

The Utility of Indocyanine Green Angiography in Breast Reconstruction to Detect Mastectomy Skin Flap Necrosis and Free Flap Perfusion: An Umbrella Review
 , ,
, ,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Article Screening and Data Extraction
2.4. Quality Assessment
3. Results
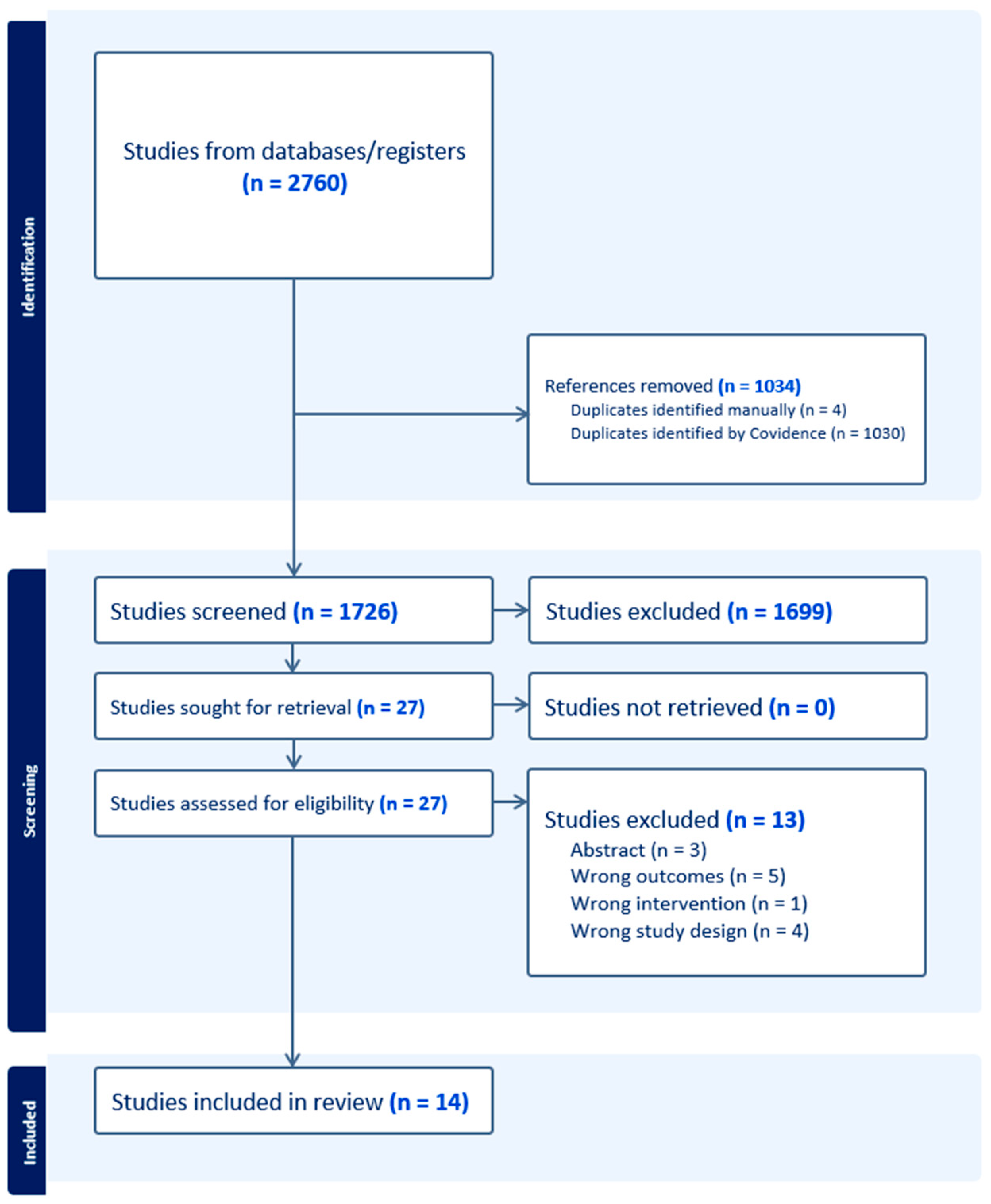
3.1. Study Selection and Quality Assessment
3.2. The Utility of ICGA in Predicting MSFN
3.3. The Utility of ICGA in Predicting BFN
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Full Search Strategy
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.; Kronowitz, S.J.; Meric-Bernstam, F.; Feig, B.W.; Symmans, W.F.; Lucci, A.; I Ross, M.; Babiera, G.V.; Kuerer, H.M.; Hunt, K.K. Local, regional, and systemic recurrence rates in patients undergoing skin-sparing mastectomy compared with conventional mastectomy. Cancer 2011, 117, 916–924. [Google Scholar] [CrossRef] [PubMed]
- Komorowska-Timek, E.; Gurtner, G.C. Intraoperative perfusion mapping with laser-assisted indocyanine green imaging can predict and prevent complications in immediate breast reconstruction. Plast. Reconstr. Surg. 2010, 125, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Jeon, F.H.K.; Varghese, J.; Griffin, M.; Butler, P.E.; Ghosh, D.; Mosahebi, A. Systematic review of methodologies used to assess mastectomy flap viability. BJS Open 2018, 2, 175–184. [Google Scholar] [CrossRef]
- Khansa, I.; Momoh, A.O.; Patel, P.P.; Nguyen, J.T.; Miller, M.J.; Lee, B.T. Fat necrosis in autologous abdomen-based breast reconstruction: A systematic review. Plast. Reconstr. Surg. 2013, 131, 443–452. [Google Scholar] [CrossRef]
- Beer, G.M.; Varga, Z.; Budi, S.; Seifert, B.; Meyer, V.E. Incidence of the superficial fascia and its relevance in skin-sparing mastectomy. Cancer 2002, 94, 1619–1625. [Google Scholar] [CrossRef]
- Robertson, S.A.; Jeevaratnam, J.A.; Agrawal, A.; Cutress, R.I. Mastectomy skin flap necrosis: Challenges and solutions. Breast Cancer Targets Ther. 2017, 9, 141–152. [Google Scholar] [CrossRef]
- Singer, R.; Lewis, C.M.; Franklin, J.D.; Lynch, J.B. Fluorescein Test for Prediction of Flap Viability during Breast Reconstructions. Plast. Reconstr. Surg. 1978, 61, 371–375. [Google Scholar] [CrossRef]
- Neto, E.d.S.; Figueiredo, P.H.M.; Moro, M.G.; Assumpção, C.B.; Perina, A.L.F.; da Costa, F.P.P.; Faria, E.P.; de Oliveira, A.C.V.; Prates, R.A. Use of laser-assisted indocyanine green angiography in breast reconstruction: Systematic review and meta-analysis. J. Surg. Oncol. 2020, 121, 759–765. [Google Scholar] [CrossRef]
- Reinhart, M.B.; Huntington, C.R.; Blair, L.J.; Heniford, B.T.; Augenstein, V.A. Indocyanine Green. Surg. Innov. 2015, 23, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Pruimboom, T.; Van Kuijk, S.M.J.; Qiu, S.S.; van den Bos, J.; Wieringa, F.; Van Der Hulst, R.R.W.J.; Schols, R.M. Optimizing Indocyanine Green Fluorescence Angiography in Reconstructive Flap Surgery: A Systematic Review and Ex Vivo Experiments. Surg. Innov. 2020, 27, 103–119. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.; Chae, M.P.; Rozen, W.M. Indocyanine green-based fluorescent angiography in breast reconstruction. Gland. Surg. 2016, 5, 133. [Google Scholar] [CrossRef]
- Duggal, C.S.; Madni, T.; Losken, A. An Outcome Analysis of Intraoperative Angiography for Postmastectomy Breast Reconstruction. Aesthetic Surg. J. 2014, 34, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Diep, G.K.; Hui, J.Y.C.; Marmor, S.; Cunningham, B.L.; Choudry, U.; Portschy, P.R.; Tuttle, T.M. Postmastectomy Reconstruction Outcomes After Intraoperative Evaluation with Indocyanine Green Angiography versus Clinical Assessment. Ann. Surg. Oncol. 2016, 23, 4080–4085. [Google Scholar] [CrossRef]
- Sood, M.; Glat, P. Potential of the SPY intraoperative perfusion assessment system to reduce ischemic complications in immediate postmastectomy breast reconstruction. Ann. Surg. Innov. Res. 2013, 7, 9. [Google Scholar] [CrossRef]
- Hembd, A.S.; Yan, J.; Zhu, H.; Haddock, N.T.; Teotia, S.S. Intraoperative Assessment of DIEP Flap Breast Reconstruction Using Indocyanine Green Angiography: Reduction of Fat Necrosis, Resection Volumes, and Postoperative Surveillance. Plast. Reconstr. Surg. 2020, 146, 1E–10E. [Google Scholar] [CrossRef]
- Malagón-López, P.; Vilà, J.; Carrasco-López, C.; García-Senosiain, O.; Priego, D.; Ibañez, J.F.J.; Higueras-Suñe, C. Intraoperative Indocyanine Green Angiography for Fat Necrosis Reduction in the Deep Inferior Epigastric Perforator (DIEP) Flap. Aesthetic Surg. J. 2019, 39, NP45–NP54. [Google Scholar] [CrossRef]
- Michi, M.; Verduijn, P.S.; Corion, L.U.M.; Vahrmeijer, A.L.; Mulder, B.G.S. Assessment of deep inferior epigastric perforator flap perfusion with near-infrared fluorescence: A pilot study and description of a standardized working protocol. J. Plast. Reconstr. Aesthetic Surg. 2022, 75, 1171–1178. [Google Scholar] [CrossRef]
- Varela, R.; Casado-Sanchez, C.; Zarbakhsh, S.; Diez, J.; Hernandez-Godoy, J.; Landin, L. Outcomes of DIEP Flap and Fluorescent Angiography: A Randomized Controlled Clinical Trial. Plast. Reconstr. Surg. 2020, 145, 1–10. [Google Scholar] [CrossRef]
- Yoo, A.; Palines, P.A.; Mayo, J.L.; Bartow, M.J.; Danos, D.M.; Hilaire, H.M.S.; Wise, M.W.; Stalder, M.W. The Impact of Indocyanine Green Angiography on Fat Necrosis in Deep Inferior Epigastric Perforator Flap Breast Reconstruction. Ann. Plast. Surg. 2022, 88, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Wapnir, I.; Dua, M.; Kieryn, A.; Paro, J.; Morrison, D.; Kahn, D.; Meyer, S.; Gurtner, G. Intraoperative imaging of nipple perfusion patterns and ischemic complications in nipple-sparing mastectomies. Ann. Surg. Oncol. 2014, 21, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Phillips, B.T.; Lanier, S.T.; Conkling, N.; Wang, E.D.; Dagum, A.B.; Ganz, J.C.; Khan, S.U.; Bui, D.T. Intraoperative perfusion techniques can accurately predict mastectomy skin flap necrosis in breast reconstruction: Results of a prospective trial. Plast. Reconstr. Surg. 2012, 129, 778e–788e. [Google Scholar] [CrossRef] [PubMed]
- Alstrup, T.; Christensen, B.O.; Damsgaard, T.E. ICG angiography in immediate and delayed autologous breast reconstructions: Peroperative evaluation and postoperative outcomes. J. Plast. Surg. Hand Surg. 2018, 52, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Gorai, K.; Inoue, K.; Saegusa, N.; Shimamoto, R.; Takeishi, M.; Okazaki, M.; Nakagawa, M. Prediction of Skin Necrosis after Mastectomy for Breast Cancer Using Indocyanine Green Angiography Imaging. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1321. [Google Scholar] [CrossRef] [PubMed]
- Hammer-Hansen, N.; Juhl, A.A.; Damsgaard, T.E. Laser-assisted indocyanine green angiography in implant-based immediate breast reconstruction: A retrospective study. J. Plast. Surg. Hand Surg. 2018, 52, 158–162. [Google Scholar] [CrossRef]
- Harless, C.A.; Jacobson, S.R. Tailoring through Technology: A Retrospective Review of a Single Surgeon’s Experience with Implant-Based Breast Reconstruction before and after Implementation of Laser-Assisted Indocyanine Green Angiography. Breast J. 2016, 22, 274–281. [Google Scholar] [CrossRef]
- Mirhaidari, S.J.; Beddell, G.M.; Orlando, M.V.; Parker, M.G.; Pedersen, J.C.; Wagner, D.S. A Prospective Study of Immediate Breast Reconstruction with Laser-Assisted Indocyanine Green Angiography. Plast. Reconstr. Surg. Glob. Open. 2018, 6, e1774. [Google Scholar] [CrossRef]
- Rinker, B. A Comparison of Methods to Assess Mastectomy Flap Viability in Skin-Sparing Mastectomy and Immediate Reconstruction: A Prospective Cohort Study. Plast. Reconstr. Surg. 2016, 137, 395–401. [Google Scholar] [CrossRef]
- Driessen, C.; Arnardottir, T.H.; Lorenzo, A.R.; Mani, M.R. How should indocyanine green dye angiography be assessed to best predict mastectomy skin flap necrosis? A systematic review. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1031–1042. [Google Scholar] [CrossRef]
- Burnier, P.; Niddam, J.; Bosc, R.; Hersant, B.; Meningaud, J.P. Indocyanine green applications in plastic surgery: A review of the literature. J. Plast. Reconstr. Aesthetic Surg. 2017, 70, 814–827. [Google Scholar] [CrossRef] [PubMed]
- Ashok, B.C.; Kabilan, H.K.; Anantheswar, Y.N.; Srikanth, V.; Somashekar, S.P.; Prasad, A. Role of Indocyanine Green in Breast Surgery. Indian. J. Surg. 2022, 84, 592–601. [Google Scholar] [CrossRef]
- Parmeshwar, N.; Sultan, S.M.; Kim, E.A.; Piper, M.L. A Systematic Review of the Utility of Indocyanine Angiography in Autologous Breast Reconstruction. Ann. Plast. Surg. 2021, 86, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Jiao, L.; Chen, S.; Li, Z.; Xiao, Y.; Du, F.; Huang, J.; Long, X. Flap perfusion assessment with indocyanine green angiography in deep inferior epigastric perforator flap breast reconstruction: A systematic review and meta-analysis. Microsurgery 2023, 43, 627–638. [Google Scholar] [CrossRef]
- Steenbeek, L.M.; Peperkamp, K.; Ulrich, D.J.O.; Hummelink, S. Alternative imaging technologies for perforator mapping in free flap breast reconstructive surgery—A comprehensive overview of the current literature. J. Plast. Reconstr. Aesthetic Surg. 2022, 75, 4074–4084. [Google Scholar] [CrossRef]
- Pruimboom, T.; Schols, R.M.; Van Kuijk, S.M.J.; Van der Hulst, R.R.W.J.; Qiu, S.S. Indocyanine green angiography for preventing postoperative mastectomy skin flap necrosis in immediate breast reconstruction. Cochrane Database Syst. Rev. 2020, 2020, CD013280. [Google Scholar] [CrossRef]
- Pagliara, D.; Schiavone, L.; Garganese, G.; Bove, S.; Montella, R.A.; Costantini, M.; Rinaldi, P.M.; Bottosso, S.; Grieco, F.; Rubino, C.; et al. Predicting Mastectomy Skin Flap Necrosis: A Systematic Review of Preoperative and Intraoperative Assessment Techniques. Clin. Breast Cancer 2023, 23, 249–254. [Google Scholar] [CrossRef]
- Liu, E.H.; Zhu, S.L.; Hu, J.; Wong, N.; Farrokhyar, F.; Thoma, A. Intraoperative SPY Reduces Post-mastectomy Skin Flap Complications: A Systematic Review and Meta-Analysis. Plast. Reconstr. Surg—Glob. Open 2019, 7, e2060. [Google Scholar] [CrossRef]
- Lauritzen, E.; Damsgaard, T.E. Use of Indocyanine Green Angiography decreases the risk of complications in autologous- and implant-based breast reconstruction: A systematic review and meta-analysis. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 1703–1717. [Google Scholar] [CrossRef]
- Johnson, A.C.; Colakoglu, S.; Chong, T.W.; Mathes, D.W. Indocyanine green angiography in breast reconstruction: Utility, limitations, and search for standardization. Plast. Reconstr. Surg—Glob. Open 2020, 8, e2694. [Google Scholar] [CrossRef]
- Shea, B.J.; Grimshaw, J.M.; A Wells, G.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef] [PubMed]
- Lie, K.H.; Barker, A.S.; Ashton, M.W. A classification system for partial and complete diep flap necrosis based on a review of 17,096 DIEP flaps in 693 articles including analysis of 152 total flap failures. Plast. Reconstr. Surg. 2013, 132, 1401–1408. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, A.; Nakagawa, T.; Oda, G.; Hosoya, T.; Hayashi, K.; Yoshino, M.; Mori, H.; Uemura, N.; Fujioka, T.; Mori, M.; et al. Study of the protocol used to evaluate skin-flap perfusion in mastectomy based on the characteristics of indocyanine green. Photodiagnosis Photodyn. Ther. 2021, 35, 102401. [Google Scholar] [CrossRef]
- Wagner, I.J.; Tong, W.M.; Halvorson, E.G. A classification system for fat necrosis in autologous breast reconstruction. Ann. Plast. Surg. 2013, 70, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Oleck, N.C.; Gu, C.; Pyfer, B.J.; Phillips, B.T. Defining Mastectomy Skin Flap Necrosis: A Systematic Review of the Literature and a Call for Standardization. Plast. Reconstr. Surg. 2022, 149, 858E–866E. [Google Scholar] [CrossRef]
- Jong, L.J.S.; Appelman, J.G.C.; Sterenborg, H.J.C.M.; Ruers, T.J.M.; Dashtbozorg, B. Spatial and Spectral Reconstruction of Breast Lumpectomy Hyperspectral Images. Sensors 2024, 24, 1567. [Google Scholar] [CrossRef]
- Thiem, D.G.E.; Frick, R.W.; Goetze, E.; Gielisch, M.; Al-Nawas, B.; Kämmerer, P.W. Hyperspectral analysis for perioperative perfusion monitoring—A clinical feasibility study on free and pedicled flaps. Clin. Oral. Investig. 2021, 25, 933–945. [Google Scholar] [CrossRef]
- Pruimboom, T.; Lindelauf, A.A.M.A.; Felli, E.; Sawor, J.H.; Deliaert, A.E.K.; van der Hulst, R.R.W.J.; Al-Taher, M.; Diana, M.; Schols, R.M. Perioperative Hyperspectral Imaging to Assess Mastectomy Skin Flap and DIEP Flap Perfusion in Immediate Autologous Breast Reconstruction: A Pilot Study. Diagnostics 2022, 12, 184. [Google Scholar] [CrossRef]
- Shapey, J.; Xie, Y.; Nabavi, E.; Bradford, R.; Saeed, S.R.; Ourselin, S.; Vercauteren, T. Intraoperative multispectral and hyperspectral label-free imaging: A systematic review of in vivo clinical studies. J. Biophotonics 2019, 12, e201800455. [Google Scholar] [CrossRef]
- Zötterman, J.; Bergkvist, M.; Iredahl, F.; Tesselaar, E.; Farnebo, S. Monitoring of partial and full venous outflow obstruction in a porcine flap model using laser speckle contrast imaging. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 936–943. [Google Scholar] [CrossRef]
- Zötterman, J.; Opsomer, D.; Farnebo, S.; Blondeel, P.; Monstrey, S.; Tesselaar, E. Intraoperative Laser Speckle Contrast Imaging in DIEP Breast Reconstruction: A Prospective Case Series Study. Plast. Reconstr. Surg—Glob. Open 2020, 8, E2529. [Google Scholar] [CrossRef] [PubMed]
- Zötterman, J.; Tesselaar, E.; Farnebo, S. The use of laser speckle contrast imaging to predict flap necrosis: An experimental study in a porcine flap model. J. Plast. Reconstr. Aesthetic Surg. 2019, 72, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Zötterman, J.; Tesselaar, E.; Elawa, S.; Farnebo, S. Correlation between Indocyanine Green Fluorescence Angiography and Laser Speckle Contrast Imaging in a Flap Model. Plast. Reconstr. Surg—Glob. Open 2023, 11, E5187. [Google Scholar] [CrossRef] [PubMed]
- Attia, A.B.E.; Balasundaram, G.; Moothanchery, M.; Dinish, U.; Bi, R.; Ntziachristos, V.; Olivo, M. A review of clinical photoacoustic imaging: Current and future trends. Photoacoustics 2019, 16, 100144. [Google Scholar] [CrossRef]
- Zhang, D.; Chen, H.; Hu, X.; Yu, A. Photoacoustic microscopy: A novel approach for studying perforator skin flap in a mouse model. Quant. Imaging Med. Surg. 2021, 11, 4365. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Study ID | Article Type | Patient Population | Article Date Range | Included Studies | Duration of Follow-Up | Main Findings | Secondary Findings | Remaining Evidence Gaps |
|---|---|---|---|---|---|---|---|---|
| Wang et al., 2023 [34] | SR and MA | 1814 patients who underwent DIEP flap breast reconstruction with and without ICGA | 2006–2022 | 5 prospective noncomparative, 5 retrospective noncomparative, 2 prospective comparative, 9 retrospective comparative, 1 RCT | Over 6 months | ICGA did not significantly alter the risk of mastectomy skin flap necrosis in DIEP flap reconstructions (RR 0.9, p = 0.88). | ICGA did not significantly alter the risk of seroma (RR 1.21, p = 0.68), hematoma (RR 0.94, p = 0.71), dehiscence (RR 1.71, p = 0.18), and infection (RR 0.77, p = 0.51) | Most included studies were retrospective and the MA only included five studies, limiting generalizability and power for detecting differences in each outcome measure. There was also significant heterogeneity among included studies regarding follow-up, ICGA protocols, and criteria for including versus excluding degrees of necrosis. |
| Pagliara et al., 2023 [37] | SR | 1151 breasts undergoing mastectomy with immediate, implant-based reconstruction | Not specified | 1 descriptive, 1 systematic review, 6 prospective, 6 retrospective | Not specified | Unclear effect of ICGA alone on MSFN, but according to one study ICGA + SPY analysis may significantly reduce risk. ICGA may increase precision for tissue debridement during mastectomy and reconstruction. Authors recommend using ICGA intraoperatively when clinical assessment is uncertain. | Widespread ICGA + SPY may not be cost effective, but is advantageous when used on high-risk patients such as smokers and obese patients | This review is limited by significant heterogeneity in the protocols by which skin flaps were assessed as well as how necrosis was classified and how comorbidities were factored into results. |
| Ashok et al., 2022 [32] | SR | All breast surgeries with any use of ICG | 1977–2021 | 55 included, breakdown not specified | Not specified | For MSFN, ICGA is superior to clinical assessment when predicting necrosis. One study reported a 90% sensitivity and a 100% specificity. | None | The review presents data on several studies regarding ICGA and preventing MSFN but provides no pooled analysis and does not discuss any heterogeneity in studies or studies with alternative conclusions. |
| Steenbeek et al., 2022 [35] | SR | Free flap breast reconstructions with perforator imaging modalities | 2004–2020 | 168 studies, breakdown not specified | Not specified | ICGA can be used to assist in early identification of MSFN to prevent complications. | ICGA can be used to support decisions for which perforators to use for free flap reconstruction. ICGA is more precise than CTA for perforator mapping but can only find superficial vessels. | This review touches on perfusion assessment of skin flaps but mainly focuses on perforator assessment in free flap surgery. |
| Lauritzen, Damsgaard, 2021 [39] | SR and MA | 4314 breast reconstructions with ICGA, mean age 49.6 | 2010–2020 | 1 RCT study, 2 clinical trials, 4 comparative studies, 8 cohort studies, and 11 case controls | 2 weeks to 24 months, reported in 23 of 26 papers | In pooled analysis when evaluating mastectomy flaps with implant reconstruction, ICGA significantly reduced major complications requiring return to OR (OR 0.56, p = 0.001) and loss of reconstruction (OR 0.46, p = 0.006). When evaluating mastectomy skin flaps with autologous reconstruction, ICGA reduced risk of minor complications (OR 0.41, p = 0.0001) but had no significant effect on major complications or losses of reconstruction. ICGA correlates significantly with reduced risk of major complications and reconstruction loss in mastectomy skin flaps. | None | The studies included in this synthesis are heterogenous in their design and definition of fat necrosis. The majority of these were retrospective in nature and may be subject to biases or confounders. |
| Pruimboom et al., 2020 [36] | SR and MA | 1589 women undergoing 2199 SSMs with immediate autologous or prosthetic reconstruction | 2014–2018, searched 1946–2019 | 7 nonrandomized, retrospective cohort studies and 2 nonrandomized, prospective cohort studies | 90 days to 6 months | Authors rated quality of evidence very low for most outcomes. For postoperative MSFN per patient, ICGA had an uncertain effect on risk (RR 0.79, 95%CI 0.40 to 1.56). For postoperative MSFN per breast, ICGA may reduce risk (RR 0.62, 95% CI 0.48 to 0.82). Overall, ICGA may reduce incidence of some complications, but specifics are unclear. | ICGA reduced reoperation when examined per patient (RR 0.5, 95% CI 0.35–0.72) and per breast (RR 0.65, 95% CI 0.47–0.92) but very low quality of evidence. When examining infection risk per breast, ICGA reduced risk (RR 0.65, 95% CI 0.44 to 0.97) but had low evidence quality. When examining hematoma per patient, ICGA reduced risk (RR 0.87, 95% CI 0.3–2.53) although had low evidence quality. No clear effect on risk for dehiscence. | Most of the available included studies are retrospective, which may introduce confounding variables, and the low sample sizes and heterogeneity of included studies make the quality of evidence low for pooled analysis. |
| Driessen et al., 2020 [30] | SR | 1656 patients undergoing mastectomy with or without immediate implant reconstruction | 2005–2018 | nonrandomized cohort studies, 6 retrospective, 10 prospective | Not specified | When using ICGA and SPY, absolute perfusion cutoffs of 7–8 were reported for tissue debridement. For relative perfusion, suggested cutoffs are 34% and 25–33%. Significant decrease in MSFN with ICG, but there is no consensus on which parameters to use for SPY. ICGA tends to increase surgical debridement intraoperatively. | None | Heterogeneity of included studies made pooled analysis impossible, limiting the conclusions that can be drawn. Small sample sizes in included studies and limited follow-up also limit generalizability. |
| Johnson et al., 2020 [40] | SR | ICGA in mastectomy skin flap assessment: 1005 patients ICGA in NAC perfusion assessment: 79 patients + 149 NACs ICGA in implant-based reconstruction: 604 patients ICGA in autologous reconstruction: 1595 patients | Not specified | 43 total studies, breakdown not provided | Not specified | In mastectomy, ICGA reduces risk of ischemic complications but is most important when clinical evaluation is unclear. For mastectomy with implant-based reconstruction, ICGA can be used to determine skin flap and NAC perfusion to aid in adjusting implant volume and debriding tissue. | None | Some confounders, such as smoking and epinephrine-containing tumescent solution, were not adjusted for in included studies and this can confound evidence. |
| daSilvaNeto et al., 2020 [10] | SR and MA | 1948 SSMs or NSM patients with reconstruction, age 26–75 | all articles before 30 August 2019 | Two studies were cohort, two were case-control, and five were retrospective reviews | 90 days to 6 months | For MSFN, clinical assessment alone resulted in significantly higher risk of necrosis than clinical assessment plus ICGA (OR 1.85, p = 0.0006). Clinical assessment alone also had significantly higher risk of reoperation (OR 2.05, p = 0.0002). Overall, ICGA appears to reduce rates of MSFN and nipple necrosis. | No significant difference in risk between using clinical assessment alone or clinical assessment with ICGA for infection (OR 1.78, p = 0.05) or seroma (OR 1.06, p = 0.85). | Larger, prospective studies are needed with standardized definitions for necrotic complications and what constitutes a perfusion-related reoperation. |
| Liu et al., 2019 [38] | SR and MA | 902 skin or nipple sparing mastectomies with reconstruction, mean age of four included studies 47–53 | searched 1 January 1960 to 1 March 2018 | 6 retrospective, 1 prospective | 3 to 16.9 months | ICGA significantly lowered rates of skin necrosis (9.8% vs. 15.2%, p = 0.001). In weighted meta-analysis, ICGA significantly reduced rate of MSFN (OR 0.56, 95% CI 0.35–0.89, p = 0.02, I2 = 40%). | ICGA significantly lowered rates of complication (26.9% vs 30.7%, p = 0.03) and reoperation (6.8% vs 15.2%, p < 0.01). In weighted meta-analysis, ICG significantly reduced rate of reoperation (OR 0.32, 95% CI 0.21–0.49, p < 0.00001, I2 = 19%) and complications (OR 0.62, 95% CI 0.41–0.94, p = 0.06, I2 = 54%). | Studies included were largely retrospective with small sample sizes. Did not include cases of necrosis requiring surgery from one study. |
| Jeon et al., 2018 [5] | SR | 2650 breasts undergoing NSM or SSM with immediate reconstruction | searched 1946–2017 | 8 prospective cohort, 4 retrospective case series, 3 prospective case series, 1 retrospective case-control study, 1 prospective pilot trial, 1 cost analysis study | Not specified | ICGA decreased rates of MSFN and reoperation in mastectomy with immediate reconstruction. ICGA tends to overpredict necrosis and underperfusion. Many variables also affect accuracy of ICGA, including room temperature, blood pressure, systemic vascular resistance, and ambient light. | None | Significant heterogeneity exists in the included studies’ definitions of skin flap necrosis. |
| Burnier et al., 2017 [31] | SR | 4368 plastic surgery patients | 2002–2015 | 41 including RCTs, feasibility studies, non-randomized comparative studies, technique descriptions, retrospective reviews | Not specified | Intraoperative ICGA can predict mastectomy skin flap necrosis accurately during breast reconstruction. ICGA has been used to lower incidence of mastectomy skin necrosis and unexpected perfusion-related reoperations | None | Heterogeneity among included studies limits conclusions that can be drawn, and low follow-up times in some included studies means all instances of breast flap necrosis may not have been captured. |
| Griffiths et al., 2016 [13] | SR | Any breast reconstruction using ICGA | 2004–2014 | 9 retrospective studies and 4 prospective studies | Not specified | Current evidence suggests use of ICGA reduces incidence of MSFN. One study found a 95% correlation between findings on ICGA and subsequent mastectomy skin flap necrosis, with a sensitivity of 100% and a specificity of 91%. However, absolute perfusion via SPY-Q software is prone to being confounded by variables such as smoking and the use of epinephrine-containing tumescent solution. | None | Data presented are qualitative, with no pooled analysis and no discussion of heterogeneity or confounders. |
| Study ID | Article Type | Patient Population | Article Date Range | Included Studies | Duration of Follow-Up | Main Findings | Secondary Findings | Remaining Evidence Gaps |
|---|---|---|---|---|---|---|---|---|
| Wang et al., 2023 [34] | SR and MA | 1814 patients who underwent DIEP flap breast reconstruction with and without ICGA | 2006–2022 | 5 prospective noncomparative, 5 retrospective noncomparative, 2 prospective comparative, 9 retrospective comparative, 1 RCT | Not specified | Authors concluded intraoperative ICGA was associated with significantly lower rates of postoperative fat necrosis (RR 0.47, p = 0.004) and ischemia-related reoperations (RR 0.41, p = 0.03). No significant difference observed for total flap loss (RR 0.89, p = 0.76) and partial flap loss (RR 0.25, p = 0.09). | ICGA did not significantly alter the risk of seroma (RR 1.21, p = 0.68), hematoma (RR 0.94, p = 0.71), dehiscence (RR 1.71, p = 0.18), and infection (RR 0.77, p = 0.51). ICGA may not be cost effective when performed repetitively. | Most included studies were retrospective and the MA only included five studies, limiting generalizability and power for detecting differences in each outcome measure. There was also significant heterogeneity among included studies regarding follow-up, ICGA protocols, and criteria for including versus excluding degrees of fat necrosis. |
| Ashok et al., 2022 [32] | SR | All breast surgeries with any use of ICG | 1977–2021 | 495 articles, 55 included in results | Not specified | ICGA is very reliable for detecting free flap hypoperfusion and guiding tissue debridement. ICGA frequently does not correlate with clinical signs of hypoperfusion, in which case tissue resection can be delayed while perfusion stabilizes. ICGA has been shown to improve partial flap survival. | None | The review mainly cites evidence from studies on free flaps in general rather than those focusing on breast reconstruction when discussing ICGA and fat necrosis. No pooled analysis or statistical data are presented. |
| Lauritzen, Damsgaard, 2021 [39] | SR and MA | 4314 breast reconstructions with ICGA, mean age 49.6 | 2010–2020 | 1 RCT study, 2 clinical trials, 4 comparative studies, 8 cohort studies, and 11 case controls | 2 weeks to 24 months, reported in 23 of 26 papers | When evaluating autologous reconstruction, ICGA significantly reduced risk of major complications (OR 0.62, p = 0.001) and minor complications (OR 0.53, p = 0.028), but had no significant effect on flap loss. ICGA lowers overall complication risk in autologous breast reconstruction | None | The studies included in this synthesis are heterogenous in their design and definition of fat necrosis. The majority of these were retrospective in nature and may be subject to biases or confounders. |
| Parmeshwar et al., 2021 [33] | SR and MA | 355 patients, 824 autologous breast reconstructions, half immediate | 1 January 2000 to 1 March 2020 | 1 prospective randomized trial, 8 retrospective cohort studies | 3 months to 1 year | ICG in single-institution studies has been shown to be useful in minimizing flap failure, MSFN, and fat necrosis. ICGA helpful for intraoperative debridement, which reduces necrosis/flap loss. ICGA significantly reduced fat necrosis in autologous flaps (OR = 0.31, p = 0.0006) but showed no statistically significant difference in total or partial flap loss. | None | The studies included in this MA had a maximum follow-up time of one year, which may be insufficient to truly determine fat necrosis rates. Studies also used differing definitions of necrosis and some did not specify theirs. |
| Pruimboom et al., 2020 [36] | SR and MA | 1589 women undergoing 2199 SSMs with immediate autologous or prosthetic reconstruction | 2014–2018, searched 1946–2019 | 7 nonrandomized, retrospective cohort studies and 2 nonrandomized, prospective cohort studies | 90 days to 6 months | Authors rated the quality of evidence very low for most outcomes and found no clear effect of ICGA on autologous flap necrosis. Overall, ICGA may reduce incidence of some complications, but specifics are unclear. | ICGA reduced reoperation when examined per patient (RR 0.5, 95% CI 0.35–0.72) and per breast (RR 0.65, 95% CI 0.47–0.92) but very low quality of evidence. When examining infection risk per breast, ICGA reduced risk (RR 0.65, 95% CI 0.44 to 0.97) but evidence was of low quality. When examining hematoma per patient, ICGA reduced risk (RR 0.87, 95% CI 0.3–2.53) but still evidence was low quality. ICGA had no clear effect on dehiscence. | Most of the available included studies are retrospective, which may introduce confounding variables. Only two included studies discussed ICGA and breast fat necrosis, so no pooled statistical analysis was conducted. |
| Johnson et al., 2020 [40] | SR | ICGA in mastectomy skin flap assessment: 1005 patients ICGA in NAC perfusion assessment: 79 patients + 149 NACs ICGA in implant-based reconstruction: 604 patients ICGA in autologous reconstruction: 1595 patients | Not specified | 43 studies | Not specified | In autologous reconstruction, ICGA is useful to visualize flap perfusion and is reliable, can decrease fat necrosis rates postoperatively, and can possibly lead to higher BREAST-Q scores. ICGA can reduce rates of unexpected reoperations; however, it tends to overestimate underperfusion and venous congestion. | None | Studies cited in this review have significant heterogeneity in their ICGA protocols and some do not adjust for confounding intraoperative factors, such as mean arterial pressure or epinephrine-containing tumescent solution. |
| Burnier et al., 2017 [31] | SR | 4368 plastic surgery patients | 2002–2015 | 41 including RCTs, feasibility studies, non-randomized comparative studies, technique descriptions, retrospective reviews | Not specified | ICGA can aid in visualizing free flap perfusion, venous congestion, and vasospasm. Not very successful for detecting DIEP perforators but can reduce partial flap loss and flap necrosis. | None | Heterogeneity among included studies limits conclusions that can be drawn, and low follow-up times in some included studies means all instances of breast flap necrosis may not have been captured. |
| Griffiths et al., 2016 [13] | SR | Any breast reconstruction using ICGA | 2004–2014 | 9 retrospective studies and 4 prospective studies | Not specified | ICGA has demonstrated utility in selection of dominant perforators for free flap reconstruction intraoperatively as well as intraoperative perfusion assessment. Many studies have correlated areas of hypoperfusion identified with ICGA with areas of postoperative flap necrosis. ICGA can also be used to evaluate microanastomotic patency and detect occlusion, thrombosis, and pedicle torsion. | None | Only two studies are mentioned regarding free flap perfusion assessment and breast flap necrosis, and much of the data focus on TRAM flaps where as DIEP flaps are more commonly performed today. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fadell, N.; Laurent, F.; Sanka, S.A.; Ochoa, E.; Yaeger, L.; Li, X.; Wood, M.D.; Sacks, J.M.; Badran, S. The Utility of Indocyanine Green Angiography in Breast Reconstruction to Detect Mastectomy Skin Flap Necrosis and Free Flap Perfusion: An Umbrella Review. Bioengineering 2024, 11, 1025. https://doi.org/10.3390/bioengineering11101025
Fadell N, Laurent F, Sanka SA, Ochoa E, Yaeger L, Li X, Wood MD, Sacks JM, Badran S. The Utility of Indocyanine Green Angiography in Breast Reconstruction to Detect Mastectomy Skin Flap Necrosis and Free Flap Perfusion: An Umbrella Review. Bioengineering. 2024; 11(10):1025. https://doi.org/10.3390/bioengineering11101025
Chicago/Turabian StyleFadell, Nicholas, Flora Laurent, Sai Anusha Sanka, Esther Ochoa, Lauren Yaeger, Xiaowei Li, Matthew D. Wood, Justin M. Sacks, and Saif Badran. 2024. "The Utility of Indocyanine Green Angiography in Breast Reconstruction to Detect Mastectomy Skin Flap Necrosis and Free Flap Perfusion: An Umbrella Review" Bioengineering 11, no. 10: 1025. https://doi.org/10.3390/bioengineering11101025
APA StyleFadell, N., Laurent, F., Sanka, S. A., Ochoa, E., Yaeger, L., Li, X., Wood, M. D., Sacks, J. M., & Badran, S. (2024). The Utility of Indocyanine Green Angiography in Breast Reconstruction to Detect Mastectomy Skin Flap Necrosis and Free Flap Perfusion: An Umbrella Review. Bioengineering, 11(10), 1025. https://doi.org/10.3390/bioengineering11101025