
Long-Bone-Regeneration Process in a Sheep Animal Model, Using Hydroxyapatite Ceramics Prepared by Tape-Casting Method

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
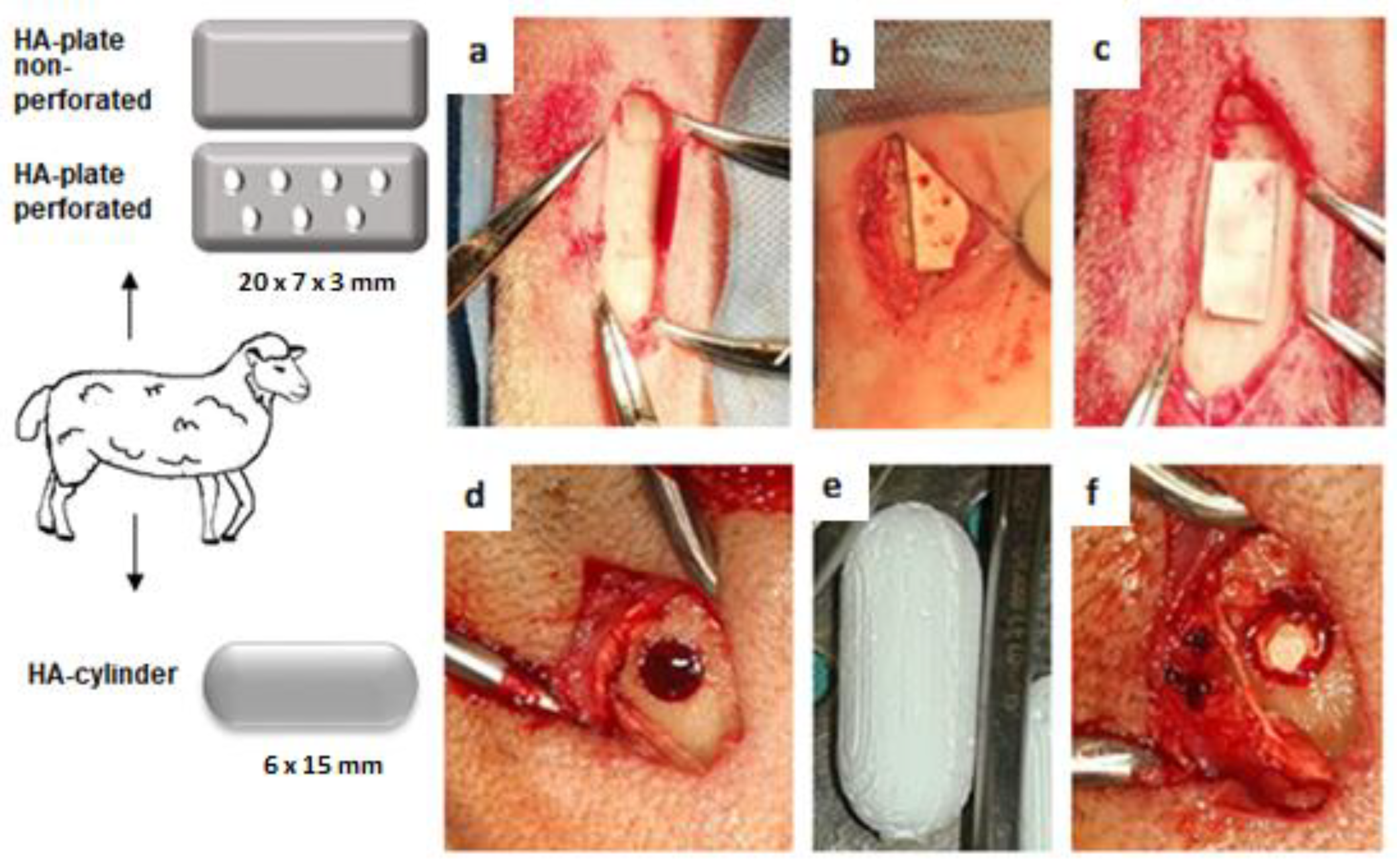
2.1. HA Synthesis and Preparation of HA Ceramics
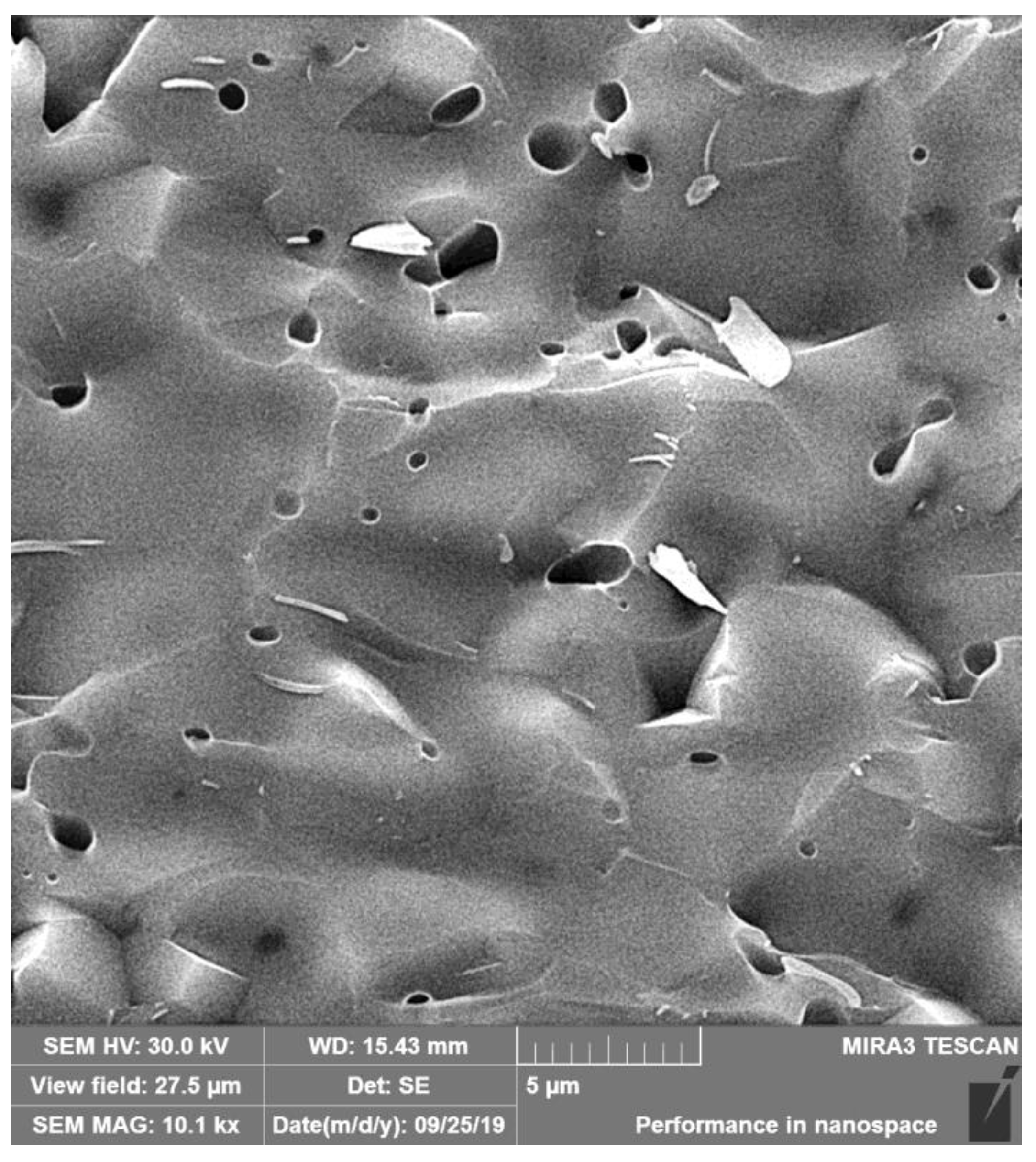
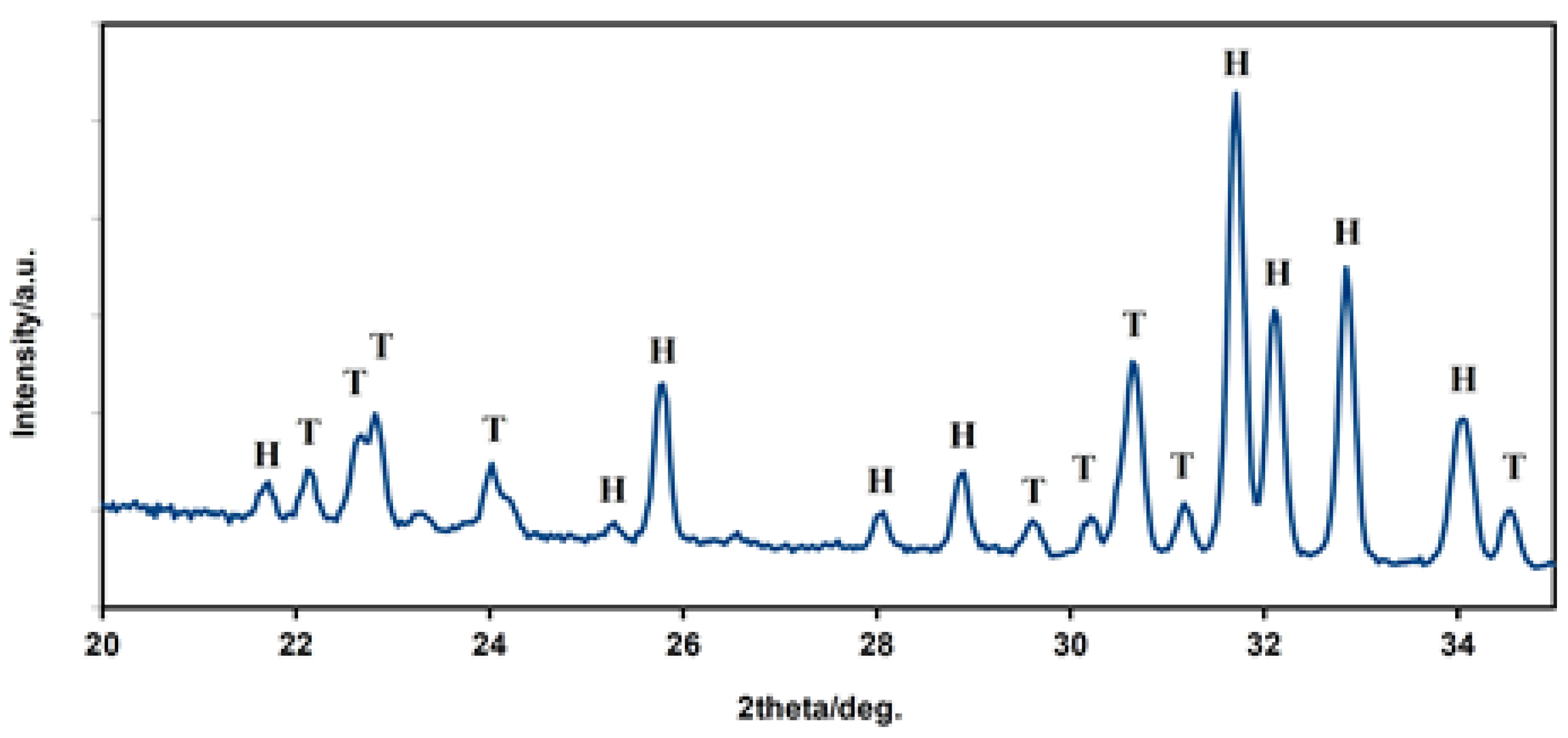
2.2. Characterization of HA Ceramics
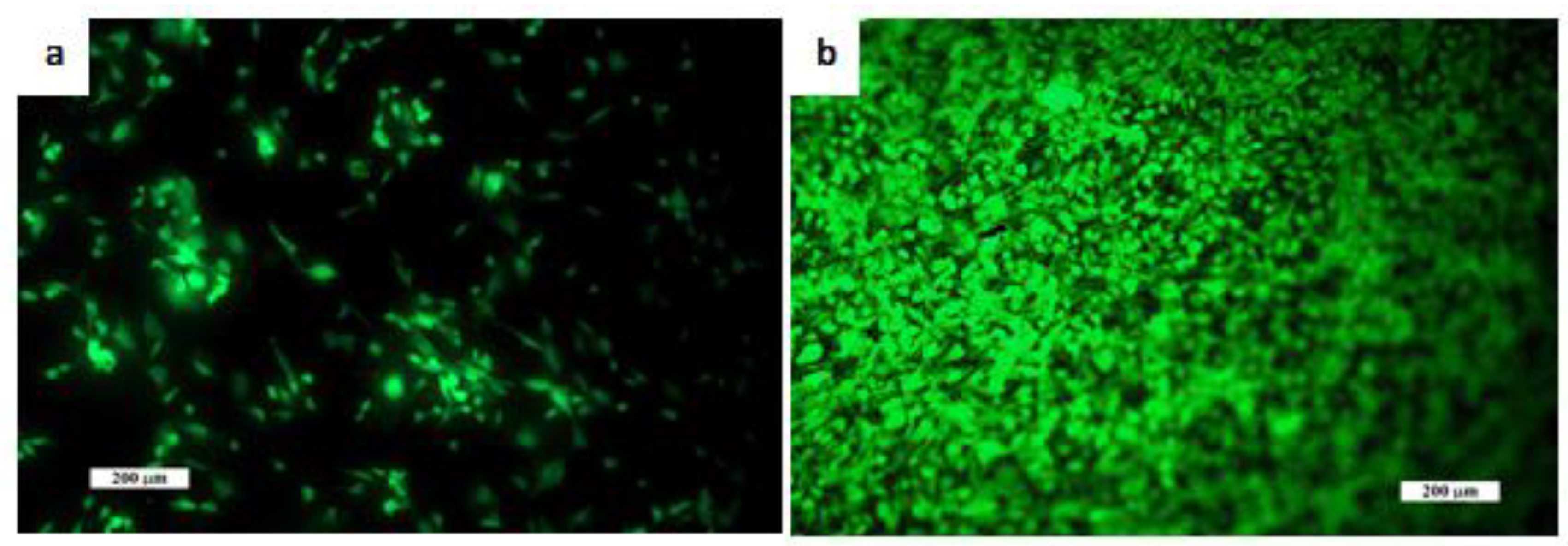
2.3. In Vitro Testing
2.4. Animals, Surgical Procedures, and Postsurgical Management
2.5. Histological and Immunohistochemical Processing
2.6. X-ray and CT Analysis
2.7. Ca/P Ratio
2.8. Statistical Analysis
3. Results
3.1. Microstructure, Properties, and Live/Dead Staining of Ceramic Samples
3.2. General Behaviour of Animals
3.3. Histomorphological and Imunohistochemical Analysis
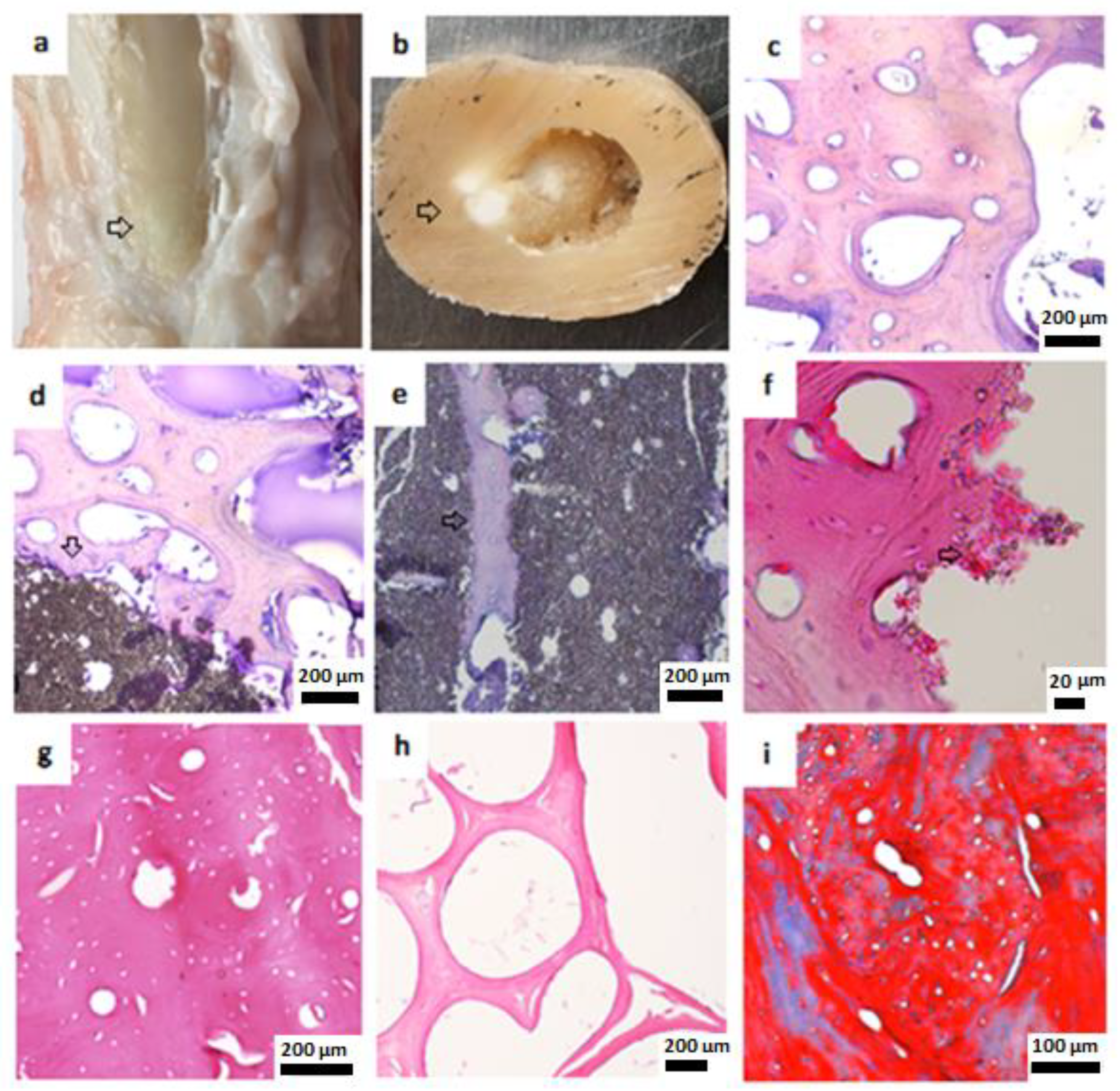
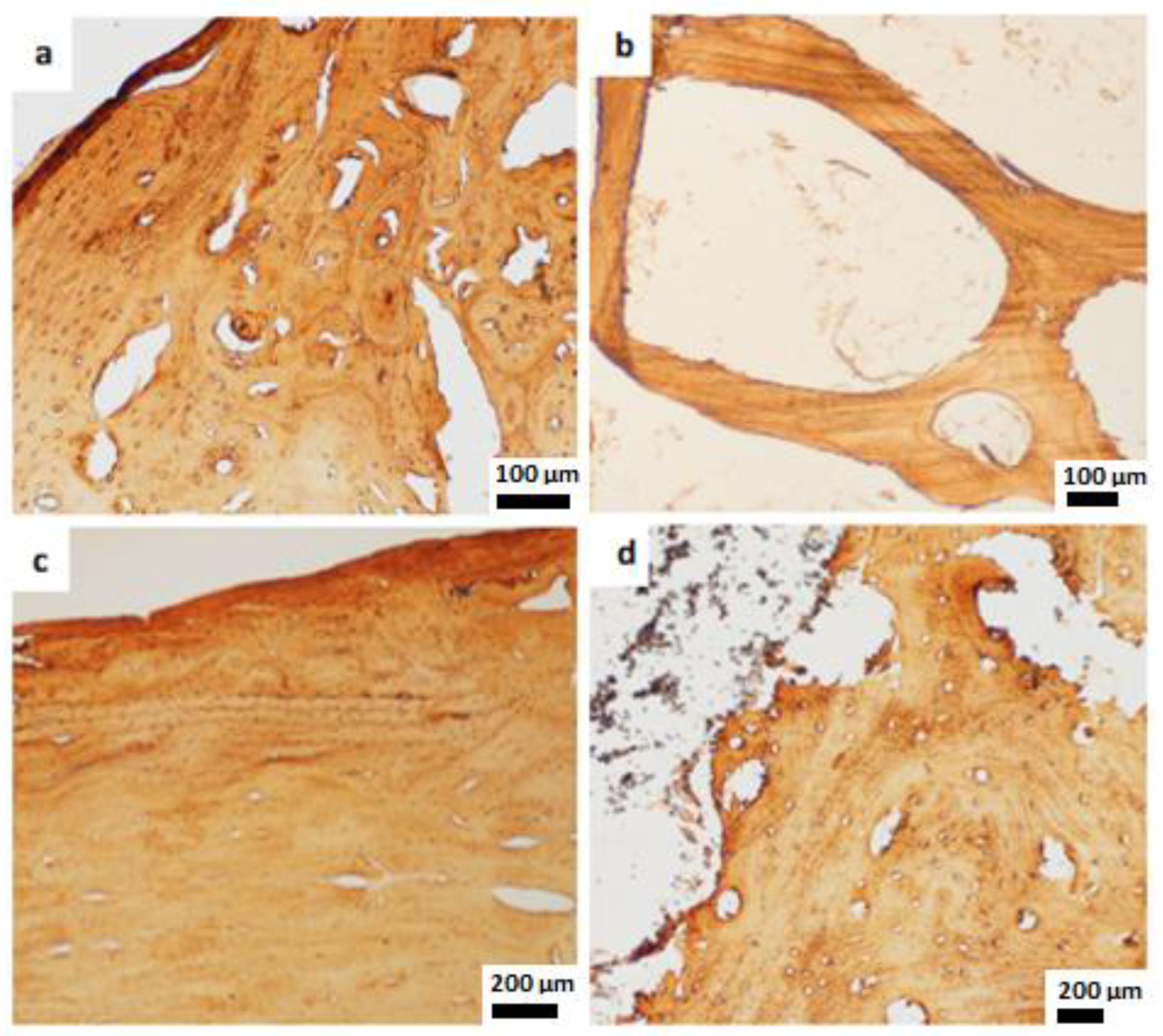
3.3.1. HA Cylinders
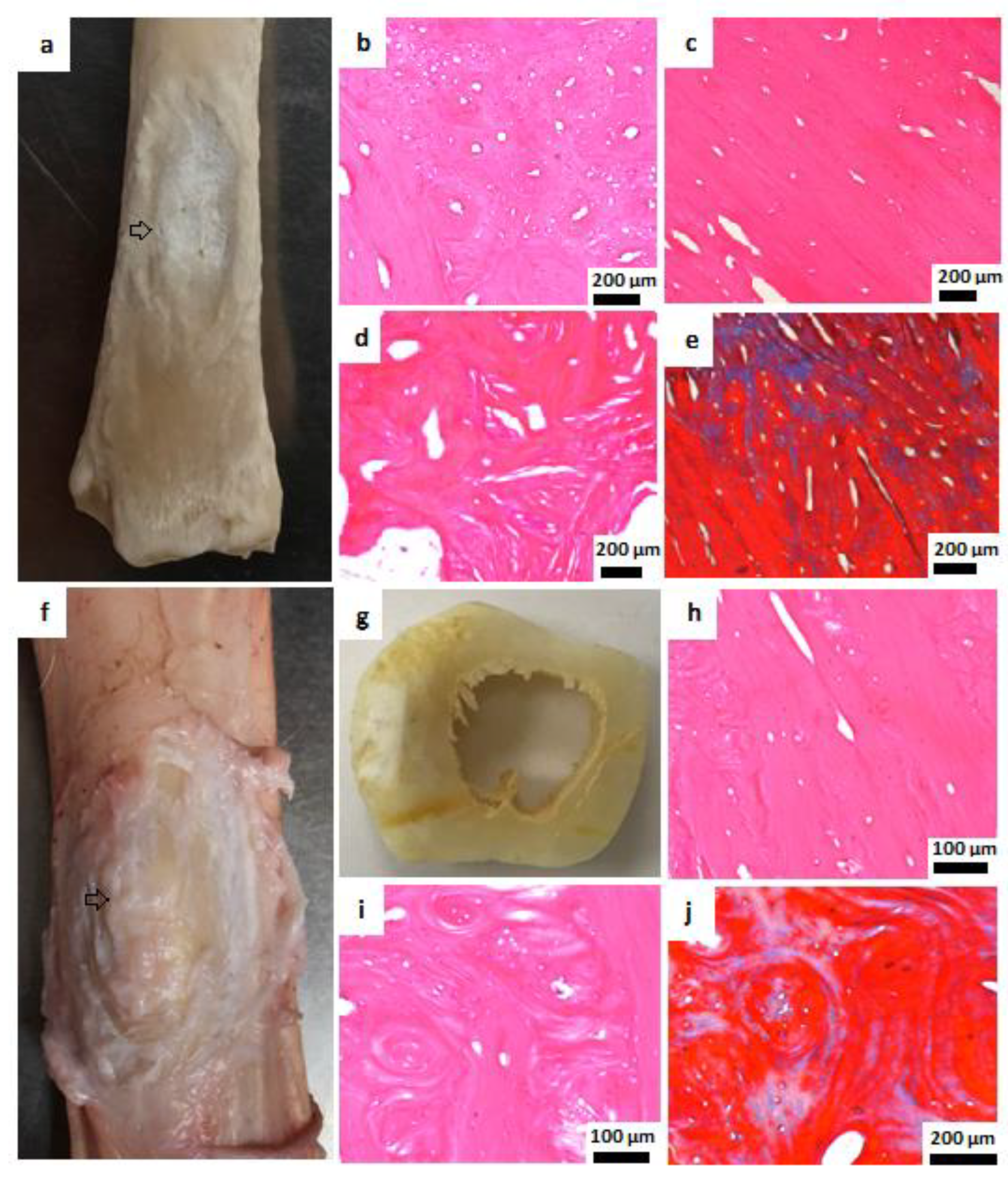
3.3.2. HA Plates
3.4. Ca/P Ratio
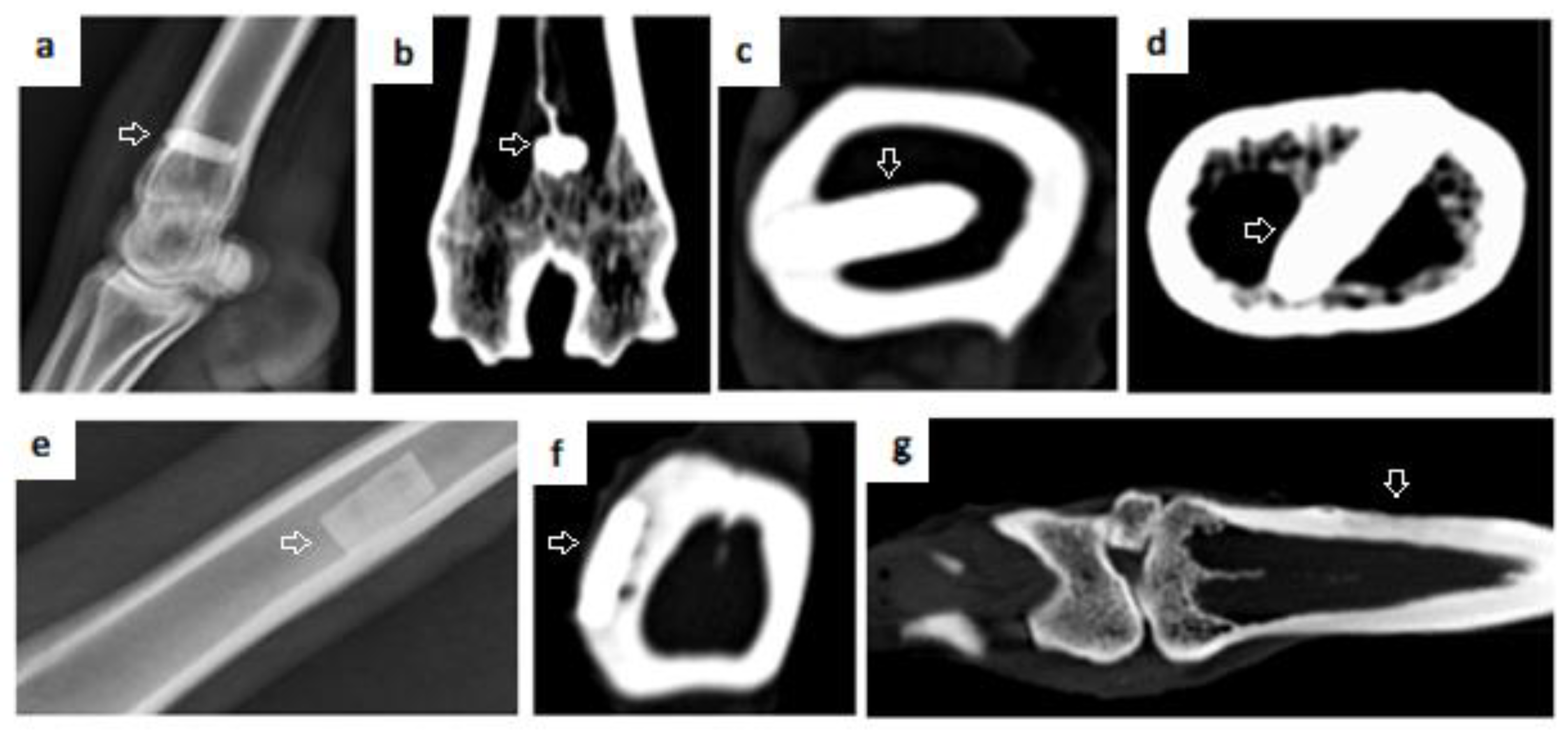
3.5. Radiographic Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Campana, V.; Milano, G.; Pagano, E.; Barba, M.; Cicione, C.; Salonna, G.; Lattanzi, W.; Logroscino, G. Bone substitutes in orthopaedic surgery: From basic science to clinical practice. J Mater. Sci. Mater. Med. 2014, 25, 2445–2461. [Google Scholar] [CrossRef]
- Loi, L.A.; Córdova, J.; Pajarinen, T.; Lin, T.; Yao, Z.; Goodman, S.B. Inflammation, fracture and bone repair. Bone 2015, 86, 119–130. [Google Scholar] [CrossRef]
- Ho-Shui-Ling, A.; Bolander, J.; Rustom, L.E.; Johnson, A.W.; Luyten, F.P.; Picart, C. Bone regeneration strategies: Engineered scaffolds, bioactive molecules and stem cells current stage and future perspectives. Biomaterials 2018, 180, 143–162. [Google Scholar] [CrossRef]
- Zhang, Y.; Shu, T.; Wang, S.; Liu, Z.; Cheng, Y.; Li, A.; Pei, D. The Osteoinductivity of Calcium Phosphate-Based Biomaterials: A Tight Interaction With Bone Healing. Front. Bioeng. Biotechnol. 2022, 16, 911180. [Google Scholar] [CrossRef]
- Bal, Z.; Kaito, T.; Korkusuz, F.; Yoshikawa, H. Bone regeneration with hydroxyapatite-based biomaterials. Emergent. Mater. 2020, 3, 521–544. [Google Scholar] [CrossRef]
- Bajuri, M.Y.; Selvanathan, N.; Dzeidee Schaff, F.N.; Abdul Suki, M.H.; Ng, A.M.H. Tissue-Engineered Hydroxyapatite Bone Scaffold Impregnated with Osteoprogenitor Cells Promotes Bone Regeneration in Sheep Model. Tissue Eng. Regen. Med. 2021, 18, 377–385. [Google Scholar] [CrossRef]
- Owen, G.R.; Dard, M.; Larjava, H. Hydroxyapatite/beta-tricalcium phosphate biphasic ceramics as regenerative material for the repair of complex bone defects. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 106, 2493–2512. [Google Scholar] [CrossRef]
- Ansari, M. Bone tissue regeneration: Biology, strategies and interface studies. Prog. Biomater. 2019, 8, 223–237. [Google Scholar] [CrossRef]
- Jeong, J.; Kim, J.H.; Shim, J.H.; Hwang, N.S.; Heo, C.Y. Bioactive calcium phosphate materials and applications in bone regeneration. Biomater. Res. 2019, 23, 4. [Google Scholar] [CrossRef]
- Ambard, A.J.; Mueninghoff, L. Calcium phosphate cement: Review of mechanical and biological properties. J. Prosthodont. 2006, 15, 321–328. [Google Scholar] [CrossRef]
- Diez-Escudero, A.; Espanol, M.; Montufar, E.; Di Pompo, G.; Ciapetti, G.; Baldini, N.; Ginebra, M.P. Focus Ion Beam/Scanning Electron Microscopy Characterization of Osteoclastic Resorption of Calcium Phosphate Substrates. Tissue Eng. Part C Methods 2017, 23, 118–124. [Google Scholar] [CrossRef]
- Kačarević, Z.P.; Kavehei, F.; Houshmand, A.; Franke, J.; Smeets, R.; Rimashevskiy, D.; Wenisch, S.; Schnettler, R.; Jung, O.; Barbeck, M. Purification processes of xenogeneic bone substitutes and their impact on tissue reactions and regeneration. Int. J. Artif. Organs. 2018, 41, 789–800. [Google Scholar] [CrossRef]
- Danoux, C.B.S.S.; Bassett, D.C.; Othman, Z.; Rodrigues, A.I.; Reis, R.L.; Barralet, J.E.; van Blitterswijk, C.A.; Habibovic, P. Elucidating the Individual Effects of Calcium and Phosphate Ions on hMSCs by Using Composite Materials. Acta Biomater. 2015, 17, 1–15. [Google Scholar] [CrossRef]
- Gauthier, O.; Müller, R.; von Stechow, D.; Lamy, B.; Weiss, P.; Bouler, J.M.; Aguado, E.; Daculsi, G. In vivo bone regeneration with injectable calcium phosphate biomaterial: A three-dimensional micro-computed tomographic, biomechanical and SEM study. Biomaterials 2005, 26, 5444–5453. [Google Scholar] [CrossRef]
- Ducheyne, P.; Healy, K.E.; Hutmacher, D.W.; Grainger, D.W.; Kirkpatrick, C.J. Comprehensive Biomaterials, 1st ed.; Elsevier: Amsterdam, Netherlands, 2011; p. 3672. [Google Scholar]
- Graca, M.P.F.; Gavinho, S.R. Calcium Phosphate Cements in Tissue Engineering. In Contemporary Topics about Phosphorus in Biology and Materials; IntechOpen: London, UK, 2020; Available online: https://www.intechopen.com/books/contemporary-topics-about-phosphorus-in-biology-and-materials/calcium-phosphate-cements-in-tissue-engineering (accessed on 15 January 2022).
- Damien, C.J.; Parsons, J.R. Bone graft and bone graft substitutes: A review of current technology and applications. J. Appl. Biomater. 1991, 2, 187–208. [Google Scholar] [CrossRef]
- Silva, R.V.; Camilli, J.A.; Bertran, C.A.; Moreira, N.H. The use of hydroxyapatite and autogenous cancellous bone grafts to repair bone defects in rats. Int. J. Oral Maxillofac. Surg. 2005, 34, 178–184. [Google Scholar] [CrossRef]
- Wang, W.; Yeung, K.W.K. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2017, 2, 224–247. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Calcium Orthophosphate-Based Bioceramics. Materials 2013, 6, 3840–3942. [Google Scholar] [CrossRef]
- LeGeros, R.Z. Calcium phosphate-based osteoinductive materials. Chem. Rev. 2008, 108, 4742–4753. [Google Scholar] [CrossRef]
- Gosain, A.K.; Song, L.; Riordan, P.; Amarante, M.T.; Nagy, P.G.; Wilson, C.R.; Toth, J.M.; Ricci, J.L. A 1-year study of osteoinduction in hydroxyapatite-derived biomaterials in an adult sheep model: Part I. Plast. Reconstr. Surg. 2002, 109, 619–630. [Google Scholar] [CrossRef]
- Cheng, L.; Ye, F.; Yang, R.; Lu, X.; Shi, Y.; Li, L.; Fan, H.; Bu, H. Osteoinduction of hydroxyapatite/β-tricalcium phosphate bioceramics in mice with a fractured fibula. Acta Biomater. 2010, 6, 1569–1574. [Google Scholar] [CrossRef]
- Yuan, H.; Fernandes, H.; Habibovic, P.; de Boer, J.; Barradas, A.M.C.; de Ruiter, A.; Walsh, W.R.; van Blitterswijk, C.A.; de Bruijn, J.D. Osteoinductive ceramics as a synthetic alternative to autologous bone grafting. Proc. Natl. Acad. Sci. USA 2010, 107, 13614–13619. [Google Scholar] [CrossRef]
- Barradas, A.M.; Yuan, H.; Van der Stok, J.; Quang, B.; Fernandes, H.; Chaterjea, A.; Hogenes, M.C.; Shultz, K.; Donahue, L.R.; van Blitterswijk, C.; et al. The influence of genetic factors on the osteoinductive potential of calcium phosphate ceramics in mice. Biomaterials 2012, 33, 5696–5705. [Google Scholar] [CrossRef]
- Stastny, P.; Sedlacek, R.; Suchy, T.; Lukasova, V.; Rampichova, M.; Trunec, M. Structure Degradation and Strength Changes of Sintered Calcium Phosphate Bone Scaffolds with Different Phase Structures during Simulated Biodegradation In Vitro. Mater. Sci. Eng. C 2019, 100, 544–553. [Google Scholar] [CrossRef]
- Zhi, W.; Wang, X.; Sun, D.; Chen, T.; Yuan, B.; Li, X.; Chen, X.; Wang, J.; Xie, Z.; Zhu, X.; et al. Optimal regenerative repair of large segmental bone defect in a goat model with osteoinductive calcium phosphate bioceramic implants. Bioact. Mater. 2022, 11, 240–253. [Google Scholar] [CrossRef]
- Yoshikawa, H.; Myoui, A. Bone tissue engineering with porous hydroxyapatite ceramics. J. Artif. Organs. 2005, 8, 131–136. [Google Scholar] [CrossRef]
- França, R.; Samani, T.D.; Bayade, G.; Yahia, L.H.; Sacher, E. Nanoscale surface characterization of biphasic calcium phosphate, with comparisons to calcium hydroxyapatite and β-tricalcium phosphate bioceramics. J. Colloid Interface Sci. 2014, 420, 182–188. [Google Scholar] [CrossRef]
- Pang, K.M.; Lee, J.K.; Seo, Y.K.; Kim, S.M.; Kim, M.J.; Lee, J.H. Biologic properties of nano-hydroxyapatite: An in vivo study of calvarial defects, ectopic bone formation and bone implantation. Biomed. Mater. Eng. 2015, 25, 25–38. [Google Scholar] [CrossRef]
- Sakamoto, M.; Masanori, N.; Matsumoto, T.; Okihana, H. Development of superporous hydroxyapatites and their examination with a culture of primary rat osteoblasts. J. Biomed. Mater. Res. A 2007, 82, 238–242. [Google Scholar] [CrossRef]
- Marin, C.; Luyteni, F.P.; Van der Schueren, B.; Kerckhofs, G.; Vandamme, K. The impact of type 2 diabetes on bone fracture healing. Front. Endocrinol. 2018, 9, 6. [Google Scholar] [CrossRef]
- Kattimani, V.S.; Kondaka, S.; Lingamaneni, K.P. Hydroxyapatite—Past, present, and future in bone regeneration. Bone Tissue Regen. Insights. 2016, 7, 9–19. [Google Scholar] [CrossRef]
- Zhou, H.; Lee, J. Nanoscale hydroxyapatite particles for bone tissue engineering. Acta Biomater. 2011, 7, 2769–2781. [Google Scholar] [CrossRef]
- Brum, I.S.; Carvalho, J.J.; Pires, J.L.; Carvalho, M.A.; Ferreira dos Santos, L.B.; Elias, C.N. Nanosized hydroxyapatite and β-tricalcium phosphate composite: Physico-chemical, cytotoxicity, morphological properties and in vivo trial. Sci. Rep. 2019, 9, 19602. [Google Scholar] [CrossRef]
- Salehi, M.; Naseri-Nosar, M.; Ebrahimi-Barough, S.; Nourani, M.; Vaez, A.; Farzamfar, S.; Ai, J. Regeneration of sciatic nerve crush injury by a hydroxyapatite nanoparticle-containing collagen type I hydrogel. J. Physiol. Sci. 2018, 68, 579–587. [Google Scholar] [CrossRef]
- Prado, J.P.D.S.; Yamamura, H.; Magri, A.M.P.; Ruiz, P.L.M.; Prado, J.L.D.S.; Rennó, A.C.M.; Ribeiro, D.A.; Granito, R.N. In vitro and in vivo biological performance of hydroxyapatite from fish waste. J. Mater. Sci. Mater. Med. 2021, 32, 109. [Google Scholar] [CrossRef]
- Giorno, B.; Castro-Silva, I.I.; Rossi, A.M.; Granjeiro, J. Comparative In Vivo Study of Biocompatibility of Apatites Incorporated with 1% Zinc or Lead Ions versus Stoichiometric Hydroxyapatite. J. Biomim. Biomater. Biomed. Eng. 2014, 19, 109–120. [Google Scholar] [CrossRef]
- Zhang, Y.; Wu, Y.; Qiao, X.; Lin, T.; Wang, Y.; Wang, M. Biomaterial-based strategy for bone tumor therapy and bone defect regeneration: An innovative application option. Front. Mater. 2022, 9, 990931. [Google Scholar] [CrossRef]
- Qu, H.; Fu, H.; Han, Z.; Sun, Y. Biomaterials for bone tissue engineering scaffolds: A review. RSC Adv. 2019, 9, 26252–26262. [Google Scholar] [CrossRef]
- Kong, Y.M.; Kim, H.E.; Kim, H.W. Phase Conversion of Tricalcium Phosphate into Ca-Deficient Apatite During Sintering of Hydroxyapatite–Tricalcium Phosphate Biphasic Ceramics. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 84, 334–339. [Google Scholar] [CrossRef]
- Huang, S.M.; Liu, S.M.; Chen, W.C.; Ko, C.L.; Shih, C.J.; Chen, J.C. Morphological Changes, Antibacterial Activity, and Cytotoxicity Characterization of Hydrothermally Synthesized Metal Ions-Incorporated Nanoapatites for Biomedical Application. Pharmaceuticals 2022, 15, 885. [Google Scholar] [CrossRef]
- Yang, H.; Qu, X.; Lin, W.; Wang, C.; Zhu, D.; Dai, K.; Zheng, Y. In vitro and in vivo studies on zinc-hydroxyapatite composites as novel biodegradable metal matrix composite for orthopedic applications. Acta Biomaterialia. 2018, 71, 200–214. [Google Scholar] [CrossRef]
- Chu, C.L.; Xue, X.Y.; Zhu, J.C.; Yin, Z.D. In vivo study on biocompatibility and bonding strength of hydroxyapatite-20vol%Ti composite with bone tissues in the rabbit. Biomed. Mater. Eng. 2006, 16, 203–213. [Google Scholar]
- Rustom, L.E.; Poellmann, M.J.; Wagoner Johnson, A.J. Mineralization in Micropores of Calcium Phosphate Scaffolds. Acta Biomater. 2019, 83, 435–455. [Google Scholar] [CrossRef]
- Heymann, D.; Pradal, G.; Benahmed, M. Cellular mechanisms of calcium phosphate ceramic degradation. Histol. Histopathol. 1999, 14, 871–877. [Google Scholar] [CrossRef]
- Klein, C.P.; Driessen, A.A.; de Groot, K.; van den Hooff, A. Biodegradation behavior of various calcium phosphate materials in bone tissue. J. Biomed. Mater. Res. 1983, 17, 769–784. [Google Scholar] [CrossRef]
- Cao, W.; Hench, L. Bioactive materials. Ceram. Int. 1996, 22, 493–507. [Google Scholar] [CrossRef]
- Eggli, P.S.; Müller, W.; Schenk, R.K. Porous hydroxyapatite and tricalcium phosphate cylinders with two different pore size ranges implanted in the cancellous bone of rabbits. A comparative histomorphometric and histologic study of bony ingrowth and implant substitution. Clin. Orthop. Relat. Res. 1988, 232, 127–138. [Google Scholar] [CrossRef]
- Ginebra, M.P.; Espanol, M.; Maazouz, Y.; Bergez, V.; Pastorino, D. Bioceramics and bone healing. EFORT Open Rev. 2018, 3, 173–183. [Google Scholar] [CrossRef]
- Egol, K.A.; Nauth, A.; Lee, M.; Pape, H.-C.; Watson, J.T.; Borrelli, J. Bone Grafting: Sourcing, Timing, Strategies, and Alternatives. J. Orthop. Trauma 2015, 29, 10–14. [Google Scholar] [CrossRef]
- Garcaí-Gareta, E.; Hua, J.; Knowles, J.C.; Blunn, G.W. Comparison of mesenchymal stem cell proliferation and differentiation between biomimetic and electrochemical coatings on different topographic surfaces. J. Mater. Sci. Mater. Med. 2013, 24, 199–210. [Google Scholar] [CrossRef]
- Scaran, A.; Perrotti, V.; Artese, L.; Degidi, M.; Degidi, D.; Piattelli, A.; Iezzi, G. Blood vessels are concentrated within the implant surface concavities: A histologic study in rabbit tibia. Odontology 2014, 102, 259–266. [Google Scholar] [CrossRef]
- Hing, K.A. Bioceramic bone graft substitutes: Influence of porosity and chemistry. Int. J. Appl. Ceram. Technol. 2005, 2, 184–199. [Google Scholar] [CrossRef]
- Aguirre, A.; González, A.; Navarro, M.; Castaño, Ó.; Planell, J.A.; Engel, E. Control of microenvironmental cues with a smart biomaterial composite promotes endothelial progenitor cell angiogenesis. Eur. Cells Mater. 2012, 24, 90–106. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Rahaman, M.; Liu, Y.; Huang, Y.W. Evaluation of Open Hollow Hydroxyapatite Microsphere on Bone Regeneration in Rat Calvarial Defects. bioRxiv 2019. [Google Scholar] [CrossRef]
- Tanaka, M.; Haniu, H.; Kamanaka, T.; Takizawa, T.; Sobajima, A.; Yoshida, K.; Aoki, K.; Okamoto, M.; Kato, H.; Saito, N. Physico-Chemical, In Vitro, and In Vivo Evaluation of a 3D Unidirectional Porous Hydroxyapatite Scaffold for Bone Regeneration. Materials 2017, 10, 33. [Google Scholar] [CrossRef] [PubMed]
- Willie, B.M.; Bloebaum, R.D.; Bireley, W.R.; Bachus, K.N.; Hofmann, A.A. Determining relevance of a weightbearing ovine model for bone ingrowth assessment. J. Biomed. Mater. Res. A 2004, 69, 567–576. [Google Scholar] [CrossRef]
- Charbonnier, B.; Manassero, M.; Bourguignon, A.D.; Decambron, A.; El-Hafci, H.; Morin, C.; Leon, D.; Bensidoum, M.; Corsia, S.; Petite, H.; et al. Custom-made macroporous bioceramic implants based on triply-periodic minimal surfaces for bone defects in load-bearing sites. Acta Biomater. 2020, 109, 254–266. [Google Scholar] [CrossRef]
- Machado, G.C.P.; Vaz Braga Pintor, A.; Calasans, M.M.D. Evaluation of strontium-containing hydroxyapatite as bone substitute in sheep tibiae. Braz. J. Implantol. Health Sci. 2019, 1, 153–164. [Google Scholar] [CrossRef]
- Zhao, H.; Tang, J.; Zhou, D.; Weng, Y.; Qin, W.; Liu, C.; Lv, S.; Wang, W.; Zhao, X. Electrospun Icariin-Loaded Core-Shell Collagen, Polycaprolactone, Hydroxyapatite Composite Scaffolds for the Repair of Rabbit Tibia Bone Defects. Int. J. Nanomed. 2020, 15, 3039–3056. [Google Scholar] [CrossRef]
- Barradas, A.M.; Yuan, H.; Van Blitterswijk, C.A.; Habibovic, P. Osteoinductive biomaterials: Current knowledge of properties, experimental models and biological mechanisms. Eur. Cells Mater. 2011, 21, 407–429. [Google Scholar] [CrossRef]
- Habraken, W.; Habibovic, P.; Epple, M.; Bohner, M. Calcium phosphates in biomedical applications: Materials for the future? Mater. Today 2016, 19, 69–87. [Google Scholar] [CrossRef]
- Li, X.; Ma, B.; Li, J.; Shang, L.; Liu, H.; Ge, S. A method to visually observe the degradation-diffusion-reconstruction behavior of hydroxyapatite in the bone repair process. Acta Biomater. 2020, 101, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Chow, K.L.; Leng, Y. Study of hydroxyapatite osteoinductivity with an osteogenic differentiation of mesenchymal stem cells. J. Biomed. Mater. Res. A 2009, 89, 326–335. [Google Scholar] [CrossRef]
- Ressler, A.; Žužić, A.; Ivanišević, I.; Kamboj, N.; Ivanković, H. Ionic substituted hydroxyapatite for bone regeneration applications: A review. Open Ceram. 2021, 6, 100122. [Google Scholar] [CrossRef]
- Viateau, V.; Manassero, M.; Sensébé, L.; Langonné, A.; Marchat, D.; Logeart-Avramoglou, D.; Petite, H.; Bensidhoum, M. Comparative study of the osteogenic ability of four different ceramic constructs in an ectopic large animal model. J. Tissue Eng. Regen. Med. 2016, 10, 177–187. [Google Scholar] [CrossRef]
- Bensaïd, W.; Oudina, K.; Viateau, V.; Potier, E.; Bousson, V.; Blanchat, C.; Sedel, L.; Guillemin, G. Petite, De novo reconstruction of functional bone by tissue engineering in the metatarsal sheep model. Tissue Eng. 2005, 11, 814–824. [Google Scholar] [CrossRef]
- Viateau, V.; Guillemin, G.; Bousson, V.; Oudina, K.; Hannouche, D.; Sedel, L.; Logeart-Avramoglou, D.; Petite, H. Long-bone critical-size defects treated with tissue-engineered grafts: A study on sheep. J. Orthop. Res. 2007, 25, 741–749. [Google Scholar] [CrossRef]
- Kon, E.; Salamanna, F.; Filardo, G.; Di Matteo, B.; Shabshin, N.; Shani, J.; Fini, M.; Perdisa, F.; Parrilli, A.; Sprio, S.; et al. Bone Regeneration in Load-Bearing Segmental Defects, Guided by Biomorphic, Hierarchically Structured Apatitic Scaffold. Front. Bioeng. Biotechnol. 2021, 9, 734486. [Google Scholar] [CrossRef]
- Marcacci, M.; Kon, E.; Zaffagnini, S.; Rocca, M.; Corsi, A.; Benvenuti, A.; Bianco, P.; Quarto, R.; Martin, I.; Muraglia, A.; et al. Reconstruction of extensive long-bone defects in sheep using porous hydroxyapatite sponges. Calcif. Tissue Int. 1999, 64, 83–90. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
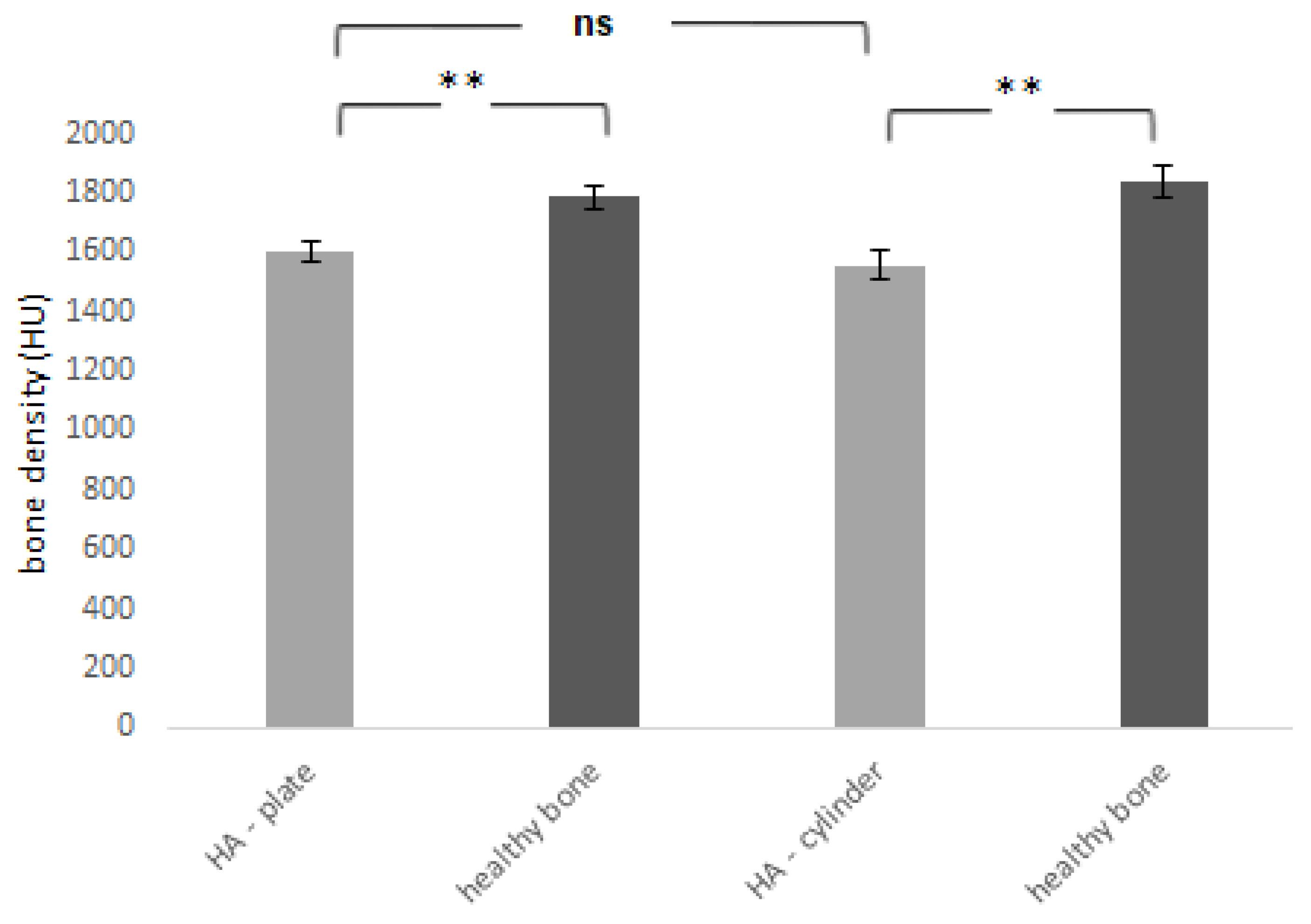
| a | a’ | b | b’ | |
|---|---|---|---|---|
| Bone density (HU) mean ± SD | 1607 ± 81 | 1789 ± 96 | 1559 ± 127 | 1839 ± 129 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kresakova, L.; Medvecky, L.; Vdoviakova, K.; Varga, M.; Danko, J.; Totkovic, R.; Spakovska, T.; Vrzgula, M.; Giretova, M.; Briancin, J.; et al. Long-Bone-Regeneration Process in a Sheep Animal Model, Using Hydroxyapatite Ceramics Prepared by Tape-Casting Method. Bioengineering 2023, 10, 291. https://doi.org/10.3390/bioengineering10030291
Kresakova L, Medvecky L, Vdoviakova K, Varga M, Danko J, Totkovic R, Spakovska T, Vrzgula M, Giretova M, Briancin J, et al. Long-Bone-Regeneration Process in a Sheep Animal Model, Using Hydroxyapatite Ceramics Prepared by Tape-Casting Method. Bioengineering. 2023; 10(3):291. https://doi.org/10.3390/bioengineering10030291
Chicago/Turabian StyleKresakova, Lenka, Lubomir Medvecky, Katarina Vdoviakova, Maros Varga, Ján Danko, Roman Totkovic, Tatiana Spakovska, Marko Vrzgula, Maria Giretova, Jaroslav Briancin, and et al. 2023. "Long-Bone-Regeneration Process in a Sheep Animal Model, Using Hydroxyapatite Ceramics Prepared by Tape-Casting Method" Bioengineering 10, no. 3: 291. https://doi.org/10.3390/bioengineering10030291
APA StyleKresakova, L., Medvecky, L., Vdoviakova, K., Varga, M., Danko, J., Totkovic, R., Spakovska, T., Vrzgula, M., Giretova, M., Briancin, J., Šimaiová, V., & Kadasi, M. (2023). Long-Bone-Regeneration Process in a Sheep Animal Model, Using Hydroxyapatite Ceramics Prepared by Tape-Casting Method. Bioengineering, 10(3), 291. https://doi.org/10.3390/bioengineering10030291