Itch in Chronic Wounds: Pathophysiology, Impact, and Management


Abstract
1. Introduction
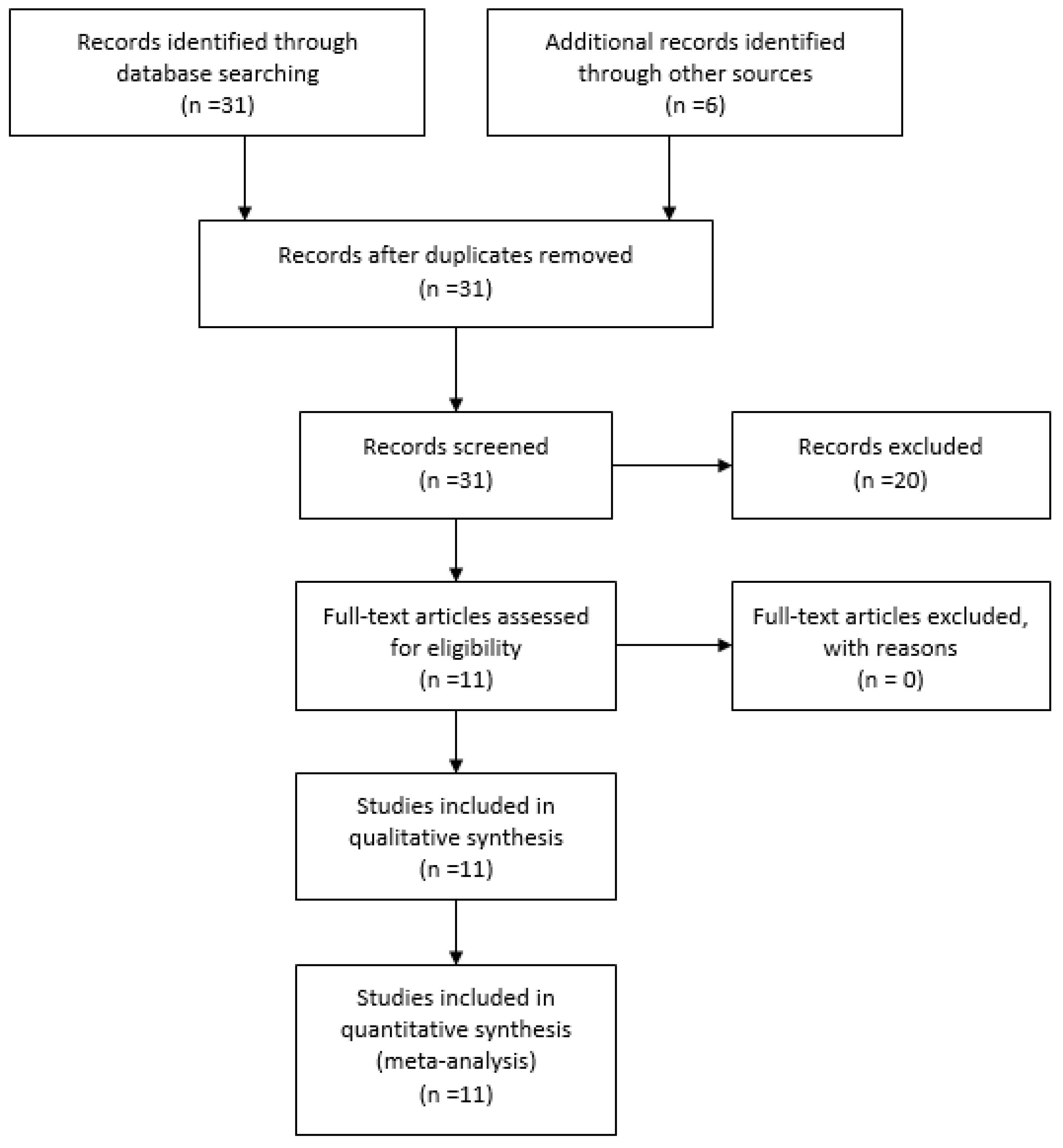
2. Methods
Literature Search
3. Results
3.1. Characteristics and Pathophysiological Mechanisms of Itch
3.2. Impact on QoL
3.3. Prevention of Itch in Chronic Wounds
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brenaut, E.; Garlantezec, R.; Talour, K.; Misery, L. Itch Characteristics in Five Dermatoses: Non-atopic Eczema, Atopic Dermatitis, Urticaria, Psoriasis and Scabies. Acta Derm. Venereol. 2013, 93, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Hareendran, A.; Bradbury, A.; Budd, J.; Geroulakos, G.; Hobbs, R.; Kenkre, J.; Symonds, T. Measuring the impact of venous leg ulcers on quality of life. J. Wound Care 2005, 14, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Hareendran, A.; Doll, H.; Wild, D.J.; Moffatt, C.J.; Musgrove, E.; Wheatley, C.; Franks, P.J. The venous leg ulcer quality of life (VLU-QoL) questionnaire: Development and psychometric validation. Wound Repair Regen. 2007, 15, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Paul, J.C.; Pieper, B.; Templin, T.N. Itch: Association with chronic venous disease, pain, and quality of life. J. Wound Ostomy Continence Nurs. 2011, 38, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Paul, J. A cross-sectional study of chronic wound-related pain and itching. Ostomy Wound Manage 2013, 59, 28–34. [Google Scholar] [PubMed]
- Paul, J. Characteristics of chronic wounds that itch. Adv. Skin Wound Care 2013, 26, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Upton, D.; Richardson, C.; Andrews, A.; Rippon, M. Wound pruritus: Prevalence, aetiology and treatment. J. Wound Care 2013, 22, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Upton, D.; Penn, F.; Richardson, C.; Rippon, M. Psychological management of wound pruritus. J. Wound Care 2014, 23, 291–299. [Google Scholar] [CrossRef] [PubMed]
- D’Erme, A.M.; Iannone, M.; Dini, V.; Romanelli, M. Contact dermatitis in patients with chronic leg ulcers a common and neglected problem: A review 2000–2015. J. Wound Care 2016, 25, S23–S29. [Google Scholar] [CrossRef] [PubMed]
- Paul, J. Descriptors for Itch Related to Chronic Wounds. Wounds 2018, 30, 4–9. [Google Scholar] [PubMed]
- Parnell, L.K.S. Itching for Knowledge About Wound and Scar Pruritus. Wounds 2018, 30, 17–36. [Google Scholar] [PubMed]
- Lerner, E. Why Do Wounds Itch? Wounds 2018, 30, 1–3. [Google Scholar] [PubMed]
- Gardner, S.E.; Frantz, R.A. Wound bioburden and infection. In Wound Care Essentials: Practice Principles, 3rd ed.; Baranoski, S., Ayello, E.A., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; Volume 1, pp. 126–174. [Google Scholar]
- Schultz, G.S.; Sibbald, R.G.; Falanga, V.; Ayello, E.A.; Dowsett, C.; Harding, K.; Romanelli, M.; Stacey, M.C.; Teot, L.; Vanscheidt, W. Wound bed preparation: A systematic approach to wound management. Wound Repair Regen. 2003, 11, S1–S28. [Google Scholar] [CrossRef] [PubMed]
- Duque, M.I.; Yosipovitch, G.; Chan, Y.H.; Smith, R.; Levy, P. Itch, pain, and burning sensation are common symptoms in mild to moderate chronic venous insufficiency with an impact on quality of life. J. Am. Acad. Dermatol. 2005, 53, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Gray, M.; Weir, D. Prevention and treatment of moisture-associated skin damage (maceration) in the periwound skin. J. Wound Ostomy Continence Nurs. 2007, 34, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Weisshaar, E.; Szepietowski, J.C.; Dalgard, F.J.; Garcovich, S.; Gieler, U.; Giménez-Arnau, A.M.; Lambert, J.; Leslie, T.; Mettang, T.; Misery, L.; et al. European S2k Guideline on Chronic Pruritus. Acta Derm. Venereol. 2019, 99, 469–506. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Year | Country | Type of Article | Purpose of Study | Findings |
|---|---|---|---|---|---|
| Hareendran A. et al. [2] | 2005 | United Kingdom | Qualitative and quantitative methods were used to explore health related quality of life (HRQoL) issues in 38 patients | Identify HRQoL issues in patients with venous leg ulcers | Itching was reported in 69.4% of patients but no influence on sleep and functional limitations were found |
| Hareendran A. et al. [3] | 2007 | United Kingdom | In-depth interviews with focus group of 36 patients | To develop and validate a disease-specific quality of life (QoL) measure, based on the conceptual model of the Skin Disease impact on quality of life Index (SKINDEX-29) for patients with chronic venous leg ulcers | Itch was ranked 4th among ten symptoms causing distress in chronic venous ulcers |
| Paul J.C. et al. [4] | 2011 | Michigan (USA) | Cross sectional study on 161 patients | Investigate itch related to chronic venous disease, pain, and QoL | Positive correlation between intensity of itch and severity of venous disease with lower QoL |
| Paul J. [5] | 2013 | Michigan (USA) | Cross sectional study on 199 patients with chronic wounds of different etiologies | Comparing pain and itch in chronic wounds | Wound-related itch was significantly associated with age, xerosis, employment status, and with venous wounds. Itch was rated higher on the perilesional skin, while pain was rated higher on the wound bed. |
| Paul J. [6] | 2013 | Michigan (USA) | Observational study on 200 patients with chronic wounds of different etiologies | Explore characteristics of wound-related itch | Itch characterizes more severe wounds with larger size, more tissue edema, and granulation issue and was also associated with moderate exudate amount or necrotic tissue |
| Upton D. et al. [7] | 2013 | United Kingdom | Literature review | Overview of the physiological mechanisms of itch and comorbidities in acute and chronic wounds | The itch causes a range of physical and psychological problems, reducing QoL and delaying healing. There are no specific guidelines on itch management in chronic wounds and further studies are needed. |
| Upton D. et al. [8] | 2013 | Australia | Literature review | Overview on psychological itch treatment in wounds | Unconventional treatments such as habit reversal training, relaxation, massage, and itch coping programs showed a potential role in reducing itch in association with standard treatments, but current literature evidence is limited. |
| D’Erme A.M. et al. [9] | 2016 | Italy | Literature review | Overview on contact allergy and polysensitization in patients with chronic wounds | Advanced dressings can cause allergic contact dermatitis. The most frequent was hydrogel, followed by hydrocolloid and by silver wound dressings. Primary prevention is required, avoiding sensitizers and irritant products, along with secondary prevention using patch tests in all patients with non-healing wounds. |
| Paul J. [10] | 2018 | Michigan (USA) | Structured interviews of 199 patients with chronic wounds | Identify descriptors for wound-related itch | 15 descriptors identified (annoying, bothersome, just want itching to go away, unpleasant, stubborn, disturbing sleep, insistent, disgusting, severe, awful, prickly, warm, worrisome, unbearable, uncontrollable) |
| Parnell L.K.S. et al. [11] | 2018 | Texas (USA) | Literature review | Overview on itch research focusing on itch in wound care | Importance of multidimensional questionnaires to characterize itch. The authors described sensory, affective dimensions of itch, the itch trigger, and itch receptors and pathways. They highlighted both conventional and unconventional pharmacological therapies. |
| Lerner E. [12] | 2018 | South Carolina (USA) | Literature review | Overview of current understanding on the physiology of itch in wounds | Proposal for unconventional therapeutic approaches based on physiology |
| Take-Home Messages |
|---|
| ✓ Itch in wounds is a very frequent symptom and should never be underestimated. The underlying mechanisms are very complex, including those of a subjective and multidimensional nature, which make investigations a real challenge for clinicians. |
| ✓ The application of the tissue debridement, inflammation/infection, moisture imbalance, epithelial edge advancement (TIME) principles of wound bed preparation, the topical management of perilesional skin, and a stepwise therapeutic approach based on European S2k Guideline on chronic itch (if causative treatment fails) seem to be the best management strategies to date. |
| ✓ Further studies are needed to better characterize and develop targeted therapies for itch in chronic wounds, adopting a tailored-based approach and drawing up practical guidelines. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iannone, M.; Janowska, A.; Dini, V.; Tonini, G.; Oranges, T.; Romanelli, M. Itch in Chronic Wounds: Pathophysiology, Impact, and Management. Medicines 2019, 6, 112. https://doi.org/10.3390/medicines6040112
Iannone M, Janowska A, Dini V, Tonini G, Oranges T, Romanelli M. Itch in Chronic Wounds: Pathophysiology, Impact, and Management. Medicines. 2019; 6(4):112. https://doi.org/10.3390/medicines6040112
Chicago/Turabian StyleIannone, Michela, Agata Janowska, Valentina Dini, Giulia Tonini, Teresa Oranges, and Marco Romanelli. 2019. "Itch in Chronic Wounds: Pathophysiology, Impact, and Management" Medicines 6, no. 4: 112. https://doi.org/10.3390/medicines6040112
APA StyleIannone, M., Janowska, A., Dini, V., Tonini, G., Oranges, T., & Romanelli, M. (2019). Itch in Chronic Wounds: Pathophysiology, Impact, and Management. Medicines, 6(4), 112. https://doi.org/10.3390/medicines6040112