

Radiomics Prediction of Muscle Invasion in Bladder Cancer Using Semi-Automatic Lesion Segmentation of MRI Compared with Manual Segmentation

Abstract
:1. Introduction
2. Materials and Methods
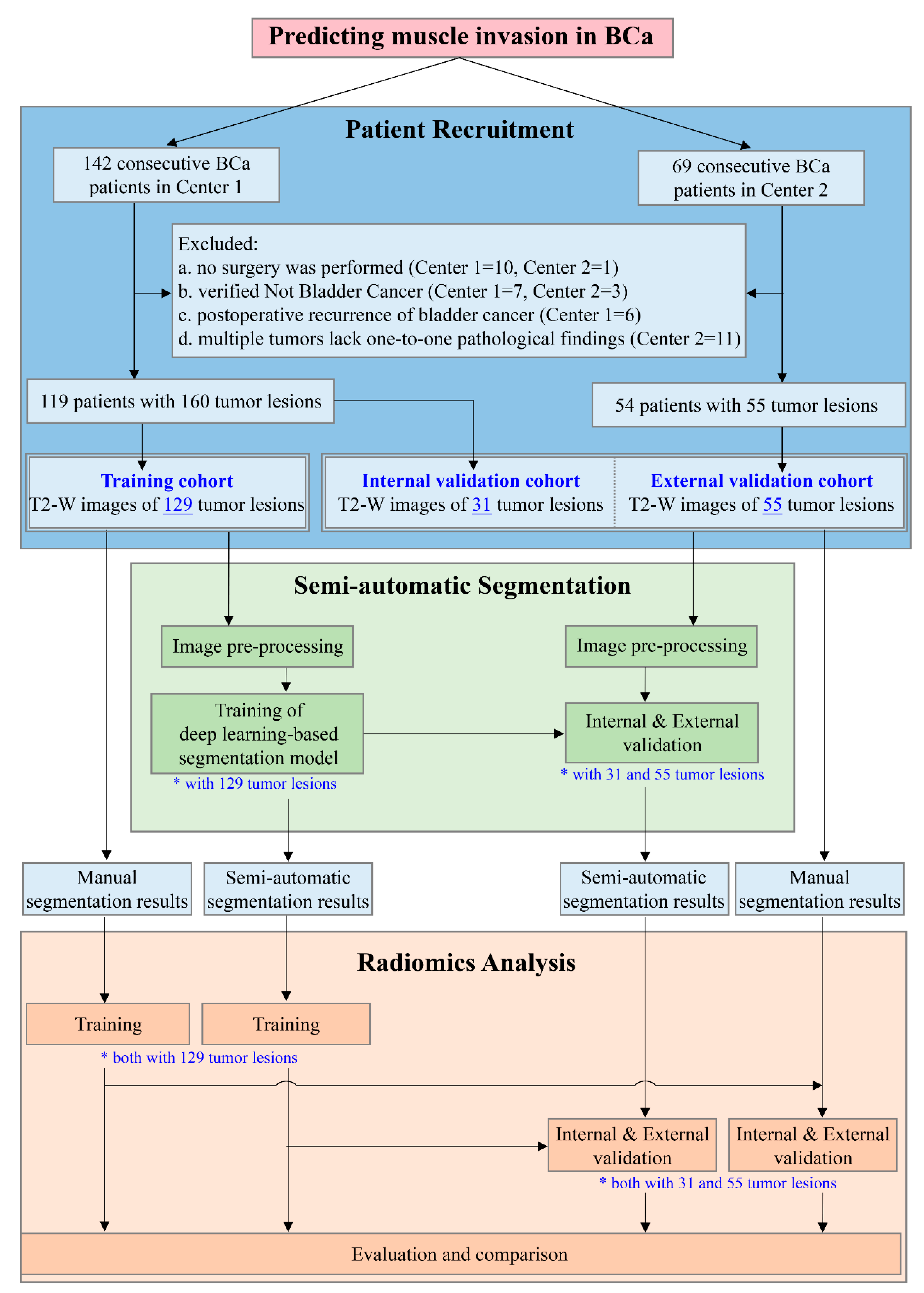
2.1. Patients and Study Design
2.2. The Development and Validation of the Deep Learning-Based Semi-Automatic Segmentation Model
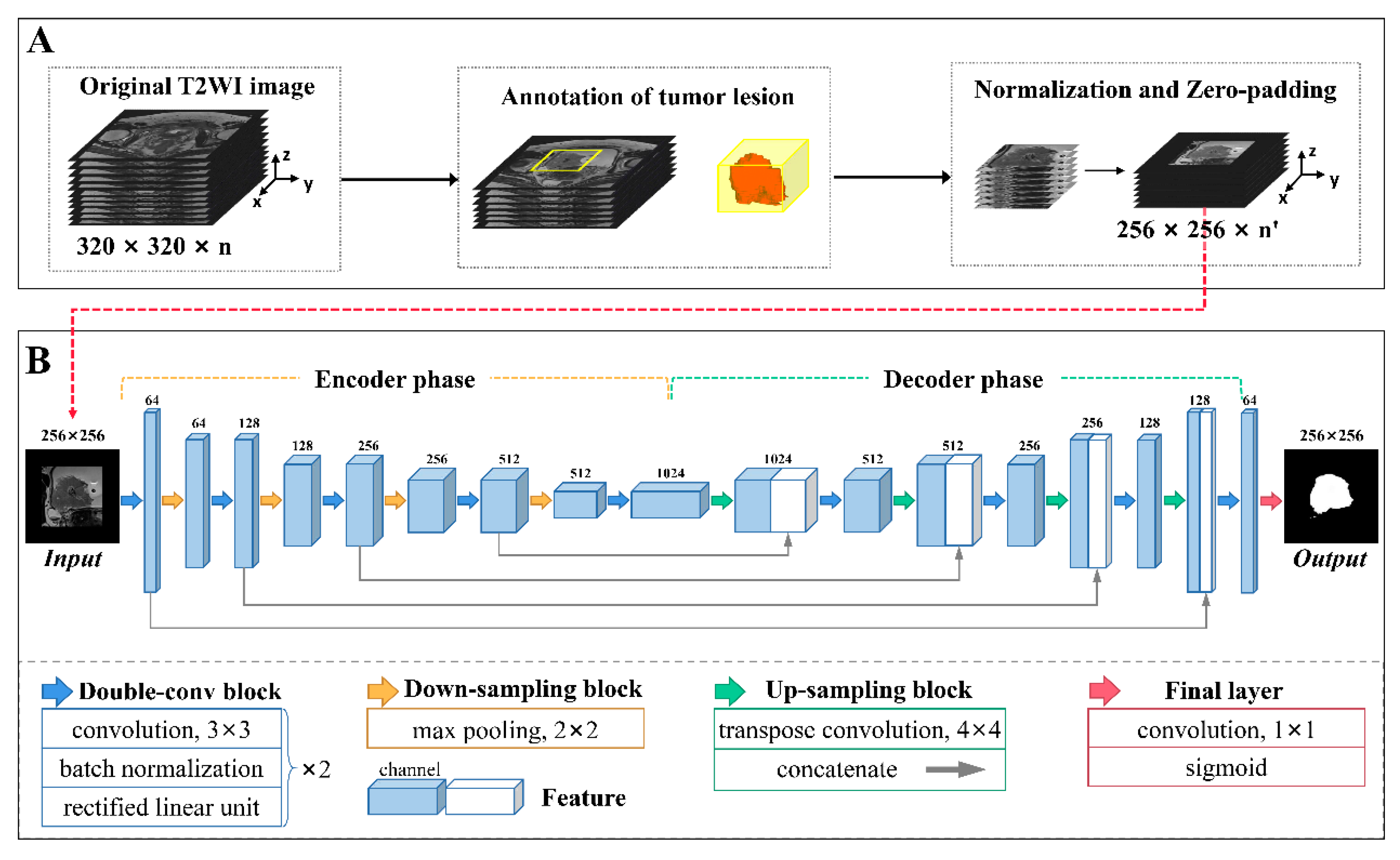
2.2.1. Image Preprocessing
2.2.2. Network Architecture
2.2.3. The Development and Validation of the Semi-Automatic Segmentation Model
2.3. The Development and Validation of the Radiomics Model Based on Semi-Automatic Segmentation Results
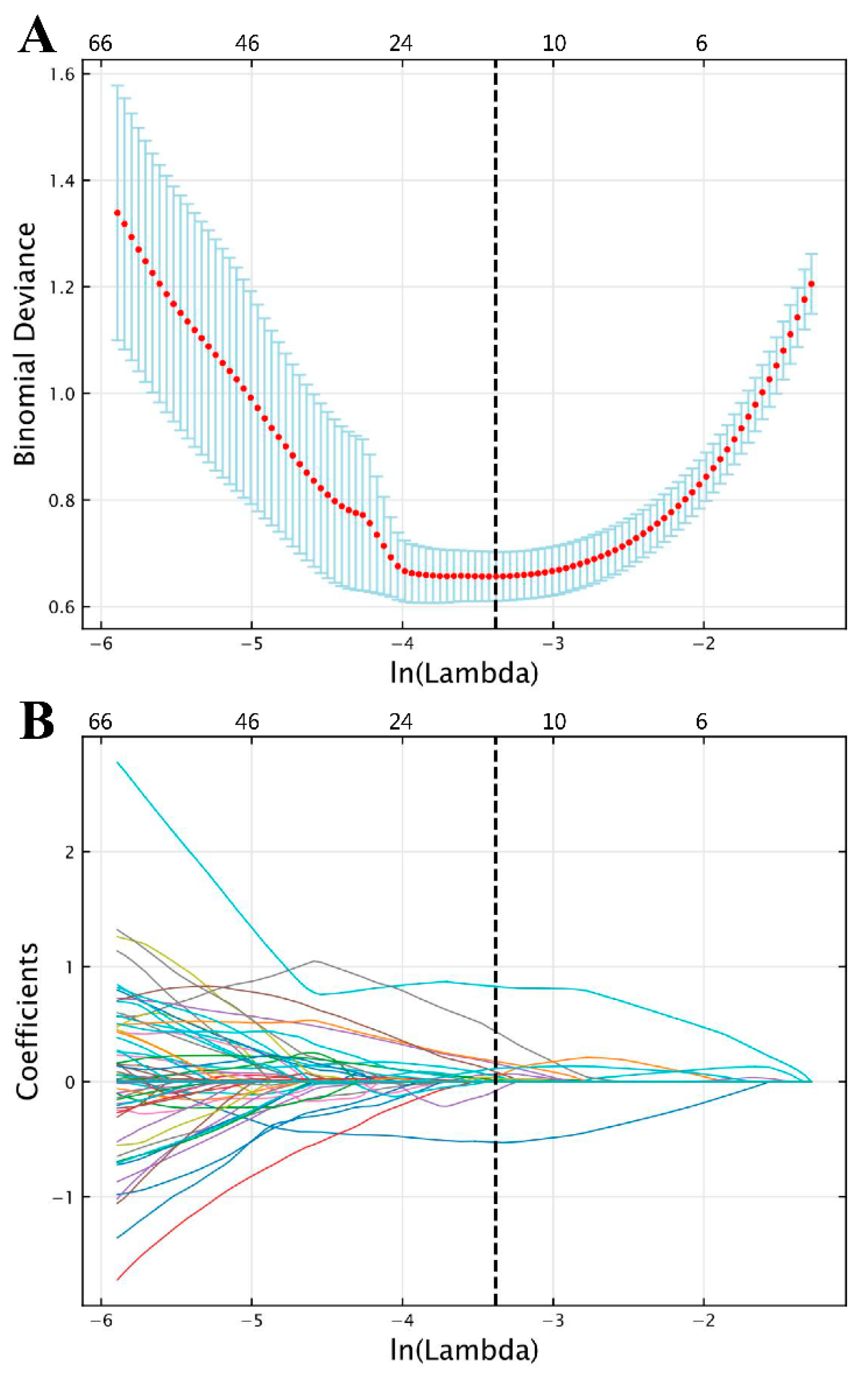
2.3.1. Feature Extraction and Selection
2.3.2. The Development and Validation of the Radiomics Model
2.4. The Development and Validation of the Radiomics Model Based on Manual Segmentation Results
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Performance Evaluation of the Deep Learning-Based Semi-Automatic Segmentation Model
3.3. Performance Evaluation of the Radiomics Model Based on Semi-Automatic Segmentation Results
3.3.1. Radiomics Feature Selection
3.3.2. Classification Performance in the Validation Cohorts
3.4. Comparison of the Radiomics Models Based on Different Segmentation Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Powles, T.; Bellmunt, J.; Comperat, E.; De Santis, M.; Huddart, R.; Loriot, Y.; Necchi, A.; Valderrama, B.P.; Ravaud, A.; Shariat, S.F.; et al. Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 244–258. [Google Scholar] [CrossRef]
- Lenis, A.T.; Lec, P.M.; Chamie, K.; Mshs, M.D. Bladder Cancer: A Review. JAMA 2020, 324, 1980–1991. [Google Scholar] [CrossRef]
- Magers, M.J.; Lopez-Beltran, A.; Montironi, R.; Williamson, S.R.; Kaimakliotis, H.Z.; Cheng, L. Staging of bladder cancer. Histopathology 2019, 74, 112–134. [Google Scholar] [CrossRef]
- Knowles, M.A.; Hurst, C.D. Molecular biology of bladder cancer: New insights into pathogenesis and clinical diversity. Nat. Rev. Cancer 2014, 15, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Comperat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Comperat, E.M.; Cowan, N.C.; Gakis, G.; Hernandez, V.; Linares Espinos, E.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef]
- Cumberbatch, M.G.K.; Foerster, B.; Catto, J.W.F.; Kamat, A.M.; Kassouf, W.; Jubber, I.; Shariat, S.F.; Sylvester, R.J.; Gontero, P. Repeat Transurethral Resection in Non-muscle-invasive Bladder Cancer: A Systematic Review. Eur. Urol. 2018, 73, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Engilbertsson, H.; Aaltonen, K.E.; Bjornsson, S.; Kristmundsson, T.; Patschan, O.; Ryden, L.; Gudjonsson, S. Transurethral bladder tumor resection can cause seeding of cancer cells into the bloodstream. J. Urol. 2015, 193, 53–57. [Google Scholar] [CrossRef]
- Panebianco, V.; De Berardinis, E.; Barchetti, G.; Simone, G.; Leonardo, C.; Grompone, M.D.; Del Monte, M.; Carano, D.; Gallucci, M.; Catto, J.; et al. An evaluation of morphological and functional multi-parametric MRI sequences in classifying non-muscle and muscle invasive bladder cancer. Eur. Radiol. 2017, 27, 3759–3766. [Google Scholar] [CrossRef]
- van der Pol, C.B.; Chung, A.; Lim, C.; Gandhi, N.; Tu, W.; McInnes, M.D.F.; Schieda, N. Update on multiparametric MRI of urinary bladder cancer. J. Magn. Reson. Imaging 2018, 48, 882–896. [Google Scholar] [CrossRef]
- Huang, B.; Lin, X.; Shen, J.; Chen, X.; Chen, J.; Li, Z.P.; Wang, M.; Yuan, C.; Diao, X.F.; Luo, Y.; et al. Accurate and Feasible Deep Learning Based Semi-Automatic Segmentation in CT for Radiomics Analysis in Pancreatic Neuroendocrine Neoplasms. IEEE J. Biomed. Health Inform. 2021, 25, 3498–3506. [Google Scholar] [CrossRef]
- Zheng, Z.; Xu, F.; Gu, Z.; Yan, Y.; Xu, T.; Liu, S.; Yao, X. Combining Multiparametric MRI Radiomics Signature With the Vesical Imaging-Reporting and Data System (VI-RADS) Score to Preoperatively Differentiate Muscle Invasion of Bladder Cancer. Front. Oncol. 2021, 11, 619893. [Google Scholar] [CrossRef]
- Li, J.; Cao, K.; Lin, H.; Deng, L.; Yang, S.; Gao, Y.; Liang, M.; Lin, C.; Zhang, W.; Xie, C.; et al. Predicting muscle invasion in bladder cancer by deep learning analysis of MRI: Comparison with vesical imaging-reporting and data system. Eur. Radiol. 2023, 33, 2699–2709. [Google Scholar] [CrossRef]
- Xu, X.; Liu, Y.; Zhang, X.; Tian, Q.; Wu, Y.; Zhang, G.; Meng, J.; Yang, Z.; Lu, H. Preoperative prediction of muscular invasiveness of bladder cancer with radiomic features on conventional MRI and its high-order derivative maps. Abdom. Radiol. 2017, 42, 1896–1905. [Google Scholar] [CrossRef]
- Wang, H.; Hu, D.; Yao, H.; Chen, M.; Li, S.; Chen, H.; Luo, J.; Feng, Y.; Guo, Y. Radiomics analysis of multiparametric MRI for the preoperative evaluation of pathological grade in bladder cancer tumors. Eur. Radiol. 2019, 29, 6182–6190. [Google Scholar] [CrossRef]
- Choi, S.J.; Park, K.J.; Heo, C.; Park, B.W.; Kim, M.; Kim, J.K. Radiomics-based model for predicting pathological complete response to neoadjuvant chemotherapy in muscle-invasive bladder cancer. Clin. Radiol. 2021, 76, 627.e13–627.e21. [Google Scholar] [CrossRef]
- Ramtohul, T.; Djerroudi, L.; Lissavalid, E.; Nhy, C.; Redon, L.; Ikni, L.; Djelouah, M.; Journo, G.; Menet, E.; Cabel, L.; et al. Multiparametric MRI and Radiomics for the Prediction of HER2-Zero, -Low, and -Positive Breast Cancers. Radiology 2023, 308, e222646. [Google Scholar] [CrossRef]
- Fan, X.; Li, J.; Huang, B.; Lu, H.; Lu, C.; Pan, M.; Wang, X.; Zhang, H.; You, Y.; Wang, X.; et al. Noninvasive radiomics model reveals macrophage infiltration in glioma. Cancer Lett. 2023, 573, 216380. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Jian, J.; Li, Y.; Gao, X. Deep learning-based segmentation of epithelial ovarian cancer on T2-weighted magnetic resonance images. Quant. Imaging Med. Surg. 2023, 13, 1464–1477. [Google Scholar] [CrossRef]
- Ren, H.; Ren, C.; Guo, Z.; Zhang, G.; Luo, X.; Ren, Z.; Tian, H.; Li, W.; Yuan, H.; Hao, L.; et al. A novel approach for automatic segmentation of prostate and its lesion regions on magnetic resonance imaging. Front. Oncol. 2023, 13, 1095353. [Google Scholar] [CrossRef] [PubMed]
- Rani, G.; Thakkar, P.; Verma, A.; Mehta, V.; Chavan, R.; Dhaka, V.S.; Sharma, R.K.; Vocaturo, E.; Zumpano, E. KUB-UNet: Segmentation of Organs of Urinary System from a KUB X-ray Image. Comput. Methods Programs Biomed. 2022, 224, 107031. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Li, J.; Fan, H.; Fan, L. TGDAUNet: Transformer and GCNN based dual-branch attention UNet for medical image segmentation. Comput. Biol. Med. 2023, 167, 107583. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Du, B.; Yan, P.; Lu, H.; Zhang, L. Shape prior constrained PSO model for bladder wall MRI segmentation. Neurocomputing 2018, 294, 19–28. [Google Scholar] [CrossRef]
- Hammouda, K.; Khalifa, F.; Soliman, A.; Ghazal, M.; El-Ghar, M.A.; Badawy, M.A.; Darwish, H.E.; Khelifi, A.; El-Baz, A. A multiparametric MRI-based CAD system for accurate diagnosis of bladder cancer staging. Comput. Med. Imaging Graph. 2021, 90, 101911. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Feng, N.; Pu, H.; Dong, Q.; Liu, Y.; Liu, Y.; Xu, X. PIxel-Level Segmentation of Bladder Tumors on MR Images Using a Random Forest Classifier. Technol. Cancer Res. Treat. 2022, 21, 15330338221086395. [Google Scholar] [CrossRef] [PubMed]
- Coroama, D.M.; Diosan, L.; Telecan, T.; Andras, I.; Crisan, N.; Medan, P.; Andreica, A.; Caraiani, C.; Lebovici, A.; Boca, B.; et al. Fully automated bladder tumor segmentation from T2 MRI images using 3D U-Net algorithm. Front. Oncol. 2023, 13, 1096136. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Medical Image Computing and Computer-Assisted Intervention—MICCAI 2015; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Lin, T.Y.; Goyal, P.; Girshick, R.; He, K.; Dollar, P. Focal Loss for Dense Object Detection. IEEE Trans. Pattern Anal. Mach. Intell. 2020, 42, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Milletari, F.; Navab, N.; Ahmadi, S.-A. V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–26 October 2016; pp. 565–571. [Google Scholar]
- Kingma, D.P.; Ba, J.L. ADAM: A method for stochastic optimization. In Proceedings of the 3rd International Conference for Learning Representations, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Cortes, C.; Vapnik, V. Support-vector network. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Chang, C.-C.; Lin, C.-J. Libsvm: A Library for Support Vector Machines. ACM Trans. Intell. Syst. Technol. 2011, 2, 1–27. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Obuchowski, N.A. ROC analysis. Am. J. Roentgenol. 2005, 184, 364–372. [Google Scholar] [CrossRef]
- Dercle, L.; Fronheiser, M.; Lu, L.; Du, S.; Hayes, W.; Leung, D.K.; Roy, A.; Wilkerson, J.; Guo, P.; Fojo, A.T.; et al. Identification of Non-Small Cell Lung Cancer Sensitive to Systemic Cancer Therapies Using Radiomics. Clin. Cancer Res. 2020, 26, 2151–2162. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Park, S.H.; Lee, K.H. How to demonstrate similarity by using noninferiority and equivalence statistical testing in radiology research. Radiology 2013, 267, 328–338. [Google Scholar] [CrossRef]
- XH, Z.; NA, O.; DK, M. Statistical Methods in Diagnostic Medicine, 2nd ed.; Wiley: New York, NY, USA, 2002; pp. 188–192. [Google Scholar]
- Dong, Q.; Huang, D.; Xu, X.; Li, Z.; Liu, Y.; Lu, H.; Liu, Y. Content and shape attention network for bladder wall and cancer segmentation in MRIs. Comput. Biol. Med. 2022, 148, 105809. [Google Scholar] [CrossRef]
- Moribata, Y.; Kurata, Y.; Nishio, M.; Kido, A.; Otani, S.; Himoto, Y.; Nishio, N.; Furuta, A.; Onishi, H.; Masui, K.; et al. Automatic segmentation of bladder cancer on MRI using a convolutional neural network and reproducibility of radiomics features: A two-center study. Sci. Rep. 2023, 13, 628. [Google Scholar] [CrossRef]
- Ge, R.; Cai, H.; Yuan, X.; Qin, F.; Huang, Y.; Wang, P.; Lyu, L. MD-UNET: Multi-input dilated U-shape neural network for segmentation of bladder cancer. Comput. Biol. Chem. 2021, 93, 107510. [Google Scholar] [CrossRef]
- Brown, A.L.; Jeong, J.; Wahab, R.A.; Zhang, B.; Mahoney, M.C. Diagnostic accuracy of MRI textural analysis in the classification of breast tumors. Clin. Imaging 2021, 77, 86–91. [Google Scholar] [CrossRef]
- Agazzi, G.M.; Ravanelli, M.; Roca, E.; Medicina, D.; Balzarini, P.; Pessina, C.; Vermi, W.; Berruti, A.; Maroldi, R.; Farina, D. CT texture analysis for prediction of EGFR mutational status and ALK rearrangement in patients with non-small cell lung cancer. La Radiol. Medica 2021, 126, 786–794. [Google Scholar] [CrossRef]
- Lafci, O.; Celepli, P.; Seher Oztekin, P.; Kosar, P.N. DCE-MRI Radiomics Analysis in Differentiating Luminal A and Luminal B Breast Cancer Molecular Subtypes. Acad. Radiol. 2023, 30, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zheng, H.; Xu, X.; Zhang, X.; Du, P.; Liang, J.; Lu, H. The invasion depth measurement of bladder cancer using T2-weighted magnetic resonance imaging. Biomed. Eng. Online 2020, 19, 92. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Training Cohort | Internal Validation Cohort | External Validation Cohort | ||
|---|---|---|---|---|---|
| Center 1 | Center 1 | p | Center 2 | p | |
| Number, n | 129 | 31 | - | 55 | - |
| Age (years) | 0.553 † | 0.244 † | |||
| Median (IQR) | 67 (59, 75) | 69 (62, 71) | 64 (55, 73) | ||
| Sex | 0.561 ‡ | 0.869 ‡ | |||
| Male | 109 | 31 | 47 | ||
| Female | 20 | 0 | 8 | ||
| MRI-determined tumor size (cm) | 0.892 † | <0.001 † | |||
| <3 | 100 | 25 | 12 | ||
| ≥3 | 29 | 6 | 43 | ||
| Pathological T stage | - | - | |||
| Ta | 75 | 23 | 20 | ||
| T1 | 28 | 4 | 3 | ||
| T2 | 15 | 2 | 15 | ||
| T3 | 4 | 2 | 13 | ||
| T4 | 7 | 0 | 4 | ||
| Pathological grade | - | - | |||
| Low | 51 | 16 | 10 | ||
| High | 78 | 15 | 45 | ||
| Degree of infiltration | - | - | |||
| NMIBC | 103 | 27 | 23 | ||
| MIBC | 26 | 4 | 32 | ||
| Dataset | DSC | Recall | Precision | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | Range | Mean ± SD | Median | Mean ± SD | Median | |
| Internal Validation Cohort (n = 31 †) | 0.836 ± 0.085 | 0.861 | 0.558–0.921 | 0.803 ± 0.115 | 0.845 | 0.885 ± 0.072 | 0.900 |
| External Validation Cohort (n = 55 †) | 0.801 ± 0.112 | 0.841 | 0.525–0.951 | 0.782 ± 0.119 | 0.821 | 0.838 ± 0.140 | 0.880 |
| Feature Name | Coefficient | Training Cohort | Internal Validation Cohort | External Validation Cohort | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NMIBC | MIBC | p * | NMIBC | MIBC | p * | NMIBC | MIBC | p * | ||
| original_firstorder_Kurtosis | 0.129 | −0.398 (−0.637, 0.060) | 0.763 (−0.085, 1.974) | <0.001 | −0.411 (−0.628, −0.245) | 1.787 (1.125, 3.313) | <0.001 | −0.027 (−0.422, 0.235) | 0.730 (0.037, 1.370) | <0.001 |
| original_shape_Sphericity | −0.077 | 0.307 (−0.219, 0.805) | −0.471 (−1.195, −0.085) | <0.001 | 0.439 (−0.492, 0.704) | −1.366 (−1.619, −1.109) | 0.005 | −0.340 (−1.106, 0.168) | −2.318 (−3.933, −1.116) | <0.001 |
| original_firstorder_Skewness | 0.048 | −0.232 (−0.842, 0.201) | 1.316 (0.389, 1.834) | <0.001 | 0.037 (−0.670, 0.363) | 1.962 (1.403, 2.433) | <0.001 | −0.179 (−0.698, 0.317) | 0.877 (0.149, 1.196) | <0.001 |
| log-sigma-5-0-mm-3D_gldm_LargeDependenceHighGrayLevelEmphasis | 0.032 | −0.512 (−0.697, −0.011) | 0.667 (−0.086, 2.005) | <0.001 | −0.273 (−0.450, −0.109) | 1.781 (1.354, 3.022) | <0.001 | 0.298 (0.019, 1.243) | 1.933 (1.049, 4.171) | <0.001 |
| log-sigma-1-0-mm-3D_ firstorder_Skewness | 0.028 | −0.105 (−0.590, 0.630) | −0.123 (−0.669, 0.426) | 0.787 | 0.071 (−0.700, 0.377) | −0.112 (−0.912, 0.072) | 0.589 | −0.439 (−1.075, −0.100) | 0.351 (−0.120, 1.177) | <0.001 |
| wavelet-LLL_firstorder_ Skewness | 0.020 | −0.310 (0.751, 0.265) | 1.247 (0.442, 1.837) | <0.001 | 0.002 (−0.538, 0.243) | 1.860 (1.210, 2.433) | <0.001 | −0.199 (−0.588, 0.070) | 0.787 (0.107, 1.205) | <0.001 |
| log-sigma-1-0-mm-3D_glcm_ClusterShade | 0.014 | 0.110 (−0.076, 0.159) | 0.151 (0.066, 0.188) | 0.040 | 0.121 (−0.304, 0.180) | 0.146 (0.034, 0.245) | 0.589 | −0.136 (−0.633, 0.091) | 0.247 (0.139, 0.584) | <0.001 |
| wavelet-HHL_glcm_MCC | −0.009 | −0.222 (−0.687, 0.531) | −0.514 (−0.826, 0.292) | 0.080 | −0.223 (−0.496, 0.636) | −0.135 (−0.679, 0.702) | 0.932 | −0.260 (−0.476, 0.431) | −0.446 (−0.623, 0.011) | 0.091 |
| original_shape_ MinorAxisLength | 0.007 | −0.453 (−0.750, 0.027) | 0.451 (0.044, 1.915) | <0.001 | −0.285 (−0.593, −0.056) | 1.591 (0.778, 2.108) | <0.001 | 0.075 (−0.524, 0.408) | 1.181 (0.483, 1.992) | <0.001 |
| wavelet-HLH_glszm_ GrayLevelNonUniformity | 0.004 | −0.364 (−0.403, 0.205) | −0.097 (−0.230, 0.580) | <0.001 | −0.310 (−0.373, −0.227) | 1.165 (0.444, 2.328) | <0.001 | 0.111 (−0.281, 0.698) | 1.636 (0.749, 4.001) | <0.001 |
| log-sigma-5-0-mm-3D_gldm_DependenceNonUniformity | 0.002 | −0.394 (−0.452, −0.267) | −0.043 (−0.268, 1.126) | <0.001 | −0.379 (−0.433, −0.245) | 0.972 (0.260, 2.074) | <0.001 | 0.183 (−0.329, 0.717) | 1.829 (0.448, 4.083) | <0.001 |
| log-sigma-5-0-mm-3D_glszm_SmallAreaEmphasis | 0.002 | −0.248 (−1.035, 0.377) | 0.659 (0.357, 1.002) | <0.001 | −0.294 (−0.898, 0.863) | 1.079 (0.832, 1.310) | 0.039 | 0.094 (−0.238, 0.450) | 0.630 (0.283, 0.984) | 0.001 |
| Dataset | Segmentation Method | Accuracy | Sensitivity | Specificity | AUC (95% CI) | AUC Difference (95% CI) | p | |
|---|---|---|---|---|---|---|---|---|
| Internal validation cohort (MIBC/NMIBC = 4/27) | Semi-automatic | 1.000 | 1.000 | 1.000 | 1.000 (0.888–1.000) | 0.009 (−0.016–0.035) | <0.001 † | 0.480 ‡ |
| Manual | 0.968 | 1.000 | 0.963 | 0.991 (0.871–1.000) | <0.001 † | |||
| External validation cohort (MIBC/NMIBC = 32/23) | Semi-automatic | 0.818 | 0.750 | 0.913 | 0.892 (0.779–0.960) | 0.002 (−0.044–0.048) | <0.001 † | 0.930 ‡ |
| Manual | 0.800 | 0.750 | 0.870 | 0.894 (0.781–0.961) | <0.001 † | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, Y.; Luo, Z.; Qiu, Z.; Cao, K.; Huang, B.; Deng, L.; Zhang, W.; Liu, G.; Zou, Y.; Zhang, J.; et al. Radiomics Prediction of Muscle Invasion in Bladder Cancer Using Semi-Automatic Lesion Segmentation of MRI Compared with Manual Segmentation. Bioengineering 2023, 10, 1355. https://doi.org/10.3390/bioengineering10121355
Ye Y, Luo Z, Qiu Z, Cao K, Huang B, Deng L, Zhang W, Liu G, Zou Y, Zhang J, et al. Radiomics Prediction of Muscle Invasion in Bladder Cancer Using Semi-Automatic Lesion Segmentation of MRI Compared with Manual Segmentation. Bioengineering. 2023; 10(12):1355. https://doi.org/10.3390/bioengineering10121355
Chicago/Turabian StyleYe, Yaojiang, Zixin Luo, Zhengxuan Qiu, Kangyang Cao, Bingsheng Huang, Lei Deng, Weijing Zhang, Guoqing Liu, Yujian Zou, Jian Zhang, and et al. 2023. "Radiomics Prediction of Muscle Invasion in Bladder Cancer Using Semi-Automatic Lesion Segmentation of MRI Compared with Manual Segmentation" Bioengineering 10, no. 12: 1355. https://doi.org/10.3390/bioengineering10121355
APA StyleYe, Y., Luo, Z., Qiu, Z., Cao, K., Huang, B., Deng, L., Zhang, W., Liu, G., Zou, Y., Zhang, J., & Li, J. (2023). Radiomics Prediction of Muscle Invasion in Bladder Cancer Using Semi-Automatic Lesion Segmentation of MRI Compared with Manual Segmentation. Bioengineering, 10(12), 1355. https://doi.org/10.3390/bioengineering10121355