

Artificial Intelligence Algorithms for Benign vs. Malignant Dermoscopic Skin Lesion Image Classification
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
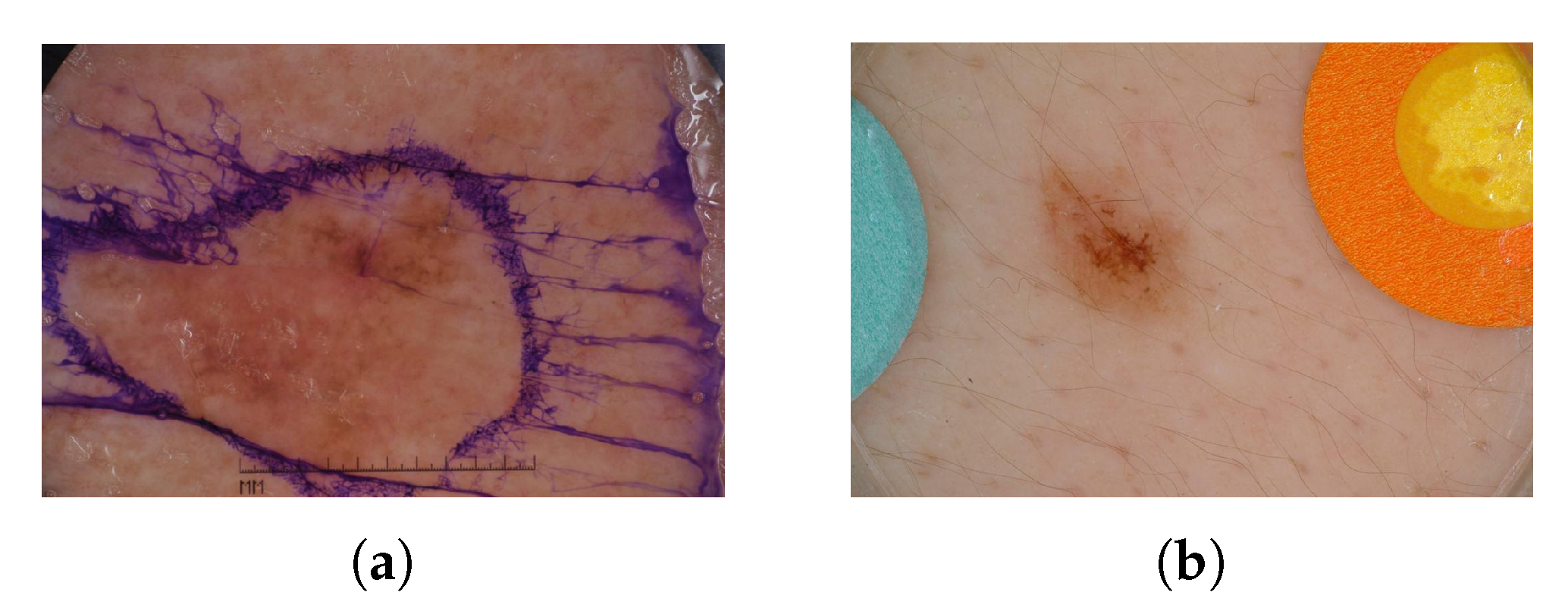
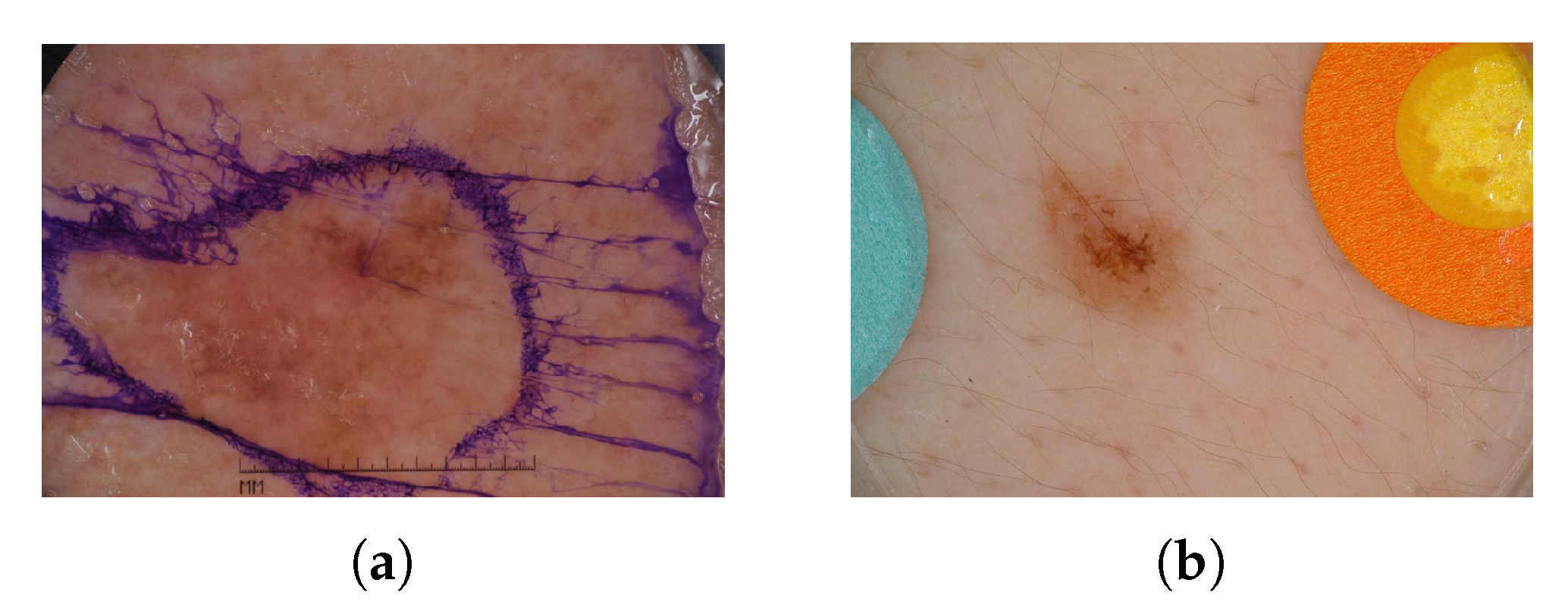
2.1. Dataset
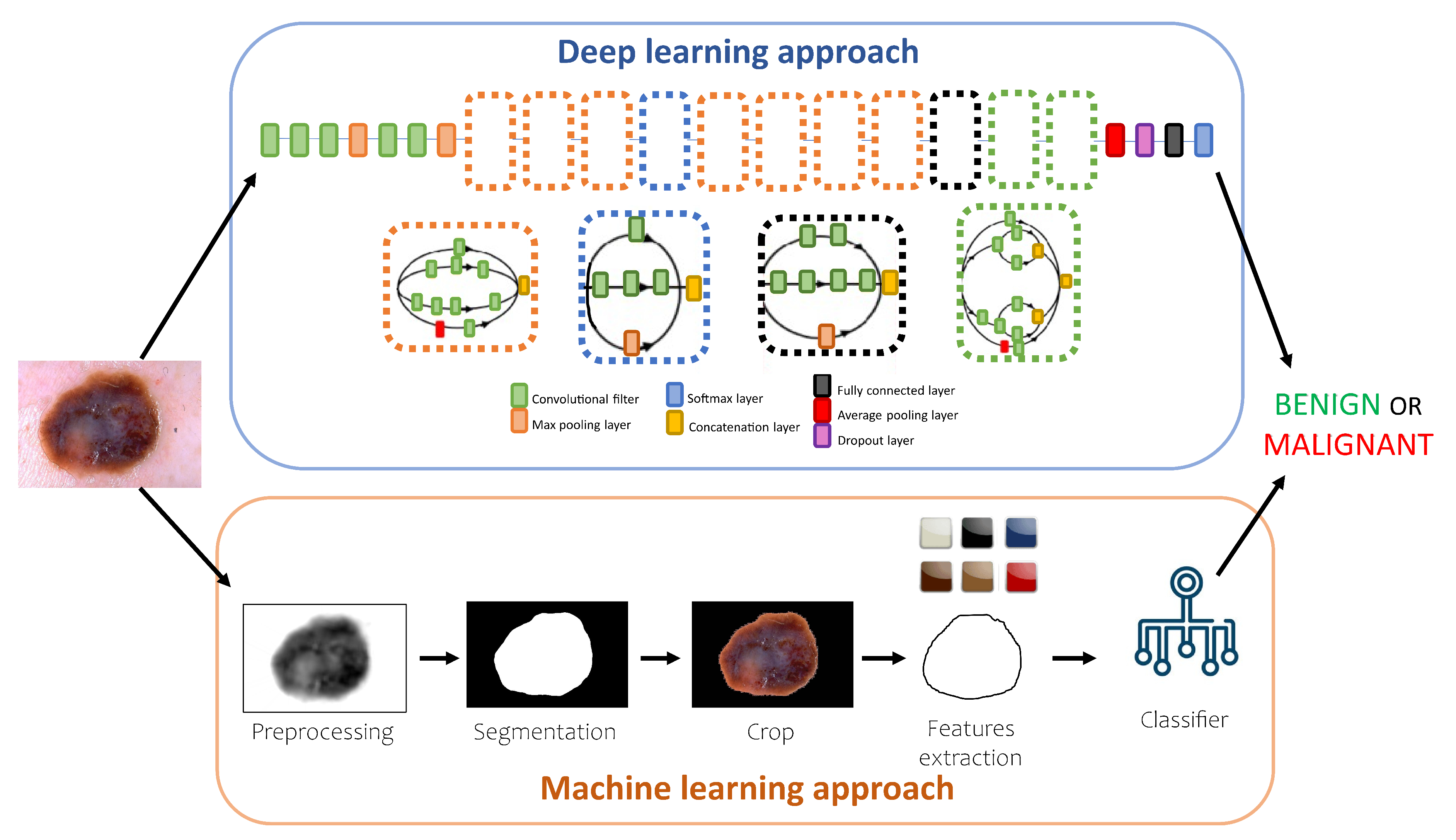
2.2. Machine Learning Approach
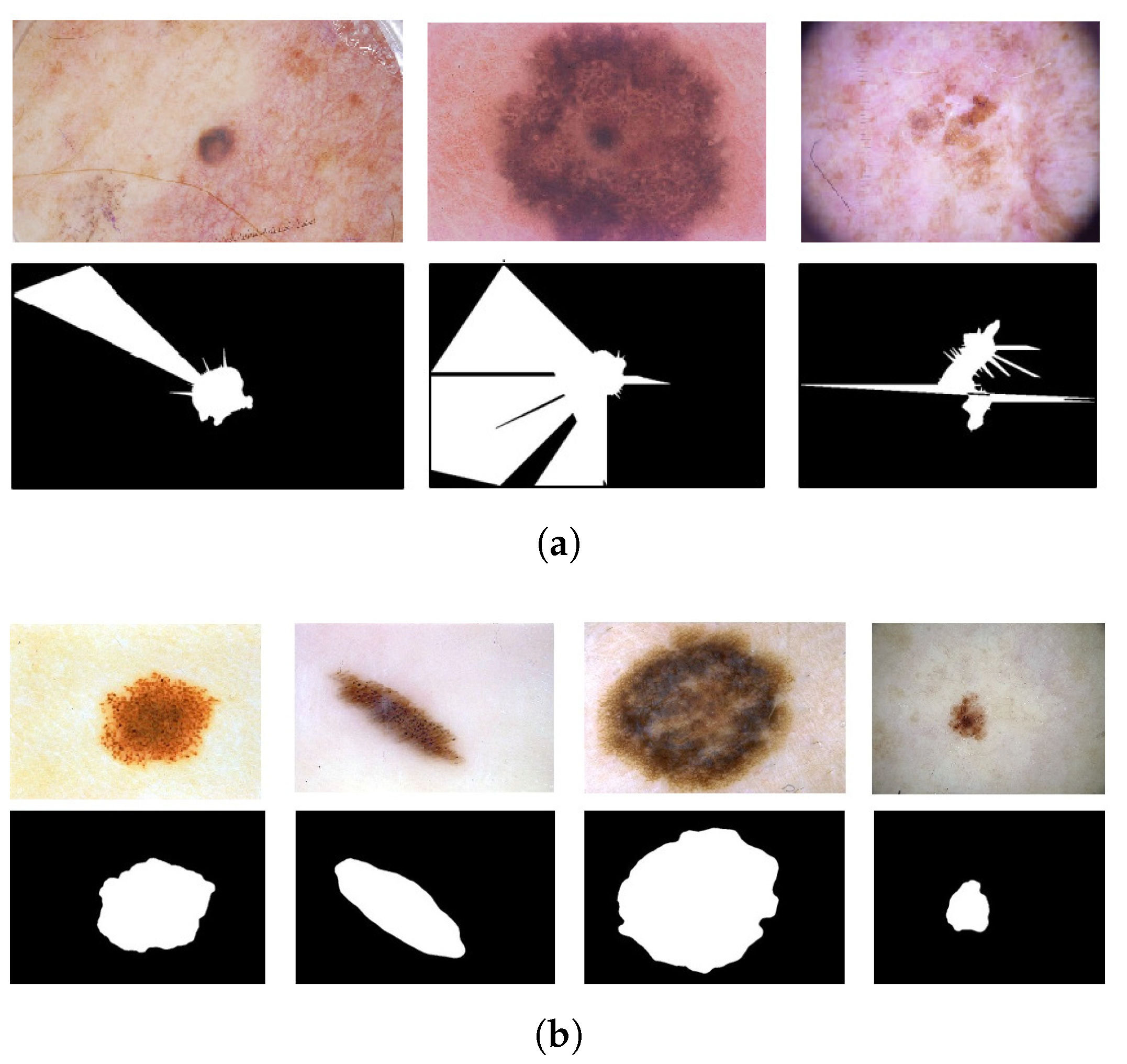
2.2.1. Preprocessing and Segmentation
2.2.2. Feature Extraction and Classification
- Shape asymmetry.
- Border irregularity.
- Fractal dimension index.
- Compactness index.
- Color density.
- Color asymmetry index.
- Standard deviation (SD) of the color distribution.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Extracted Feature | Formula/Algorithm | Source | Output Range |
|---|---|---|---|
| Shape asymmetry | NEF | [23,26] | [0–5] |
| Border irregularity | [11] | [0–5] | |
| Fractal dimension index | Box-counting algorithm | [24] | [0–5] |
| Compactness index | [27] | [0–5] | |
| Color density | K-means + | [11] | [0–100]% |
| Color asymmetry index | Minimum Euclidean distance | [23,26] | [0–5] |
| Standard deviation (SD) of the color distribution | (White, black, red, light brown, dark brown, blue-gray) | [11] | [0–100] |
2.3. Deep Learning Approach
3. Results
3.1. Dataset
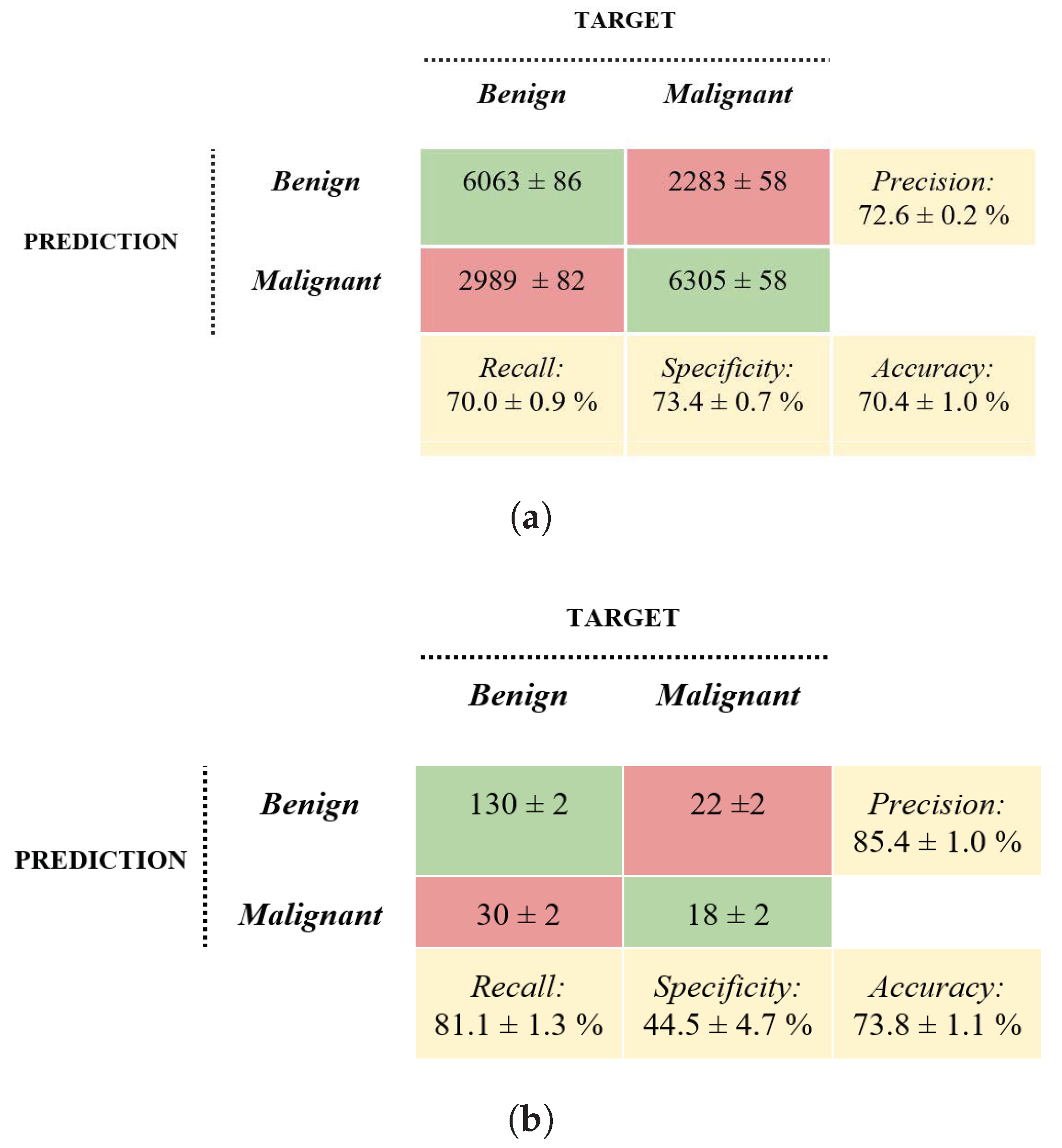
3.2. Machine Learning Approach
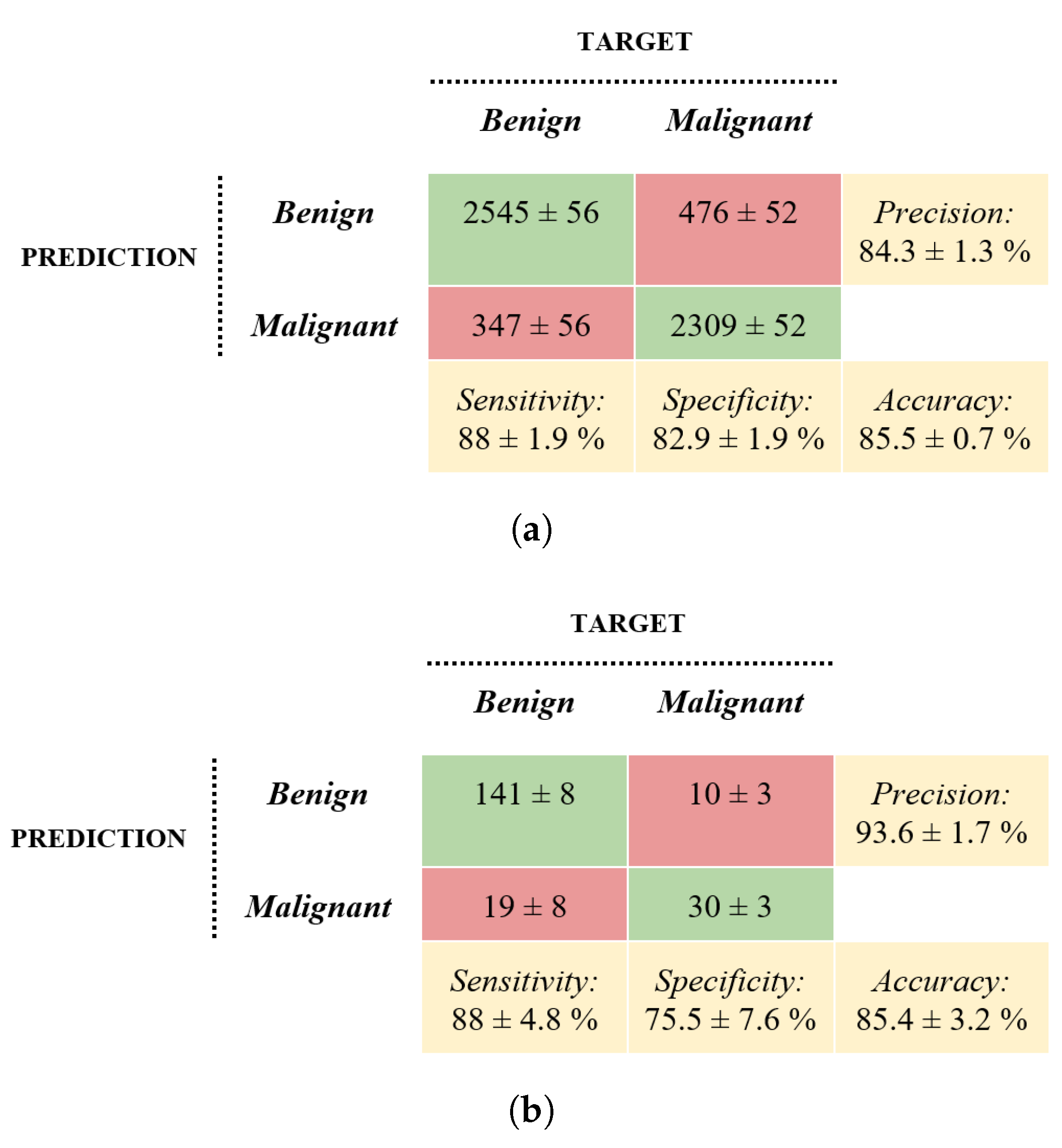
3.3. Deep Learning Approach
4. Related Works and Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| ML | Machine learning |
| DL | Deep learning |
| CNN | Convolutional neural network |
| ISIC | International Skin Imaging Collaboration |
| KNN | k-Nearest Neighbors |
| SVM | Support Vector Machine |
References
- U.S. Cancer Statistics Working Group. US Cancer Statistics Data Visualizations Tool, Based on November 2017 Submission Data (1999–2015): US Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; Centers for Disease Control and Prevention and National Cancer Institute: Atlanta, GA, USA, 2018; Volume 6. [Google Scholar]
- Tumori, A.I.R. I Numeri del Cancro in Italia 2020, Brescia, Italy. Available online: https://www.aiom.it/wp-content/uploads/2020/10/2020_Numeri_Cancro-operatori_web.pdf (accessed on 20 June 2021).
- Dzwierzynski, W.W. Melanoma Risk Factors and Prevention. Clin. Plast. Surg. 2021, 48, 543–550. [Google Scholar] [CrossRef]
- Brochez, L.; Verhaeghe, E.; Bleyen, L.; Naeyaert, J.M. Diagnostic ability of general practitioners and dermatologists in discriminating pigmented skin lesions. J. Am. Acad. Dermatol. 2001, 44, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Weber, P.; Tschandl, P.; Sinz, C.; Kittler, H. Dermatoscopy of neoplastic skin lesions: Recent advances, updates, and revisions. Curr. Treat. Options Oncol. 2018, 19, 1–17. [Google Scholar] [CrossRef]
- Thomas, L.; Puig, S. Dermoscopy, Digital Dermoscopy and Other Diagnostic Tools in the Early Detection of Melanoma and Follow-up of High-risk Skin Cancer Patients. Acta-Derm.-Venereol. 2017, 97, 14–21. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Pham, T.C.; Luong, C.M.; Hoang, V.D.; Doucet, A. AI outperformed every dermatologist in dermoscopic melanoma diagnosis, using an optimized deep-CNN architecture with custom mini-batch logic and loss function. Sci. Rep. 2021, 11, 17485. [Google Scholar] [CrossRef]
- Bechelli, S.; Delhommelle, J. Machine Learning and Deep Learning Algorithms for Skin Cancer Classification from Dermoscopic Images. Bioengineering 2022, 9, 97. [Google Scholar] [CrossRef]
- Liu, L.; Mou, L.; Zhu, X.X.; Mandal, M. Automatic skin lesion classification based on mid-level feature learning. Comput. Med. Imaging Graph. 2020, 84, 101765. [Google Scholar] [CrossRef]
- Khan, H.; Yadav, A.; Santiago, R.; Chaudhari, S. Automated Non-invasive Diagnosis of Melanoma Skin Cancer using Dermo-scopic Images. In Proceedings of the ITM Web of Conferences. EDP Sciences, Craiova, Romania, 29–31 October 2020; Volume 32, p. 03029. [Google Scholar]
- Premaladha, J.; Ravichandran, K. Novel approaches for diagnosing melanoma skin lesions through supervised and deep learning algorithms. J. Med. Syst. 2016, 40, 96. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; GholamHosseini, H.; Sinha, R.; Lindén, M. Melanoma classification using a novel deep convolutional neural network with dermoscopic images. Sensors 2022, 22, 1134. [Google Scholar] [CrossRef] [PubMed]
- Mahbod, A.; Schaefer, G.; Ellinger, I.; Ecker, R.; Pitiot, A.; Wang, C. Fusing fine-tuned deep features for skin lesion classification. Comput. Med. Imaging Graph. 2019, 71, 19–29. [Google Scholar] [CrossRef]
- Tschandl, P.; Rosendahl, C.; Kittler, H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci. Data 2018, 5, 180161. [Google Scholar] [CrossRef] [PubMed]
- Codella, N.; Rotemberg, V.; Tschandl, P.; Celebi, M.E.; Dusza, S.; Gutman, D.; Helba, B.; Kalloo, A.; Liopyris, K.; Marchetti, M.; et al. Skin lesion analysis toward melanoma detection 2018: A challenge hosted by the international skin imaging collaboration (isic). arXiv 2019, arXiv:1902.03368. [Google Scholar]
- Codella, N.C.; Gutman, D.; Celebi, M.E.; Helba, B.; Marchetti, M.A.; Dusza, S.W.; Kalloo, A.; Liopyris, K.; Mishra, N.; Kittler, H.; et al. Skin lesion analysis toward melanoma detection: A challenge at the 2017 international symposium on biomedical imaging (isbi), hosted by the international skin imaging collaboration (isic). In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), IEEE, Washington, DC, USA, 4–7 April 2018; pp. 168–172. [Google Scholar]
- Kawahara, J.; Daneshvar, S.; Argenziano, G.; Hamarneh, G. Seven-Point Checklist and Skin Lesion Classification Using Multitask Multimodal Neural Nets. IEEE J. Biomed. Health Inform. 2019, 23, 538–546. [Google Scholar] [CrossRef]
- Mendonça, T.; Ferreira, P.M.; Marques, J.S.; Marcal, A.R.; Rozeira, J. PH 2-A dermoscopic image database for research and benchmarking. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), IEEE, Osaka, Japan, 3–7 July 2013; pp. 5437–5440. [Google Scholar]
- Vandaele, R.; Nervo, G.A.; Gevaert, O. Topological image modification for object detection and topological image processing of skin lesions. Sci. Rep. 2020, 10, 21061. [Google Scholar] [CrossRef] [PubMed]
- Tralie, C.; Saul, N.; Bar-On, R. Ripser. py: A lean persistent homology library for python. J. Open Source Softw. 2018, 3, 925. [Google Scholar] [CrossRef]
- Bradski, G. The openCV library. Dr. Dobb’S J. Softw. Tools Prof. Program. 2000, 25, 120–123. [Google Scholar]
- Sancen-Plaza, A.; Santiago-Montero, R.; Sossa, H.; Perez-Pinal, F.J.; Martinez-Nolasco, J.J.; Padilla-Medina, J.A. Quantitative evaluation of binary digital region asymmetry with application to skin lesion detection. BMC Med. Inform. Decis. Mak. 2018, 18, 50. [Google Scholar] [CrossRef]
- Bhuiyan, M.A.H.; Azad, I.; Uddin, M.K. Image processing for skin cancer features extraction. Int. J. Sci. Eng. Res. 2013, 4, 1–6. [Google Scholar]
- Dalila, F.; Zohra, A.; Reda, K.; Hocine, C. Segmentation and classification of melanoma and benign skin lesions. Optik 2017, 140, 749–761. [Google Scholar] [CrossRef]
- Santiago-Montero, R.; López-Morales, M.; Sossa, J. Digital shape compactness measure by means of perimeter ratios. Electron. Lett. 2014, 50, 171–173. [Google Scholar] [CrossRef]
- Golston, J.E.; Stoecker, W.V.; Moss, R.H.; Dhillon, I.P. Automatic detection of irregular borders in melanoma and other skin tumors. Comput. Med. Imaging Graph. 1992, 16, 199–203. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Fei-Fei, L. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar] [CrossRef]
- De Logu, F.; Ugolini, F.; Maio, V.; Simi, S.; Cossu, A.; Massi, D.; Italian Association for Cancer Research (AIRC) Study Group; Nassini, R.; Laurino, M. Recognition of cutaneous melanoma on digitized histopathological slides via artificial intelligence algorithm. Front. Oncol. 2020, 10, 1559. [Google Scholar] [CrossRef]
- Sumithra, R.; Suhil, M.; Guru, D. Segmentation and classification of skin lesions for disease diagnosis. Procedia Comput. Sci. 2015, 45, 76–85. [Google Scholar] [CrossRef]
- Iqbal, I.; Younus, M.; Walayat, K.; Kakar, M.U.; Ma, J. Automated multi-class classification of skin lesions through deep convolutional neural network with dermoscopic images. Comput. Med. Imaging Graph. 2021, 88, 101843. [Google Scholar] [CrossRef]
- López-Labraca, J.; González-Díaz, I.; Díaz-de María, F.; Fueyo-Casado, A. An interpretable CNN-based CAD system for skin lesion diagnosis. Artif. Intell. Med. 2022, 132, 102370. [Google Scholar] [CrossRef]
- Xie, Y.; Zhang, J.; Xia, Y.; Shen, C. A mutual bootstrapping model for automated skin lesion segmentation and classification. IEEE Trans. Med. Imaging 2020, 39, 2482–2493. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Wang, Y.; Zhao, S.; Yao, C. Deep metric attention learning for skin lesion classification in dermoscopy images. Complex Intell. Syst. 2022, 8, 1487–1504. [Google Scholar] [CrossRef]
- Skin Cancer: Malignant, vs. Benign|Kaggle. Available online: https://www.kaggle.com/datasets/fanconic/skin-cancer-malignant-vs-benign (accessed on 1 November 2021).
- Gutman, D.; Codella, N.C.; Celebi, E.; Helba, B.; Marchetti, M.; Mishra, N.; Halpern, A. Skin lesion analysis toward melanoma detection: A challenge at the international symposium on biomedical imaging (ISBI) 2016, hosted by the international skin imaging collaboration (ISIC). arXiv 2016, arXiv:1605.01397. [Google Scholar]
- Veronica, R.; Nicholas, K.; Brigid, B.S.; Liam, C.; Emmanouil, C.; Noel, C.; Marc, C.; Dusza, S.; Pascale, G.; Gutman, D.; et al. A patient-centric dataset of images and metadata for identifying melanomas using clinical context. Sci. Data 2021, 8, 34. [Google Scholar]


| Dataset Name | DB1 | DB2 | DB3 |
|---|---|---|---|
| Source | ISIC 2019 [15,16,17] | [18] | PH2 [19] |
| No. benign lesions | 9640 | 667 | 160 |
| No. malignant lesions | 9281 | 344 | 40 |
| % females | 49% | 52% | - |
| % males | 51% | 48% | - |
| Mean age | 51 | - | - |
| Used for | Training | Training | Testing |
| Pixel range | [10, 10] | |
| Data augmentation | Scale range | [0.5, 1.5] |
| Rotation | [−90°, 90°] | |
| Frozen layers | 20 | |
| Hyperparameters | Learning rate | 0.001 |
| Mini-batch size | 16 | |
| Training time | 13 h | |
| Method | Dataset | Best Classification Metrics | |
|---|---|---|---|
| Present study’s DL approach | CNN based on pre-trained Inception-v3 | ISIC [15,16,17] and [18] for training and validation, PH2 [19] for a disjoint test dataset | Accuracy = 85.4 ± 3.2% Specificity = 75.5 ± 7.6% Precision = 93.6 ± 1.7% Recall = 88 ± 4.8% |
| Present study’s ML approach | Homology segmentation + ensemble boosted tree classifier | ISIC [15,16,17] and [18] for training and validation, PH2 [19] for a disjoint test dataset | Accuracy = 73.8 ± 1.1% Specificity = 44.5 ± 4.7% Precision = 85.4 ± 1.0% Recall = 81.1 ± 1.3% |
| Bechelli and Delhomelle, 2022 | DL approach | HAM10000 dataset [15], Kaggle dataset from ISIC archive [35] | Accuracy = 88% Precision = 93% Recall = 83% F1 = 0.88 |
| Bechelli and Delhomelle, 2022 | ML approach | Kaggle dataset from ISIC archive [35] | Accuracy = 73% Precision = 57% Recall = 79% F1 = 0.66 |
| Kaur et al., 2022 | DCNN | ISIC 2016 [36], 2017 [17], and 2020 [37]; PH2 [19] for a disjoint test dataset | Accuracy = 90.4% Precision = 90.4% Recall = 90.3% On PH2: Accuracy = 76% Precision = 67.8% Recall = 75.3% |
| Liu et al., 2021 | Mid-level feature learning based on pre-trained CNN + SVM classifier | ISIC 2017 [17] | AUC = 92.1% |
| Khan et al., 2020 | Neural Network Classifier | Three data subsets of ISIC, ISBI 2016 [36], and PH2 [19] | Accuracy = 98.4% Precision = 98.5% F1 = 0.98 |
| Mahbod et al., 2018 | Hybrid CNN + SVM Classifier | ISIC 2016 [36] and 2017 [17] | AUC = 91.4% Accuracy = 87.7% |
| Premaladha and Ravichandran,2016 | Neural Network + Hybrid Adaboost SVM | 992 images | Accuracy = 90% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brutti, F.; La Rosa, F.; Lazzeri, L.; Benvenuti, C.; Bagnoni, G.; Massi, D.; Laurino, M. Artificial Intelligence Algorithms for Benign vs. Malignant Dermoscopic Skin Lesion Image Classification. Bioengineering 2023, 10, 1322. https://doi.org/10.3390/bioengineering10111322
Brutti F, La Rosa F, Lazzeri L, Benvenuti C, Bagnoni G, Massi D, Laurino M. Artificial Intelligence Algorithms for Benign vs. Malignant Dermoscopic Skin Lesion Image Classification. Bioengineering. 2023; 10(11):1322. https://doi.org/10.3390/bioengineering10111322
Chicago/Turabian StyleBrutti, Francesca, Federica La Rosa, Linda Lazzeri, Chiara Benvenuti, Giovanni Bagnoni, Daniela Massi, and Marco Laurino. 2023. "Artificial Intelligence Algorithms for Benign vs. Malignant Dermoscopic Skin Lesion Image Classification" Bioengineering 10, no. 11: 1322. https://doi.org/10.3390/bioengineering10111322
APA StyleBrutti, F., La Rosa, F., Lazzeri, L., Benvenuti, C., Bagnoni, G., Massi, D., & Laurino, M. (2023). Artificial Intelligence Algorithms for Benign vs. Malignant Dermoscopic Skin Lesion Image Classification. Bioengineering, 10(11), 1322. https://doi.org/10.3390/bioengineering10111322