
A Population-Based Cohort Study on the Ability of Acupuncture to Reduce Post-Stroke Depression


Abstract
:1. Introduction
2. Materials and Method
2.1. Source of Data
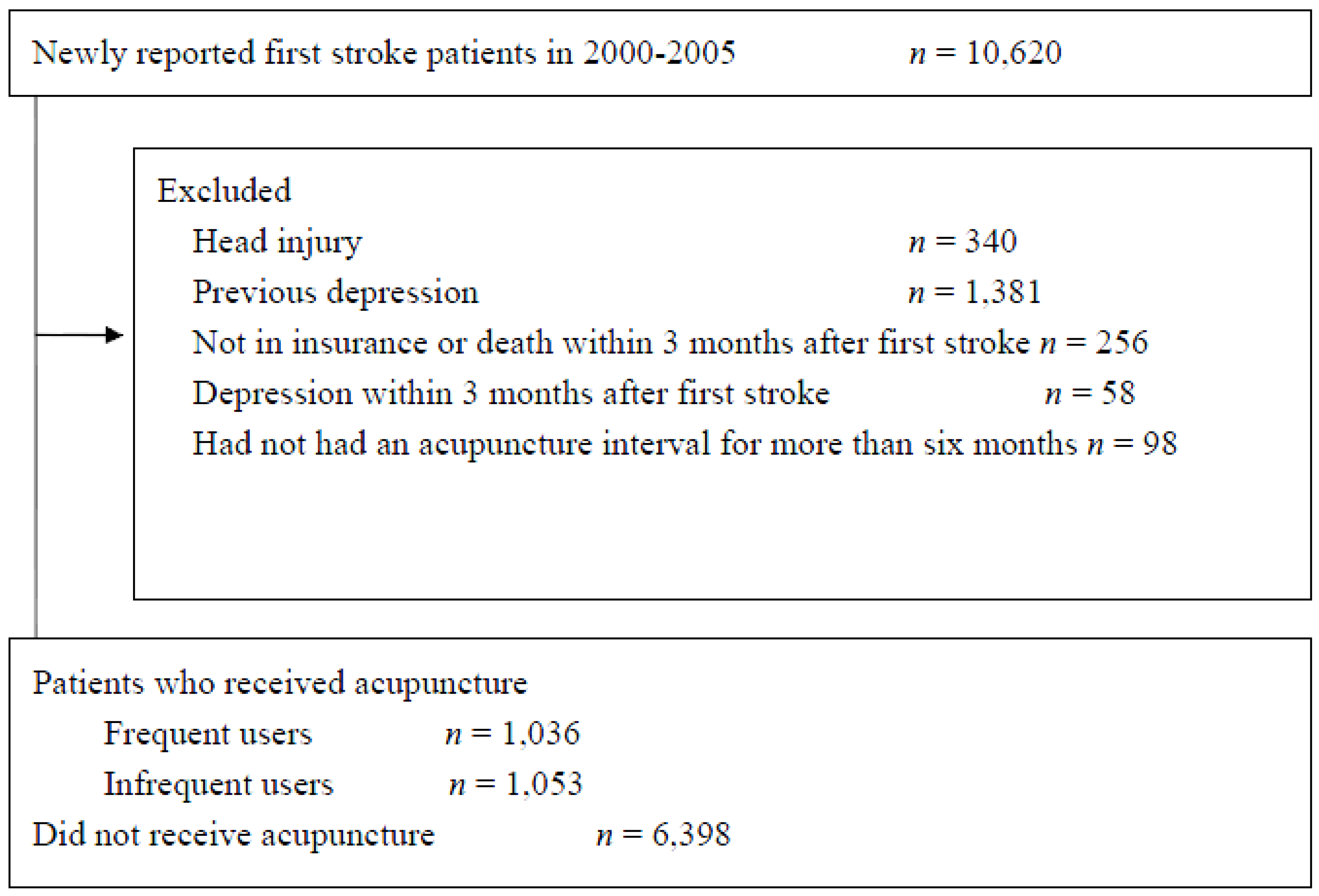
2.2. Participants and End-Point
2.3. Covariates
2.4. Statistical Analysis
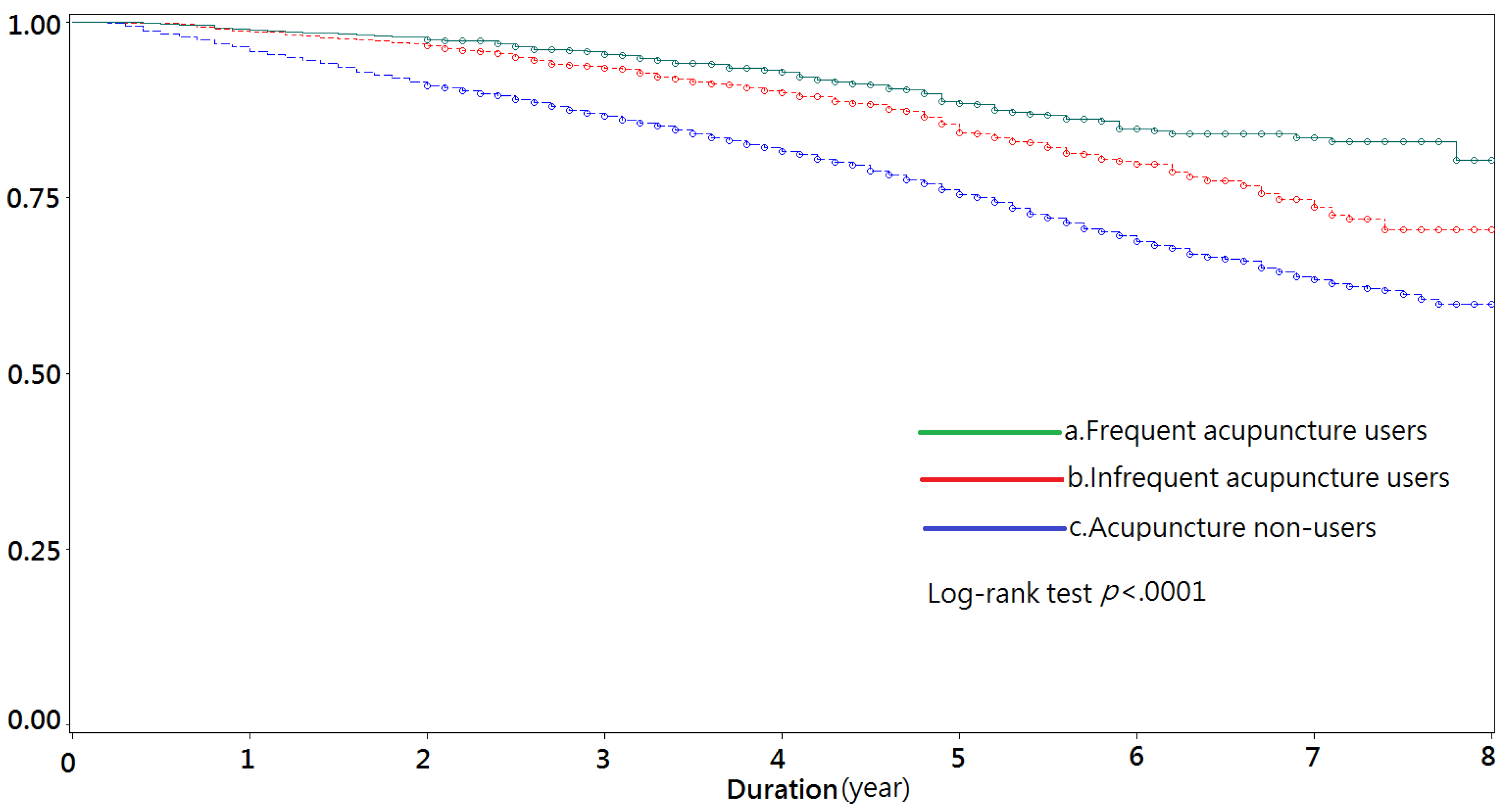
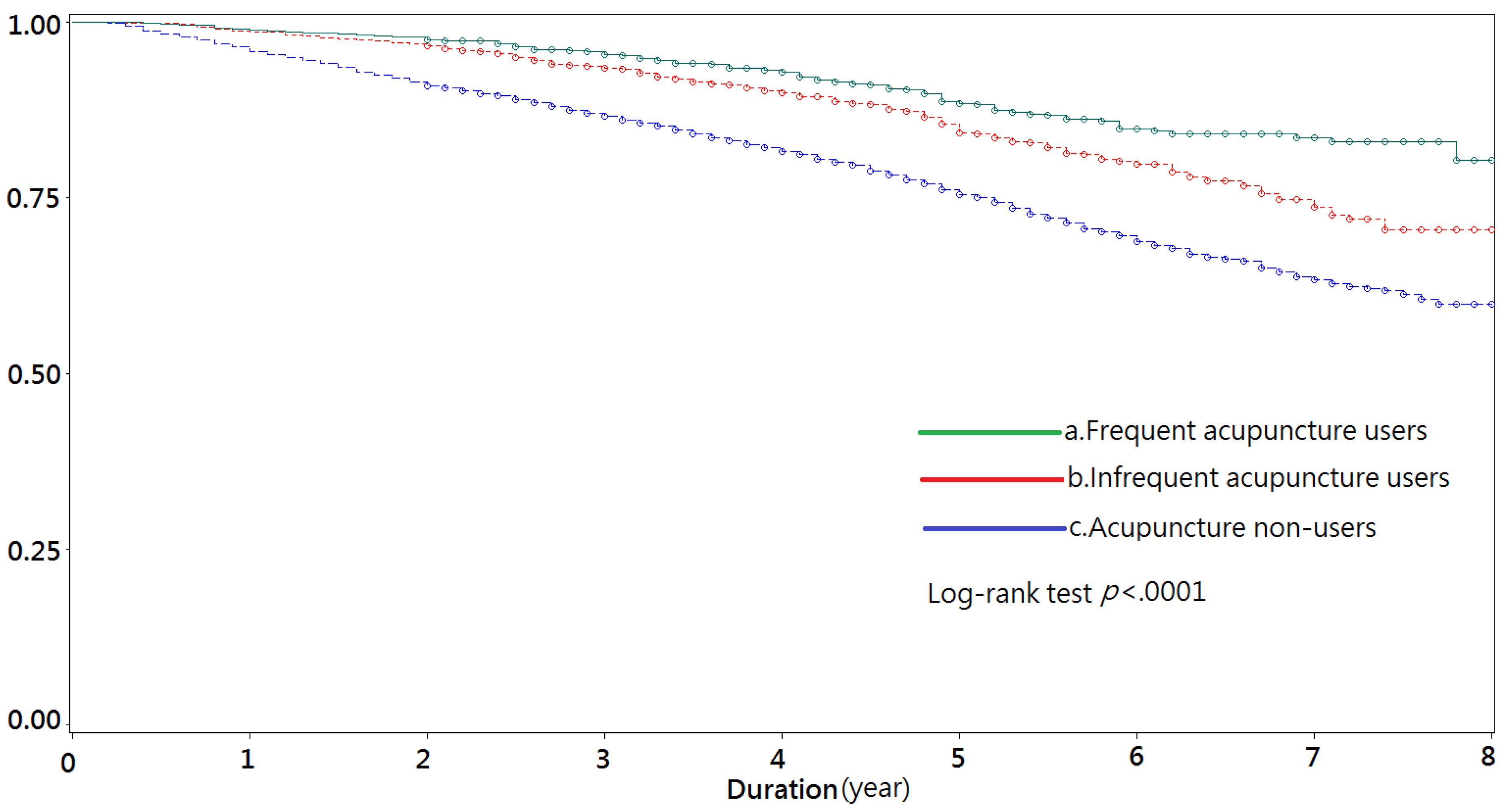
3. Results
3.1. Sample Characteristics
3.2. Cox Proportional Hazard Regression Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hsieh, F.I.; Chiou, H.Y. Stroke-Morbidity, Risk Factors, and Care in Taiwan. J. Stroke 2014, 16, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Pohjasvaara, T.V.R.; Vataja, R.; Leppävuori, A.; Kaste, M.; Erkinjuntti, T. Cognitive functions and depression as predictors of poor outcome 15 months after stroke. Cerebrovasc. Dis. 2002, 14, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Hackett, M.L.; Anderson, C.S.; House, A.; Halteh, C. Interventions for preventing depression after stroke. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef]
- Hou, W.H.; Liang, H.W.; Hsieh, C.L.; Hou, C.Y.; Wen, P.C.; Li, C.Y. Effects of stroke rehabilitation on incidence of poststroke depression: A population-based cohort study. J. Clin. Psychiatry 2013, 74, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Lee, Y.C.; Lin, C.C.; Chang, C.H.; Chiu, C.D.; Chou, L.W.; Sun, M.F.; Yen, H.R. Characteristics of traditional Chinese medicine usage in patients with stroke in Taiwan: A nationwide population-based study. J. Ethnopharmacol. 2016, 186, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Andersen, G.; Vestergaard, K.; Ingemann-Nielsen, M.; Lauritzen, L. Risk factors for post-stroke depression. Acta Psychiatrica Scand. 1995, 92, 193–198. [Google Scholar] [CrossRef]
- Hirata, S.; Ovbiagele, B.; Markovic, D.; Towfighi, A. Key factors associated with major depression in a national sample of stroke survivors. J. Stroke Cerebrovasc. Dis. 2016, 25, 1090–1095. [Google Scholar] [CrossRef] [PubMed]
- De Ryck, A.; Brouns, R.; Geurden, M.; Elseviers, M.; De Deyn, P.P.; Engelborghs, S. Risk factors for poststroke depression identification of inconsistencies based on a systematic review. J. Geriatr. Psychiatry Neurol. 2014, 27, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Caeiro, L.; Ferro, J.M.; Santos, C.O.; Figueira, M.L. Depression in acute stroke. J. Psychiatry Neurosci. 2006, 31, 377–383. [Google Scholar] [PubMed]
- Ayerbe, L.; Ayis, S.; Rudd, A.G.; Heuschmann, P.U.; Wolfe, C.D. Natural history, predictors, and associations of depression 5 years after stroke the South London Stroke Register. Stroke 2011, 42, 1907–1911. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-F.; Lee, S.-P.; Li, C.-Y. Sex differences in the incidence of hemorrhagic and ischemic stroke among diabetics in Taiwan. J. Women’s Health 2009, 18, 647–654. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Liu, C.-Y.; Hung, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J. Health Manag. 2006, 4, 1–22. [Google Scholar]
- Sung, S.F.; Hsieh, C.Y.; KaoYang, Y.H.; Lin, H.J.; Chen, C.H.; Chen, Y.W.; Hu, Y.H. Developing a stroke severity index based on administrative data was feasible using data mining techniques. J. Clin. Epidemiol. 2015, 68, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Post Stroke Depression. Available online: https://www.researchgate.net/publication/228850728_18_Post-Stroke_Depression (accessed on 13 March 2017).
- Salom-Moreno, J.; Sánchez-Mila, Z.; Ortega-Santiago, R.; Palacios-Ceña, M.; Truyol-Domínguez, S.; Fernández-de-las-Peñas, C. Changes in Spasticity, Widespread Pressure Pain Sensitivity, and Baropodometry After the Application of Dry Needling in Patients Who Have Had a Stroke: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2014, 37, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Man, S.-C.; Hung, B.H.; Ng, R.M.; Yu, X.-C.; Cheung, H.; Fung, M.P.; Li, L.S.; Leung, K.-P.; Leung, K.-P.; Tsang, K.W.; et al. A pilot controlled trial of a combination of dense cranial electroacupuncture stimulation and body acupuncture for post-stroke depression. BMC Complement. Altern. Med. 2014. [Google Scholar] [CrossRef] [PubMed]
- Gosman-Hedström, G.; Claesson, L.; Klingenstierna, U.; Carlsson, J.; Olausson, B.; Frizell, M.; Fagerberg, B.; Blomstrand, C. Effects of acupuncture treatment on daily life activities and quality of life a controlled, prospective, and randomized study of acute stroke patients. Stroke 1998, 29, 2100–2108. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Li, Z.M.; Jiang, Y.J.; Chen, L.D. A Meta-Analysis of Acupuncture Use in the Treatment of Cognitive Impairment After Stroke. J. Altern. Complement. Med. 2014, 20, 535–544. [Google Scholar] [CrossRef]
- Hsu, Y.-C.; Chiu, C.-J.; Wray, L.A.; Beverly, E.A.; Tseng, S.-P. Impact of traditional Chinese medicine on age trajectories of health: Evidence from the Taiwan longitudinal study on aging. J. Am. Geriatr. Soc. 2015, 63, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Salinas, J.; Beiser, A.; Himali, J.; Rosand, J.; Seshadri, S.; Dunn, E. Incidence and Predictors of Poststroke Depression: Results from the Framingham Heart Study (P5. 034). Neurology 2015, 84 (Suppl. 14), 35–41. [Google Scholar]
- Robinson, R.G.; Jorge, R.E.; Moser, D.J.; Acion, L.; Solodkin, A.; Small, S.L.; Fonzetti, P.; Hegel, M.; Arndt, S. Escitalopram and problem-solving therapy for prevention of poststroke depression: A randomized controlled trial. Jama 2008, 299, 2391–2400. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristic | Frequent Acupuncture Users a (N = 1036, 12.21%) | Infrequent Acupuncture Users b (N = 1053, 12.41%) | Acupuncture Non-Users c (N = 6398, 75.39%) | p Value |
|---|---|---|---|---|
| Female (%) | 444 (42.86) | 425 (40.36) | 2622 (40.98) | 0.378 |
| Age of diagnosis (Mean ± SD) | 61.28 ± 13.19 | 61.77 ± 13.59 | 66.21 ± 14.35 | <0.001 |
| Follow-up time (year) (Mean ± SD) | 4.67 ± 1.78 | 4.82 ± 1.76 | 4.28 ± 1.87 | <0.001 |
| Living area (%) | <0.001 | |||
| Urban area | 307 (30.10) | 275 (26.52) | 1471 (23.45) | |
| Satellite city | 303 (29.71) | 305 (29.41) | 1668 (26.59) | |
| Rural area | 410 (40.20) | 457 (44.07) | 3133 (49.95) | |
| Insurance income ranks (%) d,e | <0.001 | |||
| <15,000 NTD | 320 (30.89%) | 314 (29.82) | 2379 (37.18%) | |
| ≥15,000 NTD | 716 (69.11%) | 739 (70.18) | 4019 (62.82%) | |
| Type of stroke | <0.001 | |||
| hemorrhagic stroke | 261 (25.19) | 217 (20.61) | 1288 (20.13) | |
| occlusion stroke | 617 (59.56) | 647 (61.44) | 3923 (61.32) | |
| unknown | 158 (15.25) | 189 (17.95) | 1187 (18.55) | |
| Hospitalization days | <0.001 | |||
| ≤7 days | 458 (44.21) | 536 (50.90) | 3540 (52.20) | |
| 8–14 days | 253 (24.42) | 298 (28.30) | 1626 (25.52) | |
| 15–21 days | 111 (10.71) | 74 (7.03) | 541 (8.46) | |
| 22–28 days | 63 (6.08) | 52 (4.94) | 316 (4.94) | |
| ≥28 days | 151 (14.58) | 93 (8.83) | 575 (8.99) | |
| Comorbidities f | ||||
| Rheumatoid arthritis (%) | 91 (8.78) | 83 (7.88) | 440 (6.88) | 0.018 |
| Peripheral arterial disease (%) | 265 (25.58) | 234 (22.22) | 1216 (19.01) | <0.001 |
| Myocardial infarction (%) | 50 (4.83) | 54 (5.13) | 278 (4.35) | 0.312 |
| Cancer (%) | 152 (14.67) | 173 (16.43) | 919 (14.36) | 0.400 |
| Diabetes (%) | 531 (51.25) | 520 (49.38) | 2989 (46.72) | 0.003 |
| Hypertension (%) | 873 (84.27) | 887 (84.24) | 5160 (80.65) | <0.001 |
| Chronic kidney diseases (%) | 112 (10.81) | 110 (10.45) | 767 (11.99) | 0.140 |
| Chronic obstructive pulmonary diseases (%) | 554 (53.47) | 572 (54.32) | 3592 (56.14) | 0.070 |
| Head traumatic injury (%) | 23 (2.22) | 31 (2.94) | 231 (3.33) | 0.055 |
| Rehabilitation g | 390 (37.64) | 295 (28.02) | 1126 (17.60) | <0.001 |
| SSI (Mean ± SD) h | −0.16 ± 1.39 | −0.35 ± 1.22 | −0.14 ± 1.40 | <0.001 |
| Censor after stroke i | ||||
| Yes | 110 (10.62) | 177 (16.81) | 1551 (24.24) | <0.001 |
| Characteristic | Hazard Ratio a | p Value | 95% CI | |
|---|---|---|---|---|
| Acupuncture users (ref: Acupuncture non-users d) | ||||
| Frequent acupuncture users b | 0.475 | <0.001 | 0.389 | 0.580 |
| Infrequent acupuncture users c | 0.718 | <0.001 | 0.612 | 0.842 |
| Female | 0.777 | <0.001 | 0.705 | 0.856 |
| Age of diagnosis | 1.045 | <0.001 | 1.040 | 1.050 |
| Living area (ref: Rural area) | ||||
| Urban area | 0.836 | 0.005 | 0.738 | 0.947 |
| Satellite city | 0.966 | 0.548 | 0.861 | 1.082 |
| Insurance income (ref: <15,000 NTD) e,f | ||||
| ≥15,000 NTD | 1.082 | 0.128 | 0.978 | 1.198 |
| Type of stroke (ref: unknown) | ||||
| hemorrhagic stroke | 0.796 | 0.006 | 0.676 | 0.936 |
| occlusion stroke | 0.911 | 0.131 | 0.808 | 1.028 |
| Hospitalization days g | 1.098 | <0.001 | 1.053 | 1.145 |
| Comorbidities | ||||
| Rheumatoid arthritis | 0.998 | 0.989 | 0.833 | 1.195 |
| Peripheral arterial disease | 0.878 | 0.029 | 0.781 | 0.986 |
| Myocardial Infarction | 1.298 | 0.005 | 1.080 | 1.559 |
| Cancer | 1.423 | <0.001 | 1.268 | 1.597 |
| Diabetes | 1.136 | 0.009 | 1.032 | 1.251 |
| Hypertension | 0.844 | 0.008 | 0.744 | 0.956 |
| Chronic kidney diseases | 1.519 | <0.001 | 1.345 | 1.715 |
| Chronic obstructive pulmonary diseases | 1.219 | <0.001 | 1.097 | 1.355 |
| Head traumatic injury | 1.629 | <0.001 | 1.335 | 1.988 |
| Rehabilitation h (ref: no rehabilitation) | 0.929 | 0.221 | 0.825 | 1.045 |
| SSI i | 1.210 | <0.001 | 1.166 | 1.256 |
| Characteristic e | Hemorrhagic Stroke | Occlusion Stroke | ||||||
|---|---|---|---|---|---|---|---|---|
| Hazard Ratio a | p Value | 95% CI | Hazard Ratio a | p Value | 95% CI | |||
| Acupuncture users (ref: Acupuncture non-users d) | ||||||||
| Frequent acupuncture users b | 0.446 | <0.001 | 0.283 | 0.702 | 0.499 | <0.001 | 0.391 | 0.638 |
| Infrequent acupuncture users c | 0.831 | 0.318 | 0.577 | 1.196 | 0.707 | <0.001 | 0.578 | 0.865 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, S.-P.; Hsu, Y.-C.; Chiu, C.-J.; Wu, S.-T. A Population-Based Cohort Study on the Ability of Acupuncture to Reduce Post-Stroke Depression. Medicines 2017, 4, 16. https://doi.org/10.3390/medicines4010016
Tseng S-P, Hsu Y-C, Chiu C-J, Wu S-T. A Population-Based Cohort Study on the Ability of Acupuncture to Reduce Post-Stroke Depression. Medicines. 2017; 4(1):16. https://doi.org/10.3390/medicines4010016
Chicago/Turabian StyleTseng, Shuo-Ping, Yu-Ching Hsu, Ching-Ju Chiu, and Shang-Te Wu. 2017. "A Population-Based Cohort Study on the Ability of Acupuncture to Reduce Post-Stroke Depression" Medicines 4, no. 1: 16. https://doi.org/10.3390/medicines4010016
APA StyleTseng, S.-P., Hsu, Y.-C., Chiu, C.-J., & Wu, S.-T. (2017). A Population-Based Cohort Study on the Ability of Acupuncture to Reduce Post-Stroke Depression. Medicines, 4(1), 16. https://doi.org/10.3390/medicines4010016