

Zirconia Dental Implants: A Closer Look at Surface Condition and Intrinsic Composition by SEM-EDX

Abstract
:1. Introduction
2. Materials and Method
2.1. Cutting off the Implants
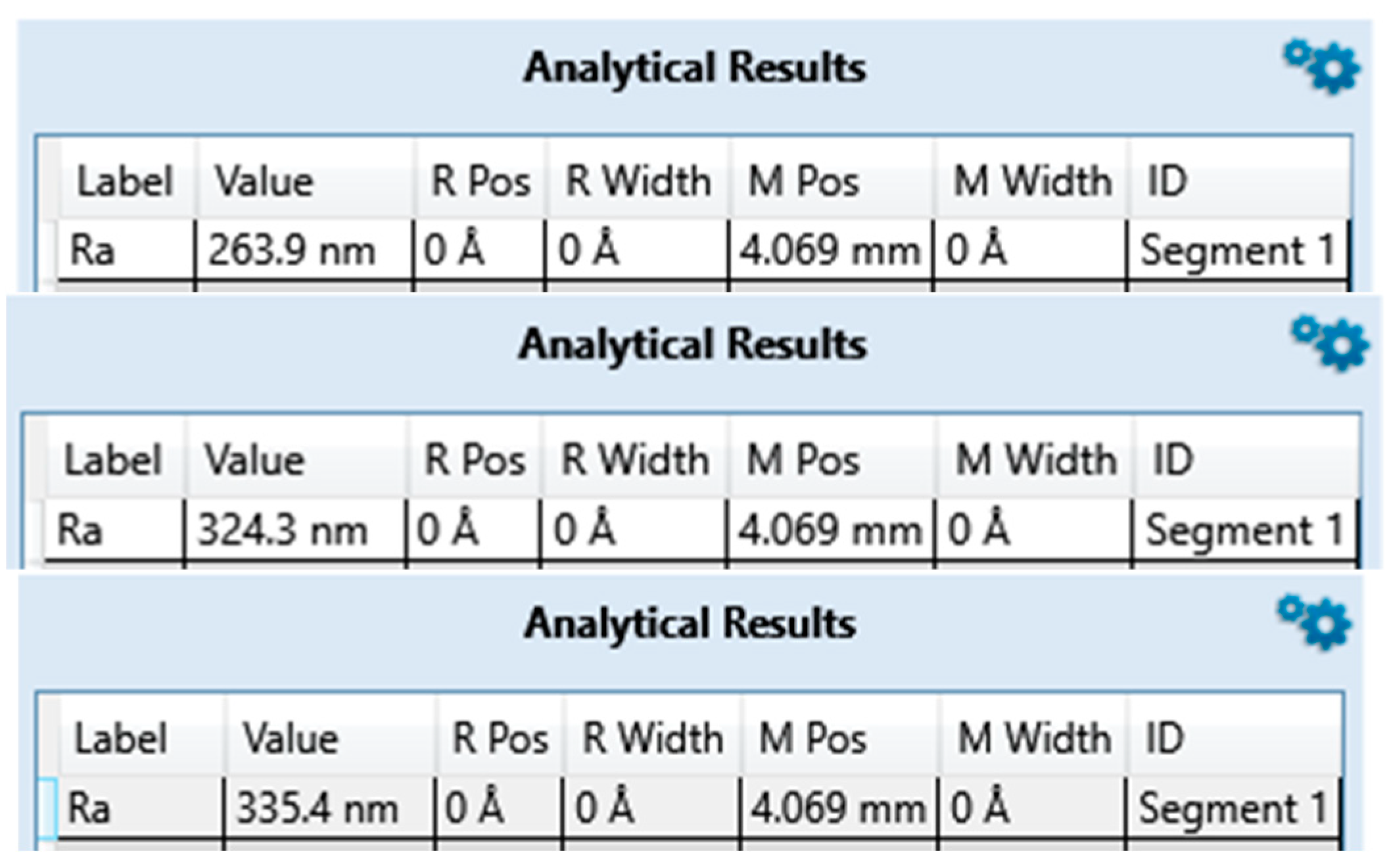
2.2. Surface Characterization with Tactile Profilometer
- Measurement length: 200 μm.
- Long cut OFF: 0.8 μm/short cut OFF: 0.08 µm.
2.3. SEM-EDS Composition Analysis
3. Results
3.1. Surface Roughness
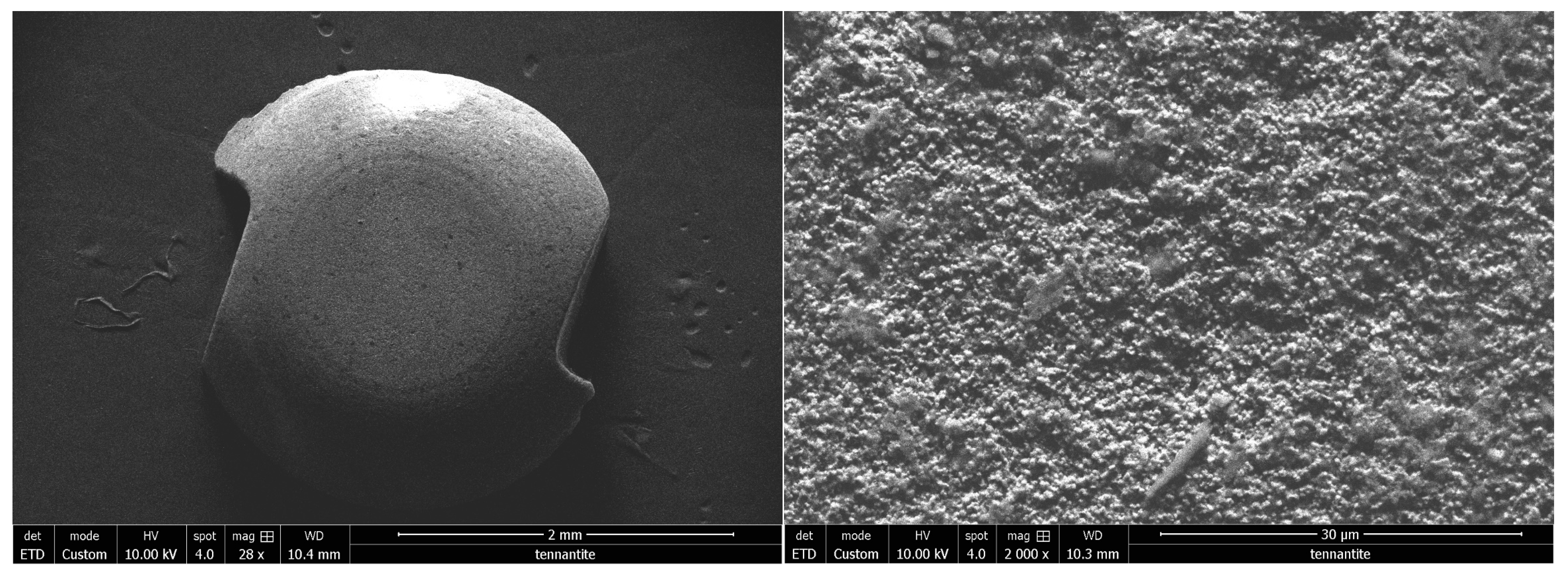
3.2. Scanning Electron Microscope Observation
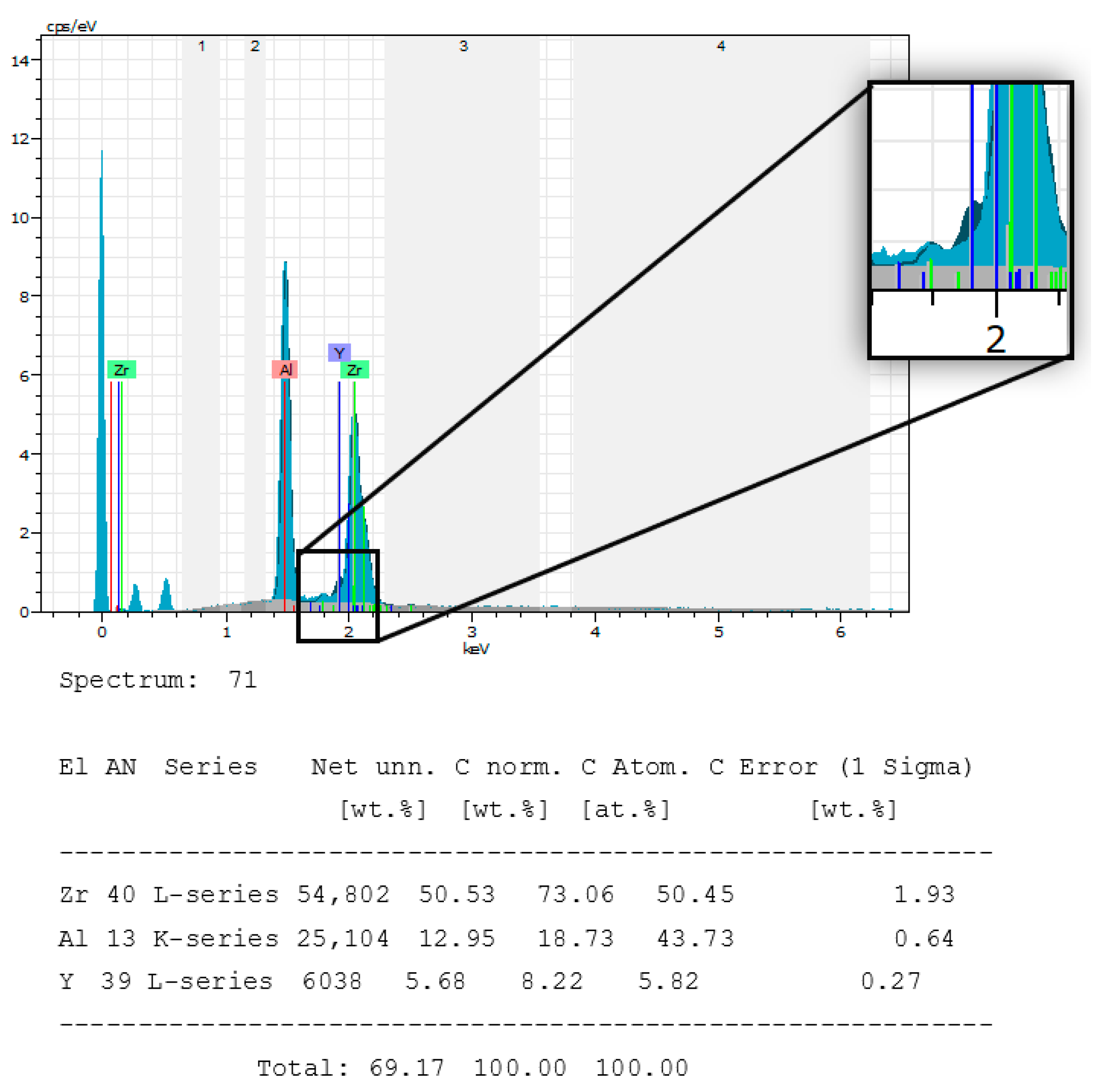
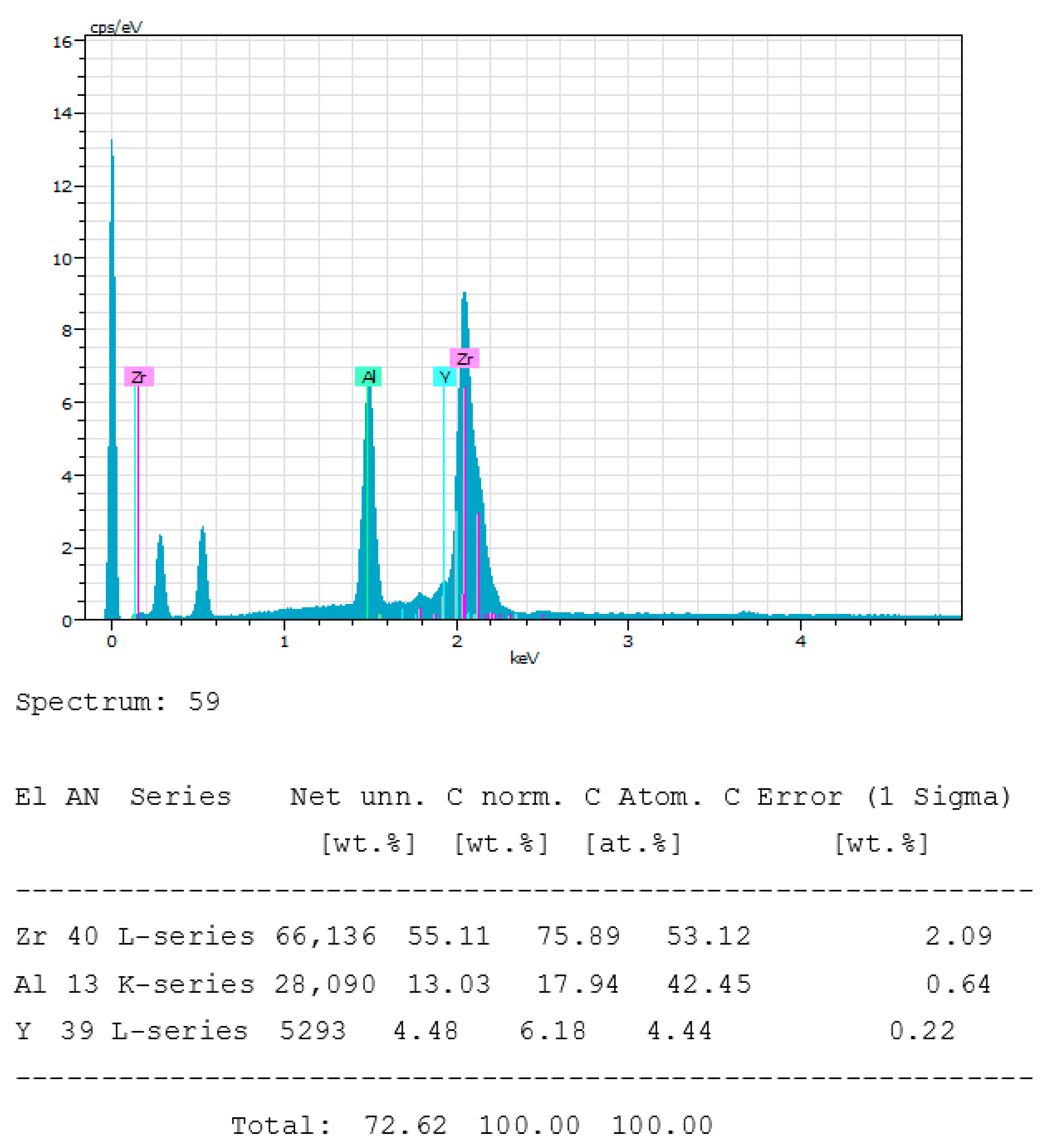
3.3. SEM-EDS Composition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaur, M.; Singh, K. Review on titanium and titanium based alloys as biomaterials for orthopaedic applications. Mater. Sci. Eng. C 2019, 102, 844–862. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, H.; Takeuchi, Y.; Imai, H.; Kawai, T.; Yoneyama, T. Application of titanium and titanium alloys to fixed dental prostheses. J. Prosthodont. Res. 2019, 63, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Niinomi, M. Mechanical properties of biomedical titanium alloys. Mater. Sci. Eng. A 1998, 243, 231–236. [Google Scholar] [CrossRef]
- Dias Corpa Tardelli, J.; Bolfarini, C.; Cândido dos Reis, A. Comparative analysis of corrosion resistance between beta titanium and Ti-6Al-4V alloys: A systematic review. J. Trace Elem. Med. Biol. 2020, 62, 126618. [Google Scholar] [CrossRef]
- Prando, D.; Brenna, A.; Diamanti, M.V.; Beretta, S.; Bolzoni, F.; Ormellese, M.; Pedeferri, M. Corrosion of Titanium: Part 1: Aggressive Environments and Main Forms of Degradation. J. Appl. Biomater. Funct. Mater. 2017, 15, e291–e302. [Google Scholar] [CrossRef]
- Piconi, C.; Maccauro, G.; Muratori, F.; Brach Del Prever, E. Alumina and zirconia ceramics in joint replacements. J. Appl. Biomater. Biomech. 2003, 1, 19–32. [Google Scholar]
- Garvie, R.C.; Hannink, R.H.; Pascoe, R.T. Ceramic steel? Nature 1975, 258, 703–704. [Google Scholar] [CrossRef]
- Uo, M.; Sjoren, G.; Sundh, A.; Watari, F.; Bergman, M.; Lerner, U. Cytotoxicity and bonding property of dental ceramics. Dent. Mater. 2003, 19, 487–492. [Google Scholar] [CrossRef]
- Rimondini, L.; Cerroni, L.; Carrassi, A.; Torricelli, P. Bacterial colonization of zirconia ceramic surfaces: An in vitro and in vivo study. Int. J. Oral Maxillofac. Implant. 2002, 17, 793–798. [Google Scholar]
- EJung, R.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.S.; Thoma, D. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implant. Res. 2012, 23, 2–21. [Google Scholar] [CrossRef]
- Tchinda, A.; Pierson, G.; Chezeau, L.; Kouitat-Njiwa, R.; Rihn, B.H.; Bravetti, P. Desulfovibrio fairfieldensis adhesion on implantable titanium used in odontology: A preliminary study. Cell. Mol. Biol. 2021, 67, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Roehling, S.; Schlegel, K.A.; Woelfler, H.; Gahlert, M. Zirconia compared to titanium dental implants in preclinical studies—A systematic review and meta-analysis. Clin. Oral Implant. Res. 2019, 30, 365–395. [Google Scholar] [CrossRef] [PubMed]
- Tchinda, A.; Chézeau, L.; Pierson, G.; Kouitat-Njiwa, R.; Rihn, B.H.; Bravetti, P. Biocompatibility of ZrO2 vs. Y-TZP Alloys: Influence of Their Composition and Surface Topography. Materials 2022, 15, 4655. [Google Scholar] [CrossRef] [PubMed]
- Covacci, V.; Bruzzese, N.; Maccauro, G.; Andreassi, C.; Ricci, G.A.; Piconi, C.; Marmo, E.; Burger, W.; Cittadini, A. In vitro evaluation of the mutagenic and carcinogenic power of high purity zirconia ceramic. Biomaterials 1999, 20, 371–376. [Google Scholar] [CrossRef]
- Pourquoi la Biocompatibilité est si Importante en Implantologie ? AOnews le Magazine Dentaire qui Nous Rassemble. Available online: http://www.aonews-lemag.fr/ao-33-pourquoi-biocompatibilité-importante-en-implantologie-avril-2020/ (accessed on 12 May 2022).
- Phénomène D’électrogalvanisme en Implantologie Orale: Revue de la Littérature. Available online: https://123dok.net/document/nzwkplze-phenomene-electrogalvanisme-implantologie-orale-revue-litterature.html (accessed on 12 May 2022).
- Schwartz, Z.; Nasazky, E.; Boyan, B.D. Surface microtopography regulates osteointegration: The role of implant surface microtopography in osteointegration. Alpha Omegan 2005, 98, 9–19. [Google Scholar]
- Bernard, J.-P.; Szmukler-Moncler, S.; Pessotto, S.; Vazquez, L.; Belser, U.C. The anchorage of Brånemark ITI implants of different lengths, I. An experimental study in the canine mandible. Clin. Oral Implant. Res. 2003, 14, 593–600. [Google Scholar] [CrossRef]
- Persson, L.G.; Berglundh, T.; Lindhe, J.; Sennerby, L. Re-osseointegration after treatment of peri-implantitis at different implant surfaces. An experimental study in the dog. Clin. Oral Implant. Res. 2001, 12, 595–603. [Google Scholar] [CrossRef]
- Tchinda, A.P.; Pierson, G.; Kouitat-Njiwa, R.; Bravetti, P. The Surface Conditions and Composition of Titanium Alloys in Implantology: A Comparative Study of Dental Implants of Different Brands. Materials 2022, 15, 1018. [Google Scholar] [CrossRef]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammächer, C.; Stein, J.M. Definition, etiology, prevention and treatment of peri-implantitis--a review. Head. Face Med. 2014, 10, 34. [Google Scholar] [CrossRef]
- Jordana, F.; Susbielles, L.; Colat-Parros, J. Periimplantitis and Implant Body Roughness: A Systematic Review of Literature. Implant. Dent. 2018, 27, 672–681. [Google Scholar] [CrossRef]
- Sridhar, S.; Wang, F.; Wilson, T.G.; Palmer, K.; Valderrama, P.; Rodrigues, D.C. The role of bacterial biofilm and mechanical forces in modulating dental implant failures. J. Mech. Behav. Biomed. Mater. 2019, 92, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Perumal, G.; Grewal, H.S.; Pole, M.; Reddy, L.V.K.; Mukherjee, S.; Singh, H.; Manivasagam, G.; Arora, H.S. Enhanced Biocorrosion Resistance and Cellular Response of a Dual-Phase High Entropy Alloy through Reduced Elemental Heterogeneity. ACS Appl. Bio Mater. 2020, 3, 1233–1244. [Google Scholar] [CrossRef]
- Cordeiro, J.M.; Barão, V.A.R. Is there scientific evidence favoring the substitution of commercially pure titanium with titanium alloys for the manufacture of dental implants? Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 71, 1201–1215. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Wang, P.; Shen, T.; Hu, C.; Han, Y.; Song, M.; Bian, Y.; Li, Y.; Zhu, Y. Aluminum Trichloride Inhibited Osteoblastic Proliferation and Downregulated the Wnt/β-Catenin Pathway. Biol. Trace Elem. Res. 2017, 177, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Huo, H.; Xiu, C.; Song, M.; Han, Y.; Li, Y.; Zhu, Y. Inhibition of osteoblast differentiation by aluminum trichloride exposure is associated with inhibition of BMP-2/Smad pathway component expression. Food Chem. Toxicol. 2016, 97, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Ren, L.; Song, M.; Shao, B.; Han, Y.; Cao, Z.; Li, Y. Fas- and Mitochondria-Mediated Signaling Pathway Involved in Osteoblast Apoptosis Induced by AlCl3. Biol. Trace Elem. Res. 2018, 184, 173–185. [Google Scholar] [CrossRef]
- Yu, H.; Zhang, J.; Ji, Q.; Yu, K.; Wang, P.; Song, M.; Cao, Z.; Zhang, X.; Li, Y. Melatonin alleviates aluminium chloride-induced immunotoxicity by inhibiting oxidative stress and apoptosis associated with the activation of Nrf2 signaling pathway. Ecotoxicol. Environ. Saf. 2019, 173, 131–141. [Google Scholar] [CrossRef]
- Igbokwe, I.O.; Igwenagu, E.; Igbokwe, N.A. Aluminium toxicosis: A review of toxic actions and effects. Interdiscip. Toxicol. 2019, 12, 45–70. [Google Scholar] [CrossRef]
- Mirza, A.; King, A.; Troakes, C.; Exley, C. Aluminium in brain tissue in familial Alzheimer’s disease. J. Trace Elem. Med. Biol. 2017, 40, 30–36. [Google Scholar] [CrossRef]
- Mold, M.; Cottle, J.; Exley, C. Aluminium in Brain Tissue in Epilepsy: A Case Report from Camelford. Int. J. Environ. Res. Public Health 2019, 16, 2129. [Google Scholar] [CrossRef]
- Kumar, V.; Gill, K.D. Aluminium neurotoxicity: Neurobehavioural and oxidative aspects. Arch. Toxicol. 2009, 83, 965–978. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ZrO2-1 | ZrO2-2 | ZrO2-3 | |
|---|---|---|---|
| Brands | Nobel® | Metoxit® | Z-systems® |
| Model | NobelPearl | Ziraldent FR2 | Z look 3 Evo |
| Dimensions | 4.2 × 10 | 4 × 9 | 5 × 13 |
| ZrO2-1 | ZrO2-2 | ZrO2-3 | |
|---|---|---|---|
| Brands | Nobel® | Metoxit® | Z-systems® |
| Model | NobelPearl | Ziraldent FR2 | Z look 3 Evo |
| Ra (µm) Announced | Not specified | 2 | 3.62 |
| Ra (µm) Measured | 0.307 | 0.677 | 0.823 |
| Nobelpearl (ZrO2-1) | ZrO2 | Al2O3 | Y2O3 |
|---|---|---|---|
| Reported composition | Not specified | ||
| Measured composition | 50.45% | 43.73% | 5.82% |
| Ziraldent FR2 (ZrO2-2) | ZrO2 | Al2O3 | Y2O3 |
|---|---|---|---|
| Reported composition | >99.5% | ||
| Measured composition | 53.12% | 42.45% | 4.44% |
| Z Look 3 (ZrO2-3) | ZrO2 | Al2O3 | Y2O3 |
|---|---|---|---|
| Reported composition | 95% | 0.25% | 5% |
| Measured composition | 75.36% | 14.37% | 10.27% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tchinda, A.; Lerebours, A.; Kouitat-Njiwa, R.; Bravetti, P. Zirconia Dental Implants: A Closer Look at Surface Condition and Intrinsic Composition by SEM-EDX. Bioengineering 2023, 10, 1102. https://doi.org/10.3390/bioengineering10091102
Tchinda A, Lerebours A, Kouitat-Njiwa R, Bravetti P. Zirconia Dental Implants: A Closer Look at Surface Condition and Intrinsic Composition by SEM-EDX. Bioengineering. 2023; 10(9):1102. https://doi.org/10.3390/bioengineering10091102
Chicago/Turabian StyleTchinda, Alex, Augustin Lerebours, Richard Kouitat-Njiwa, and Pierre Bravetti. 2023. "Zirconia Dental Implants: A Closer Look at Surface Condition and Intrinsic Composition by SEM-EDX" Bioengineering 10, no. 9: 1102. https://doi.org/10.3390/bioengineering10091102
APA StyleTchinda, A., Lerebours, A., Kouitat-Njiwa, R., & Bravetti, P. (2023). Zirconia Dental Implants: A Closer Look at Surface Condition and Intrinsic Composition by SEM-EDX. Bioengineering, 10(9), 1102. https://doi.org/10.3390/bioengineering10091102