

Prospective Observational Study of a Non-Arthroscopic Autologous Cartilage Micrografting Technology for Knee Osteoarthritis


Abstract
:
1. Introduction
2. Materials and Methods
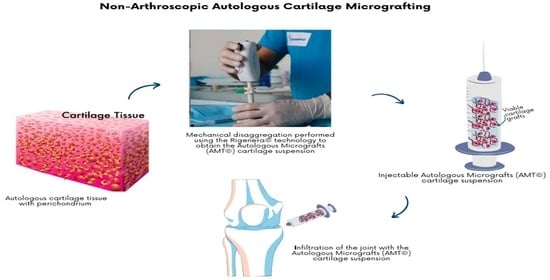
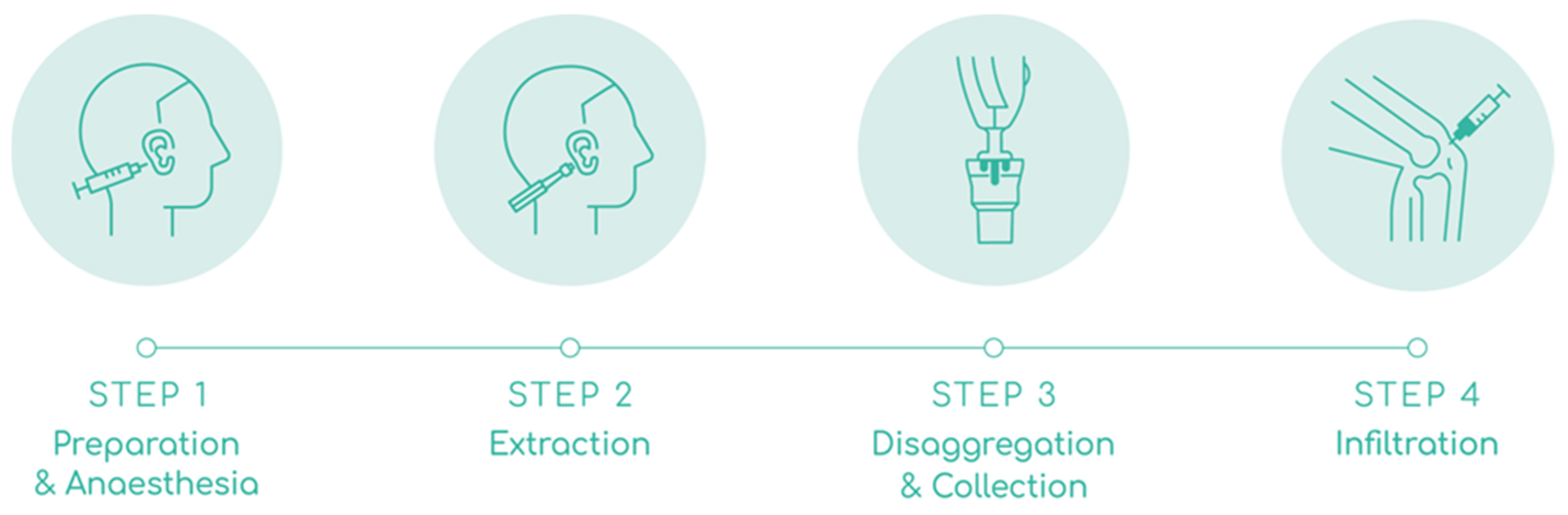
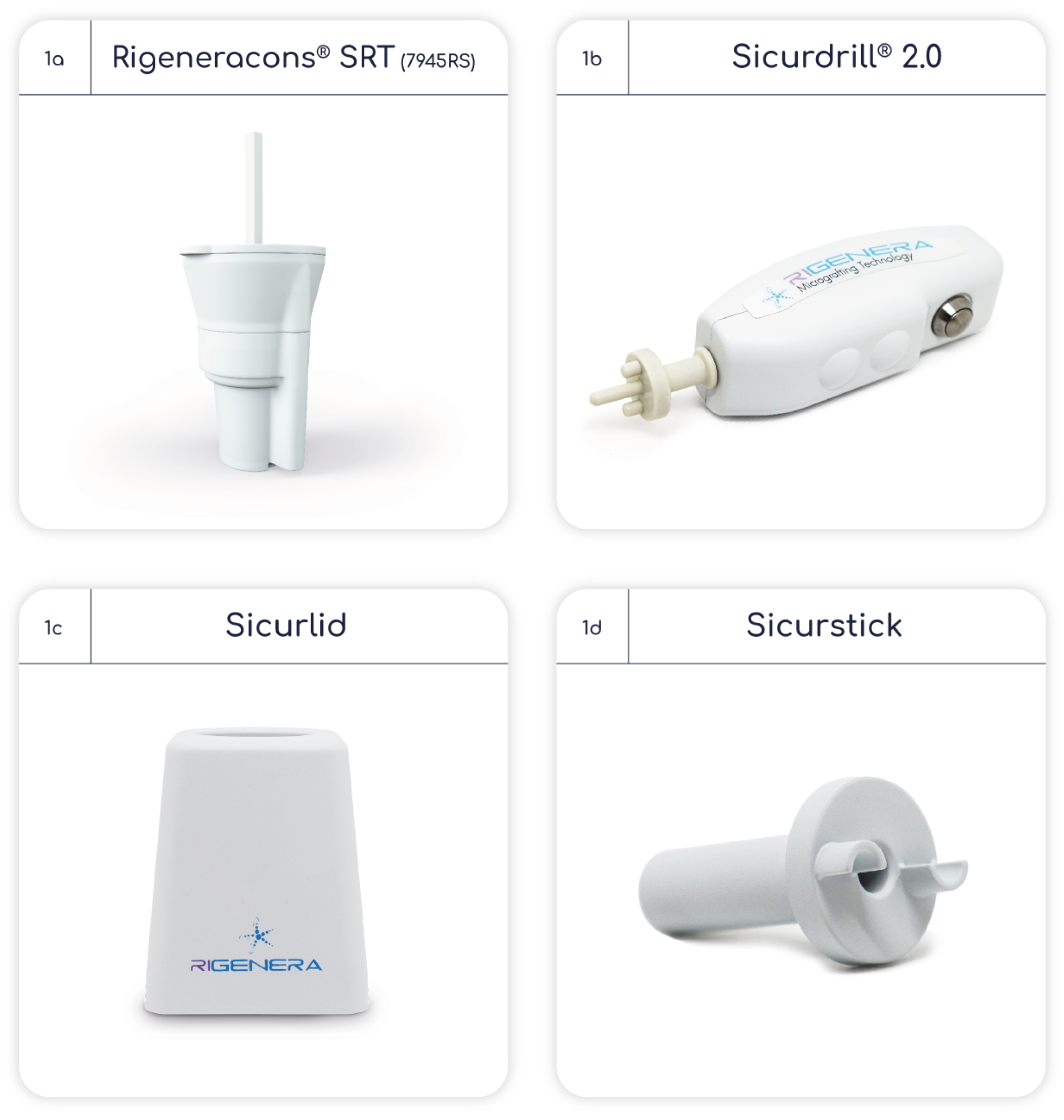
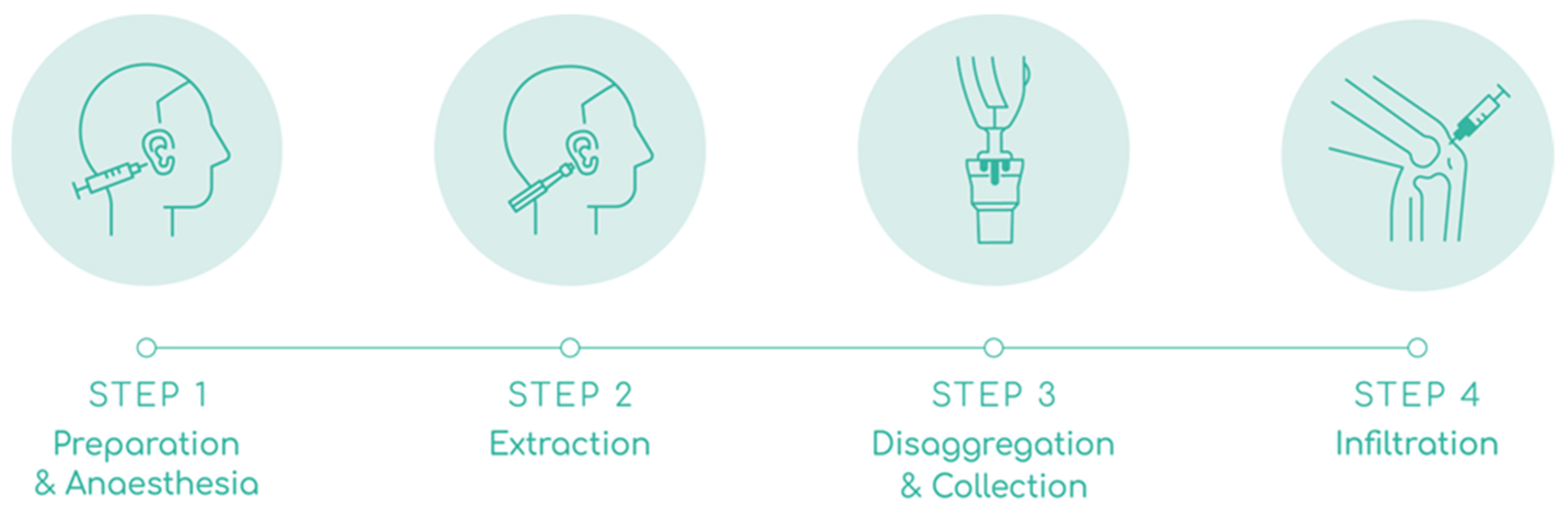
2.1. AMT® Procedure
2.2. Eligibility Criteria
2.3. Assessments
2.4. Statistical Analysis
3. Results
3.1. MRI and X-ray Findings
3.2. AMT® Procedure Outcomes
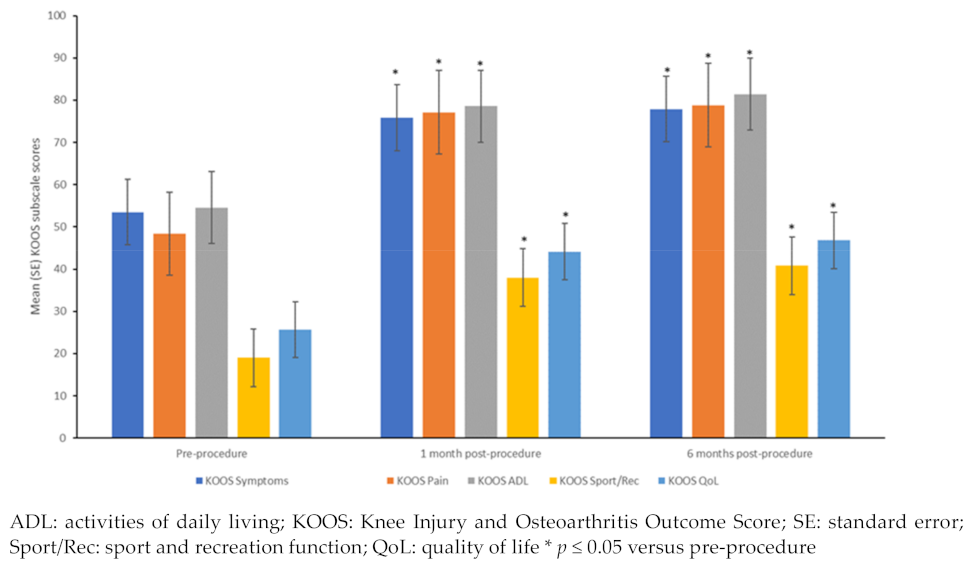
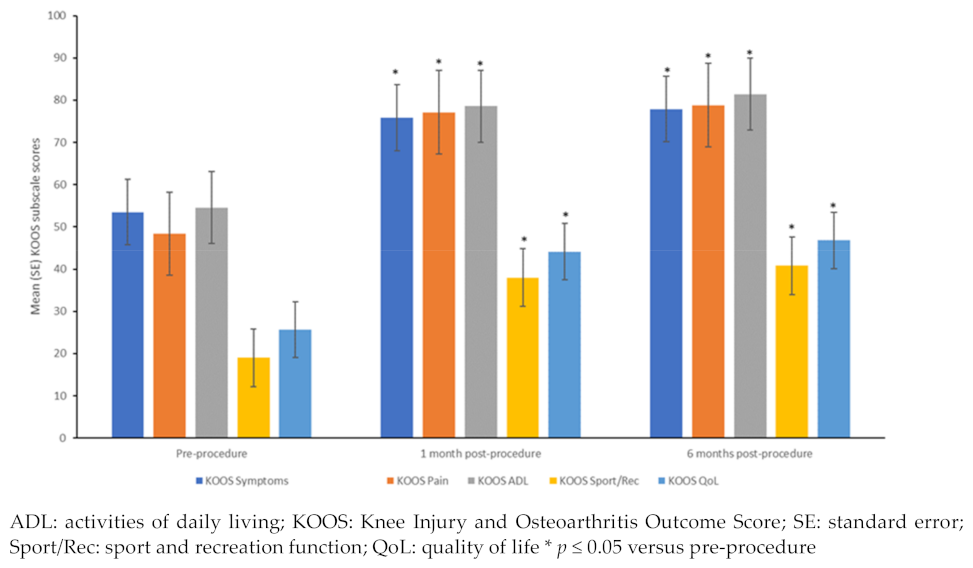
3.3. KOOS Subscale Scores
3.4. Safety and Long-Term Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, Regional Prevalence, Incidence and Risk Factors of Knee Osteoarthritis in Population-Based Studies. Eclinical. Med. 2020, 29–30, 100587. [Google Scholar]
- Hunter, D.J.; March, L.; Chew, M. Osteoarthritis in 2020 and Beyond: A Lancet Commission. Lancet 2020, 396, 1711–1712. [Google Scholar] [CrossRef] [PubMed]
- Grässel, S.; Muschter, D. Recent Advances in the Treatment of Osteoarthritis. F1000Research 2020, 9, 325. [Google Scholar] [CrossRef]
- Marcarelli, M.; Zappia, M.; Rissolio, L.; Baroni, C.; Astarita, C.; Trovato, L.; Graziano, A. Cartilage Micrografts as a Novel Non-Invasive and Non-Arthroscopic Autograft Procedure for Knee Chondropathy: Three-Year Follow-Up Study. J. Clin. Med. 2021, 10, 322. [Google Scholar] [CrossRef] [PubMed]
- Fusco, G.; Gambaro, F.M.; Di Matteo, B.; Kon, E. Injections in the Osteoarthritic Knee: A Review of Current Treatment Options. EFORT Open Rev. 2021, 6, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Siddiq, M.A.B.; Clegg, D.; Jansen, T.L.; Rasker, J.J. Emerging and New Treatment Options for Knee Osteoarthritis. Curr. Rheumatol. Rev. 2022, 18, 20–32. [Google Scholar]
- Liu, Y.; Shah, K.M.; Luo, J. Strategies for Articular Cartilage Repair And Regeneration. Front. Bioeng. Biotechnol. 2021, 9, 770655. [Google Scholar]
- Roseti, L.; Desando, G.; Cavallo, C.; Petretta, M.; Grigolo, B. Articular Cartilage Regeneration in Osteoarthritis. Cells 2019, 8, 1305. [Google Scholar] [CrossRef]
- Di Matteo, B.; Vandenbulcke, F.; Vitale, N.D.; Iacono, F.; Ashmore, K.; Marcacci, M.; Kon, E. Minimally Manipulated Mesenchymal Stem Cells for The Treatment of Knee Osteoarthritis: A Systematic Review of Clinical Evidence. Stem Cells Int. 2019, 2019, 1735242. [Google Scholar] [CrossRef]
- Desando, G.; Grigolo, B.; Deangelles Pereira Florentino, A.; Teixeira, M.W.; Barbagallo, F.; Naro, F.; da Silva-Junior, V.A.; Soares, A.F. Preclinical Evidence of Intra-Articular Autologous Cartilage Micrograft for Osteochondral Repair: Evaluation in a Rat Model. Cartilage 2021, 13, 1770S–1779S. [Google Scholar] [CrossRef]
- European Medicines Agency. Reflection Paper on Classification of Advanced Therapy Medicinal Products. EMA/CAT/600280/2010 rev.1. 2015. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-classification-advanced-therapy-medicinal-products_en-0.pdf (accessed on 21 July 2023).
- Giaccone, M.; Brunetti, M.; Camandona, M.; Trovato, L.; Graziano, A. A New Medical Device, Based on Rigenera® Protocol, in the Management of Complex Wounds. J. Stem Cells Res. Rev. Rep. 2014, 1, 3. [Google Scholar]
- Purpura, V.; Bondioli, E.; Graziano, A.; Trovato, L.; Melandri, D.; Ghetti, M.; Marchesini, A.; Cusella De Angelis, M.G.; Benedetti, L.; Ceccarelli, G.; et al. Tissue Characterization after a New Disaggregation Method for Skin Micro-Grafts Generation. J. Vis. Exp. 2016, 4, e53579. [Google Scholar]
- Trovato, L.; Monti, M.; Del Fante, C.; Cervio, M.; Lampinen, M.; Ambrosio, L.; Redi, C.A.; Perotti, C.; Kankuri, E.; Ambrosio, G.; et al. A New Medical Device Rigeneracons Allows to Obtain Viable Micro-Grafts from Mechanical Disaggregation of Human Tissues. J. Cell. Physiol. 2015, 230, 2299–2303. [Google Scholar] [CrossRef] [PubMed]
- Marcarelli, M.; Trovato, L.; Novarese, E.; Riccio, M.; Graziano, A. Rigenera® Protocol in the Treatment of Surgical Wound Dehiscence. Int. Wound J. 2016, 14, 277–281. [Google Scholar] [CrossRef]
- De Francesco, F.; Graziano, A.; Trovato, L.; Ceccarelli, G.; Romano, M.; Marcarelli, M.; Cusella De Angelis, G.M.; Cillo, U.; Riccio, M.; Ferraro, G.A. A Regenerative Approach with Dermal Micrografts in the Treatment of Chronic Ulcers. Stem Cell Rev. 2017, 13, 139–148. [Google Scholar] [CrossRef]
- Riccio, M.; Marchesini, A.; Zingaretti, N.; Carella, S.; Senesi, L.; Onesti, M.G.; Parodi, P.C.; Ribuffo, D.; Vaienti, L.; De Francesco, F. A Multicentre Study: The Use of Micrografts in the Reconstruction of Full-Thickness Posttraumatic Skin Defects of the Limbs—A Whole Innovative Concept in Regenerative Surgery. Stem Cells Int. 2019, 2019, 5043518. [Google Scholar] [CrossRef]
- Graziano, A.; Carinci, F.; Scolaro, S.; D’Aquino, R. Periodontal Tissue Generation Using Autologous Dental Ligament Micro-Grafts: Case Report with 6 Months Follow-Up. Ann. Oral. Maxillofac. Surg. 2013, 1, 20. [Google Scholar] [CrossRef]
- Gentile, P.; Scioli, M.G.; Bielli, A.; Orlandi, A.; Cervelli, V. A Combined Use of Chondrocytes Micro Grafts (CMG) Mixed with Platelet Rich Plasma (PRP) in Patients Affected by Pinch Nose Deformity. J. Regen. Med. 2016, 5, 2. [Google Scholar]
- Gentile, P.; Scioli, M.G.; Bielli, A.; Orlandi, A.; Cervelli, V. Reconstruction of Alar Nasal Cartilage Defects Using a Tissue Engineering Technique Based on a Combined Use of Autologous Chondrocyte Micrografts and Plateletrich Plasma: Preliminary Clinical and Instrumental Evaluation. Plast. Reconstr. Surg. Glob. Open 2016, 4, e1027. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, G.; Gentile, P.; Marcarelli, M.; Balli, M.; Ronzoni, F.L.; Benedetti, L.; Cusella De Angelis, M.G. In Vitro and In Vivo Studies of Alar-Nasal Cartilage Using Autologous Micro-Grafts: The Use of the Rigenera® Protocol in the Treatment of an Osteochondral Lesion of the Nose. Pharmaceuticals 2017, 10, 53. [Google Scholar] [CrossRef] [PubMed]
- Zanzottera, F.; Lavezzari, E.; Trovato, L.; Icardi, A.; Graziano, A. Adipose Derived Stem Cells and Growth Factors Applied on Hair Transplantation. Follow-Up Of Clinical Outcome. J. Cosmet. Dermatol. Sci. Appl. 2014, 04, 268–274. [Google Scholar] [CrossRef]
- Gentile, P.; Scioli, M.G.; Bielli, A.; Orlandi, A.; Cervelli, V. Stem Cells from Human Hair Follicles: First Mechanical Isolation for Immediate Autologous Clinical Use in Androgenetic Alopecia and Hair Loss. Stem Cell Investig. 2017, 4, 58. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P.; Scioli, M.G.; Cervelli, V.; Orlandi, A.; Garcovich, S. Autologous Micrografts from Scalp Tissue: Trichoscopic and Long-Term Clinical Evaluation in Male and Female Androgenetic Alopecia. Biomed Res. Int. 2020, 2020, 7397162. [Google Scholar] [CrossRef]
- Zari, S. Short-Term Efficacy of Autologous Cellular Micrografts in Male and Female Androgenetic Alopecia: A Retrospective Cohort Study. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1725–1736. [Google Scholar] [CrossRef]
- Svolacchia, F.; De Francesco, F.; Trovato, L.; Graziano, A.; Ferraro, G.A. An Innovative Regenerative Treatment of Scars with Dermal Micrografts. J. Cosmet. Dermatol. 2016, 15, 245–253. [Google Scholar] [CrossRef]
- Fernández, A.D.; Luengo, A.B. Biostimulation of Knee Cartilage Using Autologous Micro-Grafts: A Preliminary Study of the Rigenera Protocol in Osteochondral Lesions of the Knee. Rehabil. Sci. 2018, 3, 8–12. [Google Scholar] [CrossRef]
- Kellgren, J.; Lawrence, J. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a Self-Administered Outcome Measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Vigano, M.; Tessaro, I.; Trovato, L.; Colombini, A.; Scala, M.; Magi, A.; Toto, A.; Peretti, G.; de Girolamo, L. Rationale and Pre-Clinical Evidences for the Use of Autologous Cartilage Micrografts In Cartilage Repair. J. Orthop. Surg. Res. 2018, 13, 279. [Google Scholar] [CrossRef]
- Vágó, J.; Takács, R.; Kovács, P.; Hajdú, T.; van der Veen, D.R.; Matta, C. Combining Biomechanical Stimulation and Chronobiology: A Novel Approach for Augmented Chondrogenesis? Front. Bioeng. Biotechnol. 2023, 11, 1232465. [Google Scholar] [CrossRef] [PubMed]
- Erggelet, C.; Mandelbaum, B.R.; Mrosek, E.H.; Scopp, J.M. Principles of Cartilage Repair; Springer: Berlin, Germany, 2008; Available online: https://link.springer.com/book/10.1007/978-3-7985-1593-2 (accessed on 24 October 2023).
- Pearle, A.D.; Warren, R.F.; Rodeo, S.A. Basic Science of Articular Cartilage and Osteoarthritis. Clin. Sports Med. 2005, 24, 1–12. [Google Scholar] [CrossRef]
- Buckwalter, J.A.; Mankin, H.J.; Grodzinsky, A.J. Articular Cartilage and Osteoarthritis. Instr. Course Lect. 2005, 54, 465–480. [Google Scholar]
- Buckwalter, J.A.; Mankin, H.J. Articular Cartilage: Degeneration and Osteoarthritis, Repair, Regeneration, and Transplantation. Instr. Course Lect. 1998, 47, 487–504. [Google Scholar] [PubMed]
- Armiento, A.R.; Alini, M.; Stoddart, M.J. Articular Fibrocartilage—Why Does Hyaline Cartilage Fail to Repair? Adv. Drug Deliv. Rev. 2019, 146, 289–305. [Google Scholar] [CrossRef]
- Ho, C.L.; Huang, L.L.H.; Shieh, S.J. Perichondrial Progenitor Cells Promote Proliferation and Chondrogenesis of Mature Chondrocytes. Regen. Biomater. 2022, 9, rbab078. [Google Scholar] [CrossRef] [PubMed]
- Gvaramia, D.; Kern, J.; Jakob, Y.; Zenobi-Wong, M.; Rotter, N. Regenerative Potential of Perichondrium: A Tissue Engineering Perspective. Tissue Eng. Part B Rev. 2021, 28, 531–541. [Google Scholar] [CrossRef]
- Bruns, J.; Meyer-Pannwitt, U.; Silbermann, M. The Rib Perichondrium. An Anatomical Study in Sheep of a Tissue Used as Transplant in the Treatment of Hyaline-Cartilage Defects. Acta. Anat. 1992, 144, 258–266. [Google Scholar] [CrossRef]
- Mori, M. Studies on Cartilage Regeneration, Based on Experimental Studies on Rabbit Ear [in German]. Dtsch. Z. Chir. 1905, 76, 220. [Google Scholar] [CrossRef]
- Skoog, T.; Ohlsén, L.; Sohn, S.A. Perichondrial Potential for Cartilagenous Regeneration. Scand. J. Plast. Reconstr. Surg. 1972, 6, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From Joint Injury to Osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [PubMed]
- Mercieca-Bebber, R.; King, M.T.; Calvert, M.J.; Stockler, M.R.; Friedlander, M. The Importance of Patient-Reported Outcomes in Clinical Trials and Strategies for Future Optimization. Patient Relat. Outcome Meas. 2018, 9, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Collins, N.J.; Prinsen, C.A.C.; Christensen, R.; Bartels, E.M.; Terwee, C.B.; Roos, E.M. Knee Injury and Osteoarthritis Outcome Score (KOOS): Systematic Review and Meta-Analysis of Measurement Properties. Osteoarthr. Cartil. 2016, 24, 1317–1329. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Age (Years) | Sex | BMI (kg/m2) | Diagnosis Based on KL Scale | Clinical History | Past Medications | Past Procedures |
|---|---|---|---|---|---|---|---|
| 1 | 63 | Male | 25 | OA grade 3; chondropathy in left knee | Pain for the past 4 years and stiffness which became worse around a month before enrollment into study. Medial meniscus posterior horn tear 10 years prior to study enrollment which was not treated | None | None |
| 2 | 84 | Female | 23 | OA grade 3–4 | Pain in right knee from past 10 years | None | None |
| 3 | 64 | Female | 22 | OA grade 3–4 | Left knee pain for 8 years, worsening over time. Gonarthrosis for 8 years | NSAIDs | PRP injections in 2020 and 2021 |
| 4 | 37 | Male | 25 | Chondropathy grade 3 | Gonarthrosis | NSAIDs and paracetamol | Physiotherapy and PRP |
| 5 | 74 | Female | 23 | OA grade 3 | Gonarthrosis. Pain in affected right knee for the past 10 years that became worse after an accident nearly 7 months prior to study enrolment | None | None |
| 6 | 73 | Female | 22 | OA grade 2 | Pain for past 2 years | NSAIDs for 3 months | Physiotherapy |
| 7 | 73 | Female | 22 | OA grade 1-early 2 | Very mild pain for the past less than 1 year | None | None |
| 8 | 64 | Female | 23 | OA grade 1 early 2 | Pain for the past one year. Fibromyalgia and depression | None | None |
| 9 | 53 | Male | 31 | OA grade 1 early 2 | Pain, reduced mobility and grinding sensation (crackling) | NSAIDs, education about weight control | Physiotherapy |
| 10 | 53 | Male | 31 | OA grade 3 symptomatic | Mild pain and reduced mobility | None | None |
| Patient Number | MRI Findings | X-Ray Findings |
|---|---|---|
| 1 | Subchondral bone edema medial femoral condyle with small cartilage lesion, medial meniscus degenerative tear. Chondropathy patella grade III. | Standing X-ray: medial compartment narrowing |
| 2 | Chondropathy patella II–III and medial femoral condyle grade III–IV. | Osteoarthritis KL scale grade 3–early 4 |
| 3 | Medial compartment narrowing with chondropathy both condyles.Baker cyst 4 cm × 9 cm | Osteophytes present; KL scale grade 3 to 4 of osteoarthritis with medial compartment narrowing |
| 4 | Patella alta 3rd degree chondropathy patella and cartilage wear 1.7 cm × 1.5 cm at the femoral trochlea | Patella alta |
| 5 | Chondropathy with diffuse cartilage defects | Osteoarthritis grade 3 |
| 6 | Chondropathy patella grade III with cartilage defects | Osteoarthritis grade 2 |
| 7 | Diffuse cartilage wear Outerbridge grade II | Osteoarthritis grade 1–2 |
| 8 | Three-plane study of the left knee. Internal meniscus of preserved morphology and signal. External meniscus with increased horizontal signal that also extended to the lower articular surface compatible with meniscal tear and associated with the presence of small loculated cystic images that extended anteriorly with a larger component that crossed the lateral retinaculum which might correspond to the palpable swelling, compatible with parameniscal cyst. Conclusion: Rupture of the external meniscus body with parameniscal cyst extending anteriorly, crossing the lateral retinaculum. Slight decrease in the thickness of the patellar cartilage in its superior and central portion. | Osteoarthritis KL grade 1–2 |
| 9 | Chondropathy wear lateral tibial condyle | Osteoarthritis of the femorotibial joint left knee KL grade 1–2 |
| 10 | Cartilage wear medial femoral condyle Outerbridge grade 2 and medial tibial condyle grade 2–3. | Osteoarthritis KL grade 3 |
| Patient Number | Description of Clinical Condition |
|---|---|
| 1 | No pain and good mobility at 10 months post-procedure |
| 2 | Lateral pain and good mobility as early as 3 weeks post-procedure |
| 3 | Less pain and better mobility as early as 3 weeks post-procedure |
| 4 | Impressive improvement in mobility and pain reduction from within 2 months post-procedure. The patient started bicycling post-procedure, which was stopped earlier due to pain |
| 5 | Improvement in clinical outcomes as early as 6 weeks post-procedure The patient started running at 2 months and playing basketball at low intensity at 3 months |
| 6 | Able to do daily activities without any pain. Clinical improvement observed was maintained even after 11 months post-procedure |
| 7 | No pain while carrying out daily activities, while pre-procedure the patient could not be on foot for more than 2 h The patient was able to walk for longer periods and was also able to take the stairs instead of the elevator Clinical improvement observed was maintained even after 1-year post-procedure |
| 8 | No pain and good mobility which was maintained even after 10 months post-procedure |
| 9 | Reduced pain and ability to walk long distances of more than 10 km with only minimal pain The patient lost some weight, but not sufficient to significantly help with the overall body inflammation and biomechanics in the joint |
| 10 | Reduced pain and improved mobility |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsoukas, D.; Muntean, I.; Simos, C.; Sabido-Vera, R. Prospective Observational Study of a Non-Arthroscopic Autologous Cartilage Micrografting Technology for Knee Osteoarthritis. Bioengineering 2023, 10, 1294. https://doi.org/10.3390/bioengineering10111294
Tsoukas D, Muntean I, Simos C, Sabido-Vera R. Prospective Observational Study of a Non-Arthroscopic Autologous Cartilage Micrografting Technology for Knee Osteoarthritis. Bioengineering. 2023; 10(11):1294. https://doi.org/10.3390/bioengineering10111294
Chicago/Turabian StyleTsoukas, Dimitrios, Ilie Muntean, Christos Simos, and Ruben Sabido-Vera. 2023. "Prospective Observational Study of a Non-Arthroscopic Autologous Cartilage Micrografting Technology for Knee Osteoarthritis" Bioengineering 10, no. 11: 1294. https://doi.org/10.3390/bioengineering10111294
APA StyleTsoukas, D., Muntean, I., Simos, C., & Sabido-Vera, R. (2023). Prospective Observational Study of a Non-Arthroscopic Autologous Cartilage Micrografting Technology for Knee Osteoarthritis. Bioengineering, 10(11), 1294. https://doi.org/10.3390/bioengineering10111294