmud, S.; Alqahtani, A.; Chowdhury, M.E. M2ECG: Wearable Mechanocardiograms to Electrocardiogram Estimation Using Deep Learning. IEEE J. Mag. 2024, 12, 12963–12975. [Google Scholar] [CrossRef]
- Duraj, K.M.; Siecinski, S.; Doniec, R.J.; Piaseczna, N.J.; Kostka, P.S.; Tkacz, E.J. Heartbeat Detection in Seismocardiograms with Semantic Segmentation. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, Scotland, UK, 11–15 July 2022; pp. 662–665. [Google Scholar]
- Mora, N.; Cocconcelli, F.; Matrella, G.; Ciampolini, P. Detection and Analysis of Heartbeats in Seismocardiogram Signals. Sensors 2020, 20, 1670. [Google Scholar] [CrossRef]
- Chan, M.; Gazi, A.H.; Soliman, M.; Richardson, K.L.; Abdallah, C.A.; Ozmen, G.C.; Nikbakht, M.; Inan, O.T. Estimating Heart Rate from Seismocardiogram Signal Using a Novel Deep Dominant Frequency Regressor and Domain Adversarial Training. In Proceedings of the 2022 IEEE Biomedical Circuits and Systems Conference (BioCAS), Taipei, Taiwan, 13–15 October 2022; pp. 158–162. [Google Scholar]
- Chen, Y.; Xu, W.; Zhu, W.; Ma, G.; Chen, X.; Wang, L. Beat-to-Beat Heart Rate Detection Based on Seismocardiogram Using BiLSTM Network. In Proceedings of the 2021 IEEE 20th International Conference on Trust, Security and Privacy in Computing and Communications (TrustCom), Shenyang, China, 20–22 October 2021; pp. 1503–1507. [Google Scholar]
- Choudhary, T.; Bhuyan, M.K.; Sharma, L.N. A Novel Method for Aortic Valve Opening Phase Detection Using SCG Signal. IEEE Sens. J. 2020, 20, 899–908. [Google Scholar] [CrossRef]
- Liu, L.; Yu, D.; Lu, H.; Shan, C.; Wang, W. Camera-Based Seismocardiogram for Heart Rate Variability Monitoring. IEEE J. Biomed. Health Inform. 2024, 28, 2794–2805. [Google Scholar] [CrossRef]
- Neha; Sardana, H.K.; Kanwade, R.; Tewary, S. Arrhythmia Detection and Classification Using ECG and PPG Techniques: A Review. Phys. Eng. Sci. Med. 2021, 44, 1027–1048. [Google Scholar] [CrossRef]
- Sahoo, S.; Dash, M.; Behera, S.; Sabut, S. Machine Learning Approach to Detect Cardiac Arrhythmias in ECG Signals: A Survey. Innov. Res. Biomed. Eng. 2020, 41, 185–194. [Google Scholar] [CrossRef]
- Murat, F.; Yildirim, O.; Talo, M.; Baloglu, U.B.; Demir, Y.; Acharya, U.R. Application of Deep Learning Techniques for Heartbeats Detection Using ECG Signals-Analysis and Review. Comput. Biol. Med. 2020, 120, 103726. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Niskanen, J.-P.; Lipponen, J.A.; Ranta-aho, P.O.; Karjalainen, P.A. Kubios HRV—Heart Rate Variability Analysis Software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Carreiras, C.; Alves, A.P.; Lourenço, A.; Canento, F.; Silva, H.; Fred, A. Biosppy: Biosignal Processing in Python. Accessed 2015, 3, 2018. [Google Scholar]
- van Gent, P.; Farah, H.; van Nes, N.; van Arem, B. HeartPy: A Novel Heart Rate Algorithm for the Analysis of Noisy Signals. Transp. Res. Part F Traffic Psychol. Behav. 2019, 66, 368–378. [Google Scholar] [CrossRef]
- Bartels, R.; Peçanha, T. HRV: A Pythonic Package for Heart Rate Variability Analysis. J. Open Source Softw. 2020, 5, 1867. [Google Scholar] [CrossRef]
- Makowski, D.; Pham, T.; Lau, Z.J.; Brammer, J.C.; Lespinasse, F.; Pham, H.; Schölzel, C.; Chen, S.H.A. NeuroKit2: A Python Toolbox for Neurophysiological Signal Processing. Behav. Res. Methods 2021, 53, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Gomes, P.; Margaritoff, P.; Plácido da Silva, H. pyHRV: Development and Evaluation of an Open-Source Python Toolbox for Heart Rate Variability (HRV). In Proceedings of the International Conference on Electrical, Electronic and Computing Engineering, London, UK, 3–5 July 2019. [Google Scholar]
- Gabrieli, G.; Azhari, A.; Esposito, G. PySiology: A Python Package for Physiological Feature Extraction; Springer: Singapore, 2019; ISBN 9789811389498. [Google Scholar]
- Kirk, P.A.; Davidson Bryan, A.; Garfinkel, S.N.; Robinson, O.J. RapidHRV: An Open-Source Toolbox for Extracting Heart Rate and Heart Rate Variability. PeerJ 2022, 10, e13147. [Google Scholar] [CrossRef] [PubMed]
- Legrand, N.; Allen, M. Systole: A Python Package for Cardiac Signal Synchrony and Analysis. J. Open Source Softw. 2022, 7, 3832. [Google Scholar] [CrossRef]
- van Rossum, G.; de Boer, J. Interactively Testing Remote Servers Using the Python Programming Language. CWI Q. 1991, 4, 283–304. [Google Scholar]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, 3, 230–236. [Google Scholar] [CrossRef]
- Hamilton, P. Open Source ECG Analysis. In Computers in Cardiology; IEEE: New York, NY, USA, 2002; pp. 101–104. [Google Scholar]
- Elgendi, M.; Jonkman, M.; De Boer, F. Frequency Bands Effects on QRS Detection. Biosignals 2010, 2003, 431. [Google Scholar]
- Lourenco, A.; Plácido da Silva, H.; Leite, P.; Lourenço, R.; Fred, A. Real Time Electrocardiogram Segmentation for Finger Based ECG Biometrics. In Proceedings of the International Conference on Bio-Inspired Systems and Signal Processing (BIOSIGNALS-2012), Vilamoura, Algarve, Portugal, 1–4 February 2012; pp. 49–54. [Google Scholar]
- Emrich, J.; Koka, T.; Wirth, S.; Muma, M. Accelerated Sample-Accurate R-Peak Detectors Based on Visibility Graphs. In Proceedings of the 2023 31st European Signal Processing Conference (EUSIPCO), Helsinki, Finland, 4–8 September 2023; pp. 1090–1094. [Google Scholar]
- Zong, W.; Heldt, T.; Moody, G.B.; Mark, R.G. An Open-Source Algorithm to Detect Onset of Arterial Blood Pressure Pulses. In Proceedings of the Computers in Cardiology, Thessaloniki, Greece, 21–24 September 2003; pp. 259–262. [Google Scholar]
- Martinez, J.P.; Almeida, R.; Olmos, S.; Rocha, A.P.; Laguna, P. A Wavelet-Based ECG Delineator: Evaluation on Standard Databases. IEEE Trans. Biomed. Eng. 2004, 51, 570–581. [Google Scholar] [CrossRef]
- Christov, I.I. Real Time Electrocardiogram QRS Detection Using Combined Adaptive Threshold. Biomed. Eng. Online 2004, 3, 28. [Google Scholar] [CrossRef]
- Gamboa, H. Multi-Modal Behavioral Biometrics Based on HCI and Electrophysiology. Ph.D. Thesis, Universidade Tecnica de Lisboa Instituto Superior Tecnico, Lisboa, Portugal, 2008. [Google Scholar]
- Manikandan, M.S.; Soman, K.P. A Novel Method for Detecting R-Peaks in Electrocardiogram (ECG) Signal. Biomed. Signal Process. Control 2012, 7, 118–128. [Google Scholar] [CrossRef]
- Kalidas, V.; Tamil, L. Real-Time QRS Detector Using Stationary Wavelet Transform for Automated ECG Analysis; IEEE Computer Society: Washington, DC, USA, 2017; pp. 457–461. [Google Scholar]
- Nabian, M.; Yin, Y.; Wormwood, J.; Quigley, K.S.; Barrett, L.F.; Ostadabbas, S. An Open-Source Feature Extraction Tool for the Analysis of Peripheral Physiological Data. IEEE J. Transl. Eng. Health Med. 2018, 6, 2800711. [Google Scholar] [CrossRef] [PubMed]
- Sadhukhan, D.; Mitra, M. R-Peak Detection Algorithm for Ecg Using Double Difference And RR Interval Processing. Procedia Technol. 2012, 4, 873–877. [Google Scholar] [CrossRef]
- Gutiérrez-Rivas, R.; García, J.J.; Marnane, W.P.; Hernández, Á. Novel Real-Time Low-Complexity QRS Complex Detector Based on Adaptive Thresholding. IEEE Sens. J. 2015, 15, 6036–6043. [Google Scholar] [CrossRef]
- Rodrigues, T.; Samoutphonh, S.; Silva, H.; Fred, A. A Low-Complexity R-Peak Detection Algorithm with Adaptive Thresholding for Wearable Devices. In Proceedings of the 2020 25th International Conference on Pattern Recognition (ICPR), Milan, Italy, 10–15 January 2021; pp. 1–8. [Google Scholar]
- Koka, T.; Muma, M. Fast and Sample Accurate R-Peak Detection for Noisy ECG Using Visibility Graphs. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2022, 2022, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H. Effect of Measurement Duration on Accuracy of Pulse-Counting. Ergonomics 2013, 56, 1940–1944. [Google Scholar] [CrossRef] [PubMed]
- Drobczyk, M.; Lubken, A.; Strowik, C.; Albrecht, U.-V.; Rust, J.; Beringer, J.; Kulau, U. A Wireless Communication Network With a Ballistocardiography Experiment on the ISS: Scenario, Components and Preflight Demonstration. IEEE J. Radio Freq. Identif. 2022, 6, 258–268. [Google Scholar] [CrossRef]
- Kulau, U.; Rust, J.; Albrecht, U.V. Demo: BCG Measurement by Differential Sensing in Real-Time; IEEE: New York, NY, USA, 2022; pp. 75–78. [Google Scholar]
- Matsakis, N.D.; Klock, F.S. The Rust Language. ACM SIGAda Ada Lett. 2014, 34, 103–104. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Codename | Source | Description |
|---|---|---|
| neurokit | Neurokit2 package [27] | 0.5 Hz high-pass Butterworth filter (order = 5), followed by powerline filtering (50 Hz) |
| biosppy | Biosppy package [24] | a finite impulse response filter with the order defined as [0.3 × sampling rate] with bandpass cut-off frequencies 3 and 45 Hz |
| pantompkins1985 | Pan and Tompkins (1985) [33] | a 1-order bandpass Butterworth filter with 5 and 15 Hz cut-off frequencies |
| hamilton2002 | Hamilton et al. (2002) [34] | a combination of 1-order Butterworth 8 Hz high-pass and 16 Hz low-pass filters |
| elgendi2010 | Elgendi et al. (2010) [35] | a 2-order bandpass Butterworth filter with 8 and 20 Hz cut-off frequencies |
| current_paper | Current paper | a 4-order bandpass Butterworth filter with 5 and 35 Hz cut-off frequencies |
| engzeemod2012 | Lourenco et al. (2012) [36] | a 5-order bandstop Butterworth filter with 48 and 52 Hz cut-off frequencies |
| Codename | Source | Description |
|---|---|---|
| neurokit | Neurokit2 package [27] | QRS complexes are detected based on the steepness of the absolute gradient of the ECG signal; subsequently, R-peaks are detected as local maxima in the QRS complexes |
| pantompkins1985 | Pan and Tompkins (1985) [33] | an algorithm based on dynamically changing thresholds |
| hamilton2002 | Hamilton (2002) [34] | adaptive thresholding |
| zong2003 | Zong et al. (2003) [38] | a low-pass filter, slope sum function, and a decision rule |
| martinez2004 | Martinez et al. (2004) [39] | combined adaptive filters |
| christov2004 | Christov et al. (2004) [40] | two parallel running algorithms with a combination of three adaptive thresholds: steep-slope, integrating threshold for high-frequency signal components, and beat expectation threshold |
| gamboa2008 | Gamboa et al. (2008) [41] | the first derivative and restrictions on possible RR lengths |
| elgendi2010 | Elgendi et al. (2010) [35] | potential blocks generated based on two moving averages and the following thresholding |
| engzeemod2012 | Lourenco et al. (2012) [36] | 5-s intervals to determine adaptive threshold linearly changing in defined intervals |
| manikandan2012 | Manikandan and Soman (2012) [42] | Shannon energy envelope (SEE) |
| kalidas2017 | Kalidas and Tamil (2017) [43] | stationary wavelet transform (SWT) |
| nabian2018 | Nabian et al. (2018) [44] | Pan-Tompkins inspired algorithm with moving windows and highest peak detection |
| rodrigues2021 | Sadhukhan and Mitra (2012) [45], Gutiérrez-Rivas et al. (2015) [46], and Rodrigues et al. (2021) [47] | double derivative, squaring, moving window integration as preprocessing and a finite-state-machine for decision-making |
| emrich2023 | Koka et al. (2022) [48] and Emrich et al. (2023) [37] | the fast natural visibility graph (FastNVG) algorithm based on the visibility graph detector; the algorithm transforms the ECG into a graph representation and extracts exact R-peak positions using graph metrics |
| promac | Neurokit2 package [27] | combination of several R-peak detectors in a probabilistic way: for a given peak detector, the binary signal representing the peak locations is convolved with a Gaussian distribution, resulting in a probabilistic representation of each peak location; the procedure is repeated for all selected methods, accumulating the resulting signals; a threshold is used to accept or reject the peak locations |
| Rank | Detection Method | Preprocessing Method | HR (SCG), bpm | HR (ECG), bpm | HR diff, bpm | Precision | Recall | F1-Score |
|---|---|---|---|---|---|---|---|---|
| 1 | nabian2018 | hamilton2002 | 70.8 ± 9.8 | 70.1 ± 9.8 | 0.9 ± 2.4 | 98.7 ± 3.1 | 99.7 ± 0.9 | 0.992 ± 0.018 |
| 2 | neurokit | hamilton2002 | 85.0 ± 21.5 | 70.1 ± 9.8 | 15.0 ± 21.0 | 85.6 ± 17.0 | 99.4 ± 1.5 | 0.91 ± 0.11 |
| 3 | elgendi2010 | hamilton2002 | 86.0 ± 22.0 | 70.2 ± 9.8 | 15.8 ± 20.2 | 84.3 ± 16.7 | 98.9 ± 2.1 | 0.901 ± 0.106 |
| Rank | Detection Method | Preprocessing Method | HR (SCG), bpm | HR (ECG), bpm | HR diff, bpm | Precision | Recall | F1-Score |
|---|---|---|---|---|---|---|---|---|
| 1 | nabian2018 | hamilton2002 | 70.8 ± 9.8 | 70.1 ± 9.8 | 0.9 ± 2.4 | 98.7 ± 3.1 | 99.7 ± 0.9 | 0.992 ± 0.018 |
| 2 | nabian2018 | pustozerov2024 | 69.9 ± 9.5 | 70.1 ± 9.8 | 0.9 ± 2.1 | 98.6 ± 4.5 | 98.3 ± 4.5 | 0.985 ± 0.043 |
| 3 | nabian2018 | elgendi2010 | 71.3 ± 10.1 | 70.1 ± 9.8 | 1.4 ± 3.6 | 92.0 ± 9.7 | 93.4 ± 9.4 | 0.926 ± 0.093 |
| 4 | nabian2018 | pantompkins1985 | 71.2 ± 10.0 | 70.1 ± 9.8 | 1.5 ± 3.9 | 98.0 ± 4.7 | 99.4 ± 1.8 | 0.986 ± 0.029 |
| 5 | nabian2018 | biosppy | 70.3 ± 9.5 | 70.8 ± 9.4 | 1.8 ± 3.9 | 98.3 ± 4.5 | 97.7 ± 5.6 | 0.979 ± 0.045 |
| 6 | nabian2018 | none | 70.3 ± 9.5 | 71.5 ± 9.9 | 2.5 ± 6.7 | 98.0 ± 4.8 | 96.7 ± 8.4 | 0.972 ± 0.061 |
| 7 | nabian2018 | engzeemod2012 | 70.3 ± 9.5 | 71.7 ± 10.0 | 2.7 ± 7.2 | 98.1 ± 4.8 | 96.6 ± 8.8 | 0.971 ± 0.063 |
| 8 | nabian2018 | neurokit | 71.1 ± 9.6 | 71.4 ± 9.8 | 3.2 ± 6.8 | 97.0 ± 5.3 | 96.8 ± 8.3 | 0.967 ± 0.060 |
| Subject | State | Best Patch and Axes | HR (SCG), bpm | HR (ECG), bpm | HR diff, bpm | p-Value | Precision | Recall | F1-Score |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Rest | Patch1_z | 67.4 ± 0.7 | 67.4 ± 0.6 | 0.1 ± 0.1 | 0.733 | 100.0 ± 0.0 | 100.0 ± 0.0 | 1.0 ± 0.0 |
| 1 | Interference | Patch1_y | 72.4 ± 1.8 | 76.6 ± 1.1 | 4.2 ± 1.1 | 0.001 | 89.2 ± 3.9 | 83.9 ± 3.7 | 0.864 ± 0.037 |
| 2 | Rest | Patch0_z | 83.5 ± 2.7 | 83.5 ± 2.7 | 0.0 ± 0.0 | 0.071 | 100.0 ± 0.0 | 100.0 ± 0.0 | 1.0 ± 0.0 |
| 2 | Interference | Patch1_z | 82.2 ± 2.9 | 91.8 ± 1.3 | 9.7 ± 2.5 | 0.001 | 98.0 ± 1.2 | 87.7 ± 3.6 | 0.926 ± 0.025 |
| 3 | Rest | Patch1_x | 68.6 ± 2.1 | 68.3 ± 1.6 | 0.3 ± 0.6 | 0.332 | 99.7 ± 0.6 | 100.0 ± 0.0 | 0.999 ± 0.003 |
| 3 | Interference | Patch1_x | 73.6 ± 1.1 | 79.1 ± 1.4 | 5.5 ± 1.9 | 0.003 | 92.5 ± 2.3 | 86.2 ± 2.0 | 0.892 ± 0.018 |
| All | Rest | various | 73.2 ± 7.8 | 73.1 ± 7.8 | 0.1 ± 0.3 | 0.278 | 99.9 ± 0.4 | 100.0 ± 0.0 | 1.000 ± 0.002 |
| All | Interference | various | 76.1 ± 4.9 | 82.5 ± 7.0 | 6.5 ± 3.0 | <0.001 | 93.2 ± 4.5 | 86.0 ± 3.4 | 0.894 ± 0.036 |
| All | Both | various | 74.6 ± 6.6 | 77.8 ± 8.7 | 3.3 ± 3.8 | <0.001 | 96.6 ± 4.6 | 93.0 ± 7.5 | 0.947 ± 0.059 |
| N | Paper | Method | Metric and Value |
|---|---|---|---|
| 1 | Current paper | moving window and simple peak detection | sensitivity, 99.7 ± 0.9%; precision, 98.7 ± 3.1%; F1-score, 0.992 ± 0.018; HR diff, bpm = 0.9 ± 2.4 |
| 2 | Prithvi et al. [12] | convolutional neural network (CNN) | sensitivity, 98%; precision, 98% |
| 3 | Mora et al. [15] | unsupervised segmentation | sensitivity, 98.5 ± 1.2%; precision, 98.6 ± 1.2%; specificity, 98.6 ± 1.2% |
| 4 | Duraj et al. [14] | U-Net-based semantic segmentation | sensitivity, 99.9%; precision, 97% |
| 5 | Chen et al. [17] | BiLSTM network | sensitivity, 97%; precision, 98% |
| 6 | Choudhary et al. [18] | data-adaptive variational mode decomposition (VMD) | sensitivity, 97.4%; precision, 97.4%; accuracy, 95.1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pustozerov, E.; Kulau, U.; Albrecht, U.-V. Automated Heart Rate Detection in Seismocardiograms Using Electrocardiogram-Based Algorithms—A Feasibility Study. Bioengineering 2024, 11, 596. https://doi.org/10.3390/bioengineering11060596
Pustozerov E, Kulau U, Albrecht U-V. Automated Heart Rate Detection in Seismocardiograms Using Electrocardiogram-Based Algorithms—A Feasibility Study. Bioengineering. 2024; 11(6):596. https://doi.org/10.3390/bioengineering11060596
Chicago/Turabian StylePustozerov, Evgenii, Ulf Kulau, and Urs-Vito Albrecht. 2024. "Automated Heart Rate Detection in Seismocardiograms Using Electrocardiogram-Based Algorithms—A Feasibility Study" Bioengineering 11, no. 6: 596. https://doi.org/10.3390/bioengineering11060596
APA StylePustozerov, E., Kulau, U., & Albrecht, U.-V. (2024). Automated Heart Rate Detection in Seismocardiograms Using Electrocardiogram-Based Algorithms—A Feasibility Study. Bioengineering, 11(6), 596. https://doi.org/10.3390/bioengineering11060596