
Stress Effect in the Knee Joint Based on the Fibular Osteotomy Level and Varus Deformity: A Finite Element Analysis Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
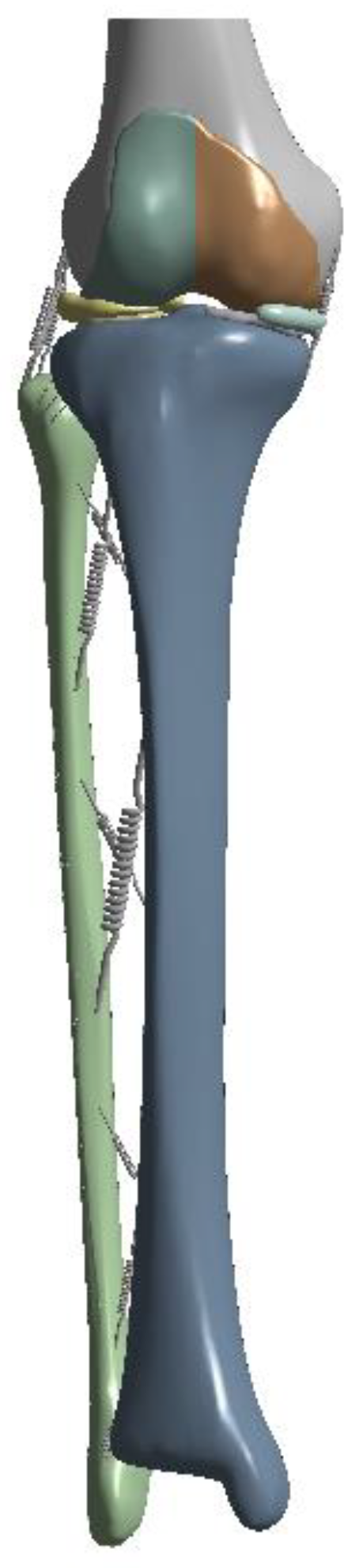
2.1. Construction of a Bone Model Based on Patient Image Data
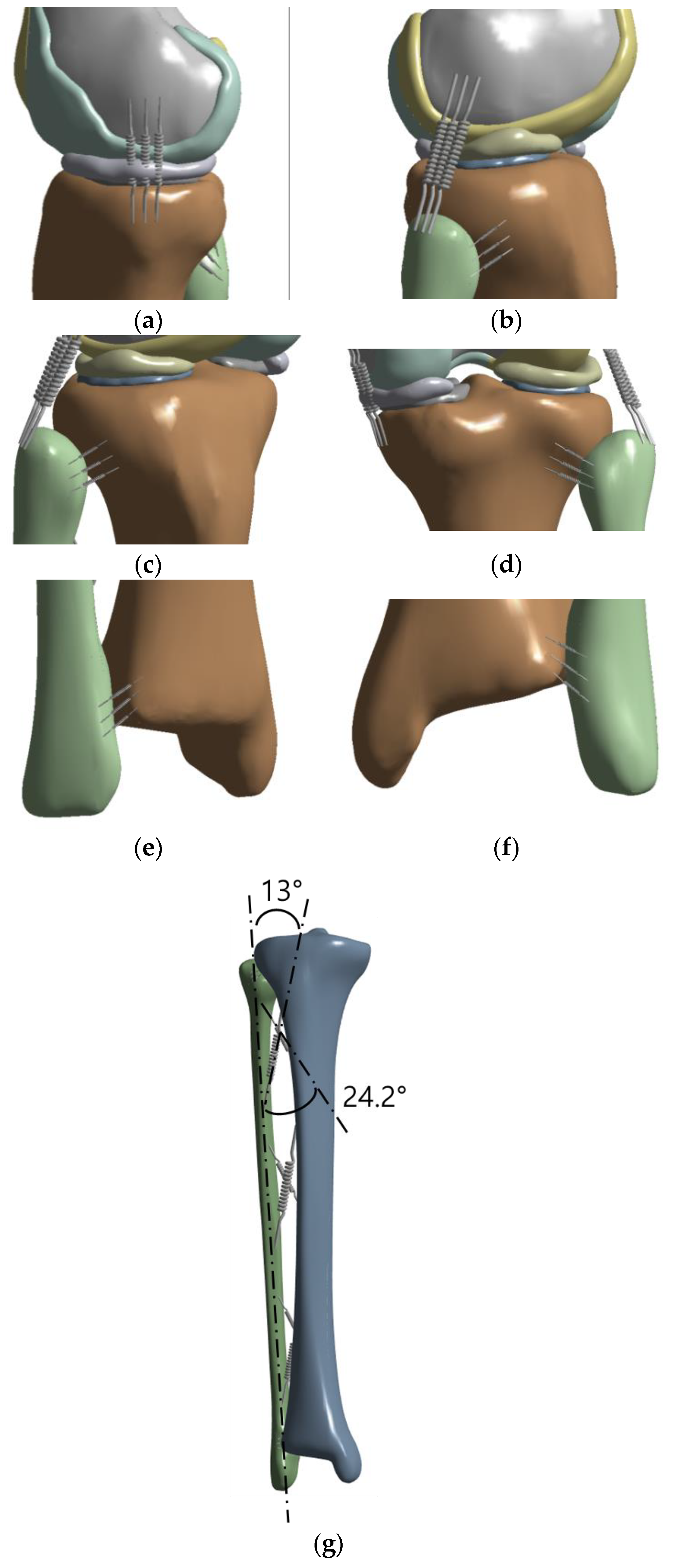
2.2. Establishment of Ligament
2.3. Material Properties
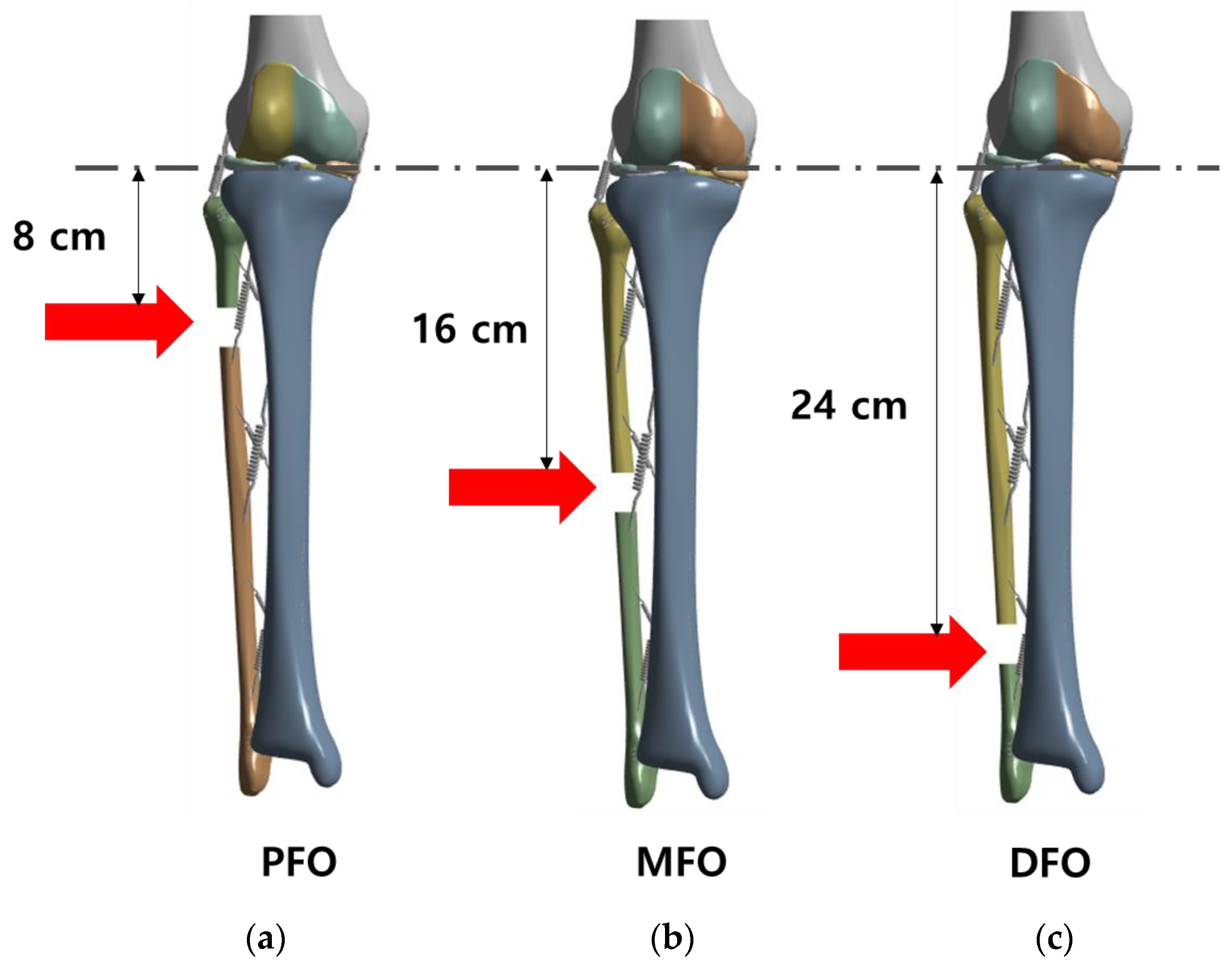
2.4. Load and Boundary Conditions
2.5. Validation of the Bone Model Using a Finite Element Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vandekerckhove, P.T.K.; Matlovich, N.; Teeter, M.G.; MacDonald, S.J.; Howard, J.L.; Lanting, B.A. The relationship between constitutional alignment and varus osteoarthritis of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2873–2879. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Bowles, K.A.; Wang, Y.; Cicuttini, F.; Davies-Tuck, M.; Hinman, R.S. Higher dynamic medial knee load predicts greater cartilage loss over 12 months in medial knee osteoarthritis. Ann. Rheum. Dis. 2011, 70, 1770–1774. [Google Scholar] [CrossRef]
- Miyazaki, T.; Wada, M.; Kawahara, H.; Sato, M.; Baba, H.; Shimada, S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann. Rheum. Dis. 2002, 61, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L.; Song, J.; Dunlop, D.; Felson, D.; Lewis, C.E.; Segal, N.; Torner, J.; Cooke, T.D.V.; Hietpas, J.; Lynch, J.; et al. Varus and valgus alignment and incident and progressive knee osteoarthritis. Ann. Rheum. Dis. 2010, 69, 1940–1945. [Google Scholar] [CrossRef] [PubMed]
- Sischek, E.L.; Birmingham, T.B.; Leitch, K.M.; Martin, R.; Willits, K.; Giffin, J.R. Staged medial opening wedge high tibial osteotomy for bilateral varus gonarthrosis: Biomechanical and clinical outcomes. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2672–2681. [Google Scholar] [CrossRef] [PubMed]
- Kettelkamp, D.B.; Wenger, D.R.; Chao, E.Y.; Thompson, C. Results of proximal tibial osteotomy. The effects of tibiofemoral angle, stance-phase flexion-extension, and medial-plateau force. J. Bone Jt. Surg. Am. 1976, 58, 952–960. [Google Scholar] [CrossRef]
- Majeed, A.S.; Thaha, N.; Varghese, B. High tibial osteotomy in medial compartment osteoarthritis of knee: Functional outcome of medial open wedge and lateral closing wedge osteotomies-How does the outliers fare in the medium term? Musculoskelet. Surg. 2023, 107, 313–322. [Google Scholar] [CrossRef]
- Yang, Z.Y.; Chen, W.; Li, C.X.; Wang, J.; Shao, D.C.; Hou, Z.Y.; Gao, S.J.; Wang, F.; Li, J.D.; Hao, J.D.; et al. Medial compartment decompression by fibular osteotomy to treat medial compartment knee osteoarthritis: A pilot study. Orthopedics 2015, 38, e1110–e1114. [Google Scholar] [CrossRef]
- Huda, N.; Islam, M.S.U.; Kumar, H.; Pant, A.; Bishnoi, S. Proximal fibular osteotomy for medial compartment knee osteoarthritis: Is it worth? Indian J. Orthop. 2020, 54, 47–51. [Google Scholar] [CrossRef]
- Utomo, D.N.; Mahyudin, F.; Wijaya, A.M.; Widhiyanto, L. Proximal fibula osteotomy as an alternative to TKA and HTO in late-stage varus type of knee osteoarthritis. J. Orthop. 2018, 15, 858–861. [Google Scholar] [CrossRef]
- Pan, D.; Tianye, L.; Peng, Y.; Jingli, X.; Hongzhu, L.; Heran, Z.; Qingwen, Z.; Leilei, C.; Zhenqiu, C.; Qiushi, W. Effects of proximal fibular osteotomy on stress changes in mild knee osteoarthritis with varus deformity: A finite element analysis. J. Orthop. Surg. Res. 2020, 15, 375. [Google Scholar] [CrossRef]
- Chen, Y.N.; Chang, C.W.; Li, C.T.; Chen, C.H.; Chung, C.R.; Chang, C.H.; Peng, Y.T. Biomechanical investigation of the type and configuration of screws used in high tibial osteotomy with titanium locking plate and screw fixation. J. Orthop. Surg. Res. 2019, 14, 35. [Google Scholar] [CrossRef]
- Chang, C.W.; Chen, Y.N.; Li, C.T.; Chung, Y.H.; Chang, C.H.; Peng, Y.T. Role of screw proximity in the fixation of transverse patellar fractures with screws and a wire. J. Orthop. Surg. 2018, 26, 2309499018789705. [Google Scholar] [CrossRef]
- Chu, A.; Weiner, L. Distal fibula malunions. J. Am. Acad. Orthop. Surg. 2009, 17, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Sugianto, J.A.; Hadipranata, T.; Lazarus, G.; Amrullah, A.H. Proximal fibular osteotomy for the management of medial compartment knee osteoarthritis: A systematic review and meta-analysis. Knee 2021, 28, 169–185. [Google Scholar] [CrossRef] [PubMed]
- Elamrani, D.; Aumar, A.; Wavreille, G.; Fontaine, C. Comparative morphometry of the antebrachial and crural interosseous membranes: Preliminary study for the use of the crural interosseous membrane in the surgical repair of the antebrachial interosseous membrane tears. Surg. Radiol. Anat. 2014, 36, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Chitsazan, A.; Rouhi, G.; Abbasi, M.; Pezeshki, S.; Tavakoli, A. Assessment of stress distribution in ankle joint: Simultaneous application of experimental and finite element methods. Int. J. Exp. Comput. Biomech. 2015, 3, 45–61. [Google Scholar] [CrossRef]
- Kim, S.H.; Chang, S.H.; Jung, H.J. The finite element analysis of a fractured tibia applied by composite bone plates considering contact conditions and time-varying properties of curing tissues. Compos. Struct. 2010, 92, 2109–2118. [Google Scholar] [CrossRef]
- Hopkins, A.R.; New, A.M.; Rodriguez-y-Baena, F.; Taylor, M. Finite element analysis of unicompartmental knee arthroplasty. Med. Eng. Phys. 2010, 32, 14–21. [Google Scholar] [CrossRef]
- Cho, H.J.; Kwak, D.S. Mechanical properties and characteristics of the anterolateral and collateral ligaments of the knee. Appl. Sci. 2020, 10, 6266. [Google Scholar] [CrossRef]
- Marchetti, D.C.; Moatshe, G.; Phelps, B.M.; Dahl, K.D.; Ferrari, M.B.; Chahla, J.; Turnbull, T.L.; LaPrade, R.F. The proximal tibiofibular joint: A biomechanical analysis of the anterior and posterior ligamentous complexes. Am. J. Sports Med. 2017, 45, 1888–1892. [Google Scholar] [CrossRef] [PubMed]
- Beumer, A.; van Hemert, W.L.; Swierstra, B.A.; Jasper, L.E.; Belkoff, S.M. A biomechanical evaluation of the tibiofibular and tibiotalar ligaments of the ankle. Foot Ankle Int. 2003, 24, 426–429. [Google Scholar] [CrossRef]
- Wang, X.; Wei, L.; Lv, Z.; Zhao, B.; Duan, Z.; Wu, W.; Zhang, B.; Wei, X. Proximal fibular osteotomy: A new surgery for pain relief and improvement of joint function in patients with knee osteoarthritis. J. Int. Med. Res. 2017, 45, 282–289. [Google Scholar] [CrossRef]
- Unal, O.K.; Dagtas, M.Z.; Demir, C.; Najafov, T.; Ugutmen, E. The effects of proximal fibular osteotomy on the knee and ankle joints: A finite element analysis. Acta Chir. Orthop. Traumatol. Cech. 2021, 88, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Han, P.; Jang, Y.W.; Yoo, O.S.; Kim, J.S.; Kim, H.S.; Lim, D. Evaluation of biomechanical stability of newly developed revision total knee arthroplasty through strain and stress distribution analysis within the tibia: Finite element analysis. J. Biomed. Eng. Res. 2013, 34, 14–23. [Google Scholar] [CrossRef]
- Nie, Y.; Ma, J.; Huang, Z.; Xu, B.; Tang, S.; Shen, B.; Kraus, V.B.; Pei, F. Upper partial fibulectomy improves knee biomechanics and function and decreases knee pain of osteoarthritis: A pilot and biomechanical study. J. Biomech. 2018, 71, 22–29. [Google Scholar] [CrossRef]
- Rupp, R.E.; Podeszwa, D.; Ebraheim, N.A. Danger zones associated with fibular osteotomy. J. Orthop. Trauma 1994, 8, 54–58. [Google Scholar] [CrossRef]
- Ye, Y.; You, W.; Zhu, W.; Cui, J.; Chen, K.; Wang, D. The applications of finite element analysis in proximal humeral fractures. Comput. Math. Methods Med. 2017, 2017, 4879836. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Number of Nodes | Number of Elements |
|---|---|---|
| Intact model | 668,372 | 444,677 |
| Proximal fibula osteotomy (PFO) model | 664,971 | 442,267 |
| Middle fibula osteotomy (MFO) model | 664,190 | 441,591 |
| Distal fibula osteotomy (DFO) model | 662,657 | 440,770 |
| Young’s Modulus (MPa) | Poisson’s Ratio | |||
|---|---|---|---|---|
| Cortical bone [16] | Ex = 6910 | Vxy = 0.49 | ||
| Ey = 8510 | Vxz = 0.12 | |||
| Ez = 18,400 | Vyz = 0.14 | |||
| Cancellous bone [17] | 1061 | 0.225 | ||
| Cartilage [18] | 12 | 0.45 | ||
| Meniscus [18] | 80 | 0.3 | ||
| MCL /LCL [19] | Proximal Anterior/Posterior Tibiofibula Ligament [20] | Distal Anterior/Posterior Tibiofibula Ligament [21] | Anterior/Posterior Interosseous Membrane [16,21,22] | |
| Stiffness (N/mm, per 1 spring) | 24/23.2 | 44.3/36.3 | 26/33.7 | 39/39 |
| Contact Body | Contact Type |
|---|---|
| Cortical-Cancellous bone (Femur, Tibia, Fibula) | Bonded |
| Femur Bone–Femoral Cartilage | Bonded |
| Tibia Bone–Tibial Cartilage | Bonded |
| Meniscus–Tibial Cartilage | Bonded |
| Femoral Cartilage–Meniscus | Frictional, μ = 0.2 |
| Femoral Cartilage–Tibial Cartilage | Frictional, μ = 0.2 |
| Tibia bone–Fibula Bone | No separation, μ = 0 |
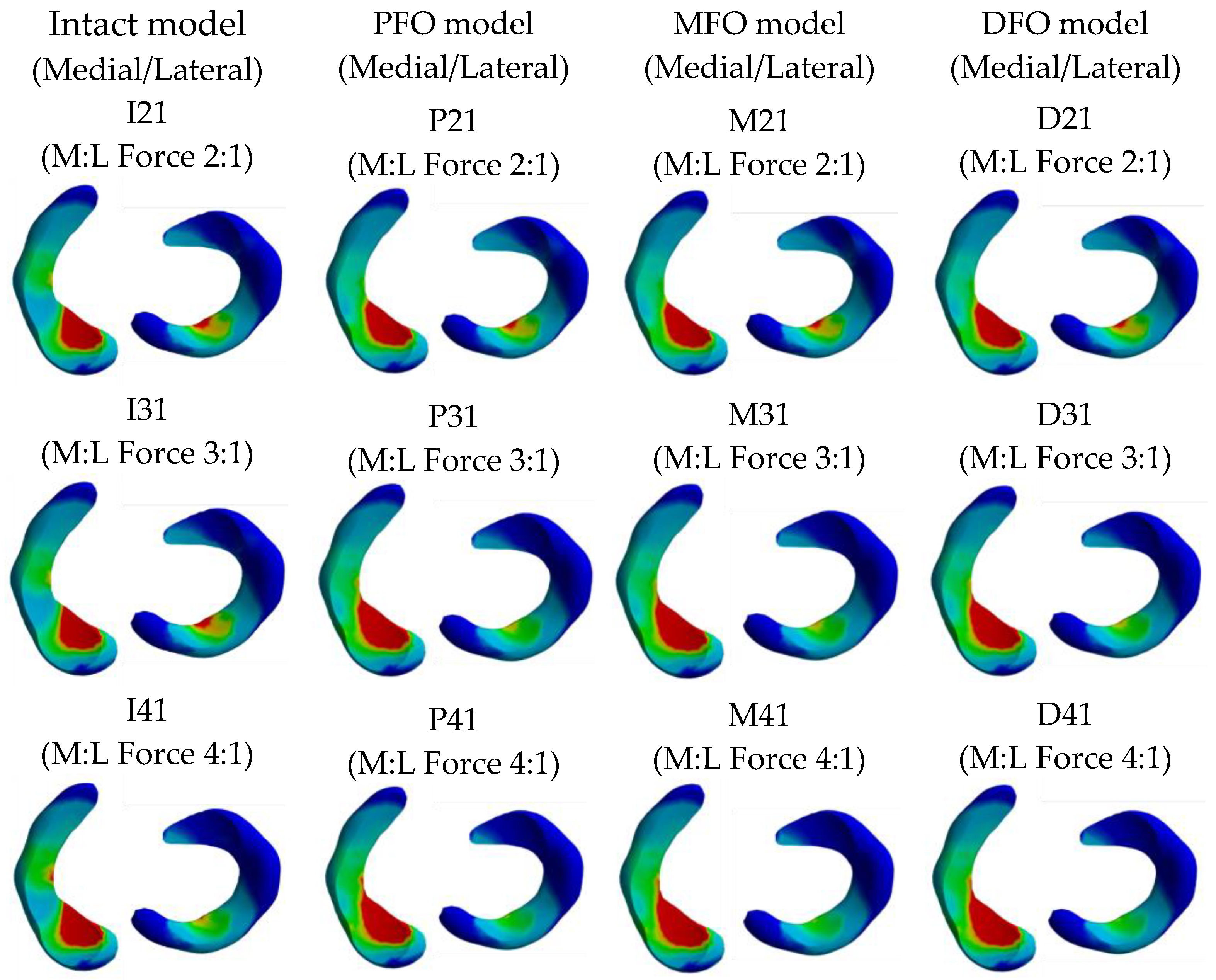
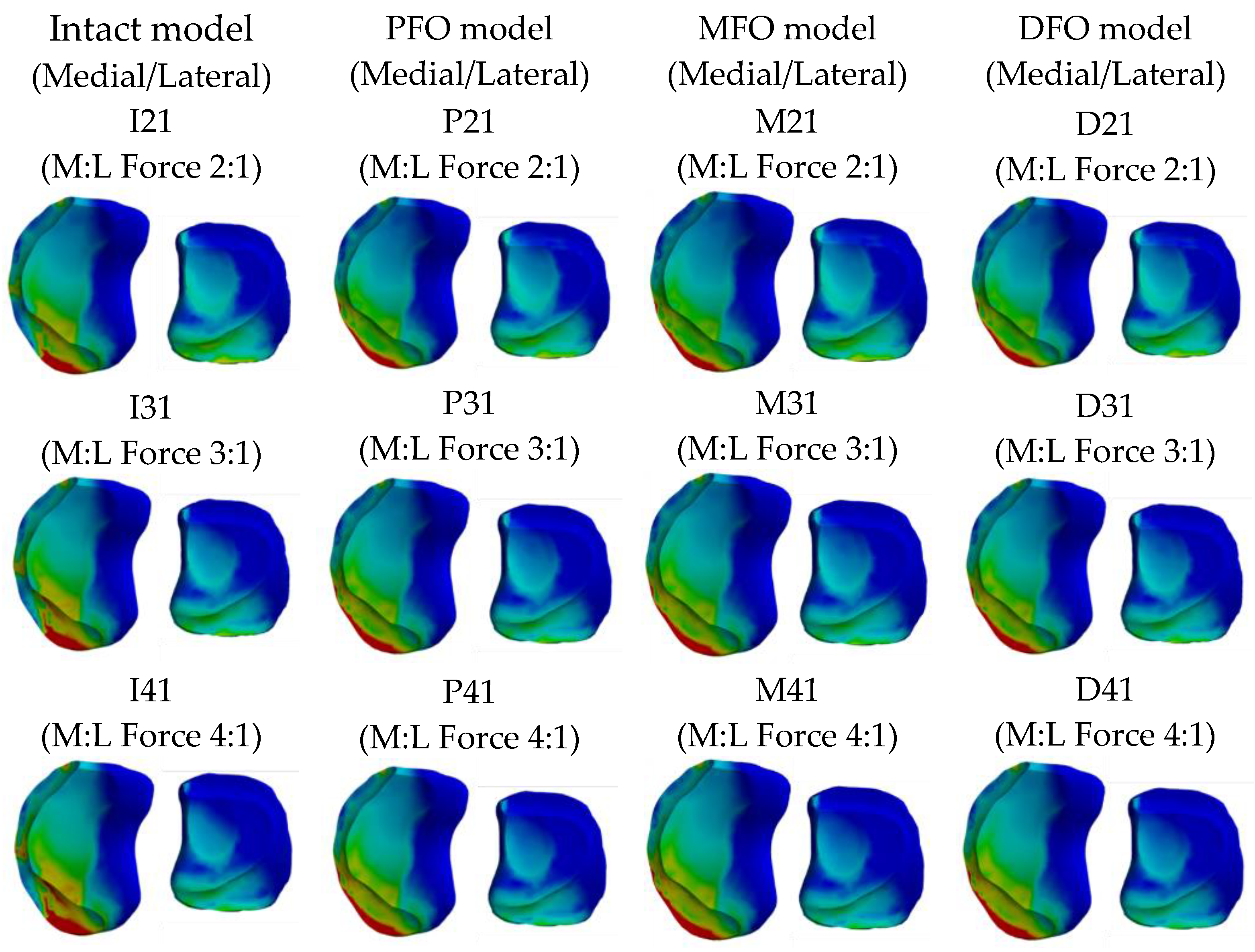
| Bone Model | Intact Model | PFO Model | MFO Model | DFO Model | |
|---|---|---|---|---|---|
| Force Ratio | |||||
| M:L = 2:1 | I21 | P21 | M21 | D21 | |
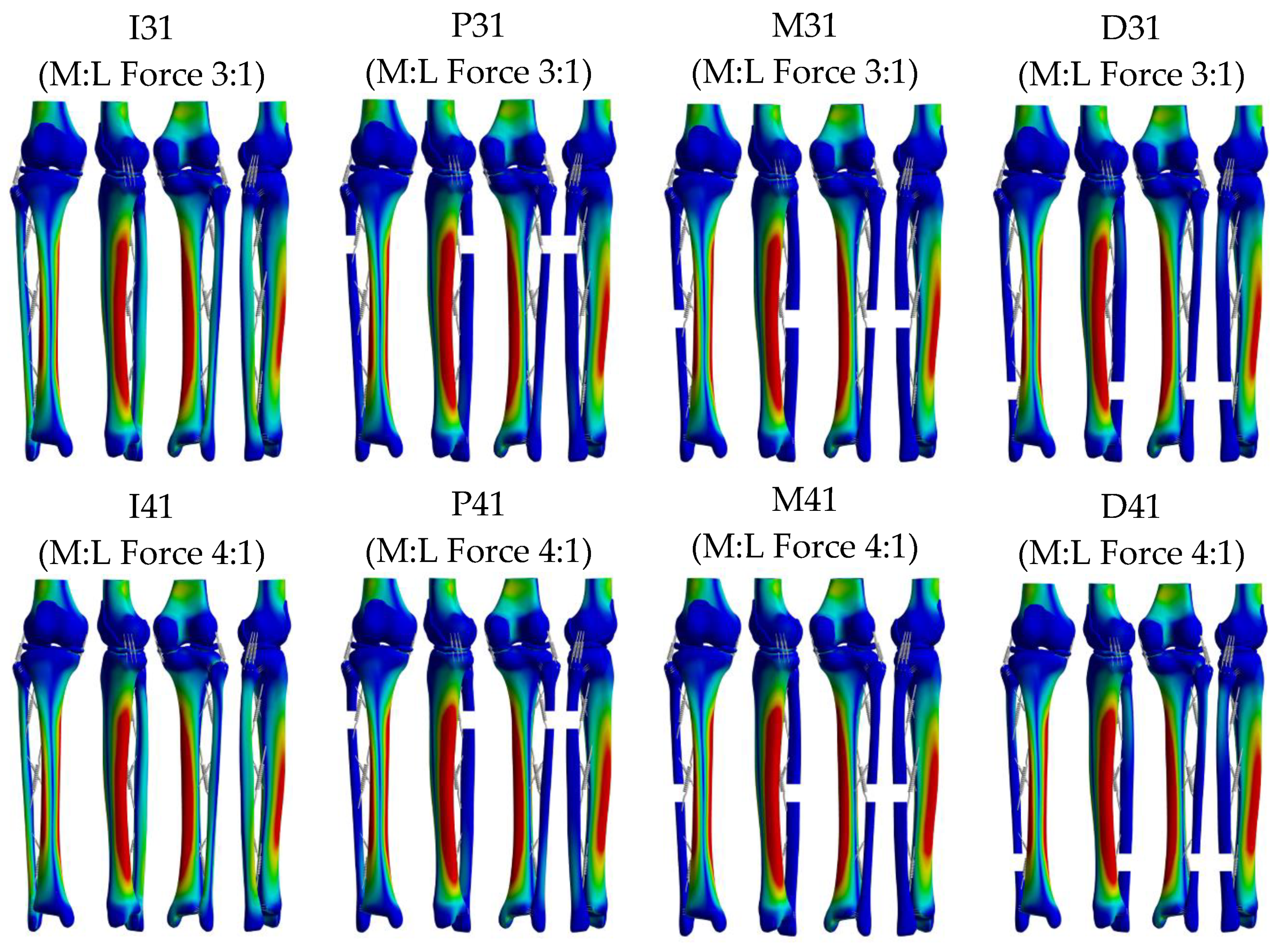
| M:L = 3:1 | I31 | P31 | M31 | D31 | |
| M:L = 4:1 | I41 | P41 | M41 | D41 | |
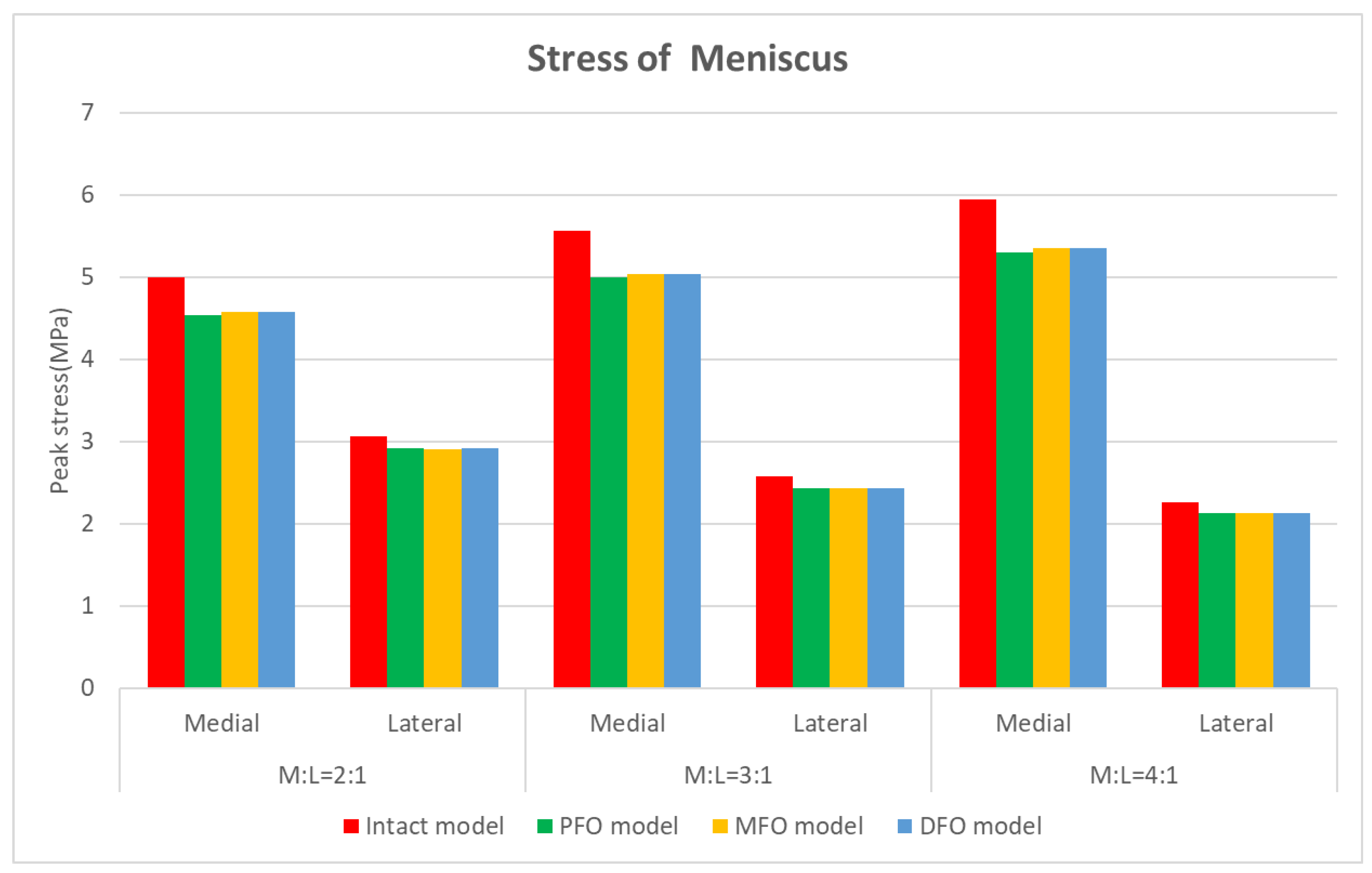
| Peak von Mises Stress [MPa] | ||||||
|---|---|---|---|---|---|---|
| Model | M:L = 2:1 | M:L = 3:1 | M:L = 4:1 | |||
| Medial (vs. Intact) | Lateral (vs. Intact) | Medial (vs. Intact) | Lateral (vs. Intact) | Medial (vs. Intact) | Lateral (vs. Intact) | |
| Intact model | 5.000 | 3.058 | 5.562 | 2.574 | 5.941 | 2.257 |
| PFO model | 4.537 (−9.3%) | 2.915 (−4.7%) | 4.995 (−10.2%) | 2.435 (−5.4%) | 5.301 (−10.8%) | 2.126 (−5.8%) |
| MFO model | 4.579 (−8.4%) | 2.905 (−5.0%) | 5.039 (−9.4%) | 2.429 (−5.6%) | 5.345 (−10.0%) | 2.123 (−5.9%) |
| DFO model | 4.579 (−8.4%) | 2.911 (−4.8%) | 5.040 (−9.4%) | 2.433 (−5.5%) | 5.346 (−10.0%) | 2.125 (−5.9%) |
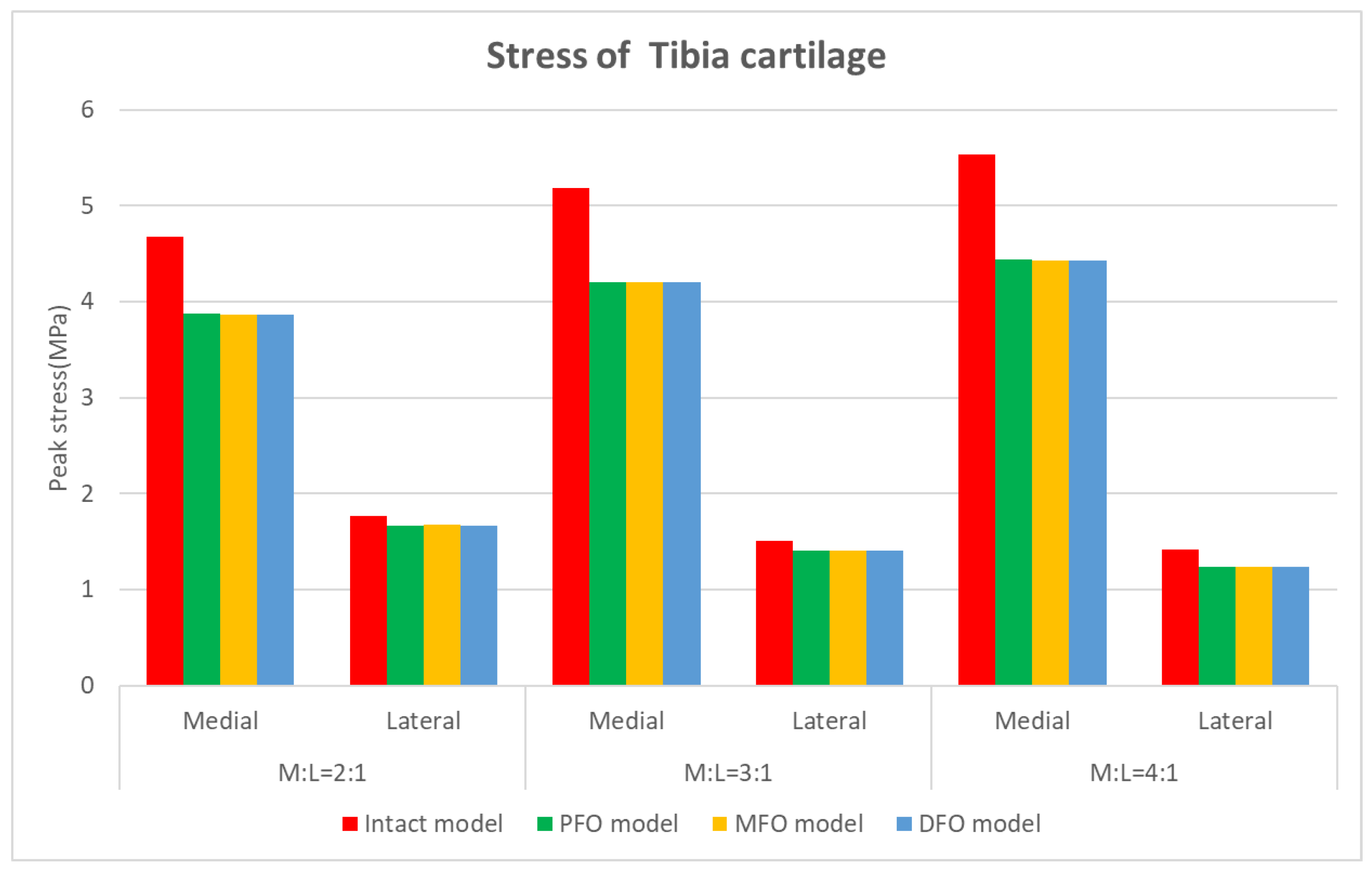
| Peak von Mises Stress [MPa] | ||||||
|---|---|---|---|---|---|---|
| Model | M:L = 2:1 | M:L = 3:1 | M:L = 4:1 | |||
| Medial (vs. Intact) | Lateral (vs. Intact) | Medial (vs. Intact) | Lateral (vs. Intact) | Medial (vs. Intact) | Lateral (vs. Intact) | |
| Intact model | 4.681 | 1.772 | 5.182 | 1.503 | 5.533 | 1.419 |
| PFO model | 3.871 (−17.3%) | 1.671 (−5.7%) | 4.207 (−18.8%) | 1.405 (−6.5%) | 4.438 (−19.8%) | 1.240 (−12.6%) |
| MFO model | 3.867 (−17.4%) | 1.673 (−5.6%) | 4.202 (−18.9%) | 1.407 (−6.4%) | 4.433 (−19.9%) | 1.241 (−12.6%) |
| DFO model | 3.867 (−17.4%) | 1.668 (−5.8%) | 4.202 (−18.9%) | 1.404 (−6.6%) | 4.433 (−19.9%) | 1.240 (−12.6%) |
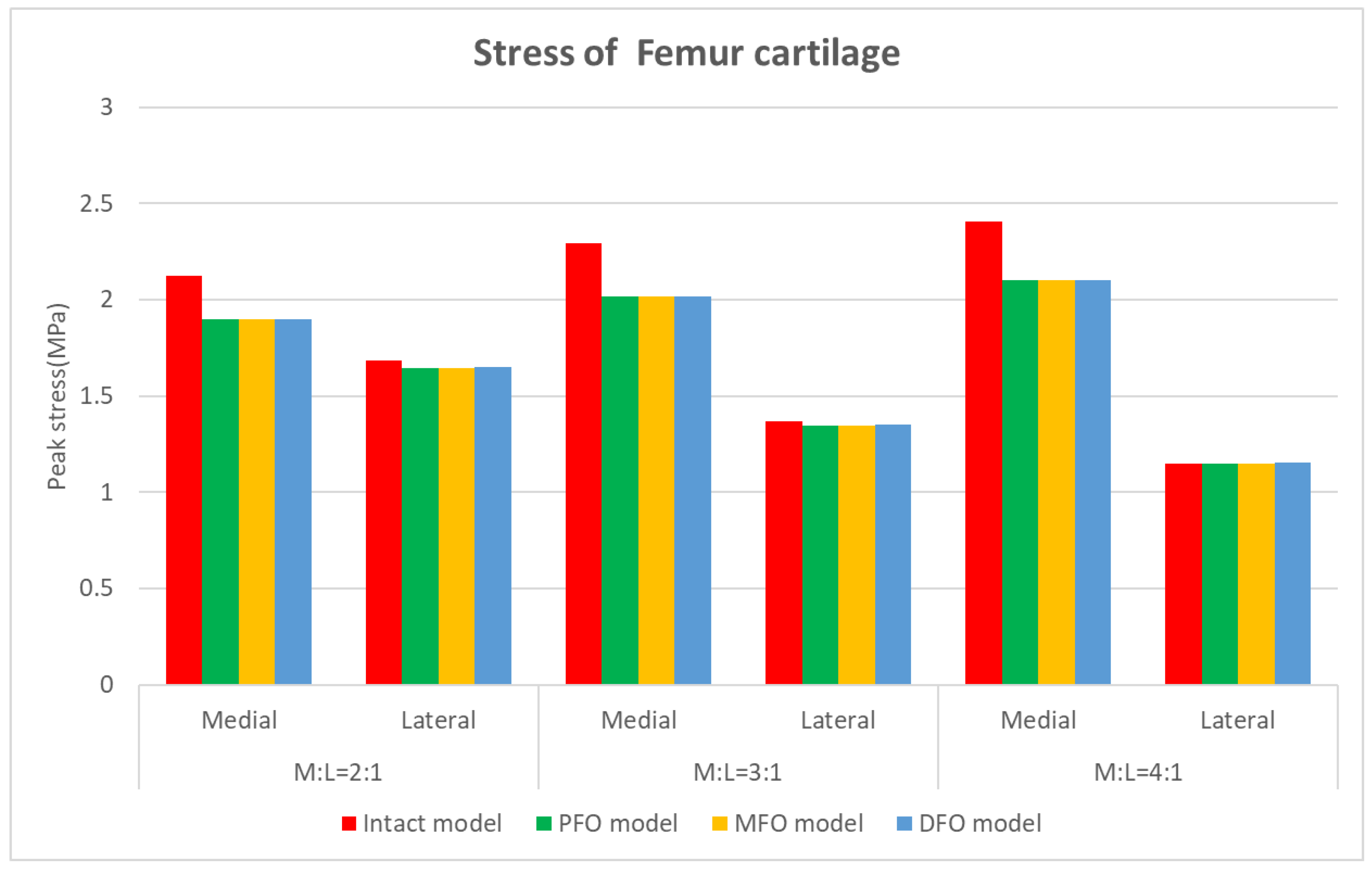
| Peak von Mises Stress [MPa] | ||||||
|---|---|---|---|---|---|---|
| Model | M:L = 2:1 | M:L = 3:1 | M:L = 4:1 | |||
| Medial (vs. Intact) | Lateral (vs. Intact) | Medial (vs. Intact) | Lateral (vs. Intact) | Medial (vs. Intact) | Lateral (vs. Intact) | |
| Intact model | 2.124 | 1.684 | 2.292 | 1.366 | 2.408 | 1.146 |
| PFO model | 1.897 (−10.7%) | 1.645 (−2.3%) | 2.019 (−11.9%) | 1.345 (−1.5%) | 2.099 (−12.8%) | 1.146 (0.0%) |
| MFO model | 1.897 (−10.7%) | 1.645 (−2.3%) | 2.019 (−11.9%) | 1.346 (−1.5%) | 2.099 (−12.8%) | 1.147 (0.1%) |
| DFO model | 1.897 (−10.7%) | 1.652 (−1.9%) | 2.019 (−11.9%) | 1.352 (−1.0%) | 2.099 (−12.8%) | 1.152 (0.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, Y.; Kim, J.; Sim, J.A.; Moon, M.; Park, J.-C.; Cho, S.H.; Lee, B.H. Stress Effect in the Knee Joint Based on the Fibular Osteotomy Level and Varus Deformity: A Finite Element Analysis Study. Bioengineering 2023, 10, 1003. https://doi.org/10.3390/bioengineering10091003
Kang Y, Kim J, Sim JA, Moon M, Park J-C, Cho SH, Lee BH. Stress Effect in the Knee Joint Based on the Fibular Osteotomy Level and Varus Deformity: A Finite Element Analysis Study. Bioengineering. 2023; 10(9):1003. https://doi.org/10.3390/bioengineering10091003
Chicago/Turabian StyleKang, Yeokyung, Jungsung Kim, Jae Ang Sim, Myeong Moon, Jong-Chul Park, Sung Ha Cho, and Byung Hoon Lee. 2023. "Stress Effect in the Knee Joint Based on the Fibular Osteotomy Level and Varus Deformity: A Finite Element Analysis Study" Bioengineering 10, no. 9: 1003. https://doi.org/10.3390/bioengineering10091003
APA StyleKang, Y., Kim, J., Sim, J. A., Moon, M., Park, J.-C., Cho, S. H., & Lee, B. H. (2023). Stress Effect in the Knee Joint Based on the Fibular Osteotomy Level and Varus Deformity: A Finite Element Analysis Study. Bioengineering, 10(9), 1003. https://doi.org/10.3390/bioengineering10091003