
Development of a Machine Learning Model of Postoperative Acute Kidney Injury Using Non-Invasive Time-Sensitive Intraoperative Predictors
 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
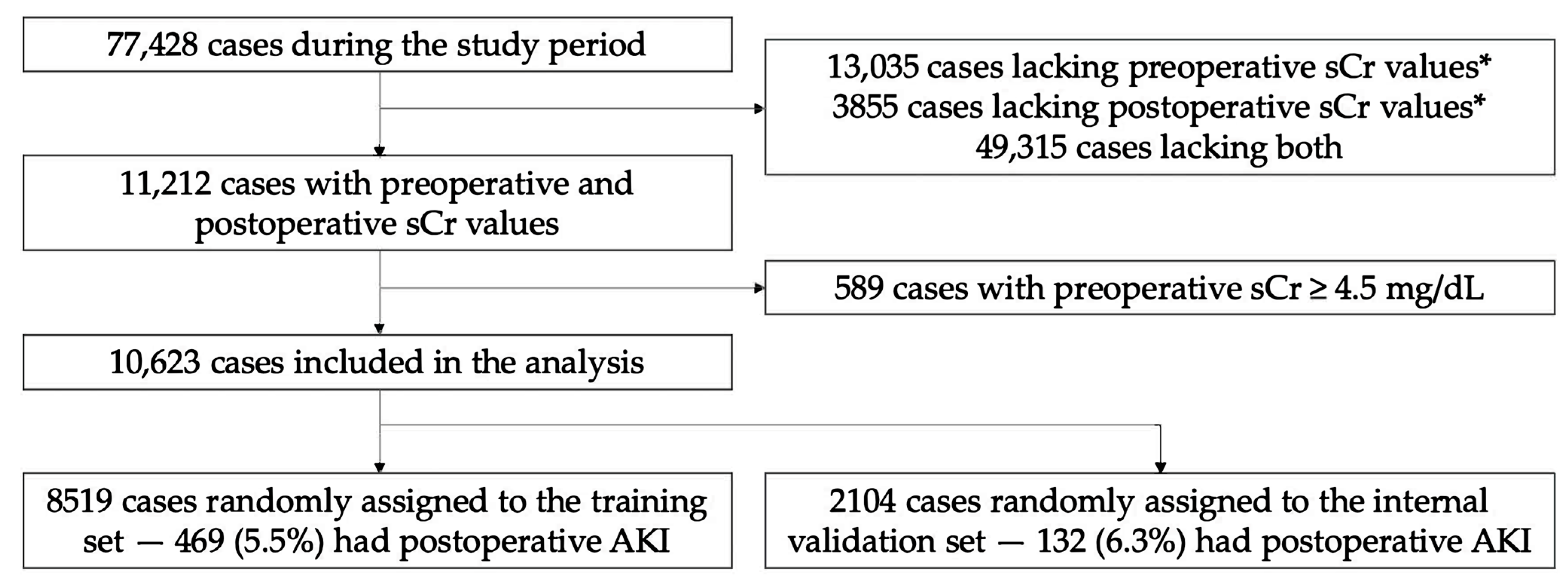
3.1. Patient Characteristics
3.2. Preoperative and Intraoperative Variables
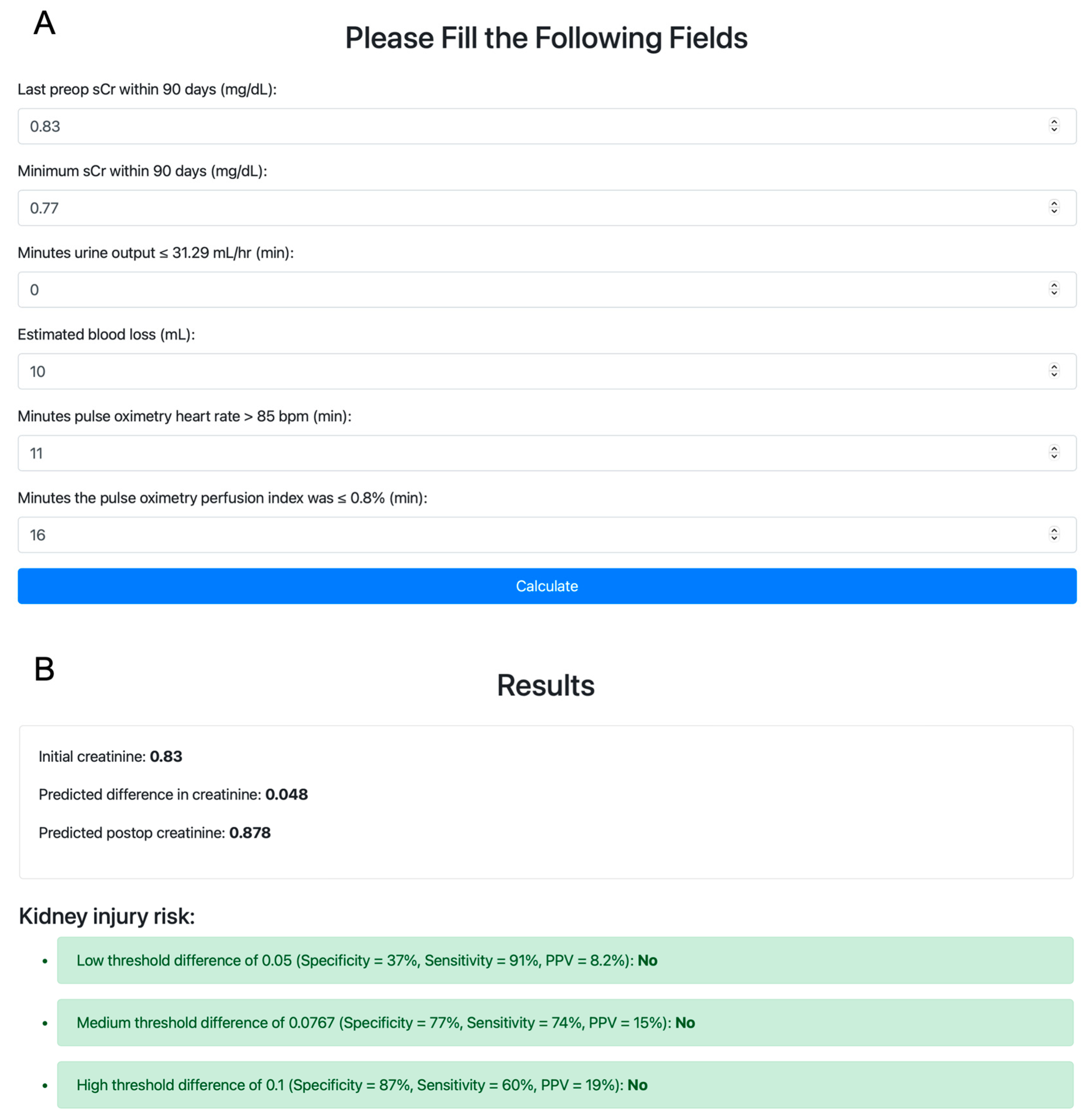
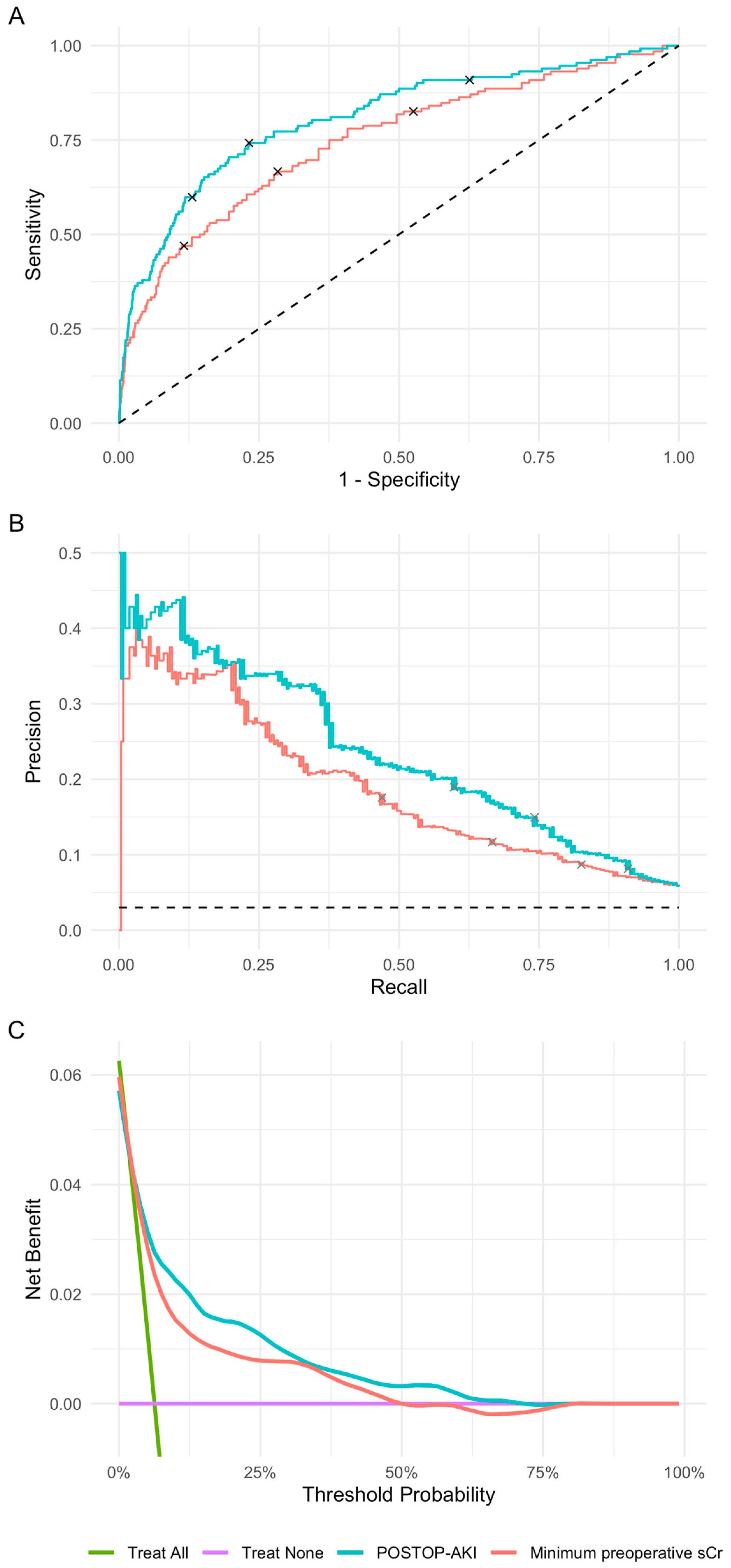
3.3. Predictive Performance of the POSTOP-AKI Model
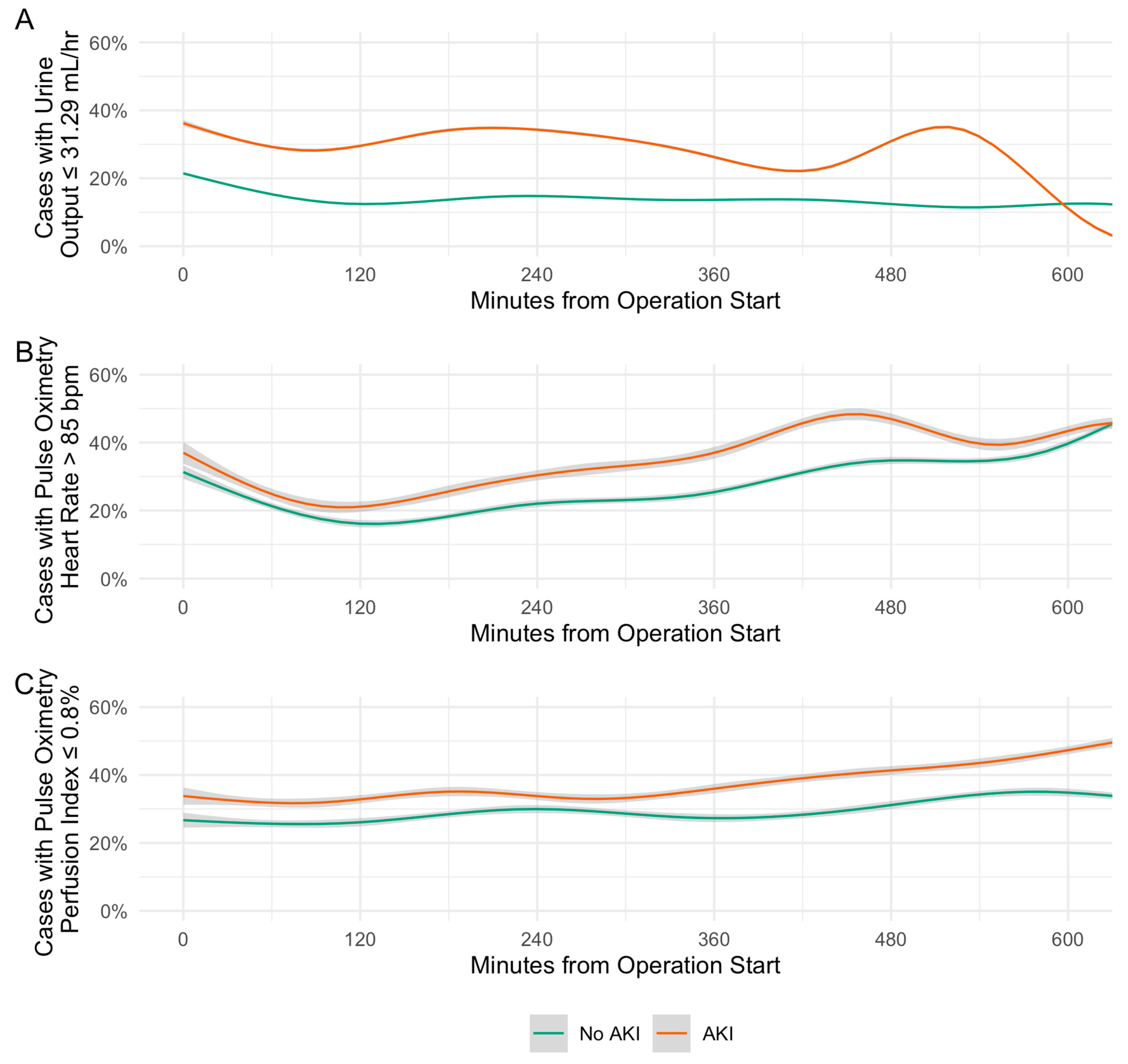
3.4. Associations of Model Variables with Postoperative AKI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hobson, C.; Ozrazgat-Baslanti, T.; Kuxhausen, A.; Thottakkara, P.; Efron, P.A.; Moore, F.A.; Moldawer, L.L.; Segal, M.S.; Bihorac, A. Cost and Mortality Associated with Postoperative Acute Kidney Injury. Ann. Surg. 2015, 261, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Bellomo, R. Cardiac Surgery-Associated Acute Kidney Injury: Risk Factors, Pathophysiology and Treatment. Nat. Rev. Nephrol. 2017, 13, 697–711. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, S.; Ricci, Z.; Ronco, C. Perioperative Acute Kidney Injury: Prevention, Early Recognition, and Supportive Measures. Nephron 2018, 140, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Sahinturk, H.; Ozdemirkan, A.; Zeyneloglu, P.; Gedik, E.; Pirat, A.; Haberal, M. Early Postoperative Acute Kidney Injury Among Pediatric Liver Transplant Recipients. Exp. Clin. Transplant. 2021, 19, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Massoth, C.; Zarbock, A.; Meersch, M. Acute Kidney Injury in Cardiac Surgery. Crit. Care Clin. 2021, 37, 267–278. [Google Scholar] [CrossRef]
- Chang, C.-Y.; Chien, Y.-J.; Kao, M.-C.; Lin, H.-Y.; Chen, Y.-L.; Wu, M.-Y. Pre-Operative Proteinuria, Postoperative Acute Kidney Injury and Mortality: A Systematic Review and Meta-Analysis. Eur. J. Anaesthesiol. 2021, 38, 702–714. [Google Scholar] [CrossRef]
- Bennett, D.; Fossi, A.; Marchetti, L.; Lanzarone, N.; Sisi, S.; Refini, R.M.; Sestini, P.; Luzzi, L.; Paladini, P.; Rottoli, P. Postoperative Acute Kidney Injury in Lung Transplant Recipients. Interact. CardioVasc. Thorac. Surg. 2019, 28, 929–935. [Google Scholar] [CrossRef]
- Helgason, D.; Helgadottir, S.; Ahlsson, A.; Gunn, J.; Hjortdal, V.; Hansson, E.C.; Jeppsson, A.; Mennander, A.; Nozohoor, S.; Zindovic, I.; et al. Acute Kidney Injury After Acute Repair of Type A Aortic Dissection. Ann. Thorac. Surg. 2021, 111, 1292–1298. [Google Scholar] [CrossRef]
- Oh, T.K.; Song, I.-A. Postoperative Acute Kidney Injury Requiring Continuous Renal Replacement Therapy and Outcomes after Coronary Artery Bypass Grafting: A Nationwide Cohort Study. J. Cardiothorac. Surg. 2021, 16, 315. [Google Scholar] [CrossRef]
- Engin, M.; Aydın, U.; Tatlı, A.B.; As, A.K.; Ata, Y. Heart Surgery and Postoperative Acute Kidney Injury. J. Card. Surg. 2022, 37, 2487–2488. [Google Scholar] [CrossRef]
- McIlroy, D.R.; Wagener, G.; Lee, H.T.; Riou, B. Biomarkers of Acute Kidney Injury. Anesthesiology 2010, 112, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Lei, V.J.; Luong, T.; Shan, E.; Chen, X.; Neuman, M.D.; Eneanya, N.D.; Polsky, D.E.; Volpp, K.G.; Fleisher, L.A.; Holmes, J.H.; et al. Risk Stratification for Postoperative Acute Kidney Injury in Major Noncardiac Surgery Using Preoperative and Intraoperative Data. JAMA Netw. Open 2019, 2, e1916921. [Google Scholar] [CrossRef] [PubMed]
- Mathis, M.R.; Naik, B.I.; Freundlich, R.E.; Shanks, A.M.; Heung, M.; Kim, M.; Burns, M.L.; Colquhoun, D.A.; Rangrass, G.; Janda, A.; et al. Preoperative Risk and the Association between Hypotension and Postoperative Acute Kidney Injury. Anesthesiology 2020, 132, 461–475. [Google Scholar] [CrossRef]
- Garg, A.X.; Kurz, A.; Sessler, D.I.; Cuerden, M.; Robinson, A.; Mrkobrada, M.; Parikh, C.R.; Mizera, R.; Jones, P.M.; Tiboni, M.; et al. Perioperative Aspirin and Clonidine and Risk of Acute Kidney Injury: A Randomized Clinical Trial. JAMA 2014, 312, 2254. [Google Scholar] [CrossRef]
- Bonventre, J.V.; Yang, L. Cellular Pathophysiology of Ischemic Acute Kidney Injury. J. Clin. Investig. 2011, 121, 4210–4221. [Google Scholar] [CrossRef] [PubMed]
- Sharfuddin, A.A.; Molitoris, B.A. Pathophysiology of Ischemic Acute Kidney Injury. Nat. Rev. Nephrol. 2011, 7, 189–200. [Google Scholar] [CrossRef]
- Park, S.; Lee, H.-C.; Jung, C.-W.; Choi, Y.; Yoon, H.J.; Kim, S.; Chin, H.J.; Kim, M.; Kim, Y.C.; Kim, D.K.; et al. Intraoperative Arterial Pressure Variability and Postoperative Acute Kidney Injury. CJASN 2020, 15, 35–46. [Google Scholar] [CrossRef]
- Silverton, N.A.; Lofgren, L.R.; Hall, I.E.; Stoddard, G.J.; Melendez, N.P.; Van Tienderen, M.; Shumway, S.; Stringer, B.J.; Kang, W.; Lybbert, C.; et al. Noninvasive Urine Oxygen Monitoring and the Risk of Acute Kidney Injury in Cardiac Surgery. Anesthesiology 2021, 135, 406–418. [Google Scholar] [CrossRef]
- Roman, M.J.; Devereux, R.B. Association of Central and Peripheral Blood Pressures with Intermediate Cardiovascular Phenotypes. Hypertension 2014, 63, 1148–1153. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. Br. J. Surg. 2015, 102, 148–158. [Google Scholar] [CrossRef]
- Whitlock, E.L.; Braehler, M.R.; Kaplan, J.A.; Finlayson, E.; Rogers, S.E.; Douglas, V.; Donovan, A.L. Derivation, Validation, Sustained Performance, and Clinical Impact of an Electronic Medical Record–Based Perioperative Delirium Risk Stratification Tool. Anesth. Analg. 2020, 131, 1901–1910. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Bishara, A.; Wong, A.; Wang, L.; Chopra, M.; Fan, W.; Lin, A.; Fong, N.; Palacharla, A.; Spinner, J.; Armstrong, R.; et al. Opal: An Implementation Science Tool for Machine Learning Clinical Decision Support in Anesthesia. J Clin Monit Comput 2022, 36, 1367–1377. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Ooi, H. GlmnetUtils: Utilities for “Glmnet” 2021. R Package Version 1.1.8. Available online: https://cran.r-project.org/package=glmnetUtils (accessed on 30 July 2023).
- Lim, M.; Hastie, T. Learning Interactions via Hierarchical Group-Lasso Regularization. J. Comput. Graph. Stat. 2015, 24, 627–654. [Google Scholar] [CrossRef] [PubMed]
- Sjoberg, D.D. Dcurves: Decision Curve Analysis for Model Evaluation 2022. R Package Version 0.4.0. Available online: https://CRAN.R-project.org/package=dcurves (accessed on 30 July 2023).
- Kuhn, M. Building Predictive Models in R Using the Caret Package. J. Stat. Soft. 2008, 28, 1–26. [Google Scholar] [CrossRef]
- Wright, M.N.; Ziegler, A. Ranger: A Fast Implementation of Random Forests for High Dimensional Data in C++ and R. J. Stat. Soft. 2017, 77, 1–17. [Google Scholar] [CrossRef]
- Chen, T.; He, T. Xgboost: EXtreme Gradient Boosting 2022. R Package Version 1.6.0.1. Available online: https://CRAN.R-project.org/package=xgboost (accessed on 30 July 2023).
- Canty, A.J. Resampling Methods in R: The Boot Package. R News 2002, 2, 2–7. [Google Scholar]
- Meersch, M.; Schmidt, C.; Hoffmeier, A.; Van Aken, H.; Wempe, C.; Gerss, J.; Zarbock, A. Prevention of Cardiac Surgery-Associated AKI by Implementing the KDIGO Guidelines in High Risk Patients Identified by Biomarkers: The PrevAKI Randomized Controlled Trial. Intensive Care Med. 2017, 43, 1551–1561. [Google Scholar] [CrossRef]
- Jones, P.M.; Cherry, R.A.; Allen, B.N.; Jenkyn, K.M.B.; Shariff, S.Z.; Flier, S.; Vogt, K.N.; Wijeysundera, D.N. Association Between Handover of Anesthesia Care and Adverse Postoperative Outcomes Among Patients Undergoing Major Surgery. JAMA 2018, 319, 143. [Google Scholar] [CrossRef]
- Pinto Lima, A.; Beelen, P.; Bakker, J. Use of a Peripheral Perfusion Index Derived from the Pulse Oximetry Signal as a Noninvasive Indicator of Perfusion. Crit. Care Med. 2002, 30, 1210–1213. [Google Scholar] [CrossRef] [PubMed]
- Zaramella, P.; Freato, F.; Quaresima, V.; Ferrari, M.; Vianello, A.; Giongo, D.; Conte, L.; Chiandetti, L. Foot Pulse Oximeter Perfusion Index Correlates with Calf Muscle Perfusion Measured by Near-Infrared Spectroscopy in Healthy Neonates. J. Perinatol. 2005, 25, 417–422. [Google Scholar] [CrossRef]
- Goren, O.; Matot, I. Perioperative Acute Kidney Injury. Br. J. Anaesth. 2015, 115 (Suppl. S2), ii3–ii14. [Google Scholar] [CrossRef] [PubMed]
- Josephs, S.A.; Thakar, C.V. Perioperative Risk Assessment, Prevention, and Treatment of Acute Kidney Injury. Int. Anesth. Clin. 2009, 47, 89–105. [Google Scholar] [CrossRef]
- Nussmeier, N.; Hauser, M.; Sarwar, M.; Grigore, A.; Searles, B. Anesthesia for Cardiac Surgical Procedures. In Miller’s Anesthesia; Miller, R., Ed.; Elsevier Livingstone Churchill: Philadelphia, PA, USA, 2009. [Google Scholar]
- Park, S.; Cho, H.; Park, S.; Lee, S.; Kim, K.; Yoon, H.J.; Park, J.; Choi, Y.; Lee, S.; Kim, J.H.; et al. Simple Postoperative AKI Risk (SPARK) Classification before Noncardiac Surgery: A Prediction Index Development Study with External Validation. JASN 2019, 30, 170–181. [Google Scholar] [CrossRef]
- Sjoding, M.W.; Dickson, R.P.; Iwashyna, T.J.; Gay, S.E.; Valley, T.S. Racial Bias in Pulse Oximetry Measurement. N. Engl. J. Med. 2020, 383, 2477–2478. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall | Training Set | Validation Set | SMD |
|---|---|---|---|---|
| N | 10,623 | 8519 | 2104 | |
| Age (median [IQR]) | 62 (51, 72) | 62 (51, 72) | 62 (50, 71) | 0.02 |
| Male (%) | 5871 (55.3) | 4747 (55.7) | 1124 (53.4) | 0.05 |
| Race (%) | 0.02 | |||
| American Indian or Alaska Native | 89 (0.8) | 74 (0.9) | 15 (0.7) | |
| Black or African American | 916 (8.6) | 732 (8.6) | 184 (8.7) | |
| Other, including multiracial | 3217 (30.3) | 2573 (30.2) | 644 (30.6) | |
| White or Caucasian | 6401 (60.3) | 5140 (60.3) | 1261 (59.9) | |
| Hispanic or Latino (%) | 1558 (14.7) | 1246 (14.6) | 312 (14.8) | 0.006 |
| Weight—kg (median [IQR]) | 77 (64, 91) | 77 (64, 91) | 77 (64, 91) | 0.01 |
| Height—cm (median [IQR]) | 170 (163, 178) | 170 (163, 178) | 168 (163, 178) | 0.08 |
| Body mass index—kg/m2 (median [IQR]) | 26 (22, 30) | 26 (22, 30) | 26 (22, 30) | 0.03 |
| Diabetes mellitus (%) | 257 (2.4) | 208 (2.4) | 49 (2.3) | 0.007 |
| Hypertension (%) | 296 (2.8) | 247 (2.9) | 49 (2.3) | 0.04 |
| Heart failure (%) | 119 (1.1) | 95 (1.1) | 24 (1.1) | 0.002 |
| Liver disease (%) | 401 (3.8) | 327 (3.8) | 74 (3.5) | 0.02 |
| Surgical risk score (%) | 0.02 | |||
| 0 | 6554 (61.7) | 5238 (61.5) | 1316 (62.5) | |
| 1 | 2571 (24.2) | 2070 (24.3) | 501 (23.8) | |
| 2 | 1498 (14.1) | 1211 (14.2) | 287 (13.6) | |
| American Society of Anesthesiologists (ASA) class (%) | 0.05 | |||
| 1 | 216 (2.0) | 163 (1.9) | 53 (2.5) | |
| 2 | 5853 (55.1) | 4685 (55.0) | 1168 (55.5) | |
| 3 | 3957 (37.2) | 3184 (37.4) | 773 (36.7) | |
| 4 | 591 (5.6) | 483 (5.7) | 108 (5.1) | |
| 5 | 6 (0.1) | 4 (0.0) | 2 (0.1) | |
| ASA emergency (%) | 2675 (25.2) | 2138 (25.1) | 537 (25.5) | 0.01 |
| Primary service (%) | 0.07 | |||
| Cardiac surgery | 188 (1.8) | 151 (1.8) | 37 (1.8) | |
| Cardiology | 826 (7.8) | 680 (8.0) | 146 (6.9) | |
| Gastroenterology | 108 (1.0) | 90 (1.1) | 18 (0.9) | |
| General surgery | 1611 (15.2) | 1277 (15.0) | 334 (15.9) | |
| Neurological surgery | 1350 (12.7) | 1099 (12.9) | 251 (11.9) | |
| Orthopedic surgery | 3778 (35.6) | 3003 (35.3) | 775 (36.8) | |
| Other | 1012 (9.5) | 823 (9.7) | 189 (9.0) | |
| Plastic surgery | 324 (3.0) | 257 (3.0) | 67 (3.2) | |
| Thoracic surgery | 240 (2.3) | 193 (2.3) | 47 (2.2) | |
| Vascular surgery | 1186 (11.2) | 946 (11.1) | 240 (11.4) | |
| Booking case length—min (median [IQR]) | 210 (133, 242) | 210 (134, 242) | 210 (130, 241) | 0.02 |
| Actual case duration—min (median [IQR]) | 160 (93, 257) | 161 (94, 257) | 159 (90, 258.25) | 0.003 |
| Intraoperative | ||||
| Use of inhalational anesthetic (%) | 9827 (92.5) | 7878 (92.5) | 1949 (92.6) | 0.006 |
| Use of pressors (%) | 6468 (60.9) | 5188 (60.9) | 1280 (60.8) | 0.001 |
| Median temperature (median [IQR]) | 97 (96, 98) | 97 (96, 98) | 97 (97, 98) | 0.04 |
| Median heart rate (median [IQR]) | 72 (63, 83) | 72 (63, 83) | 72 (63, 82) | 0.02 |
| Median systolic blood pressure (median [IQR]) | 112 (103, 124) | 112 (103, 124) | 112 (103, 125) | 0.01 |
| Median respiratory rate (median [IQR]) | 12 (10, 14) | 12 (10, 14) | 12 (10, 14) | 0.008 |
| Minimum Preoperative sCr | POSTOP-AKI | |||
|---|---|---|---|---|
| Score threshold | <0.75 | ≥0.75 | <0.05 | ≥0.05 |
| No AKI | 935 | 1037 | 737 | 1235 |
| AKI | 23 | 109 | 12 | 120 |
| Score threshold | <0.945 | ≥0.945 | <0.0767 | ≥0.0767 |
| No AKI | 1413 | 559 | 1514 | 458 |
| AKI | 44 | 88 | 34 | 98 |
| Score threshold | <1.25 | ≥1.25 | <0.1 | ≥0.1 |
| No AKI | 1743 | 229 | 1714 | 258 |
| AKI | 70 | 62 | 53 | 79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamirpour, S.; Hubbard, A.E.; Feng, J.; Butte, A.J.; Pirracchio, R.; Bishara, A. Development of a Machine Learning Model of Postoperative Acute Kidney Injury Using Non-Invasive Time-Sensitive Intraoperative Predictors. Bioengineering 2023, 10, 932. https://doi.org/10.3390/bioengineering10080932
Zamirpour S, Hubbard AE, Feng J, Butte AJ, Pirracchio R, Bishara A. Development of a Machine Learning Model of Postoperative Acute Kidney Injury Using Non-Invasive Time-Sensitive Intraoperative Predictors. Bioengineering. 2023; 10(8):932. https://doi.org/10.3390/bioengineering10080932
Chicago/Turabian StyleZamirpour, Siavash, Alan E. Hubbard, Jean Feng, Atul J. Butte, Romain Pirracchio, and Andrew Bishara. 2023. "Development of a Machine Learning Model of Postoperative Acute Kidney Injury Using Non-Invasive Time-Sensitive Intraoperative Predictors" Bioengineering 10, no. 8: 932. https://doi.org/10.3390/bioengineering10080932
APA StyleZamirpour, S., Hubbard, A. E., Feng, J., Butte, A. J., Pirracchio, R., & Bishara, A. (2023). Development of a Machine Learning Model of Postoperative Acute Kidney Injury Using Non-Invasive Time-Sensitive Intraoperative Predictors. Bioengineering, 10(8), 932. https://doi.org/10.3390/bioengineering10080932