
Healing of Extraction Sites after Alveolar Ridge Preservation Using Advanced Platelet-Rich Fibrin: A Retrospective Study


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients Selection
- Patients over 18 years of age.
- Maxillary or mandibular posterior teeth (first and second molars) that cannot be retained due to severe caries, chronic periapical periodontitis, failed endodontic treatments, or fatigue tooth fractures.
- At least 2 or more bone plates exist at the extraction site.
- Patients without serious systemic diseases (ASA I and ASA II).
- Good compliance.
- Patients who want implant restorations.
- Patients in whom the insertion of implants was performed immediately after the extraction.
- Severe hypertension, diabetes, kidney, and liver disease.
- Patients taking anticoagulants, systemic steroid treatment, or systemic bisphosphonates.
- Smokers (>10 cigarettes a day), alcoholics, drug users.
- Pregnant or lactating patients.
- Patients with previous radiation therapy in the surgical area.
- Bad oral hygiene.
- Acute infection of the tooth that will be extracted.
2.3. Treatment Procedures
2.3.1. Preoperative Work-Up
2.3.2. Preparation of A-PRF Membranes
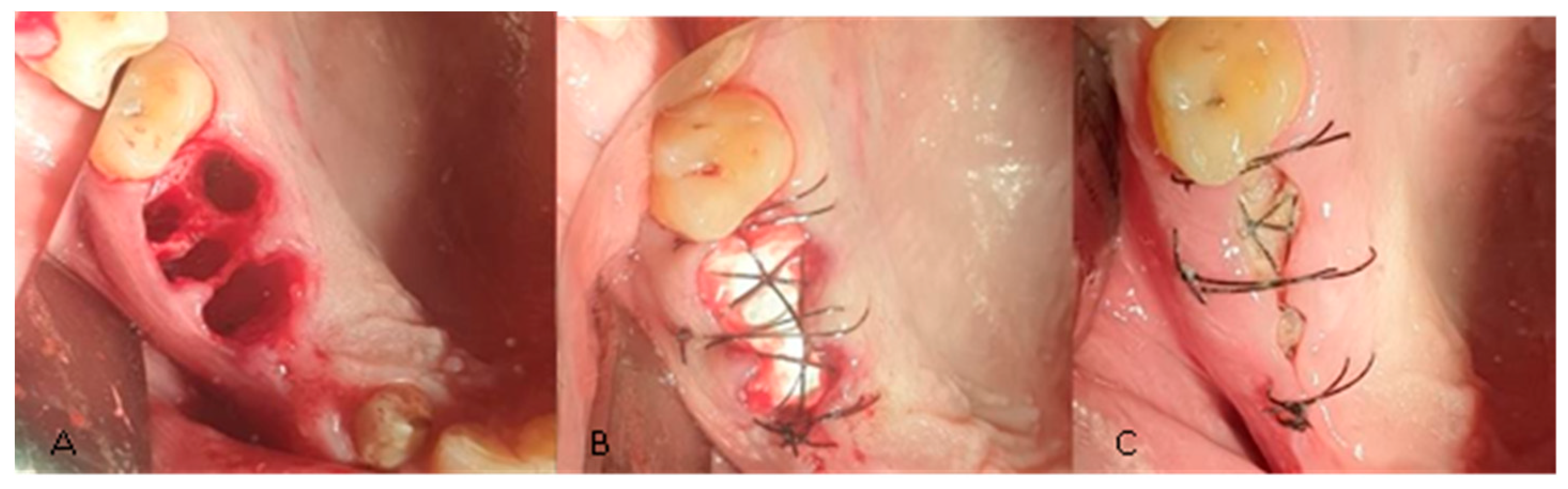
2.3.3. Surgical Procedures
2.3.4. Postoperative Protocol
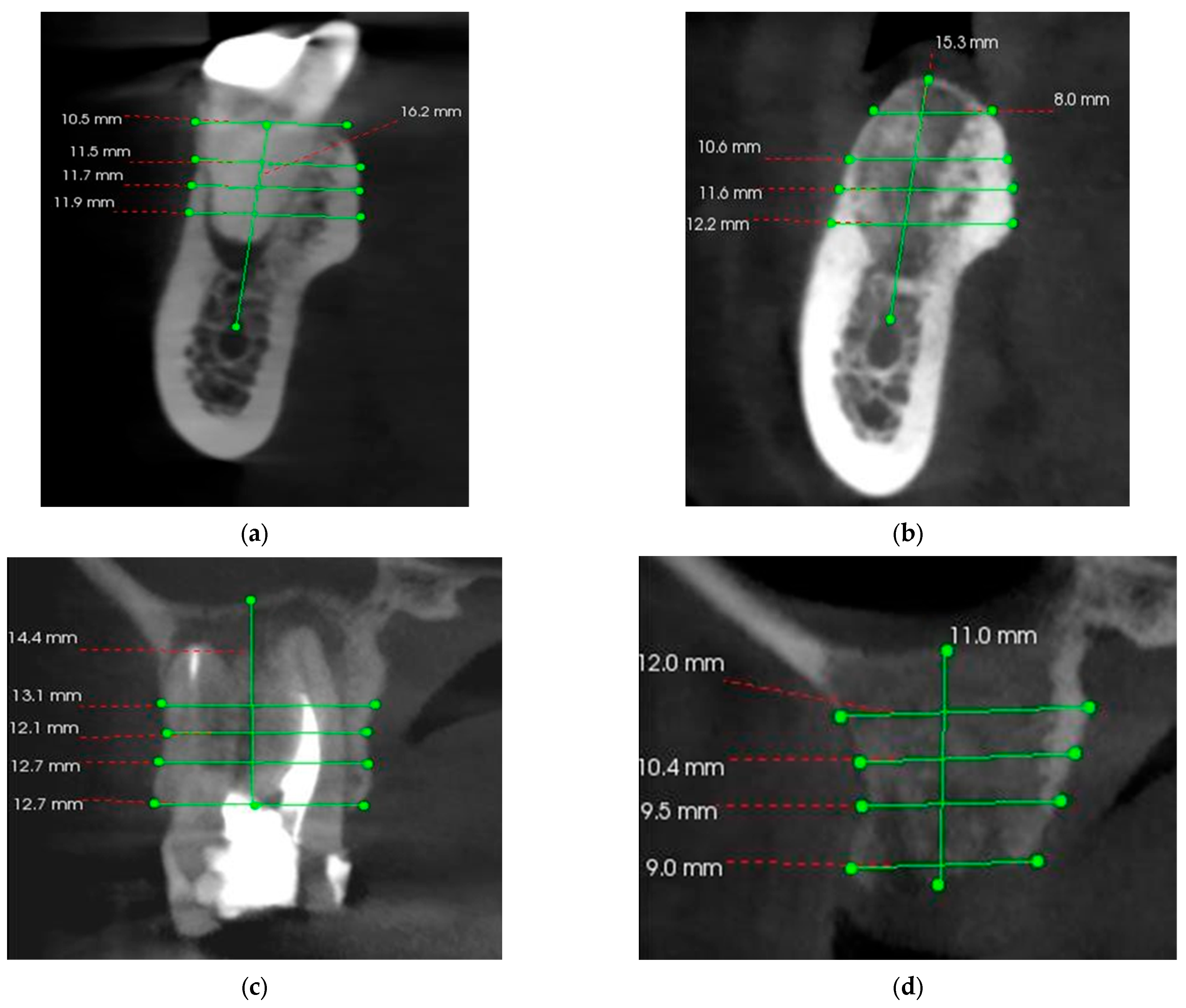
2.4. CBCT Evaluation
2.5. Statistical Analysis
3. Results
3.1. Baseline Data
3.2. Clinical Outcomes
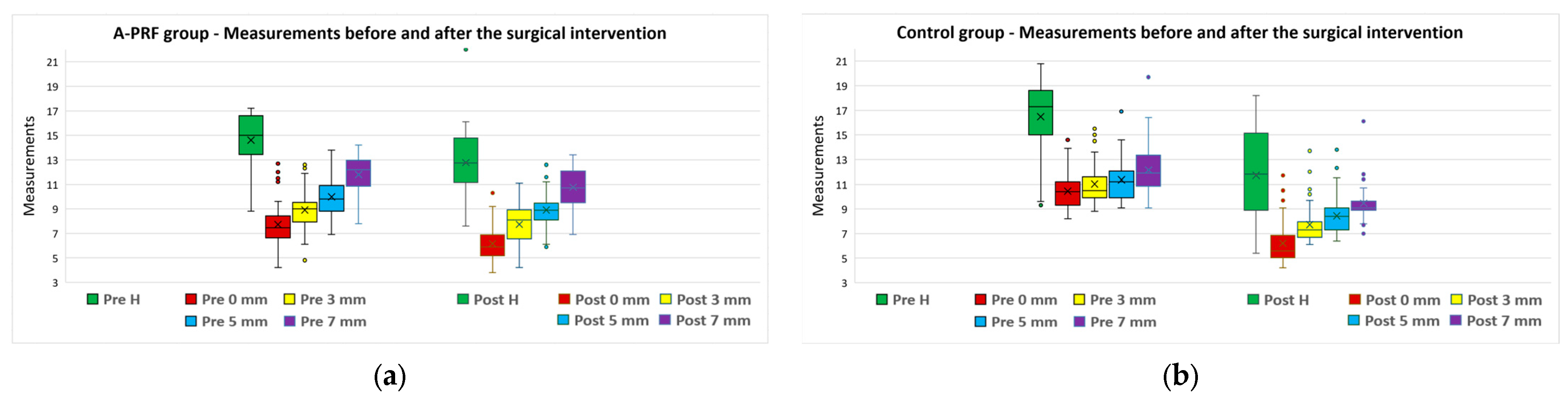
3.3. CBCT Analysis
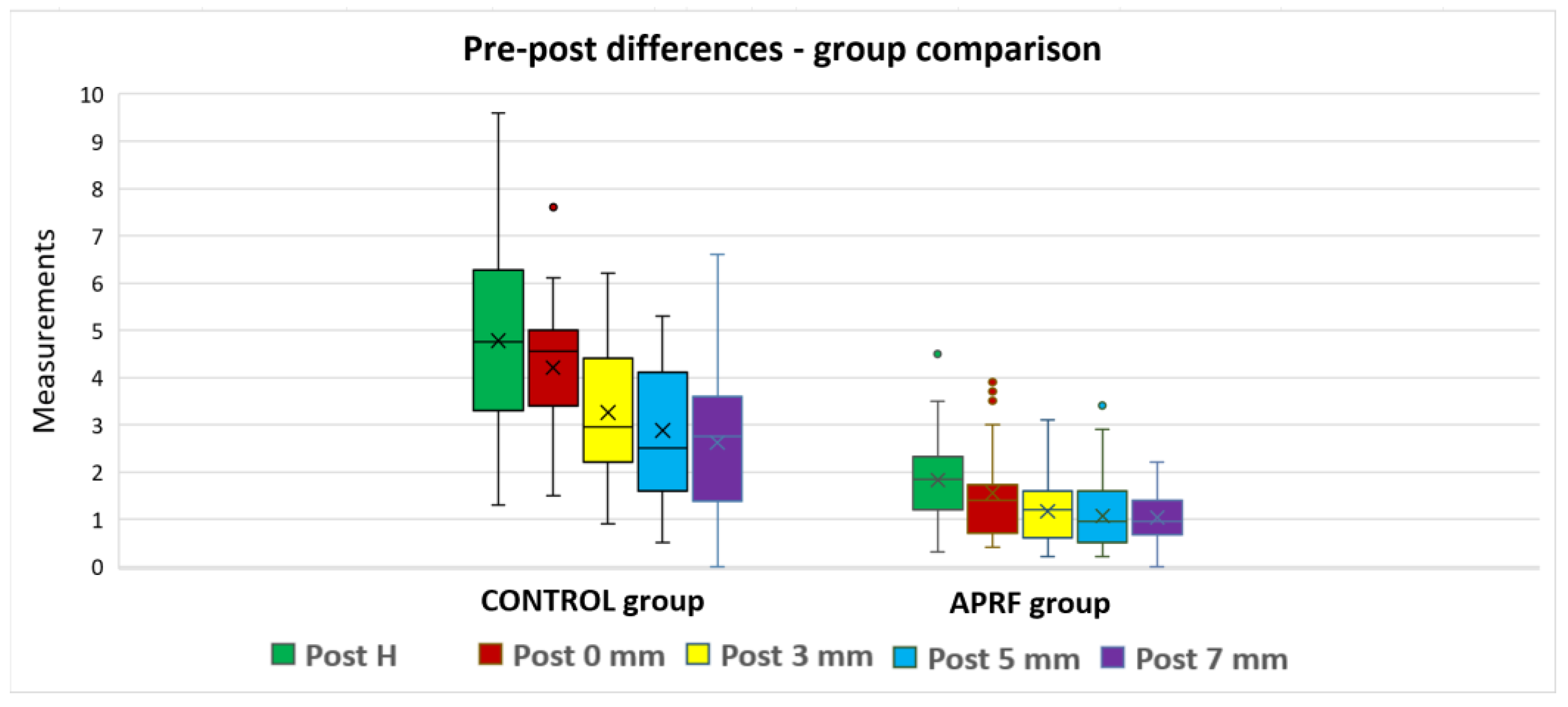
3.4. A-PRF/Control Subgroups Analysis
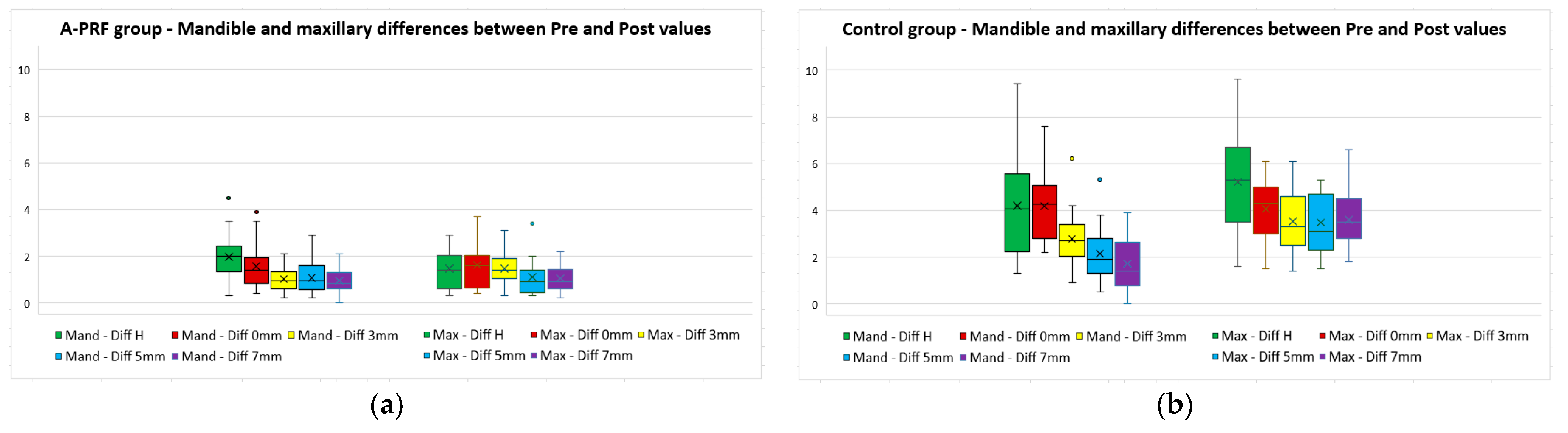
3.5. Maxillary/Mandible Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Araújo, M.G.; da Silva, J.C.C.; de Mendonça, A.F.; Lindhe, J. Ridge alterations following grafting of fresh extraction sockets in man. A randomized clinical trial. Clin. Oral Implants Res. 2015, 26, 407–412. [Google Scholar] [CrossRef]
- Avila-Ortiz, G.; Elangovan, S.; Kramer, K.W.; Blanchette, D.; Dawson, D.V. Effect of alveolar ridge preservation after tooth extraction: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 950–958. [Google Scholar] [CrossRef]
- Barootchi, S.; Tavelli, L.; Majzoub, J.; Stefanini, M.; Wang, H.L.; Avila-Ortiz, G. Alveolar ridge preservation: Complications and cost-effectiveness. Periodontology 2000 2023, 92, 235–262. [Google Scholar] [CrossRef]
- Alenazi, A.; Alotaibi, A.A.; Aljaeidi, Y.; Alqhtani, N.R. The need for socket preservation: A systematic review. J. Med. Life 2022, 15, 309–312. [Google Scholar] [CrossRef]
- Windisch, P.; Orban, K.; Salvi, G.E.; Sculean, A.; Molnar, B. Vertical-guided bone regeneration with a titanium-reinforced d-PTFE membrane utilizing a novel split-thickness flap design: A prospective case series. Clin. Oral Investig. 2021, 25, 2969–2980. [Google Scholar] [CrossRef]
- Pagni, G.; Pellegrini, G.; Giannobile, W.V.; Rasperini, G. Postextraction alveolar ridge preservation: Biological basis and treatments. Int. J. Dent. 2012, 2012, 151030. [Google Scholar] [CrossRef]
- Trombelli, L.; Farina, R.; Marzola, A.; Bozzi, L.; Liljenberg, B.; Lindhe, J. Modeling and remodeling of human extraction sockets. J. Clin. Periodontol. 2008, 35, 630–639. [Google Scholar] [CrossRef]
- Walker, C.J.; Prihoda, T.J.; Mealey, B.L.; Lasho, D.J.; Noujeim, M.; Huynh-Ba, G. Evaluation of Healing at Molar Extraction Sites with and without Ridge Preservation: A Randomized Controlled Clinical Trial. J. Periodontol. 2017, 88, 241–249. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implants Res. 2012, 23 (Suppl. S5), 1–21. [Google Scholar] [CrossRef]
- Cosyn, J.; Cleymaet, R.; De Bruyn, H. Predictors of Alveolar Process Remodeling Following Ridge Preservation in High-Risk Patients. Clin. Implant. Dent. Relat. Res. 2016, 18, 226–233. [Google Scholar] [CrossRef]
- Yang, S.; Li, Y.; Liu, C.; Wu, Y.; Wan, Z.; Shen, D. Pathogenesis and treatment of wound healing in patients with diabetes after tooth extraction. Front. Endocrinol. 2022, 13, 949535. [Google Scholar] [CrossRef]
- Shah, F.A.; Sayardoust, S.; Omar, O.; Thomsen, P.; Palmquist, A. Does Smoking Impair Bone Regeneration in the Dental Alveolar Socket? Calcif. Tissue Int. 2019, 105, 619–629. [Google Scholar] [CrossRef]
- Saldanha, J.B.; Casati, M.Z.; Neto, F.H.; Sallum, E.A.; Nociti, F.H., Jr. Smoking may affect the alveolar process dimensions and radiographic bone density in maxillary extraction sites: A prospective study in humans. J. Oral Maxillofac. Surg. 2006, 64, 1359–1365. [Google Scholar] [CrossRef]
- Campos, J.M.; Prati, A.J.; Cirano, F.R.; Pimentel, S.P.; Pastore, G.P.; Pecorari, V.G.; Ribeiro, F.V.; Casati, M.Z.; Casarin, R.C. Smoking Modulates Gene Expression of Type I Collagen, Bone Sialoprotein, and Osteocalcin in Human Alveolar Bone. J. Oral Maxillofac. Surg. 2015, 73, 2123–2131. [Google Scholar] [CrossRef]
- Moy, P.K.; Aghaloo, T. Risk factors in bone augmentation procedures. Periodontology 2000 2019, 81, 76–90. [Google Scholar] [CrossRef]
- Alrayyes, Y.; Aloraini, S.; Alkhalaf, A.; Aljasser, R. Soft-Tissue Healing Assessment after Extraction and Socket Preservation Using Platelet-Rich Fibrin (PRF) in Smokers: A Single-Blinded, Randomized, Controlled Clinical Trial. Diagnostics 2022, 12, 2403. [Google Scholar] [CrossRef]
- Politis, C.; Schoenaers, J.; Jacobs, R.; Agbaje, J.O. Wound Healing Problems in the Mouth. Front. Physiol. 2016, 7, 507. [Google Scholar] [CrossRef]
- Barone, A.; Ricci, M.; Tonelli, P.; Santini, S.; Covani, U. Tissue changes of extraction sockets in humans: A comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin. Oral Implants Res. 2013, 24, 1231–1237. [Google Scholar] [CrossRef]
- Mardas, N.; Macbeth, N.; Donos, N.; Jung, R.E.; Zuercher, A.N. Is alveolar ridge preservation an overtreatment? Periodontology 2000 2023, 93, 289–308. [Google Scholar] [CrossRef]
- Van der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef]
- Araújo, M.G.; Dias, D.R.; Matarazzo, F. Anatomical characteristics of the alveolar process and basal bone that have an effect on socket healing. Periodontology 2000 2023, 93, 277–288. [Google Scholar] [CrossRef]
- Wei, Y.; Xu, T.; Zhao, L.; Hu, W.; Chung, K.H. Ridge preservation in maxillary molar extraction sites with severe periodontitis: A prospective observational clinical trial. Clin. Oral Investig. 2022, 26, 2391–2399. [Google Scholar] [CrossRef]
- Couso-Queiruga, E.; Stuhr, S.; Tattan, M.; Chambrone, L.; Avila-Ortiz, G. Post-extraction dimensional changes: A systematic review and meta-analysis. J. Clin. Periodontol. 2021, 48, 126–144. [Google Scholar] [CrossRef]
- Zhang, H.; Wei, Y.; Xu, T.; Zhen, M.; Wang, C.; Han, Z.; Hu, W.; Chung, K.H. Assessment of soft and hard tissue characteristics of ridge preservation at molar extraction sites with severe periodontitis: A randomized controlled trial. BMC Oral Health 2022, 22, 511. [Google Scholar] [CrossRef]
- Meijndert, C.M.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J.A. Alveolar ridge preservation in defect sockets in the maxillary aesthetic zone followed by single-tooth bone level tapered implants with immediate provisionalization: A 1-year prospective case series. Int. J. Implant. Dent. 2021, 7, 18. [Google Scholar] [CrossRef]
- Chappuis, V.; Araújo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000 2017, 73, 73–83. [Google Scholar] [CrossRef]
- Cardaropoli, D.; Tamagnone, L.; Roffredo, A.; Gaveglio, L. Evaluation of Dental Implants Placed in Preserved and Nonpreserved Postextraction Ridges: A 12-Month Postloading Study. Int. J. Periodontics Restor. Dent. 2015, 35, 677–685. [Google Scholar] [CrossRef]
- Ivanova, V.; Chenchev, I.; Zlatev, S.; Mijiritsky, E. Comparison Study of the Histomorphometric Results after Socket Preservation with PRF and Allograft Used for Socket Preservation—Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 7451. [Google Scholar] [CrossRef]
- Ayoub, A.H.; Agbor, A.M. Comparative study of extraction socket preservation using autogenous PRF and TCP. EC Dent. Sci. 2017, 8, 26–37. [Google Scholar]
- Lin, H.K.; Pan, Y.H.; Salamanca, E.; Lin, Y.T.; Chang, W.J. Prevention of Bone Resorption by HA/β-TCP + Collagen Composite after Tooth Extraction: A Case Series. Int. J. Environ. Res. Public Health 2019, 16, 4616. [Google Scholar] [CrossRef]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Cardaropoli, D.; Tamagnone, L.; Roffredo, A.; Gaveglio, L.; Cardaropoli, G. Socket preservation using bovine bone mineral and collagen membrane: A randomized controlled clinical trial with histologic analysis. Int. J. Periodontics Restor. Dent. 2012, 32, 421–430. [Google Scholar]
- Hämmerle, C.H.; Araújo, M.G.; Simion, M. Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin. Oral Implants Res. 2012; 23, (Suppl. S5), 80–82. [Google Scholar]
- Cardaropoli, D.; Gaveglio, L.; Cardaropoli, G. Vertical ridge augmentation with a collagen membrane, bovine bone mineral and fibrin sealer: Clinical and histologic findings. Int. J. Periodontics Restor. Dent. 2013, 33, 583–589. [Google Scholar] [CrossRef]
- Canellas, J.V.D.S.; Soares, B.N.; Ritto, F.G.; Vettore, M.V.; Vidigal Júnior, G.M.; Fischer, R.G.; Medeiros, P.J.D. What grafting materials produce greater alveolar ridge preservation after tooth extraction? A systematic review and network meta-analysis. J. Craniomaxillofac Surg. 2021, 49, 1064–1071. [Google Scholar] [CrossRef]
- Caponio, V.C.A.; Baca-González, L.; González-Serrano, J.; Torres, J.; López-Pintor, R.M. Effect of the use of platelet concentrates on new bone formation in alveolar ridge preservation: A systematic review, meta-analysis, and trial sequential analysis. Clin. Oral Investig. 2023, 27, 4131–4146. [Google Scholar] [CrossRef]
- Araújo, M.G.; Lindhe, J. Ridge preservation with the use of Bio-Oss collagen: A 6-month study in the dog. Clin. Oral Implants Res. 2009, 20, 433–440. [Google Scholar] [CrossRef]
- Ebenezer, E.S.; Muthu, J.; Balu, P.; Kumar, R.S. Socket preservation techniques: An overview with literature review. SRM J. Res. Dent. Sci. 2022, 13, 115–120. [Google Scholar] [CrossRef]
- Clark, D.; Rajendran, Y.; Paydar, S.; Ho, S.; Cox, D.; Ryder, M.; Dollard, J.; Kao, R.T. Advanced platelet-rich fibrin and freeze-dried bone allograft for ridge preservation: A randomized controlled clinical trial. J. Periodontol. 2018, 89, 379–387. [Google Scholar] [CrossRef]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Trandafilovic, M.; Stojanovic, P. Platelet-rich fibrin: Basics of biological actions and protocol modifications. Open Med. 2021, 16, 446–454. [Google Scholar] [CrossRef]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017; 21, 1913–1927. [Google Scholar]
- Ferreira Sávio, D.S.; Silva, L.M.P.D.; Reis, G.G.D.; Denardi, R.J.; Costa, N.M.M.D.; Chaves Furlaneto, F.A.; Souza, S.L.S.; Mourão, C.F.A.B.; Miron, R.J.; Okamoto, R.; et al. Effects of platelet-rich fibrin produced by three centrifugation protocols on bone neoformation in defects created in rat calvaria. Platelets 2023, 34, 2228417. [Google Scholar] [CrossRef]
- Miron, R.J.; Xu, H.; Chai, J.; Wang, J.; Zheng, S.; Feng, M.; Zhang, X.; Wei, Y.; Chen, Y.; Mourão, C.F.A.B.; et al. Comparison of platelet-rich fibrin (PRF) produced using 3 commercially available centrifuges at both high (~700 g) and low (~200 g) relative centrifugation forces. Clin. Oral Investig. 2020, 24, 1171–1182. [Google Scholar] [CrossRef]
- Sanz, M.; Dahlin, C.; Apatzidou, D.; Artzi, Z.; Bozic, D.; Calciolari, E.; De Bruyn, H.; Dommisch, H.; Donos, N.; Eickholz, P.; et al. Biomaterials and regenerative technologies used in bone regeneration in the craniomaxillofacial region: Consensus report of group 2 of the 15th European Workshop on Periodontology on Bone Regeneration. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 82–91. [Google Scholar] [CrossRef]
- Azangookhiavi, H.; Ghodsi, S.; Jalil, F.; Dadpour, Y. Comparison of the Efficacy of Platelet- Rich Fibrin and Bone Allograft for Alveolar Ridge Preservation after Tooth Extraction: A Clinical Trial. Front. Dent. 2020, 17, 1–6. [Google Scholar] [CrossRef]
- Santos Pereira, V.B.; Barbirato, D.D.S.; Lago, C.A.P.D.; Vasconcelos, B.C.D.E. The Effect of Advanced Platelet-Rich Fibrin in Tissue Regeneration in Reconstructive and Graft Surgery: Systematic Review. J. Craniofac. Surg. 2023, 34, 1217–1221. [Google Scholar] [CrossRef]
- Lahham, C.; Ta’a, M.A.; Lahham, E.; Michael, S.; Zarif, W. The effect of recurrent application of concentrated platelet-rich fibrin inside the extraction socket on the hard and soft tissues. a randomized controlled trial. BMC Oral Health 2023, 23, 677. [Google Scholar] [CrossRef]
- Al-Maawi, S.; Becker, K.; Schwarz, F.; Sader, R.; Ghanaati, S. Efficacy of platelet-rich fibrin in promoting the healing of extraction sockets: A systematic review. Int. J. Implant. Dent. 2021, 7, 117. [Google Scholar] [CrossRef]
- Pan, J.; Xu, Q.; Hou, J.; Wu, Y.; Liu, Y.; Li, R.; Pan, Y.; Zhang, D. Effect of platelet-rich fibrin on alveolar ridge preservation: A systematic review. J. Am. Dent. Assoc. 2019, 150, 766–778. [Google Scholar] [CrossRef]
- Zhang, Y.; Ruan, Z.; Shen, M.; Tan, L.; Huang, W.; Wang, L.; Huang, Y. Clinical effect of platelet-rich fibrin on the preservation of the alveolar ridge following tooth extraction. Exp. Ther. Med. 2018, 15, 2277–2286. [Google Scholar] [CrossRef]
- Albrektsson, T.; Johansson, C. Osteoinduction, osteoconduction and osseointegration. Eur. Spine J. 2001, 10 (Suppl. S2), S96–S101. [Google Scholar]
- Pereira, V.B.S.; Lago, C.A.P.; Almeida, R.A.C.; Barbirato, D.D.S.; Vasconcelos, B.C.D.E. Biological and Cellular Properties of Advanced Platelet-Rich Fibrin (A-PRF) Compared to Other Platelet Concentrates: Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2023, 25, 482. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef]
- Pietruszka, P.; Chruścicka, I.; Duś-Ilnicka, I.; Paradowska-Stolarz, A. PRP and PRF-Subgroups and Divisions When Used in Dentistry. J. Pers. Med. 2021, 11, 944. [Google Scholar] [CrossRef]
- Egierska, D.; Perszke, M.; Mazur, M.; Duś-Ilnicka, I. Platelet-rich plasma and platelet-rich fibrin in oral surgery: A narrative review. Dent. Med. Probl. 2023, 60, 177–186. [Google Scholar] [CrossRef]
- Srinivas, B.; Das, P.; Rana, M.M.; Qureshi, A.Q.; Vaidya, K.C.; Ahmed Raziuddin, S.J. Wound Healing and Bone Regeneration in Postextraction Sockets with and without Platelet-rich Fibrin. Ann. Maxillofac. Surg. 2018, 8, 28–34. [Google Scholar]
- Alzahrani, A.A.; Murriky, A.; Shafik, S. Influence of platelet rich fibrin on post-extraction socket healing: A clinical and radiographic study. Saudi Dent. J. 2017, 29, 149–155. [Google Scholar] [CrossRef]
- Brahma Prasad Chary, N.O.; Raju, M.S.; Suresh Sajjan, M.C.; Gottumukkala, S.N.; Manyam, R. Comparison of quality of bone and insertion torque values of early implants placed at 6 and 8 weeks in sockets preserved with advanced platelet-rich fibrin: A randomized controlled trial. J. Indian Prosthodont. Soc. 2021, 21, 366–374. [Google Scholar] [CrossRef]
- Araújo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: What can we learn? Periodontology 2000 2015, 68, 122–134. [Google Scholar] [CrossRef]
- Keranmu, D.; Nuermuhanmode, N.; Ainiwaer, A.; Guli, T.D.; Shan, W.; Ling, W. Clinical application of concentrate growth factors combined with bone substitute in Alveolar ridge preservation of anterior teeth. BMC Oral Health. 2022, 22, 54. [Google Scholar] [CrossRef]
- Ghallab, N.A.; Elaskary, A.; Elsabagh, H.; Toukhy, A.E.; Abdelrahman, H.; El-Kimary, G. A novel atraumatic extraction technique using vestibular socket therapy for immediate implant placement: A randomized controlled clinical trial. Oral Maxillofac. Surg. 2023, 27, 497–505. [Google Scholar] [CrossRef]
- Tavarez, R.R.; Dos Reis, W.L.; Rocha, A.T.; Firoozmand, L.M.; Bandéca, M.C.; Tonetto, M.R.; Malheiros, A.S. Atraumatic extraction and immediate implant installation: The importance of maintaining the contour gingival tissues. J. Int. Oral Health. 2013, 5, 113–118. [Google Scholar]
- Hauser, F.; Gaydarov, N.; Badoud, I.; Vazquez, L.; Bernard, J.P.; Ammann, P. Clinical and histological evaluation of postextraction platelet-rich fibrin socket filling: A prospective randomized controlled study. Implant. Dent. 2013, 22, 295–303. [Google Scholar] [CrossRef]
- El-Sioufi, I.; Oikonomou, I.; Koletsi, D.; Bobetsis, Y.A.; Madianos, P.N.; Vassilopoulos, S. Clinical evaluation of different alveolar ridge preservation techniques after tooth extraction: A randomized clinical trial. Clin. Oral Investig. 2023, 27, 4471–4480. [Google Scholar] [CrossRef]
- Ozgul, O.; Senses, F.; Er, N.; Tekin, U.; Tuz, H.H.; Alkan, A.; Kocyigit, I.D.; Atil, F. Efficacy of platelet rich fibrin in the reduction of the pain and swelling after impacted third molar surgery: Randomized multicenter split-mouth clinical trial. Head. Face Med. 2015, 11, 37. [Google Scholar] [CrossRef]
- Makki, A.Z.; Alsulami, A.M.; Almatrafi, A.S.; Sindi, M.Z.; Sembawa, S.N. The Effectiveness of Advanced Platelet-Rich Fibrin in comparison with Leukocyte-Platelet-Rich Fibrin on Outcome after Dentoalveolar Surgery. Int. J. Dent. 2021, 2021, 6686857. [Google Scholar] [CrossRef]
- Caymaz, M.G.; Uyanik, L.O. Comparison of the effect of advanced platelet-rich fibrin and leukocyte- and platelet-rich fibrin on outcomes after removal of impacted mandibular third molar: A randomized split-mouth study. Niger. J. Clin. Pract. 2019, 22, 546–552. [Google Scholar] [CrossRef]
- Caruana, A.; Savina, D.; Macedo, J.P.; Soares, S.C. From Platelet-Rich Plasma to Advanced Platelet-Rich Fibrin: Biological Achievements and Clinical Advances in Modern Surgery. Eur. J. Dent. 2019, 13, 280–286. [Google Scholar] [CrossRef]
- Kobayashi, E.; Flückiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Miron, R.J.; Hernandez, M.; Kandalam, U.; Zhang, Y.; Choukroun, J. Optimized Platelet-Rich Fibrin With the Low-Speed Concept: Growth Factor Release, Biocompatibility, and Cellular Response. J. Periodontol. 2017, 88, 112–121. [Google Scholar] [CrossRef]
- Castro, A.B.; Van Dessel, J.; Temmerman, A.; Jacobs, R.; Quirynen, M. Effect of different platelet-rich fibrin matrices for ridge preservation in multiple tooth extractions: A split-mouth randomized controlled clinical trial. J. Clin. Periodontol. 2021, 48, 984–995. [Google Scholar] [CrossRef]
- Gowda, T.M.; Jayashri, M.; Venkatesh, U.G.; Shah, R.; Kumar, A.B.T.; Deepthi, M.; Priya, S. Autologous tooth bone graft block compared with advanced platelet-rich fibrin in alveolar ridge preservation: A clinico-radiographic study. J. Indian Soc. Periodontol. 2023, 27, 619–625. [Google Scholar] [CrossRef]
- Lekovic, V.; Milinkovic, I.; Aleksic, Z.; Jankovic, S.; Stankovic, P.; Kenney, E.B.; Camargo, P.M. Platelet-rich fibrin and bovine porous bone mineral vs. platelet-rich fibrin in the treatment of intrabony periodontal defects. J. Periodontal. Res. 2012, 47, 409–417. [Google Scholar]
- Agarwal, G.; Thomas, R.; Mehta, D. Postextraction maintenance of the alveolar ridge: Rationale and review. Compend. Contin. Educ. Dent. 2012, 33, 320–324. [Google Scholar]
- Pereira, D.A.; Mendes, P.G.J.; Prisinoto, N.R.; de Rezende Barbosa, G.L.; Soares, P.B.F.; de Oliveira, G.J.P.L. Advanced platelet-rich-fibrin (A-PRF +) has no additional effect on the healing of post-extraction sockets of upper third molars. A split mouth randomized clinical trial. Oral Maxillofac. Surg. 2023, 27, 411–419. [Google Scholar] [CrossRef]
- Adams, R.J. Is there clinical evidence to support alveolar ridge preservation over extraction alone? A review of recent literature and case reports of late graft failure. Br. Dent. J. 2022, 233, 469–474. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Variable | A-PRF Group | Control Group | TOTAL | p |
|---|---|---|---|---|
| Patients (n/%) | 42 (50.00%) | 42 (50.00%) | 84 (100%) | - |
| Age (years)—median | 48 | 52 | 0.094 | |
| Gender | ||||
| Female (n/%) | 14 (41.20%) | 20 (58.80%) | 34 (100%) | 0.182 |
| Male (n/%) | 28 (56.00%) | 22 (44.00%) | 50 (100%) | |
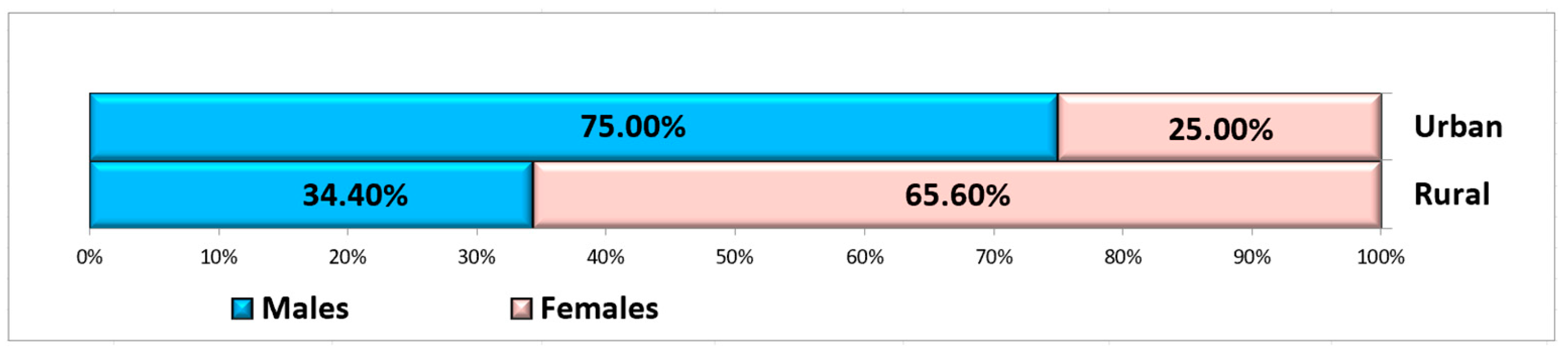
| Residence | ||||
| Urban area (n/%) | 28 (53.80%) | 24 (46.20%) | 52 (100%) | 0.369 |
| Rural area (n/%) | 14 (43.80%) | 18 (56.20%) | 31 (100%) |
| Variables | A-PRF Group | Control Group | No. of Sites | |
|---|---|---|---|---|
| Extracted teeth | 42 (50.00%) | 42 (50.00%) | 84 (100%) | |
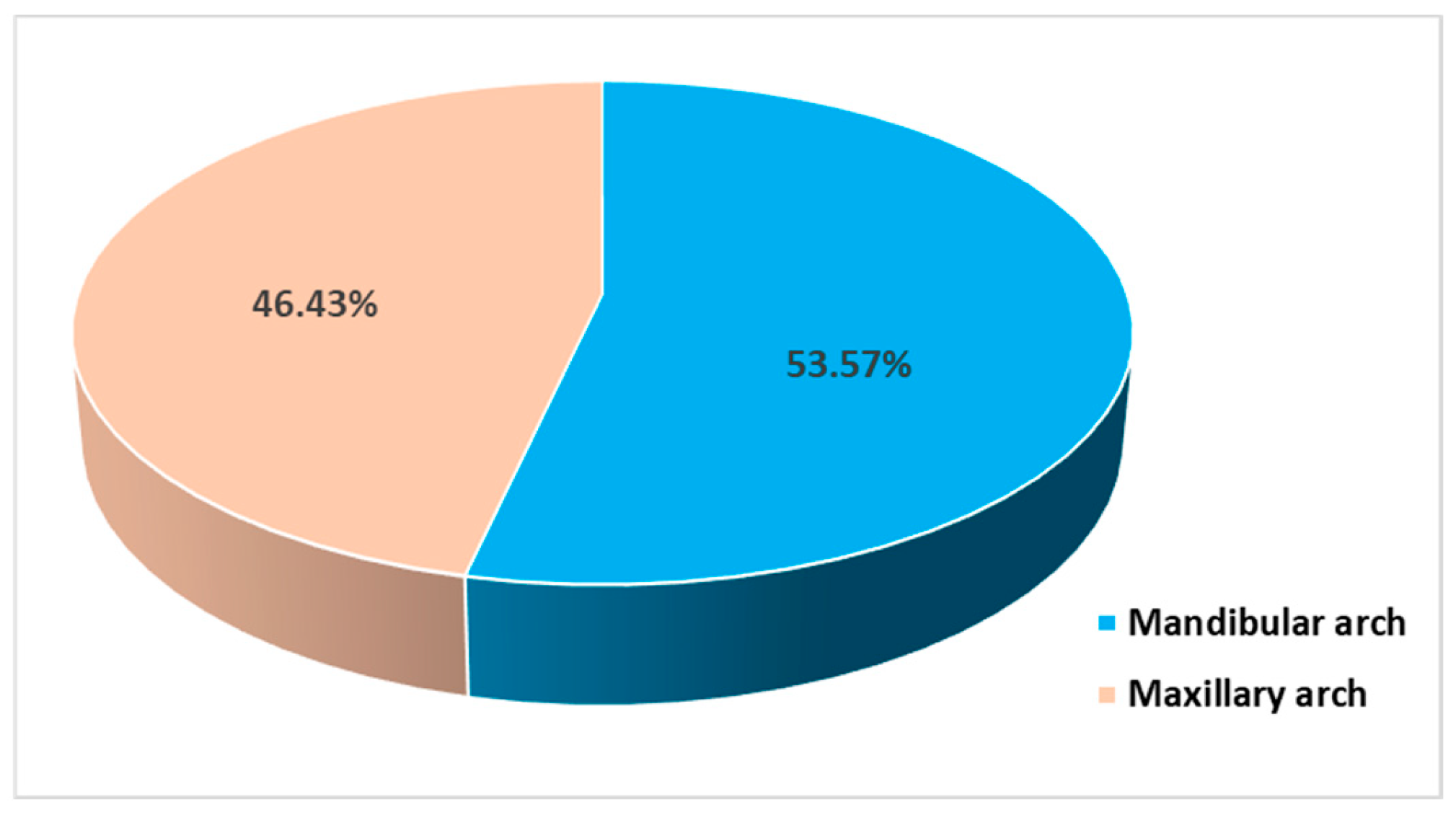
| Location | Mandibular teeth | 25 (55.56%) | 20 (44.40%) | 45 (100%) |
| Maxillary teeth | 17 (43.60%) | 22 (56.40%) | 39 (100%) | |
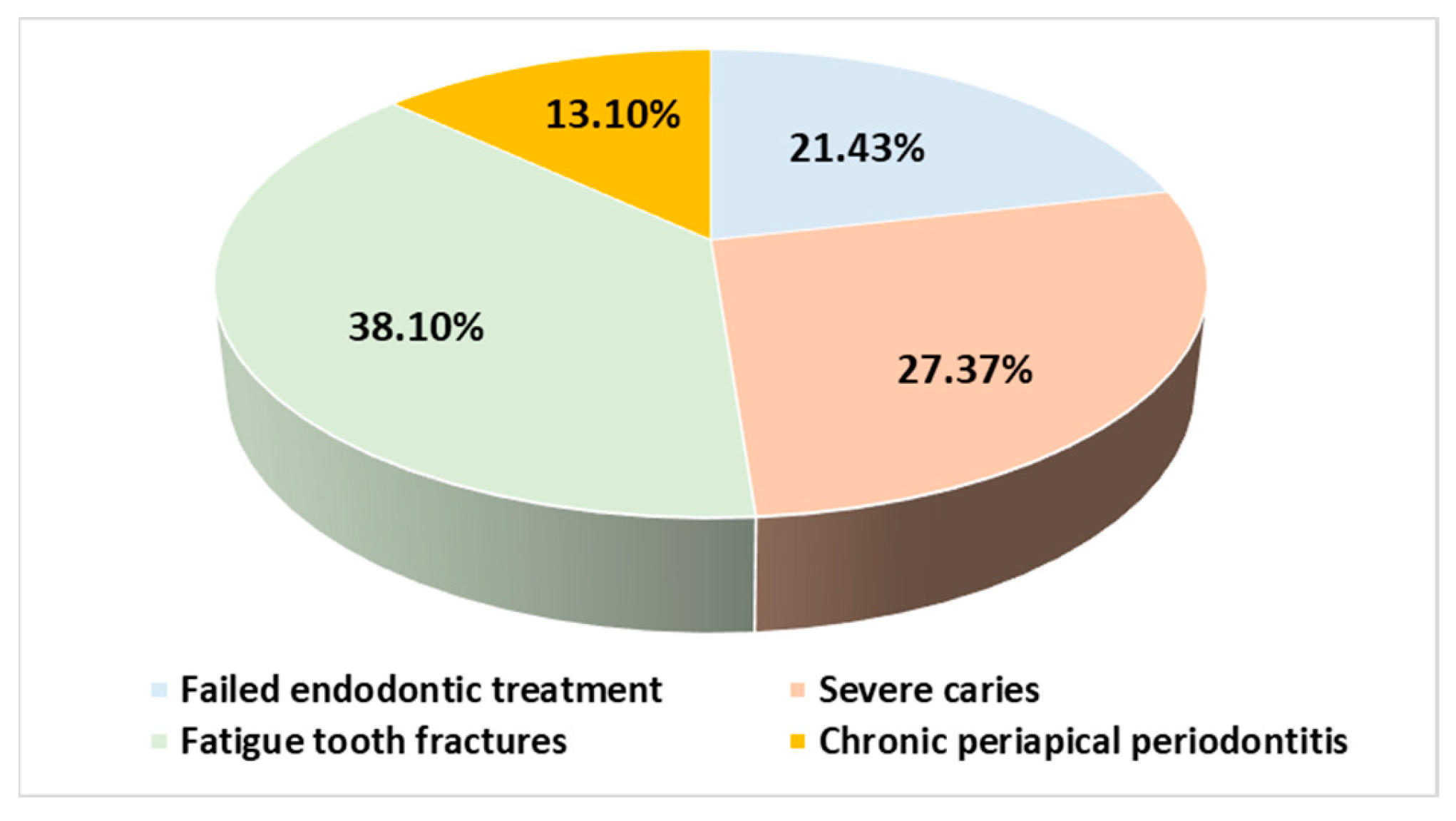
| Extraction causes | Failed endodontic treatments | 14 (77.77%) | 4 (22.23%) | 18 (100%) |
| Severe caries | 12 (52.17%) | 11 (47.83%) | 23 (100%) | |
| Fatigue tooth fractures | 5 (15.62%) | 27 (84.38%) | 32 (100%) | |
| Chronic periapical periodontitis | 11 (100%) | 0 (0.0%) | 11 (100%) | |
| Parameter | Baseline (mm) | Follow-Up (mm) | Mean Difference (mm) | Mean Percentage Variation (%) | p |
|---|---|---|---|---|---|
| A-PRF group | |||||
| Height | 14.60 ± 2.68 | 12.77 ± 2.86 | 1.83 ± 0.94 | 12.91% | ˂0.0005 1 |
| Width at 0 mm | 7.73 ± 1.99 | 6.17 ± 1.47 | 1.56 ± 0.92 | 19.35% | ˂0.0005 2 |
| Width at 3 mm | 8.90 ± 1.70 | 7.74 ± 1.57 | 1.17 ± 0.62 | 13.15% | ˂0.0005 2 |
| Width at 5 mm | 9.98 ± 1.61 | 8.90 ± 1.44 | 1.07 ± 0.70 | 10.59% | ˂0.0005 2 |
| Width at 7 mm | 11.80 ± 1.67 | 10.76 ± 1.61 | 1.03 ± 0.54 | 8.74% | ˂0.0005 2 |
| Control group | |||||
| Height | 16.50 ± 3.14 | 11.73 ± 3.70 | 4.78 ± 2.06 | 30.05% | ˂0.0005 1 |
| Width at 0 mm | 10.40 ± 1.52 | 6.20 ± 1.77 | 4.20 ± 1.24 | 40.79% | ˂0.0005 1 |
| Width at 3 mm | 10.99 ± 1.62 | 7.73 ± 1.64 | 3.26 ± 1.26 | 29.56% | ˂0.0005 1 |
| Width at 5 mm | 11.32 ± 1.71 | 8.45 ± 1.56 | 2.88 ± 1.44 | 24.87% | ˂0.0005 2 |
| Width at 7 mm | 12.09 ± 2.12 | 9.47 ± 1.56 | 2.62 ± 1.52 | 20.78% | ˂0.0005 1 |
| Parameter | A-PRF Group (Median) | Control Group (Median) | Percentage Variation (%) | U/z 1 | p 1 |
|---|---|---|---|---|---|
| Height | 1.85 | 4.75 | 38.58% | 1597.00/6.401 | ˂0.0005 |
| Width at 0 mm | 1.40 | 4.55 | 36.88% | 1676.00/7.108 | ˂0.0005 |
| Width at 3 mm | 1.20 | 2.95 | 35.56% | 1677.00/7.109 | ˂0.0005 |
| Width at 5 mm | 0.95 | 2.50 | 36.61% | 1552.50/6.004 | ˂0.0005 |
| Width at 7 mm | 0.95 | 2.75 | 38.73% | 1448.50/5.072 | ˂0.0005 |
| Parameter | Baseline (mm) | Follow-Up (mm) | Mean Percentage Variation (%) | p |
|---|---|---|---|---|
| A-PRF group—Maxilla | ||||
| Height | 13.61 ± 2.92 | 12.09 ± 2.84 | 11.40% | <0.0005 1 |
| Width at 0 mm | 8.21 ± 2.04 | 6.59 ± 1.48 | 18.84% | <0.0005 2 |
| Width at 3 mm | 8.85 ± 1.71 | 7.38 ± 1.41 | 16.46% | <0.0005 2 |
| Width at 5 mm | 9.75 ± 1.55 | 8.61 ± 1.16 | 11.28% | <0.0005 2 |
| Width at 7 mm | 11.63 ± 1.63 | 10.48 ± 1.48 | 9.76% | <0.0005 1 |
| A-PRF group—Mandible | ||||
| Height | 15.28 ± 2.32 | 13.24 ± 2.83 | 13.94% | <0.0005 1 |
| Width at 0 mm | 7.40 ± 1.93 | 5.88 ± 1.42 | 19.70% | <0.0005 2 |
| Width at 3 mm | 8.94 ± 1.73 | 7.98 ± 1.66 | 10.90% | <0.0005 1 |
| Width at 5 mm | 10.13 ± 1.66 | 9.11 ± 1.60 | 10.13% | <0.0005 2 |
| Width at 7 mm | 11.91 ± 1.73 | 10.96 ± 1.69 | 8.04% | <0.0005 1 |
| Control group—Maxilla | ||||
| Height | 14.54 ± 3.04 | 9.12 ± 2.72 | 37.56% | <0.0005 1 |
| Width at 0 mm | 11.12 ± 1.46 | 6.99 ± 2.14 | 38.15% | <0.0005 1 |
| Width at 3 mm | 11.84 ± 1.63 | 8.15 ± 2.17 | 31.75% | <0.0005 1 |
| Width at 5 mm | 12.26 ± 1.62 | 8.59 ± 2.09 | 30.42% | <0.0005 1 |
| Width at 7 mm | 13.23 ± 2.01 | 9.64 ± 1.90 | 27.21% | <0.0005 1 |
| Control group—Mandible | ||||
| Height | 18.67 ± 1.26 | 14.60 ± 2.20 | 21.80% | <0.0005 1 |
| Width at 0 mm | 9.62 ± 1.16 | 5.33 ± 0.48 | 43.70% | <0.0005 1 |
| Width at 3 mm | 10.05 ± 0.99 | 7.26 ± 0.41 | 27.14% | <0.0005 1 |
| Width at 5 mm | 10.30 ± 1.11 | 8.30 ± 0.63 | 18.76% | <0.0005 1 |
| Width at 7 mm | 10.84 ± 1.43 | 9.28 ± 1.11 | 13.72% | <0.0005 1 |
| Parameter | Maxilla (mm) | Mandible (mm) | p |
|---|---|---|---|
| A-PRF group | |||
| Height | 1.52 ± 0.76 | 2.04 ± 1.00 | 0.074 1 |
| Width at 0 mm | 1.61 ± 0.96 | 1.52 ± 0.91 | 0.598 2 |
| Width at 3 mm | 1.47 ± 0.63 | 0.96 ± 0.53 | 0.013 2 |
| Width at 5 mm | 1.14 ± 0.80 | 1.02 ± 0.64 | 0.709 2 |
| Width at 7 mm | 1.15 ± 0.60 | 0.96 ± 0.49 | 0.263 1 |
| Control group | |||
| Height | 5.41 ± 1.93 | 4.08 ± 2.01 | 0.034 1 |
| Width at 0 mm | 4.13 ± 1.16 | 4.29 ± 1.36 | 0.696 1 |
| Width at 3 mm | 3.68 ± 1.26 | 2.79 ± 1.11 | 0.016 2 |
| Width at 5 mm | 3.67 ± 1.21 | 2.00 ± 1.16 | <0.0005 2 |
| Width at 7 mm | 3.59 ± 1.13 | 1.56 ± 1.15 | ˂0.0005 1 |
| Parameter | A-PRF Group (Median) | Control Group (Median) | p |
|---|---|---|---|
| Maxilla | |||
| Height | 1.40 | 5.90 | ˂0.0005 1 |
| Width at 0 mm | 1.60 | 4.35 | ˂0.0005 1 |
| Width at 3 mm | 1.40 | 3.75 | ˂0.0005 1 |
| Width at 5 mm | 1.00 | 3.85 | ˂0.0005 2 |
| Width at 7 mm | 1.10 | 3.40 | ˂0.0005 1 |
| Mandible | |||
| Height | 2.20 | 3.70 | ˂0.0005 1 |
| Width at 0 mm | 1.40 | 4.70 | ˂0.0005 2 |
| Width at 3 mm | 0.80 | 2.70 | ˂0.0005 2 |
| Width at 5 mm | 0.90 | 1.75 | 0.001 2 |
| Width at 7 mm | 0.80 | 1.35 | 0.039 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khaddour, A.S.; Ghiță, R.E.; Ionescu, M.; Rîcă, R.G.; Mercuț, V.; Manolea, H.O.; Camen, A.; Drăghici, E.C.; Radu, A.; Popescu, S.M. Healing of Extraction Sites after Alveolar Ridge Preservation Using Advanced Platelet-Rich Fibrin: A Retrospective Study. Bioengineering 2024, 11, 566. https://doi.org/10.3390/bioengineering11060566
Khaddour AS, Ghiță RE, Ionescu M, Rîcă RG, Mercuț V, Manolea HO, Camen A, Drăghici EC, Radu A, Popescu SM. Healing of Extraction Sites after Alveolar Ridge Preservation Using Advanced Platelet-Rich Fibrin: A Retrospective Study. Bioengineering. 2024; 11(6):566. https://doi.org/10.3390/bioengineering11060566
Chicago/Turabian StyleKhaddour, Antonia Samia, Răzvan Eugen Ghiță, Mihaela Ionescu, Radu Gabriel Rîcă, Veronica Mercuț, Horia Octavian Manolea, Adrian Camen, Emma Cristina Drăghici, Andrei Radu, and Sanda Mihaela Popescu. 2024. "Healing of Extraction Sites after Alveolar Ridge Preservation Using Advanced Platelet-Rich Fibrin: A Retrospective Study" Bioengineering 11, no. 6: 566. https://doi.org/10.3390/bioengineering11060566
APA StyleKhaddour, A. S., Ghiță, R. E., Ionescu, M., Rîcă, R. G., Mercuț, V., Manolea, H. O., Camen, A., Drăghici, E. C., Radu, A., & Popescu, S. M. (2024). Healing of Extraction Sites after Alveolar Ridge Preservation Using Advanced Platelet-Rich Fibrin: A Retrospective Study. Bioengineering, 11(6), 566. https://doi.org/10.3390/bioengineering11060566