
Post-Operative Delirium and Cognitive Dysfunction in Aged Patients Undergoing Cardiac Surgery: A Randomized Comparison between Two Blood Oxygenators

 ,
,  , , ,
, , , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Measurements and Laboratory Data
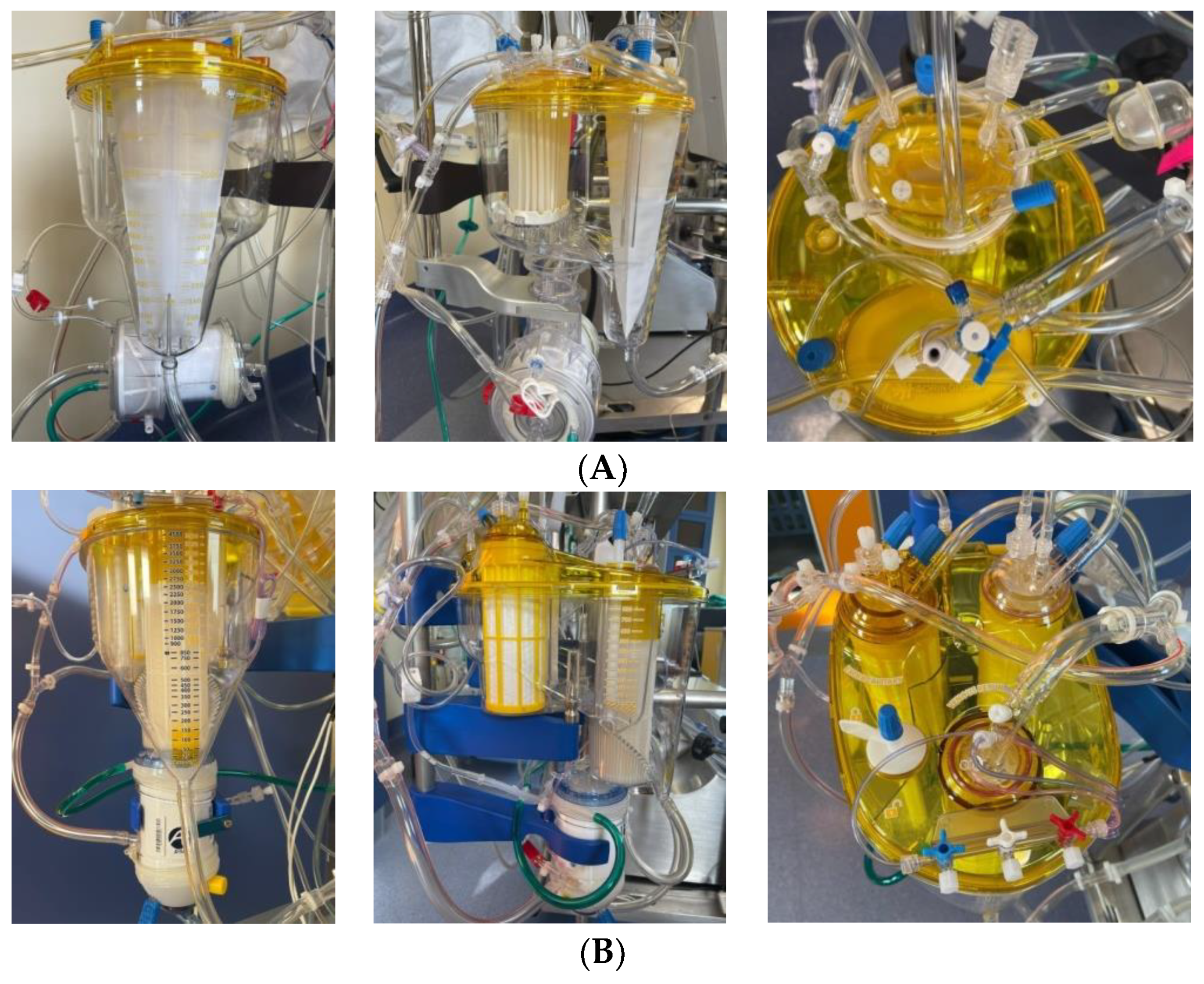
2.3. Blood Oxygenators
2.4. Statistical Analysis
3. Results
3.1. Mental Assessment and Cognitive Impairment
3.2. Inflammatory Variables
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holman, W.L.; Timpa, J.; Kirklin, J.K. Origins and Evolution of Extracorporeal Circulation. J. Am. Coll. Cardiol. 2022, 79, 1606–1622. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.; LeClerc, J.L.; Vincent, J.L. Inflammatory response to cardiopulmonarybypass: Mechanisms involved and possible therapeutic strategies. Chest 1997, 112, 676–692. [Google Scholar] [CrossRef] [PubMed]
- Kats, S.; Schönberger, J.P.; Brands, R.; Seinen, W.; van Oeveren, W. Endotoxin release in cardiac surgery with cardiopulmonary bypass: Pathophysiology and possible therapeutic strategies. An update. Eur. J. Cardio-Thoracic Surg. 2011, 39, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Mietani, K.; Hasegawa-Moriyama, M.; Inoue, R.; Ogata, T.; Shimojo, N.; Kurano, M.; Sumitani, M.; Uchida, K. Elevated neuron-specific enolase level is associated with postoperative delirium and detection of phosphorylated neurofilament heavy subunit: A prospective observational study. PLoS ONE 2021, 16, e0259217. [Google Scholar] [CrossRef] [PubMed]
- Day, J.; Taylor, K. The systemic inflammatory response syndrome and cardiopulmonary bypass. Int. J. Surg. 2005, 3, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Anastasiadis, K.; Argiriadou, H.; Kosmidis, M.H.; Megari, K.; Antonitsis, P.; Thomaidou, E.; Aretouli, E.; Papakonstantinou, C. Neurocognitive outcome after coronary artery bypass surgery using minimal versus conventional extracorporeal circulation: A randomised controlled pilot study. Heart 2011, 97, 1082–1088. [Google Scholar] [CrossRef]
- Tony, V.; Julian, A. An Update on Postoperative Cognitive Dysfunction Following Cardiac Surgery. Front. Psychiatry 2022, 13, 884907. [Google Scholar]
- Phillips-Bute, B.; Mathew, J.P.; Blumenthal, J.A.; Grocott, H.P.M.; Laskowitz, D.T.; Jones, R.H.; Mark, D.B.; Newman, M.F. Association of Neurocognitive Function and Quality of Life 1 Year After Coronary Artery Bypass Graft (CABG) Surgery. Psychosom. Med. 2006, 68, 369–375. [Google Scholar] [CrossRef]
- Funder, K.S.; Steinmetz, J.; Rasmussen, L.S. Cognitive dysfunction after cardiovascular surgery. Minerva Anestesiol. 2009, 75, 329–332. [Google Scholar]
- Kupiec, A.; Adamik, B.; Forkasiewicz-Gardynik, K.; Goździk, W. Intra-operative hyperoxia and the risk of delirium in elderly patients after cardiac surgery. Aging 2020, 12, 7006–7014. [Google Scholar] [CrossRef]
- Berger, M.; Terrando, N.; Smith, S.K.; Browndyke, J.N.; Newman, M.F.; Mathew, J.P. Neurocognitive Function after Cardiac Surgery: From Phenotypes to Mechanisms. Anesthesiology 2018, 129, 829–851. [Google Scholar] [CrossRef]
- Brown, C.H., 4th; Probert, J.; Healy, R.; Parish, M.; Nomura, Y.; Yamaguchi, A.; Tian, J.; Zehr, K.; Mandal, K.; Kamath, V.; et al. Cognitive Decline after Delirium in Patients Undergoing Cardiac Surgery. Anesthesiology 2018, 129, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Molardi, A.; Di Chicco, M.V.; Carino, D.; Goldoni, M.; Ricci, M.; Borrello, B.; Gripshi, F.; Gherli, T.; Nicolini, F. The use of RemoweLL oxygenator-integrated device in the prevention of the complications related to aortic valve surgery in the elderly patient: Preliminary results. Eur. J. Prev. Cardiol. 2018, 25, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.S.; Weiner, M.M.; Arora, R.C.; Chung, I.; Deshpande, R.; Varghese, R.; Augoustides, J.; Ramakrishna, H. Current approach to diagnosis and treatment of delirium after cardiac surgery. Ann. Card. Anaesth. 2016, 19, 328–337. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Kaza, A.K.; Cope, J.T.; Fiser, S.M.; Long, S.M.; A Kern, J.; Kron, I.L.; Tribble, C.G. Elimination of fat microemboli during cardiopulmonary bypass. Ann. Thorac. Surg. 2003, 75, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Issitt, R.W.; Harvey, I.; Walsh, B.; Voegeli, D. Quantification of Lipid Filtration and the Effects on Cerebral Injury During Cardiopulmonary Bypass. Ann. Thorac. Surg. 2017, 104, 884–890. [Google Scholar] [CrossRef]
- Villar, J.; Pérez-Méndez, L.; Blanco, J.; Añón, J.M.; Blanch, L.; Belda, J.; Santos-Bouza, A.; Fernández, R.L.; Kacmarek, R.M.; Spanish Initiative for Epidemiology, Stratification, and Therapies for ARDS (SIESTA) Network. A universal definition of ARDS: The PaO2/FiO2 ratio under a standard ventilatory setting—A prospective, multicenter validation study. Intensive Care Med. 2013, 39, 583–592. [Google Scholar] [CrossRef]
- Benstoem, C.; Bleilevens, C.; Borchard, R.; Stoppe, C.; Goetzenich, A.; Autschbach, R.; Breuer, T. Retrospective Analysis of Air Handling by Contemporary Oxygenators in the Setting of Cardiac Surgery. Ann. Thorac. Cardiovasc. Surg. 2018, 24, 230–237. [Google Scholar] [CrossRef]
- Shann, K.G.; Likosky, D.S.; Murkin, J.M.; Baker, R.A.; Baribeau, Y.R.; DeFoe, G.R.; Dickinson, T.A.; Gardner, T.J.; Grocott, H.P.; O’connor, G.T.; et al. An evidence-based review of the practice of cardiopulmonary bypass in adults: A focus on neurologic injury, glycemic control, hemodilution, and the inflammatory response. J. Thorac. Cardiovasc. Surg. 2006, 132, 283–290. [Google Scholar] [CrossRef]
- Schmitt, B.; Bauersfeld, U.; Schmid, E.R.; Tuchschmid, P.; Molinari, L.; Fanconi, S.; Bandtlow, C. Serum and CSF levels of neuron-specific enolase (NSE) in cardiac surgery with cardiopulmonary bypass: A marker of brain injury? Brain Dev. 1998, 20, 536–539. [Google Scholar] [CrossRef] [PubMed]
- Ishida, M.; Takahashi, S.; Okamura, H. Comparison of bubble removal performances of five membrane oxygenators with and without a pre-filter. Perfusion 2022, 38, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Ramlawi, B.; Rudolph, J.L.; Mieno, S.; Khabbaz, K.; Sodha, N.R.; Boodhwani, M.; Levkoff, S.E.; Marcantonio, E.R.; Sellke, F.W. Serologic markers of brain injury and cognitive function after cardiopulmonary bypass. Ann. Surg. 2006, 244, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.S.; Christiansen, M.; Rasmussen, H.; Kristensen, P.A.; Moller, J.T. Do blood concentrations of neurone specific enolase and S-100 beta protein reflect cognitive dysfunction after abdominal surgery? SPOCD Group. Br. J. Anaesth. 2000, 84, 242–244. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inspire | RemoweLL 2 | Overall | p | |
|---|---|---|---|---|
| n | 73 | 81 | 154 | |
| Male, n (%) | 49 (57.0) | 48 (56.5) | 97 (56.7) | 1.000 |
| Age (median, Q1–Q3) | 75 (71–79) | 76 (71–79) | 76 (71–79) | 0.623 |
| BMI (median, Q1–Q3) | 27.0 (24.7–29.8) | 26.0 (24.2–28.7) | 26.3 (24.4–29.1) | 0.333 |
| Recent hospitalization, n (%) | 9 (12.5) | 12 (14.8) | 21 (13.7) | 0.815 |
| Hypertension, n (%) | 59 (83.1) | 73 (90.1) | 132 (86.8) | 0.234 |
| Dyslipidemia, n (%) | 25 (34.7) | 34 (42.0) | 59 (38.6) | 0.407 |
| Type 2 diabetes, n (%) | 21 (29.2) | 18 (22.5) | 39 (25.7) | 0.360 |
| Prior MI, n (%) | 4 (5.6) | 3 (3.7) | 7 (4.6) | 0.706 |
| Prior PCI, n (%) | 5 (6.9) | 11 (13.6) | 16 (10.5) | 0.199 |
| Recent PCI, n (%) | 1 (20.0) | 1 (9.1) | 2 (12.5) | 1.000 |
| Prior CABG, n (%) | 1 (1.4) | 0 (0.0) | 1 (0.7) | 0.471 |
| Prior heart surgery, n (%) | 8 (11.1) | 5 (6.3) | 13 (8.6) | 0.387 |
| Peripheral artery disease, n (%) | 18 (25.4) | 21 (26.3) | 39 (25.8) | 1.000 |
| COPD, n (%) | 7 (9.9) | 9 (11.3) | 16 (10.6) | 1.000 |
| Anxiety disorder, n (%) | 0 (0.0) | 4 (4.9) | 4 (2.6) | 0.123 |
| Depression, n (%) | 3 (4.2) | 7 (8.8) | 10 (6.6) | 0.334 |
| Parkinson’s disease, n (%) | 0 (0.0) | 1 (1.2) | 1 (0.7) | 1.000 |
| Euroscore II (median, Q1–Q3) | 3.1 (1.8–6.0) | 3.5 (2.5–6.1) | 3.4 (2.3–6.1) | 0.325 |
| White blood cells (median, Q1–Q3) | 7.2 (6.2–8.6) | 7.2 (6.4–8.2) | 7.2 (6.2–8.3) | 0.496 |
| Haemoglobin (median, Q1–Q3) | 13.2 (11.9–14.4) | 13.2 (12.5–14.3) | 13.2 (12.3–14.3) | 0.629 |
| Platelets (median, Q1–Q3) | 194.0 (156.0–229.0) | 192.0 (171.0–234.0) | 193.5 (167.0–231.0) | 0.639 |
| Neutophils (median, Q1–Q3) | 4.8 (4.0–5.9) | 4.8 (3.9–5.7) | 4.8 (3.9–5.7) | 0.732 |
| Limphocytes (median, Q1–Q3) | 1.7 (1.2–2.1) | 1.5 (1.2–1.8) | 1.6 (1.2–2.0) | 0.203 |
| Monocytes (median, Q1–Q3) | 0.6 (0.5–0.7) | 0.6 (0.5–0.7) | 0.6 (0.5–0.7) | 1.000 |
| Creatinine (median, Q1–Q3) | 1.0 (0.8–1.2) | 1.0 (0.8–1.2) | 1.0 (0.8–1.2) | 0.841 |
| Cholesterol (median, Q1–Q3) | 151.0 (125.0–187.0) | 147.5 (128.5–169.5) | 150.0 (128.0–175.0) | 0.198 |
| Triglycerides (median, Q1–Q3) | 103.0 (76.0–133.0) | 101.5 (86.5–119.0) | 102.0 (81.0–126.0) | 0.859 |
| HDL (median, Q1–Q3) | 42.0 (36.0–51.0) | 45.0 (38.0–53.0) | 43.5 (37.0–52.0) | 0.396 |
| LDL (median, Q1–Q3) | 83.4 (68.4–108.2) | 79.4 (64.6–98.1) | 81.7 (65.6–102.4) | 0.104 |
| Albumin (median, Q1–Q3) | 4.3 (4.1–4.5) | 4.2 (3.9–4.4) | 4.2 (4.0–4.4) | 0.041 |
| C Reactive Protein (median, Q1–Q3) | 0.2 (0.1–0.4) | 0.2 (0.1–0.6) | 0.2 (0.1–0.5) | 0.486 |
| HS troponin (median, Q1–Q3) | 16.5 (14.0–29.5) | 17.0 (13.0–19.0) | 17.0 (13.0–21.0) | 0.596 |
| CCS angina class, n (%) | 0.905 | |||
| 1 | 4 (30.8) | 6 (27.3) | 10 (28.6) | |
| 2 | 6 (46.2) | 12 (54.5) | 18 (51.4) | |
| 3 | 3 (23.1) | 4 (18.2) | 7 (20.0) | |
| NYHA class, n (%) | 0.203 | |||
| 1 | 3 (4.3) | 4 (5.4) | 7 (4.9) | |
| 2 | 30 (43.5) | 42 (56.8) | 72 (50.3) | |
| 3 | 36 (52.2) | 27 (36.5) | 63 (44.1) | |
| 4 | 0 (0.0) | 1 (1.4) | 1 (0.7) | |
| Aortic valve surgery, n (%) | 51 (69.9) | 61 (76.3) | 112 (73.2) | 0.465 |
| Mitral valve surgery, n (%) | 41 (56.2) | 38 (46.9) | 79 (51.3) | 0.263 |
| Tricuspid surgery, n (%) | 15 (20.5) | 14 (17.3) | 29 (18.8) | 0.682 |
| CABG, n (%) | 48 (65.8) | 61 (75.3) | 109 (70.8) | 0.217 |
| CPB time, minutes (median, Q1–Q3) | 109.0 (89.0–132.0) | 102.5 (80.0–133.5) | 106.0 (86.0–132.5) | 0.252 |
| Days to discharge (median, Q1–Q3) | 11.5 (7.0–19.0) | 13.5 (7.0–21.0) | 12.5 (7.0–20.5) | 0.500 |
| Inspire | RemoweLL 2 | p | |
|---|---|---|---|
| n | 73 | 81 | |
| Positive CAM out of total administered CAM | 7.2% (70/971) | 5.9% (64/1080) | 0.257 |
| Patients with ≥1 positive CAM | 32.9% (24/73) | 34.6% (28/81) | 0.480 |
| Patients with ≥4 positive CAM | 12.3% (9/73) | 6.2% (5/81) | 0.148 |
| Visits with delirium therapy out of total visits | 3.7% (46/1240) | 2.9% (40/1364) | 0.277 |
| Patients with delirium therapy at discharge | 11.0% (8/73) | 6.2% (5/81) | 0.219 |
| Patients with severe delirium, defined as: ≥4 positive CAM (>24 h) and/or delirium therapy in hospital/at discharge | 26.0% (19/73) | 16.0% (13/81) | 0.093 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantovani, L.; Mikus, E.; Tenti, E.; Sangiorgi, D.; Zannoni, S.; Cavallucci, A.; Ferroni, L.; Cimaglia, P.; Tolio, V.; Tremoli, E.; et al. Post-Operative Delirium and Cognitive Dysfunction in Aged Patients Undergoing Cardiac Surgery: A Randomized Comparison between Two Blood Oxygenators. Bioengineering 2023, 10, 1429. https://doi.org/10.3390/bioengineering10121429
Mantovani L, Mikus E, Tenti E, Sangiorgi D, Zannoni S, Cavallucci A, Ferroni L, Cimaglia P, Tolio V, Tremoli E, et al. Post-Operative Delirium and Cognitive Dysfunction in Aged Patients Undergoing Cardiac Surgery: A Randomized Comparison between Two Blood Oxygenators. Bioengineering. 2023; 10(12):1429. https://doi.org/10.3390/bioengineering10121429
Chicago/Turabian StyleMantovani, Lorenzo, Elisa Mikus, Elena Tenti, Diego Sangiorgi, Samantha Zannoni, Andrea Cavallucci, Letizia Ferroni, Paolo Cimaglia, Valentina Tolio, Elena Tremoli, and et al. 2023. "Post-Operative Delirium and Cognitive Dysfunction in Aged Patients Undergoing Cardiac Surgery: A Randomized Comparison between Two Blood Oxygenators" Bioengineering 10, no. 12: 1429. https://doi.org/10.3390/bioengineering10121429
APA StyleMantovani, L., Mikus, E., Tenti, E., Sangiorgi, D., Zannoni, S., Cavallucci, A., Ferroni, L., Cimaglia, P., Tolio, V., Tremoli, E., & Savini, C. (2023). Post-Operative Delirium and Cognitive Dysfunction in Aged Patients Undergoing Cardiac Surgery: A Randomized Comparison between Two Blood Oxygenators. Bioengineering, 10(12), 1429. https://doi.org/10.3390/bioengineering10121429