
Validation of Automatically Quantified Swim Stroke Mechanics Using an Inertial Measurement Unit in Paralympic Athletes

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
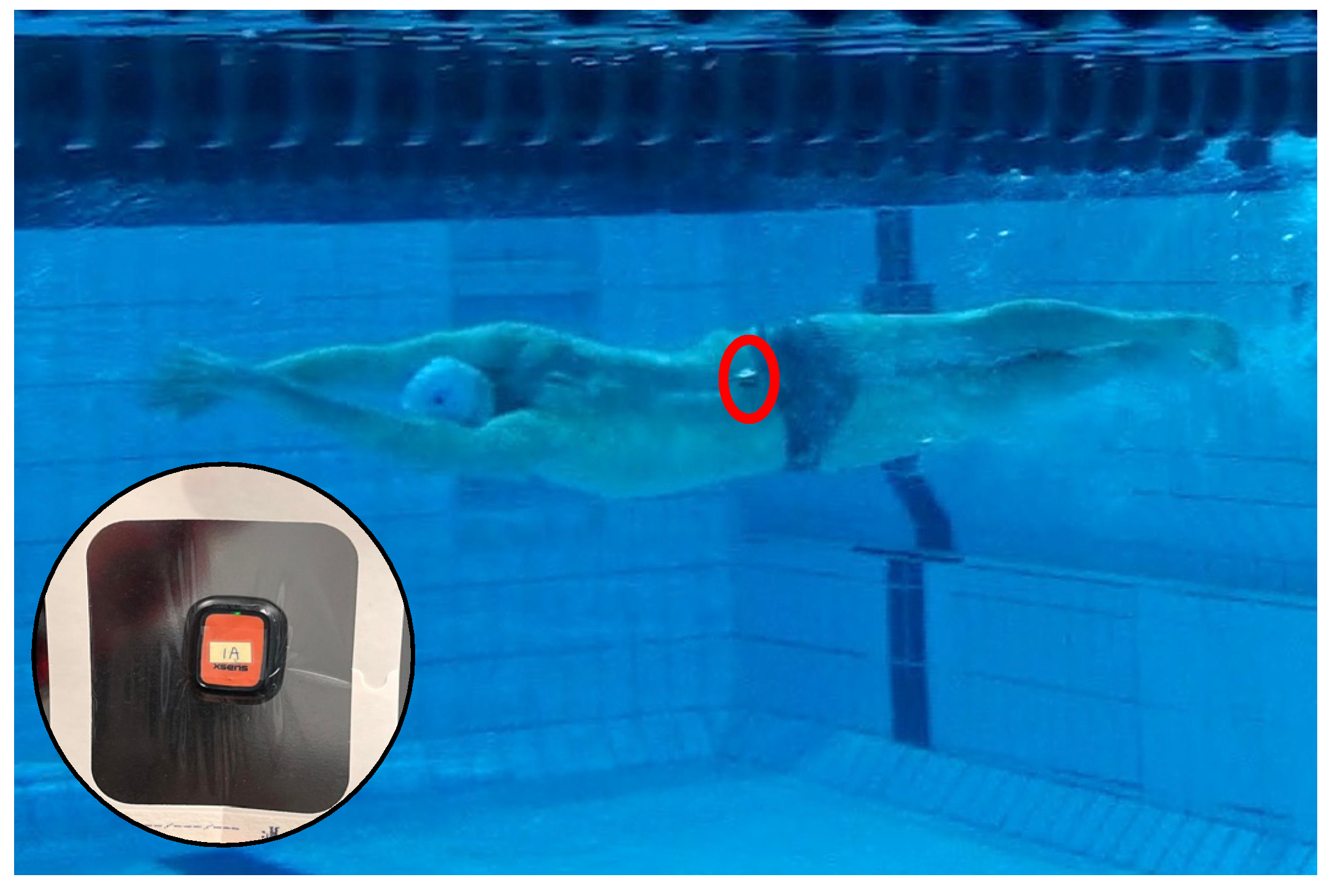
2.2. Instrumentation
2.3. Protocol
2.4. Data Processing
2.4.1. IMU Processing
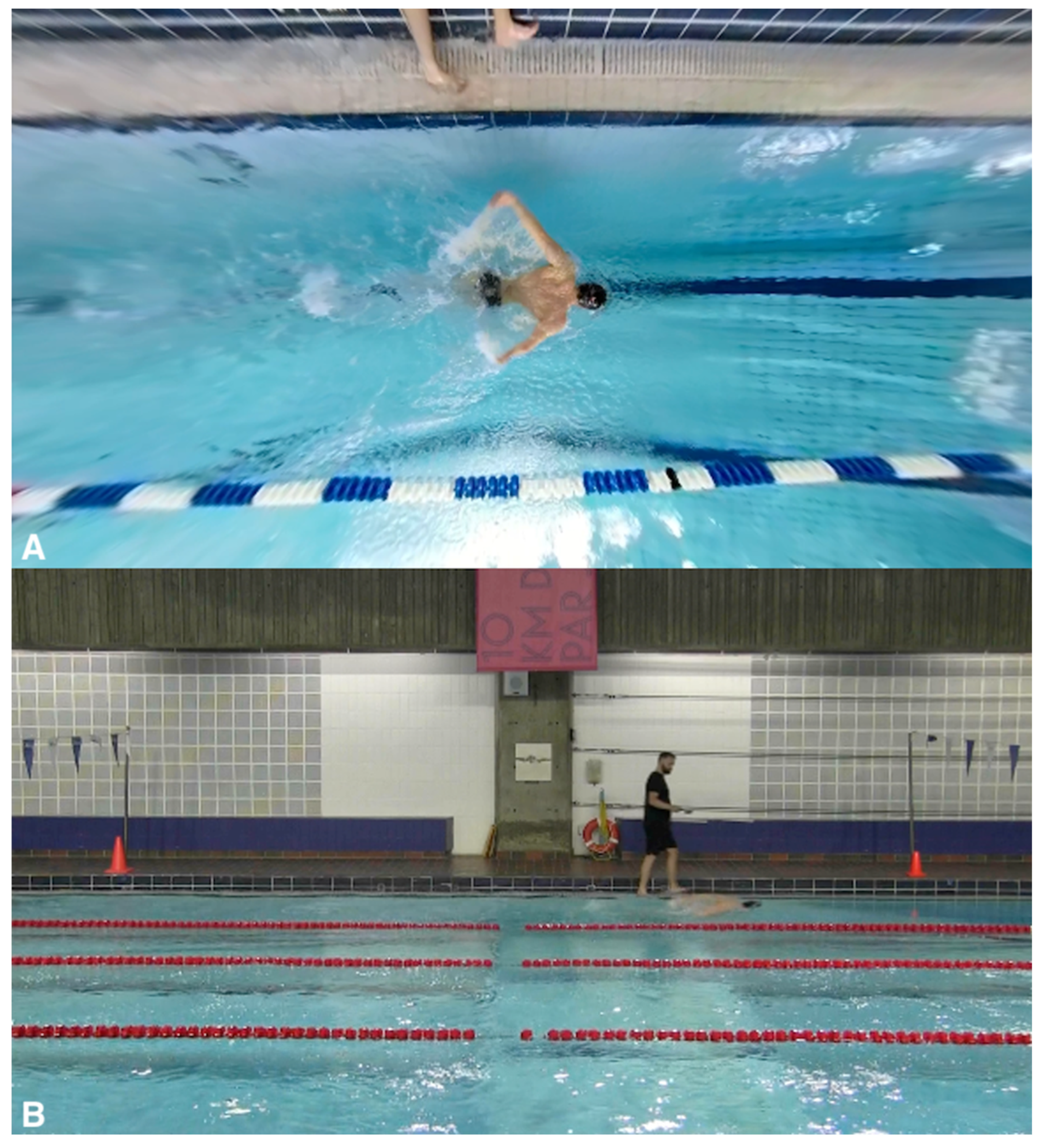
2.4.2. Video Processing
2.5. Statistical Analyses
3. Results
3.1. Stroke Count
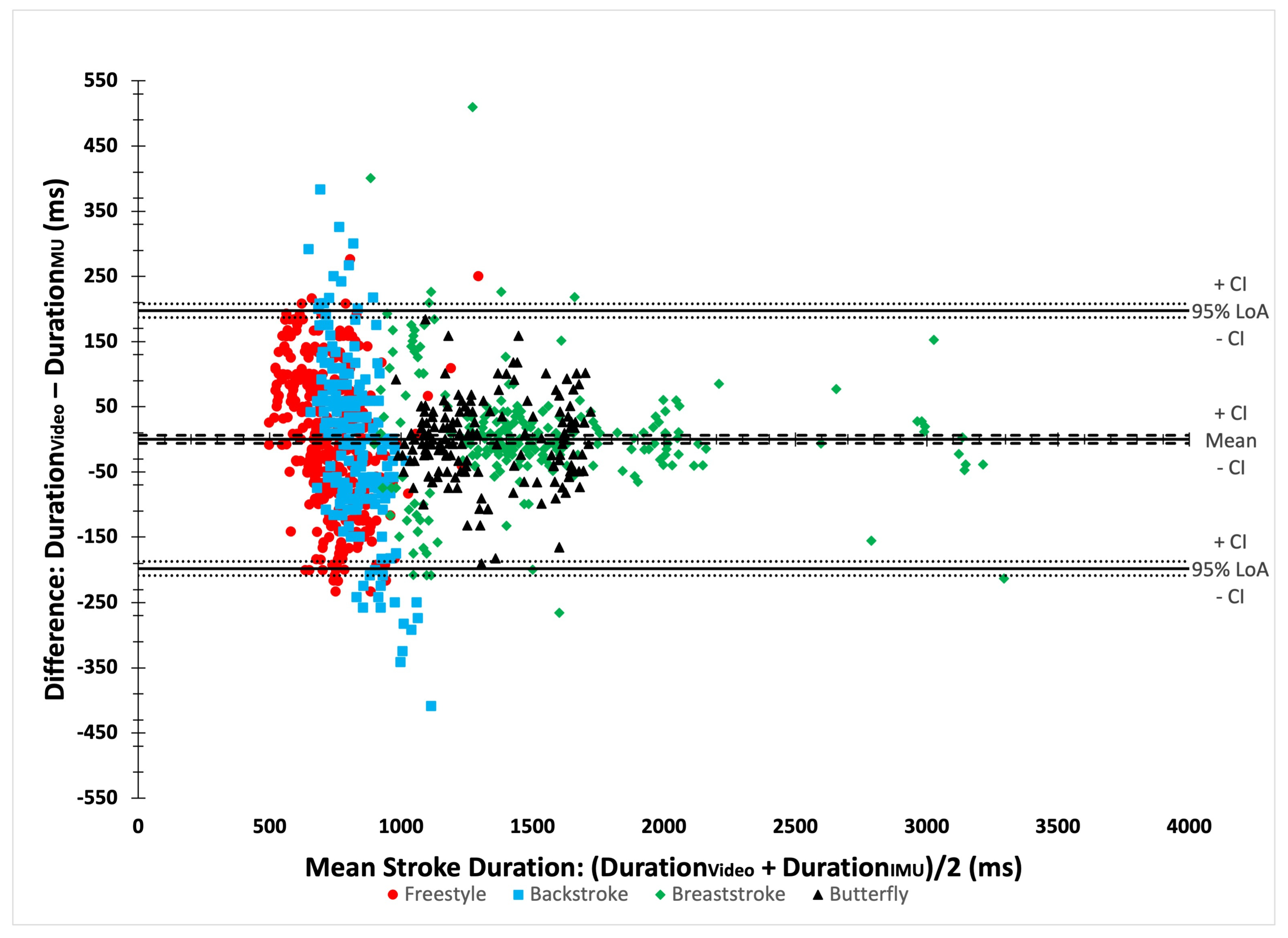
3.2. Stroke Duration
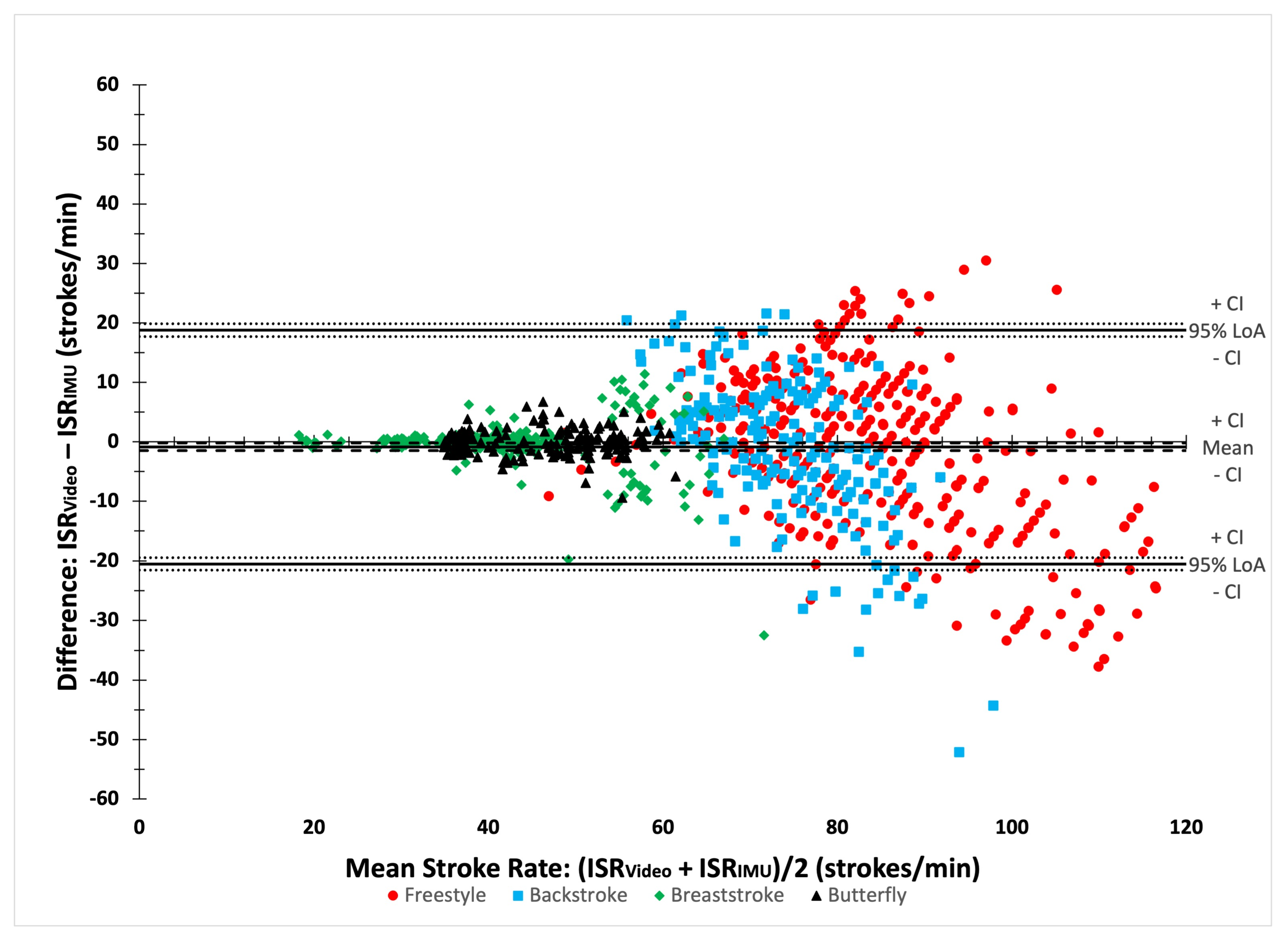
3.3. Instantaneous Stroke Rate (ISR)
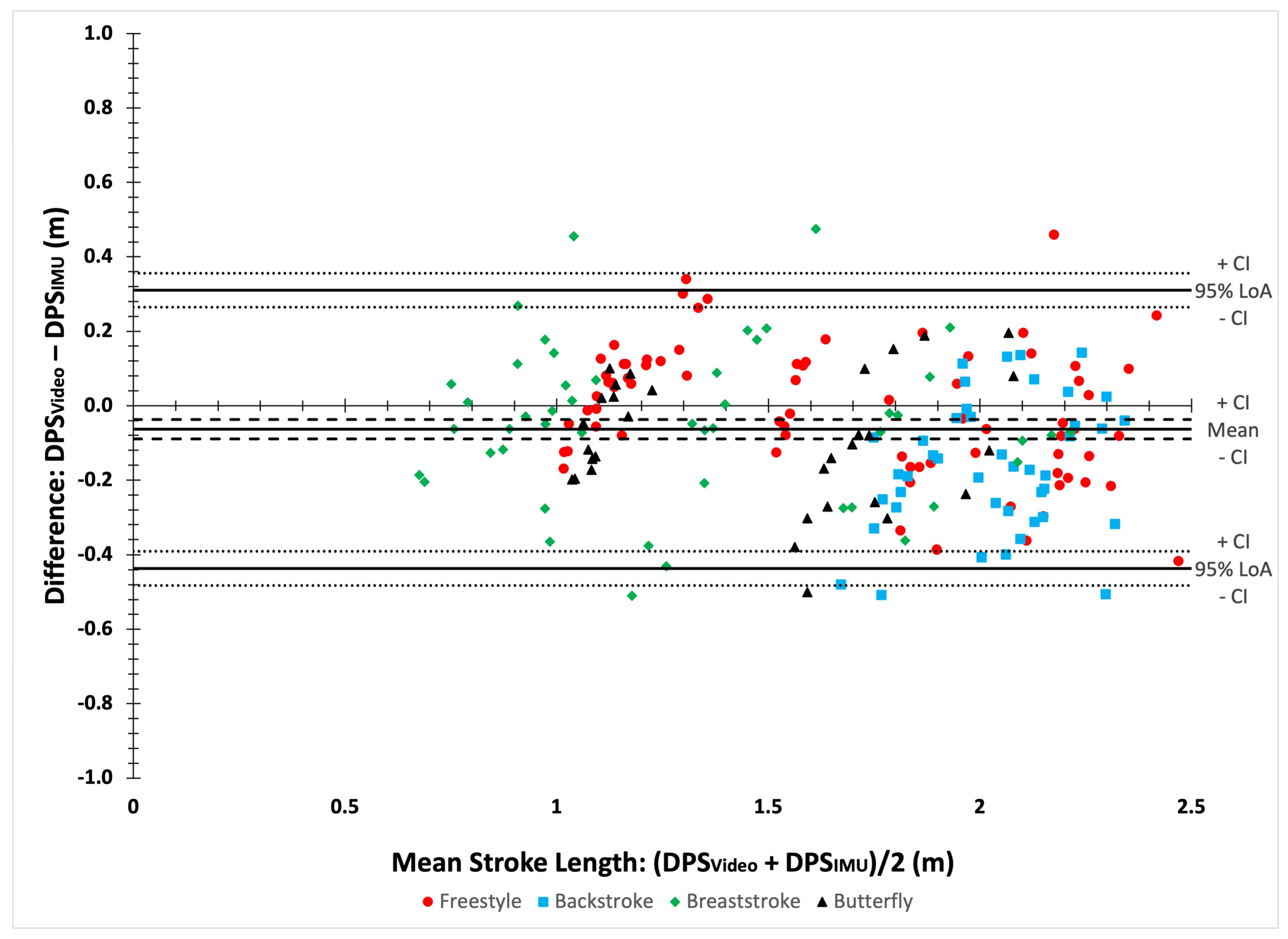
3.4. Distance Per Stroke (DPS)
3.5. Lap Time
4. Discussion
4.1. Stroke Count
4.2. Instantaneous Stroke Rate (ISR)
4.3. Distance per Stroke (DPS)
4.4. Lap Time
4.5. Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sein, M.L.; Walton, J.; Linklater, J.; Appleyard, R.; Kirkbride, B.; Kuah, D.; Murrell, G.A.C. Shoulder pain in elite swimmers: Primarily due to swim-volume-induced supraspinatus tendinopathy. Br. J. Sports Med. 2010, 44, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Zwierzchowska, A.; Gaweł, E.; Rosołek, B. Determinants of the prevalence and location of musculoskeletal pain in elite Para athletes. Medicine 2022, 101, e31268. [Google Scholar] [CrossRef] [PubMed]
- Mooney, R.; Corley, G.; Godfrey, A.; Osborough, C.; Newell, J.; Quinlan, L.R.; Ólaighin, G. Analysis of swimming performance: Perceptions and practices of US-based swimming coaches. J. Sports Sci. 2016, 34, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Beanland, E.; Main, L.C.; Aisbett, B.; Gastin, P.; Netto, K. Validation of GPS and accelerometer technology in swimming. J. Sci. Med. Sport 2014, 17, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, T.M.; Fernandes, R.J.; Keskinen, K.L.; Vilas-Boas, J.P. The influence of stroke mechanics into energy cost of elite swimmers. Eur. J. Appl. Physiol. 2008, 103, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Heinlein, S.A.; Cosgarea, A.J. Biomechanical Considerations in the Competitive Swimmer’s Shoulder. Sports Health A Multidiscip. Approach 2010, 2, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Weldon, E.J.; Richardson, A.B. Upper Extremity Overuse Injuries in Swimming: A Discussion of Swimmer’s Shoulder. Clin. Sports Med. 2001, 20, 423–438. [Google Scholar] [CrossRef]
- De Magalhaes, F.A.; Vannozzi, G.; Gatta, G.; Fantozzi, S. Wearable inertial sensors in swimming motion analysis: A systematic review. J. Sports Sci. 2015, 33, 732–745. [Google Scholar] [CrossRef]
- Guignard, B.; Rouard, A.; Chollet, D.; Seifert, L. Behavioral Dynamics in Swimming: The Appropriate Use of Inertial Measurement Units. Front. Psychol. 2017, 8, 383. [Google Scholar] [CrossRef][Green Version]
- Mooney, R.; Corley, G.; Godfrey, A.; Quinlan, L.; Ólaighin, G. Inertial Sensor Technology for Elite Swimming Performance Analysis: A Systematic Review. Sensors 2015, 16, 18. [Google Scholar] [CrossRef]
- Chakravorti, N.; Le Sage, T.; Slawson, S.E.; Conway, P.P.; West, A.A. Design and Implementation of an Integrated Performance Monitoring Tool for Swimming to Extract Stroke Information at Real Time. IEEE Trans. Hum. Mach. Syst. 2013, 43, 199–213. [Google Scholar] [CrossRef]
- Le Sage, T.; Bindel, A.; Conway, P.; Justham, L.; Slawson, S.; West, A. Development of a real time system for monitoring of swimming performance. Procedia Eng. 2010, 2, 2707–2712. [Google Scholar] [CrossRef]
- Hamidi Rad, M.; Aminian, K.; Gremeaux, V.; Massé, F.; Dadashi, F. Swimming Phase-Based Performance Evaluation Using a Single IMU in Main Swimming Techniques. Front. Bioeng. Biotechnol. 2021, 9, 793302. [Google Scholar] [CrossRef] [PubMed]
- Clément, J.; Charbonneau, M.; Thompson, M. Instantaneous velocity estimation for the four swimming strokes using a 3-axis accelerometer: Validation on paralympic athletes. J. Biomech. 2021, 117, 110261. [Google Scholar] [CrossRef] [PubMed]
- Stamm, A.; James, D.A.; Thiel, D.V. Velocity profiling using inertial sensors for freestyle swimming. Sports Eng. 2013, 16, 1–11. [Google Scholar] [CrossRef]
- Callaway, A. Measuring Kinematic Variables in Front Crawl Swimming Using Accelerometers: A Validation Study. Sensors 2015, 15, 11363–11386. [Google Scholar] [CrossRef] [PubMed]
- Dadashi, F.; Crettenand, F.; Millet, G.P.; Seifert, L.; Komar, J.; Aminian, K. Automatic front-crawl temporal phase detection using adaptive filtering of inertial signals. J. Sports Sci. 2013, 31, 1251–1260. [Google Scholar] [CrossRef]
- Stamm, A.; James, D.; Hagem, R.; Thiel, D. Investigating arm symmetry in swimming using inertial sensors. In Proceedings of the IEEE Sensors, Taipei, Taiwan, 28–31 October 2012; pp. 1–4. [Google Scholar]
- Stamm, A. Investigating Stroke Length and Symmetry in Freestyle Swimming Using Inertial Sensors. In Proceedings of the International Sports Engineering Association, Brisbane, QLD, Australia, 26–29 March 2018. [Google Scholar]
- Hamidi Rad, M.; Gremeaux, V.; Massé, F.; Dadashi, F.; Aminian, K. Monitoring weekly progress of front crawl swimmers using IMU-based performance evaluation goal metrics. Front. Bioeng. Biotechnol. 2022, 10, 910798. [Google Scholar] [CrossRef]
- Fulton, S.K.; Pyne, D.B.; Burkett, B. Validity and reliability of kick count and rate in freestyle using inertial sensor technology. J. Sports Sci. 2009, 27, 1051–1058. [Google Scholar] [CrossRef]
- Fulton, S.K.; Pyne, D.B.; Burkett, B. Quantifying freestyle kick-count and kick-rate patterns in Paralympic swimming. J. Sports Sci. 2009, 27, 1455–1461. [Google Scholar] [CrossRef]
- Regaieg, M.A.; Létocart, A.J.; Bosche, J.; Seifert, L.; Guignard, B. Automatic Detection of Key Points of the Cycle to Assess Upper Limb Coordination in Front Crawl: Effect of Swimming Speed and Impairment. IEEE Sens. J. 2023, 23, 17979–17989. [Google Scholar] [CrossRef]
- Wiesener, C.; Spieker, L.; Axelgaard, J.; Horton, R.; Niedeggen, A.; Wenger, N.; Seel, T.; Schauer, T. Supporting front crawl swimming in paraplegics using electrical stimulation: A feasibility study. J. NeuroEng. Rehabil. 2020, 17, 51. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. Reliability of measurement. In The Design and Analysis of Clinical Experiments; John Wiley & Sons Inc.: New York, NY, USA, 1986; pp. 1–32. [Google Scholar]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Bland, M.J.; Altman, D. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Le Sage, T.; Bindel, A.; Conway, P.P.; Justham, L.M.; Slawson, S.E.; West, A.A. Embedded programming and real-time signal processing of swimming strokes. Sports Eng. 2011, 14, 1. [Google Scholar] [CrossRef]
- James, D.A.; Davey, N.; Rice, T. An accelerometer based sensor platform for insitu elite athlete performance analysis. In Proceedings of the SENSORS, 2004 IEEE, Vienna, Austria, 24–27 October 2004; Volume 1373, pp. 1373–1376. [Google Scholar]
- Davey, N.; James, D.; Anderson, M. Signal Analysis of Accelerometry Data Using Gravity-Based Modeling; SPIE: Bellingham, DC, USA, 2004; Volume 5274. [Google Scholar]
- Davey, N.; Anderson, M.; James, D. An Accelerometer-Based System for Elite Athlete Swimming Performance Analysis; SPIE: Bellingham, DC, USA, 2005; Volume 5649. [Google Scholar]
- Daukantas, S.; Marozas, V.; Lukosevicius, A. Inertial sensor for objective evaluation of swimmer performance. In Proceedings of the 2008 11th International Biennial Baltic Electronics Conference, Tallinn, Estonia, 6–8 October 2008; pp. 321–324. [Google Scholar]
- Lee, M.; Lee, M.; Lee, M. Accuracy of swimming wearable watches for estimating energy expenditure. Int. J. Appl. Sports Sci. 2018, 30, 80–90. [Google Scholar] [CrossRef]
- Pla, R.; Ledanois, T.; Simbana, E.D.; Aubry, A.; Tranchard, B.; Toussaint, J.-F.; Sedeaud, A.; Seifert, L. Spatial-temporal variables for swimming coaches: A comparison study between video and TritonWear sensor. Int. J. Sports Sci. Coach. 2021, 16, 1271–1280. [Google Scholar] [CrossRef]
- Adesida, Y.; Papi, E.; McGregor, A.H. Exploring the Role of Wearable Technology in Sport Kinematics and Kinetics: A Systematic Review. Sensors 2019, 19, 1597. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Athlete ID | Disabilities | Classes | Swimming Strokes |
|---|---|---|---|
| 1 | Right femoral-fibula-ulnar syndrome; Dysmeliac right upper limb | S8, SB7, SM8 | FY, BK, BR, FR |
| 2 | Intellectual Impairment | S14, SB14, SM14 | FY, BK, BR, FR |
| 3 | Dysmelia, congenital left hand amputee | S10, SB9, SM10 | FY, BK, BR, FR |
| 4 | Cerebral palsy | S9, SB8, SM9 | FY, BK, BR, FR |
| 5 | Pseudoachondroplasia | S5, SB5, SM5 | BR, FR |
| 6 | Achondroplasia dwarfism | S6, SB6, SM6 | BK, BR, FR |
| 7 | Stroke (post-bleeding aneurysm) | S7, SB6, SM7 | FY, BK, BR, FR |
| 8 | Congenital impaired strength loss at the left hip, knee, and ankle with associated foot deformity | SB9 | FY, BK, BR, FR |
| Stroke Parameter | Unit | IMU Description | Video Camera | Video Description |
|---|---|---|---|---|
| Stroke count (SC) | count | Sum of detected stroke cycles per lap. | Above swimmer | Sum of tagged stroke cycles per lap. |
| Stroke duration | ms | Time difference between the nth and nth + 1 stroke cycle start points. | Above swimmer | Time difference between the nth and nth + 1 stroke cycle starting points. |
| Instantaneous stroke rate | Strokes/min | Estimated rate of strokes per minute (60/duration of a given stroke in seconds). | Above swimmer | Stroke duration (s) divided by 60 s. |
| Distance per stroke (DPS) | m | Displacement between the nth and nth + 1 stroke cycle start points. | Stationary and above swimmer | Displacement (stationary camera) between the nth and nth + 1 stroke cycle starting points (taken from the above swimmer camera). |
| Lap Time | s | Time difference between the 1st and 5th manually defined swim events. | Above swimmer | Time difference between the first frame where the athlete initiated the dive and the first frame where the athlete touched the wall. |
| Stroke Style | Definition of the Start of the Stroke Cycle |
|---|---|
| Freestyle | The start of torso rotation as the arm recovery phase is ending. |
| Backstroke | The start of the arm pull phase after the catch phase has finished. |
| Breaststroke | The start of the arm-pull phase after the sculling-out movement has finished. |
| Butterfly | The start of the arm pull phase after the catch phase has finished. |
| N | RMSE (Strokes) | Count Mean ± SD | Bias (Strokes) [95% CI] | 95% Limits of Agreement [95% CI] | ICC [95% CI] | SEM (Strokes) | CV | MAPE (%) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lower Limit (Strokes) | Upper Limit (Strokes) | IMU | Video | ||||||||
| Overall | 28 | 0.49 | 27.54 ± 9.73 | 0.13 [−0.05; 0.30] | −0.82 [1.13; 0.51] | 1.07 [0.76; 1.38] | 0.97 [0.93; 0.98] | 1.72 | 35.37 | 35.28 | 0.66 |
| Freestyle | 8 | 0.59 | 25.59 ± 9.49 | 0.31 [−0.06; 0.68] | −0.73 [−1.36; −0.09] | 1.35 [0.72; 1.99] | 1 [0.99; 1] | 0 | 36.58 | 37.58 | 0.91 |
| Backstroke | 7 | 0.38 | 24.14 ± 7.40 | 0.29 [0.09; 0.48] | −0.24 [−0.58; 0.10] | 0.81 [0.47; 1.15] | 1 [0.99; 1] | 0 | 30.54 | 30.81 | 1.10 |
| Breaststroke | 8 | 0.66 | 32.07 ± 12.54 | −0.14 [−0.65; 0.37] | −1.50 [−2.38; −0.61] | 1.21 [0.32; 2.10] | 1 [0.99; 1] | 0 | 39.25 | 38.99 | 1.71 |
| Butterfly | 6 | 0 | 28.83 ± 8.80 | 0 [0; 0] | 0 [0; 0] | 0 [0; 0] | 1 [1; 1] | 0 | 30.51 | 30.51 | 0 |
| N | RMSE (ms) | Duration (ms) Mean ± SD | Bias (ms) [95% CI] | 95% Limits of Agreement [95% CI] | ICC [95% CI] | SEM (ms) | CV | MAPE (%) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lower Limit (ms) | Upper Limit (ms) | IMU | Video | ||||||||
| Overall | 1011 | 100.81 | 1042 ± 430 | −0.15 [−6.37; 6.07] | −197.83 [−187.06; −208.59] | 197.53 [186.76; 208.29] | 0.97 [0.97; 0.98] | 75.05 | 41.93 | 41.25 | 8.78 |
| Freestyle | 399 | 103.05 | 735 ± 114 | 0.17 [−9.95; 10.30] | −202.05 [−219.59; −184.52] | 202.40 [184.86; 219.94] | 0.66 [0.60; 0.71] | 72.81 | 18.87 | 14.84 | 11.78 |
| Backstroke | 200 | 132.03 | 1605 ± 831 | −4.51 [−22.84; 13.83] | −263.79 [−295.55; −231.28] | 254.78 [223.02; 286.53] | 0.30 [0.17; 0.42] | 93.15 | 16.78 | 9.00 | 12.48 |
| Breaststroke | 245 | 87.97 | 1322 ± 224 | 3.47 [−7.56; 14.51] | −166.17 [−184.95; −147.40] | 173.12 [154.35; 191.89] | 0.98 [0.97; 0.99] | 67.32 | 31.52 | 30.95 | 4.34 |
| Butterfly | 167 | 62.58 | 826 ± 89 | −1.01 [−10.53; 8.51] | −124.01 [−140.50; −107.53] | 121.99 [105.51; 138.48] | 0.96 [0.95; 0.97] | 45.04 | 17.07 | 17.18 | 3.71 |
| N | RMSE (Strokes/min) | ISR (Strokes/min) Mean ± SD | Bias (Strokes/min) [95% CI] | 95% Limits of Agreement [95% CI] | ICC [95% CI] | SEM (Strokes/min) | CV | MAPE (%) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lower Limit (Strokes/min) | Upper Limit (Strokes/min) | IMU | Video | ||||||||
| Overall | 1011 | 10.05 | 65.74 ± 21.27 | −0.84 [−1.46; −0.22] | −20.48 [−21.55; −19.41] | 18.80 [17.73; 18.80] | 0.90 [0.88; 0.91] | 6.98 | 35.29 | 32.00 | 8.97 |
| Freestyle | 399 | 12.90 | 83.91 ± 13.03 | −1.45 [−2.71; 0.19] | −26.61 [−28.79; −24.61] | 23.71 [21.53; 25.89] | 0.61 [0.54; 0.67] | 9.08 | 20.03 | 13.95 | 12.02 |
| Backstroke | 200 | 12.31 | 73.94 ± 8.01 | −1.06 [−2.77; 0.64] | −25.17 [−28.12; −22.16] | 23.04 [20.09; 26.00] | 0.26 [0.12; 0.38] | 8.69 | 16.97 | 9.06 | 12.84 |
| Breaststroke | 245 | 4.30 | 41.95 ± 11.45 | −0.26 [−0.81; 0.28] | −8.78 [−9.72; −7.83] | 8.25 [7.31; 9.19] | 0.92 [0.90; 0.94] | 3.29 | 28.29 | 27.21 | 4.52 |
| Butterfly | 167 | 2.25 | 46.65 ± 7.58 | 0.05 [−0.29; 0.39] | −4.38 [−4.97; −3.79] | 4.47 [3.88; 5.07] | 0.96 [0.94; 0.97] | 1.53 | 16.41 | 16.48 | 3.70 |
| N | RMSE (m) | DPS (m) Mean ± SD | Bias (m) [95% CI] | 95% Limits of Agreement [95% CI] | ICC [95% CI] | SEM (m) | CV | MAPE (%) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lower Limit (m) | Upper Limit (m) | IMU | Video | ||||||||
| Overall | 198 | 0.20 | 1.63 ± 0.47 | −0.06 [−0.09; −0.04] | −0.44 [−0.48; −0.39] | 0.31 [0.26; 0.36] | 0.91 [0.88; 0.93] | 0.14 | 29.61 | 28.54 | 10.78 |
| Freestyle | 75 | 0.17 | 1.68 ± 0.46 | −0.01 [−0.05; 0.03] | −0.35 [−0.42; −0.28] | 0.33 [0.27; 0.40] | 0.93 [0.89; 0.96] | 0.12 | 29.41 | 26.30 | 8.54 |
| Backstroke | 43 | 0.24 | 2.03 ± 0.18 | −0.16 [−0.21; −0.11] | −0.50 [−0.59; −0.41] | 0.18 [0.09; 0.18] | 0.39 [0.11; 0.62] | 0.17 | 8.46 | 11.13 | 10.55 |
| Breaststroke | 48 | 0.21 | 1.31 ± 0.44 | −0.04 [−0.10; 0.01] | −0.45 [−0.55; 0.35] | 0.36 [0.26; 0.47] | 0.89 [0.81; 0.94] | 0.15 | 34.13 | 34.67 | 14.15 |
| Butterfly | 32 | 0.19 | 1.48 ± 0.36 | −0.09 [−0.15; −0.03] | −0.42 [−0.53; −0.32] | 0.24 [0.14; 0.34] | 0.87 [0.75; 0.93] | 0.13 | 23.93 | 25.56 | 11.31 |
| N | RMSE (s) | Lap Time (s) Mean ± SD | Bias (s) [95% CI] | 95% Limits of Agreement [95% CI] | ICC [95% CI] | SEM (s) | CV | MAPE (%) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lower Limit (s) | Upper Limit (s) | IMU | Video | ||||||||
| Overall | 30 | 0.15 | 48.29 ± 16.35 | 0.04 [−0.09; 0.02] | −0.34 [−0.43; −0.24] | 0.26 [0.17; 0.35] | 1 [1; 1] | 0 | 33.87 | 33.86 | 0.32 |
| Freestyle | 8 | 0.16 | 42.04 ± 13.43 | −0.10 [−0.19; 0.01] | −0.35 [−0.51; −0.20] | 0.16 [0.00; 0.32] | 1 [1; 1] | 0 | 31.84 | 32.05 | 0.39 |
| Backstroke | 6 | 0.14 | 46.11 ± 8.50 | −0.03 [−0.15; 0.09] | −0.32 [−0.52; 0.12] | 0.26 [0.05; 0.46] | 1 [1; 1] | 0 | 18.50 | 18.37 | 0.28 |
| Breaststroke | 8 | 0.12 | 57.16 ± 19.37 | −0.01 [−0.10; 0.08] | −0.26 [−0.41; 0.11] | 0.23 [0.08; 0.38] | 1 [1; 1] | 0 | 33.91 | 33.87 | 0.17 |
| Butterfly | 8 | 0.19 | 47.31 ± 19.00 | −0.01 [−0.15; 0.13] | −0.41 [−0.65; −0.16] | 0.39 [0.14; 0.63] | 1 [1; 1] | 0 | 40.25 | 40.07 | 0.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slopecki, M.; Charbonneau, M.; Lavallière, J.-M.; Côté, J.N.; Clément, J. Validation of Automatically Quantified Swim Stroke Mechanics Using an Inertial Measurement Unit in Paralympic Athletes. Bioengineering 2024, 11, 15. https://doi.org/10.3390/bioengineering11010015
Slopecki M, Charbonneau M, Lavallière J-M, Côté JN, Clément J. Validation of Automatically Quantified Swim Stroke Mechanics Using an Inertial Measurement Unit in Paralympic Athletes. Bioengineering. 2024; 11(1):15. https://doi.org/10.3390/bioengineering11010015
Chicago/Turabian StyleSlopecki, Matthew, Mathieu Charbonneau, Jean-Michel Lavallière, Julie N. Côté, and Julien Clément. 2024. "Validation of Automatically Quantified Swim Stroke Mechanics Using an Inertial Measurement Unit in Paralympic Athletes" Bioengineering 11, no. 1: 15. https://doi.org/10.3390/bioengineering11010015
APA StyleSlopecki, M., Charbonneau, M., Lavallière, J.-M., Côté, J. N., & Clément, J. (2024). Validation of Automatically Quantified Swim Stroke Mechanics Using an Inertial Measurement Unit in Paralympic Athletes. Bioengineering, 11(1), 15. https://doi.org/10.3390/bioengineering11010015