Benzodiazepines: Their Use either as Essential Medicines or as Toxics Substances



Abstract
1. Introduction
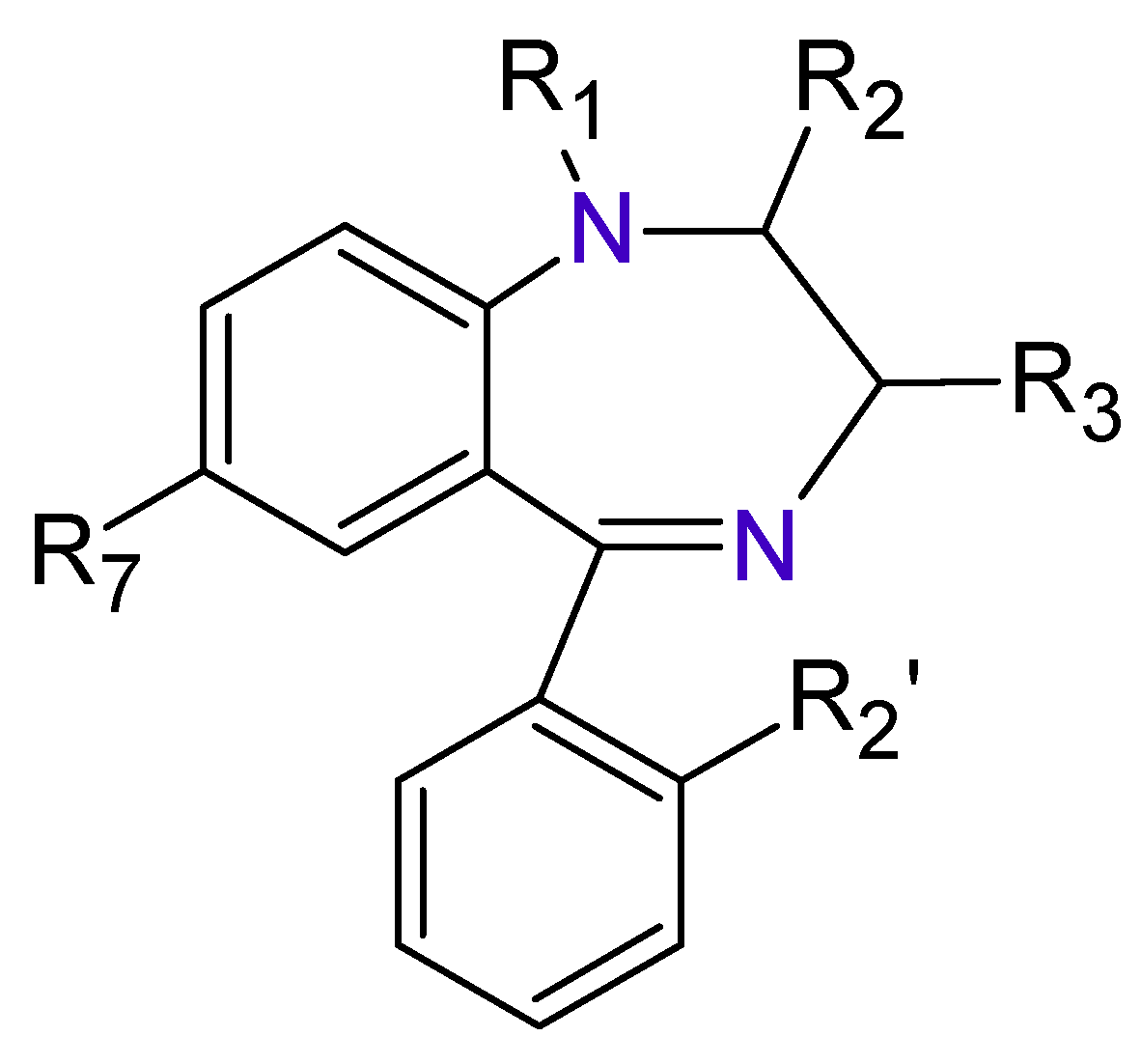
2. Benzodiazepines
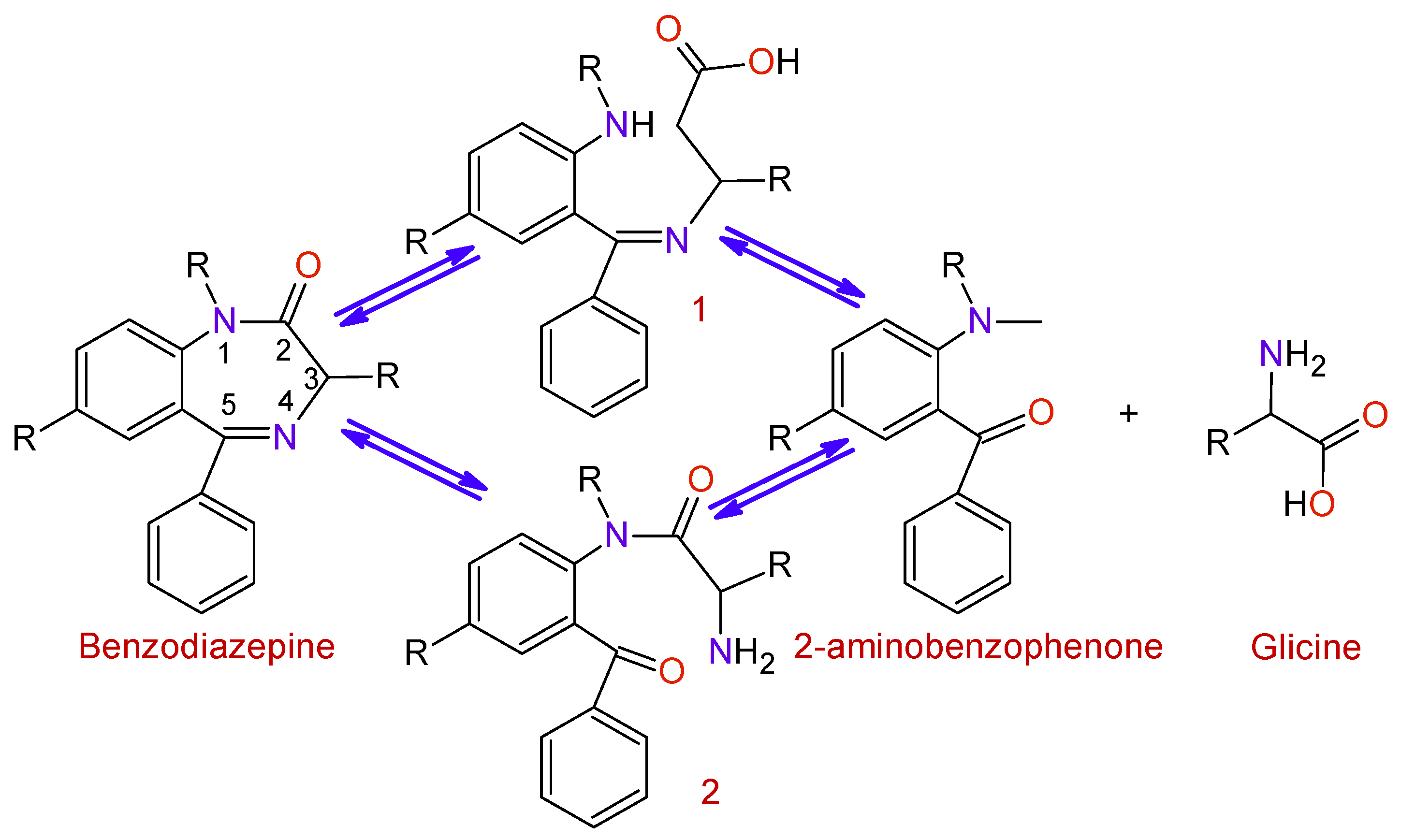
3. Synthesis of Benzodiazepines
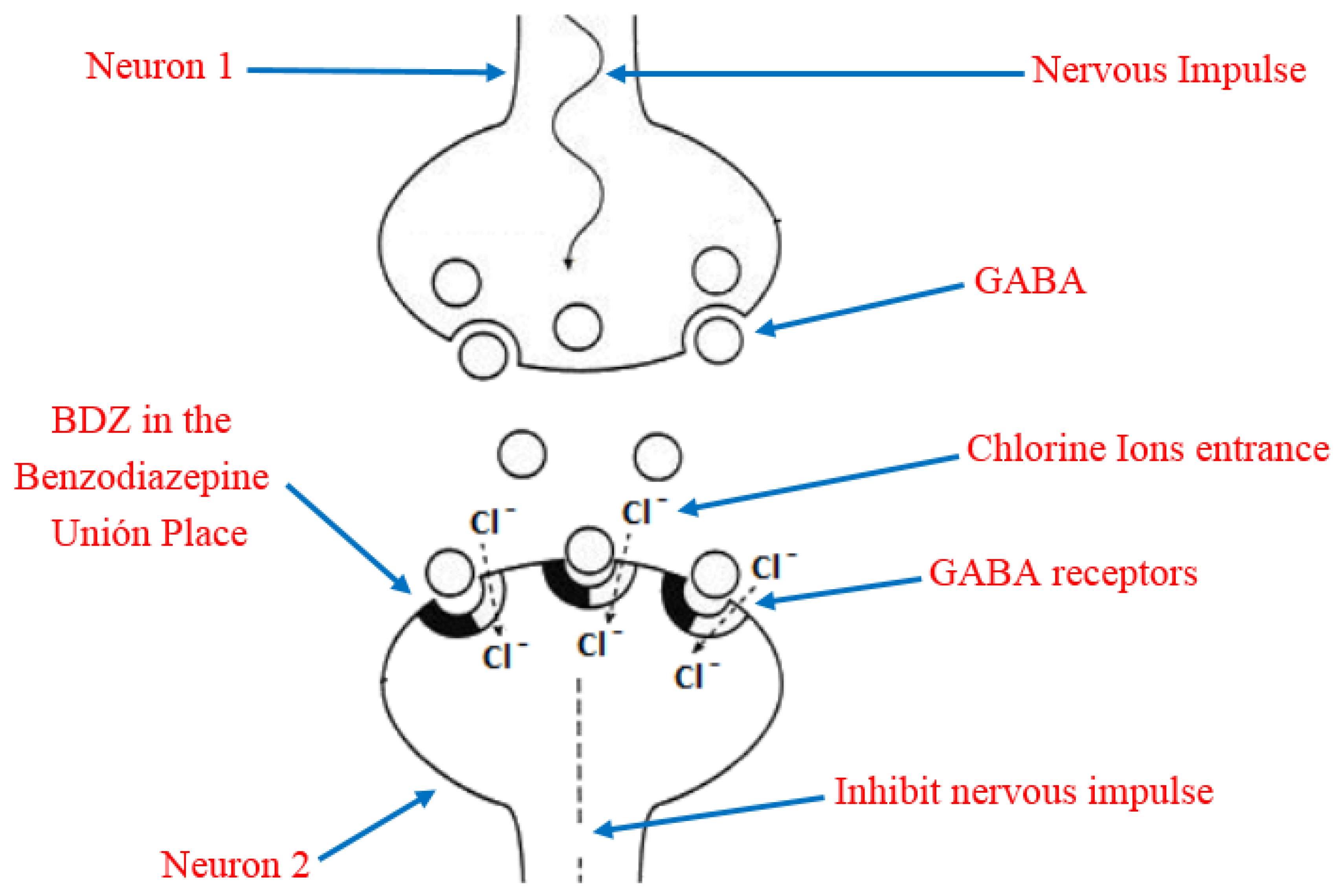
4. Benzodiazepines Action Mechanism on the Central Nervous System
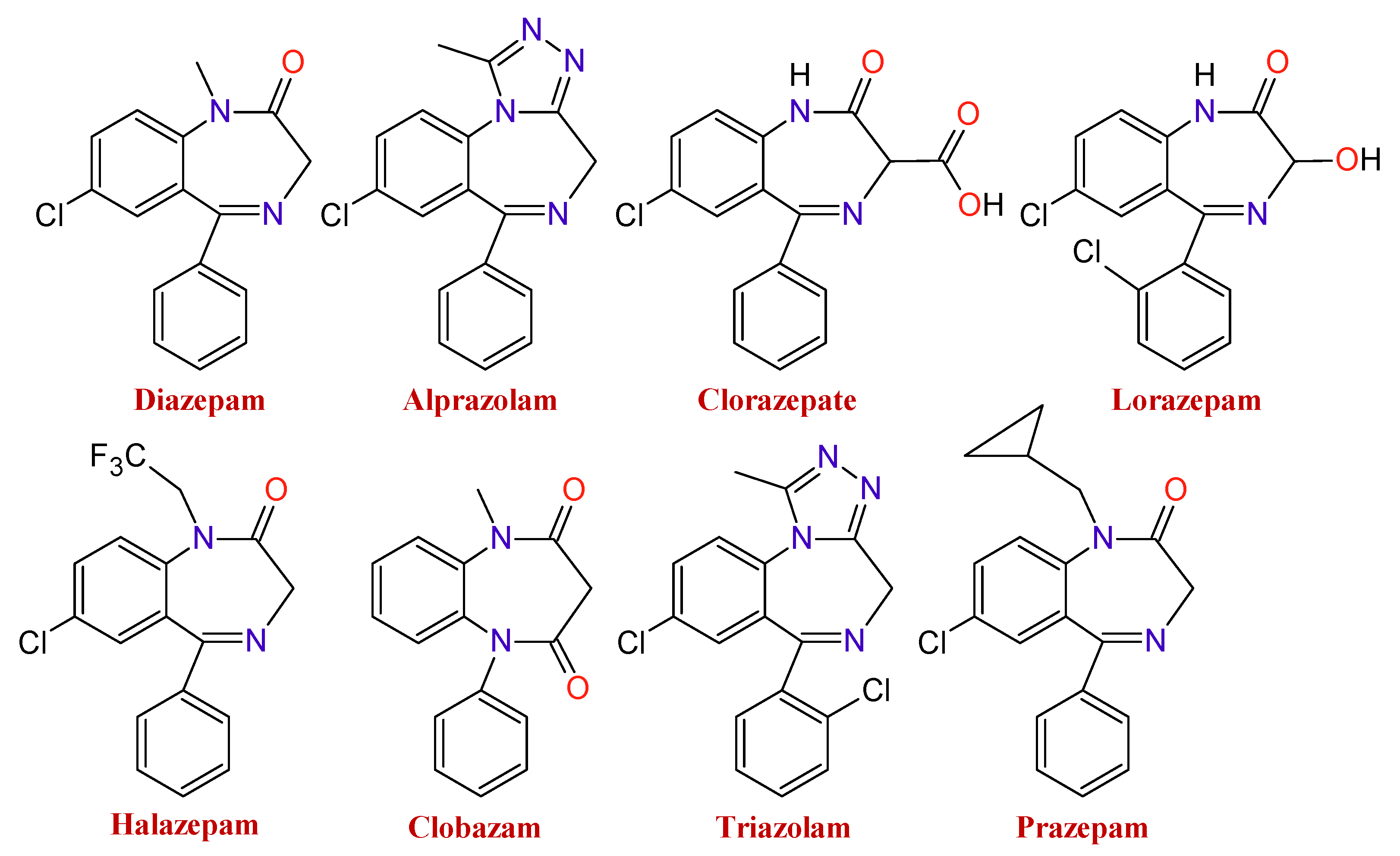
5. Pharmacological Differences between the Different Types of Benzodiazepines
6. Degradation of Benzodiazepines in the Organism
7. Toxicological Effects of Inappropriate Use of Benzodiazepines
7.1. An Essential Medicine That May Become a Weapon for the Crime
7.2. Benzodiazepines Effects on Aggressors
7.3. Suicides Mediated by Benzodiazepines
7.4. Benzodiazepines and Traffic Accidents
7.5. Adverse Effects of the Benzodiazepines Consumption by the Elderly
7.6. Adverse Effects on Pregnant Women and Newborn Children
8. Chemically Modified Benzodiazepines
9. Inadequate Use of Medicaments (Benzodiazepines) in Numbers
10. Interference with Other Medications
11. The Other Side of the Benzodiazepines
11.1. Medical Use of Benzodiazepines
11.2. Who Prescribes Benzodiazepines
11.3. Benzodiazepines Benefits
11.4. How and Why Did Benzodiazepines Start to Be Used
12. Some Efforts that Aim toward Obtaining Benzodiazepines with Less Adverse Effects in the Long-Term
13. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De, S.K.; Gibbs, R.A. Scandium (III) triflate as an efficient and reusable catalyst for synthesis of 1,5-benzodiazepinevderivatives. Tetrahedron Lett. 2005, 46, 1811–1813. [Google Scholar] [CrossRef]
- Jarikote, D.V.; Siddiqui, S.A.; Rajagopal, R.; Daniel, T.; Lahoti, R.J.; Srinivasan, K.V. Roomtemperature ionic liquid promoted synthesis of 1,5-benzodiazepine derivatives under ambient conditions. Tetrahedron Lett. 2003, 44, 1835–1838. [Google Scholar] [CrossRef]
- Jung, D.I.; Choi, T.W.; Kim, Y.Y.; Kim, I.S.; Park, Y.M.; Lee, Y.G.; Jung, D.H. Synthesis of 1,5-benzodiazepine derivatives. Synth. Commun. 1999, 29, 1941–1951. [Google Scholar]
- Pasha, M.A.; Jayashankara, V.P. Synthesis of 1,5-benzodiazepine derivatives catalyzed by zinc chloride. Heterocycles 2006, 68, 1017–1023. [Google Scholar] [CrossRef]
- Claramunt, R.M.; Sanz, D.; Aggarwal, S.; Kumar, A.; Prakash, O.; Singh, S.P.; Elgueroc, J. The reaction of o-phenylenediamine with α,β-unsaturated carbonyl compounds. Arkivoc 2006, 2006, 35–45. [Google Scholar] [CrossRef]
- An, L.-T.; Ding, F.-Q.; Zou, J.-P.; Lu, X.-H. Montmorillonite K10: An efficient catalyst forsolvent-free synthesis of 1,5-benzodiazepine derivatives. Synth. Commun. 2008, 38, 1259–1267. [Google Scholar] [CrossRef]
- Yadav, J.S.; Reddy, B.V.S.; Kumar, S.P.; Nagaiah, K. Indium(III) bromide: A novel and efficient reagent for the rapid synthesis of 1,5-benzodiazepines under solvent-free conditions. Synthesis 2005, 36, 480–484. [Google Scholar] [CrossRef]
- Kaboudin, B.; Navaee, K. Alumina/phosphorus pentoxide (APP) as an efficient reagent for the synthesis of 1,5-benzodiazepines under microwave irradiation. Heterocycles 2001, 55, 1443–1446. [Google Scholar] [CrossRef]
- Pozarentzi, M.; Stephanatou, J.S.; Tsoleridis, C.A. An efficient method for the synthesis of 1,5-benzodiazepine derivatives under microwave irradiation wihout solvent. Tetrahedron Lett. 2002, 43, 1755–1758. [Google Scholar] [CrossRef]
- Katritzky, A.R.; Xu, Y.-J.; He, H.-Y. Convenient Synthesis of 2,3,4,5-tetrahydro-1,4-benzodiazepines, 1,4-beozoxazepines and 1,4-benzotiazepines. J. Chem. Soc. Perkin Trans. 1 2002, 2, 592–598. [Google Scholar] [CrossRef]
- Ghorai, M.K.; Shahi, C.K.; Bhattacharyya, A.; Sayyad, M.; Mal, A.; Wani, I.A.; Chauhan, N. Synthesis of tetrahydrobenzodiazepines via ring-opening of activated aziridines with 2-bromoaniline Followed by Copper-Powder-Mediated C-N bond Formation. Asian J. Org. Chem. 2015, 4, 1103–1111. [Google Scholar] [CrossRef]
- Pop, T.A.; Uhl, E.; Ong, D.N.; Dittrich, S.; Bracher, F. A new appoach to monoprotected 1,4-benzodiazepines via a one pot N-deprotection/Reductive cyclization Porcedure. Tetrahedron 2016, 72, 1668–1674. [Google Scholar] [CrossRef]
- Shahi, C.K.; Bhattacharyya, A.; Nanaji, Y.; Ghorai, M.K. A stereoselective Route to tetrahydrobenzoxazepines and tetrahydrobenzodiazepines via ring-opening and Aza Michael addition of activated aziridines with 2-hydroxyphenyl and 2-aminophenyl acrylates. J. Org. Chem. 2017, 82, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Jiang, Y.; Gao, K.; Ma, D. Facile Synthesis of 1,4-benzodiazepin-3-ones from o-bromobenzylamines and amino acids via cascade coupling/condensation process. Tetrahedron 2009, 65, 8956–8960. [Google Scholar] [CrossRef]
- Clement, E.C.; Carlier, P.R. A simple route to tetrahydro-1,4-benzodiazepin-3-ones bearing diverse N1, N4, and C10 functionalization. Tetrahedron Lett. 2005, 46, 3633–3636. [Google Scholar] [CrossRef]
- Dawod, S.V.; Gerber, S.N.; Liang, X.; Biron, E. Convenient two-step synthesis of highly functionalized venzo-fused 1,4-diazepin-3-ones and 1,5-diazocin-4-ones by sequential Ugi and intramolecular SNAr reactions. Tetrahedron 2017, 73, 6347–6355. [Google Scholar] [CrossRef]
- de Silva, R.A.; Santra, S.; Andreana, P.R. A tándem one-pot microwave-assisted synthesis of regiochemically differentieted 1,2,4,5-tetrahydro-1,4-benzodiazepin-3-ones. Org. Lett. 2008, 10, 4541–4545. [Google Scholar] [CrossRef]
- Dörr, A.A.; Lubell, W.D. γ-Turn Mimicry with Benzodiazepinones and pyrrolobenzodiazepinoes synthesized from a common amino ketone intermediate. Org. Lett. 2015, 17, 3592–3595. [Google Scholar] [CrossRef]
- Mossetti, R.; Saggiorato, G.C. Tron Exploiting the acylating nature of the imide-ugi intermediate: A straightforward synthesis of tetrahydro-1,4-benzodiazepin -2-ones. J. Org. Chem. 2011, 76, 10258–10262. [Google Scholar] [CrossRef]
- Azuaje, J.; Rubio, J.M.P.; Yaziji, V.; Maatougui, A.E.; Gómez, J.C.G.; Pedregal, V.M.S.; Vásquez, A.N.; Masaguer, C.F. Integrated Ugi-Based Assembly of Functionally, Skeletally, and Stereochemically Diverse 1,4-Benzodiazepin-2-ones. J. Org. Chem. 2015, 80, 1533–1549. [Google Scholar] [CrossRef]
- Mishra, J.K.; Panda, G. A Convenient two-step synthesis of amino acid derived chiral 3-substituted [1,4]benzodiazepin-2-ones. Synthesis 2005, 11, 1881–1887. [Google Scholar] [CrossRef]
- Salomé, C.; Schmitt, M.; Bourguignon, J.-J. Novel access to 1,4-benzodiazepin-2-ones via the Buchwald reaction and application to the synthesis of novel heterocyclics. Tetrahedron Lett. 2012, 53, 1033–1035. [Google Scholar]
- Jacobson, A.F.; Goldstein, B.J.; Dominguez, R.A.; Steinbook, R.M. A placebo-controlled, double-blind comparison of clobazam and diazepam in the treatment of anxiety. J. Clin. Psychiatry 1983, 44, 296–300. [Google Scholar] [PubMed]
- Cheng, S.Z.; Fei, W.P.; Fang, W.; Xuan, X.Z.; Qiao, D.; Lei, N.T.; Qi, Z.S.; Ling, Z.H.; Hui, L.W.; Jing, L.J.; et al. Gephyrin Palmitoylation in basolateral amygdala mediates the anxiolytic action of benzodiazepine. Biol. Psychiatry 2019, 85, 202–213. [Google Scholar]
- Cornett, E.M.; Novitch, M.B.; Brunk, A.J.; Davidson, K.; Menard, B.; Urman, R.; Kaye, A.D. New benzodiazepines for sedation. Best Pract. Res. Clin. Anaesthesiol. 2018, 32, 149–164. [Google Scholar] [CrossRef] [PubMed]
- Foitzick, M.F.; Medina, N.B.; Iglesias, L.C.; Gravielle, M.C. Benzodiazepine exposure induces trnscriptional down-regulation of GABAA receptor α1 gene via L-type voltaje-gated calcium channel activation in rat cerebrocortical neurons. Neurosci. Lett. 2020, 721, 134801. [Google Scholar] [CrossRef] [PubMed]
- Ashton, H.C. Benzodiazepine abuse. Drugs Depend. 2002, 197–212. [Google Scholar]
- Gogas, K.R.; Lechner, S.M.; Markison, S.; Wlliams, J.P.; McCarthy, W.; Grigoriadis, D.E.; Foster, A.C. Anxiety. Compr. Med. Chem. II 2006, 6, 85–115. [Google Scholar]
- Skolnick, P. Anxioselective anxiolytics: On a quest for the holy grail. Trends Pharmacol. Sci. 2012, 33, 611–620. [Google Scholar] [CrossRef]
- Berro, L.F.; Rowlett, J.K. GABAA receptor subtypes and the reinforcing effects of benzodiazepines in remifentanil-experienced Rhesus monkeys. Drug Alcohol. Depend. 2020, 213, 108076. [Google Scholar] [CrossRef]
- Engin, E.; Benham, R.; Rudolph, U. An emerging circuit pharmacology of GABAA receptors. Trends Pharmacol. Sci. 2018, 39, 710–732. [Google Scholar] [CrossRef] [PubMed]
- Meng, Z.; Berro, L.; Sawyer, E.; Bettschen, D.; Cook, J.R.; Guanguan, P.; Cook, D.; James, M.; Rowlett, J. Evaluation of the anti-conflict, reinforcing, and sedative effects of YT-III-31, a ligand functionally selective for α3 subunit-containing GABAA receptors. J. Psychopharmacol. 2020, 34, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Langer, E.; Einat, H.; Stukalin, Y. Similarities and dissimilarities in the effects of benzodiazepines and specific serotonin reuptake inhibitors (SSRIs) in the defensive marble burying test: A systematic review and meta-analysis. Eur. Neuropsychopharmacol. 2020, 36, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Lechuga, G.; Indart, C. Selection of benzodiazepines: Bases for its use in the hospital. Farm. Hosp. 1996, 21, 117–122. [Google Scholar]
- Danza, A.; Cristiani, F.; Tamosiunas, G. Benzodiazepine-related risks. Arch. Med. Intern. 2009, 31, 103–107. [Google Scholar]
- Holstege, C.P. Benzodiazepines. In Encyclopedia of Toxicology, 2nd ed.; Wexler, P., Ed.; Elsevier Ltd.: Oxford, UK, 2005; Volume 1, pp. 260–262. [Google Scholar]
- Ashrafi, H.; Mobed, A.; Hasanzadeh, M.; Babaie, P.; Ansarin, K. Monitoring of five benzodiazepines using a novel polymeric interface prepared by layer by layer strategy. Microchem. J. 2019, 146, 121–125. [Google Scholar] [CrossRef]
- Pinto, J.; van Zeller, M.; Amorin, P.; Pimentel, A.; Dantas, P.; Eusebio, E.; Neves, A.; Pipa, J.; Clara, E.S.; Santiago, T.; et al. Sleep quality in times of COVID-19 pandemic. Sleep Med. 2020, 74, 81–85. [Google Scholar] [CrossRef]
- Stettin, G. America’s State of Mind Report: COVID-19 and Mental Health Medication Use. 2020. Available online: https://www.express-scripts.com/corporate/node/2332 (accessed on 21 May 2020).
- Muñoz, F.L.; Alamo, C.; Udabe, R.U.; Cuenca, E. The historical role of barbiturates in “sleep cures” for psychotic and manic disorders. Psiquiatr. Biológica 2004, 11, 242–251. [Google Scholar]
- Muñoz, F.L.; Alamo, C.; Garcia, P.G. The discovery of chlordiazepoxide and the clinical introduction of benzodiazepines: Half a century of anxiolytic drugs. J. Anxiety Disord. 2011, 25, 554–562. [Google Scholar] [CrossRef]
- World Health Organization. Model. Lists of Essential Medicines 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Boussairi, A.; Dupeyron, J.P.; Hernandez, B.; Delaitre, D.; Beugnet, L.; Espinoza, P.; Berger, O.D. Urine benzodiazepines screening of involuntarily drugged and robbed or raped patients. J. Toxicol. Clin. Toxicol. 1996, 34, 721–724. [Google Scholar] [CrossRef]
- Kraemer, T.; Maurer, H. Sedatives and hypnotic. Handb. Anal. Sep. 2008, 6, 243–286. [Google Scholar]
- Negrusz, A.; Gaensslen, R. Toxicological investigations in drug-facilitated sexual assault. Forensic Sci. 2000, 41, 7–26. [Google Scholar]
- Missliwetz, J.; Reiter, C. “Oral hygiene”-A method of killing in a medical setting. Med. Law. 1995, 14, 45–51. [Google Scholar] [PubMed]
- Ramadan, A.; Wenanu, O.; Cock, A.; Maes, V.; Lheureux, P.; Mols, P. Chemical submission to commit robbery: A series of involuntary intoxications with flunitrazepam in Asian travelers in Brussels. J. Forensic. Leg. Med. 2013, 20, 918–921. [Google Scholar] [CrossRef]
- Preliminary Investigative Report 1 October/Mass Casualty Shooting Event 1–81. Available online: https://www.reviewjournal.com/crime/homicides/read-the-final-report-from-las-vegas-police-on-the-oct-1-shooting/ (accessed on 22 May 2020).
- Daderman, A.; Fredriksson, B.; Kristianson, M.; Nilsson, L.H.; Lidberg, L. Violent behavior, impulsive decision making, and anterograde amnesia while intoxicated with flunitrazepam and alcohol or other drugs: A case study in forensic psychiatric patients. J. Am. Acad. Psychiatry Law 2003, 30, 238–251. [Google Scholar]
- Senninger, J.; Senninger, A. Crime and benzodiazepine use, abuse and dependence. Eur. Psychiatry 2017, 30, 1409. [Google Scholar] [CrossRef]
- Berecz, R.; Cáceres, M.; Szlivka, A.; Dorado, P.; Bartók, E.; LLedo, E.P.; Llerena, A.; Degrell, I. Reduced completed suicide rate in Hungary from 1990 to 2001: Relation to suicide methods. J. Affect. Disord. 2005, 88, 235–238. [Google Scholar] [CrossRef]
- Roth, T.; Roehrs, T. Efficacy and safety of sleep-promoting agents. Sleep Med. Clin. 2008, 3, 175–187. [Google Scholar] [CrossRef]
- Yaku, K.; Okabe, K.; Nakagawa, T. NAD metabolism: Implications in aging and longevity. Ageing Res. Rev. 2018, 47, 1–17. [Google Scholar] [CrossRef]
- Veler, J.; Veler, M.; Salar, L.; Avellana, J.; Moreno, L. Suitability of the use of benzodiazepines prescribed by the pharmacist in the elderly. A doctor-pharmacist collaboration study. Aten. Primaria 2012, 44, 402–410. [Google Scholar]
- Freeman, M.P.; Mogollon, L.G.; Mclnerney, K.A.; Church, T.R.; Davies, A.C.; Sosinsky, A.Z.; Noe, O.B.; Viguera, A.C.; Cohen, L.S. Obstetrical and neonatal outcomes after benzodiazepine exposure during pregnancy: Results from a prospective registry of women with psychiatric disorders. Gen. Hosp. Psychiatry 2018, 53, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Klatta, K.S.; Glebocka, M.L.; Tezyk, A.; Panienski, P.; Zaba, C.; Psuja, B.Z. Clonazolam a new designer benzodiazepine intoxication confirmed by blood concentration. Forensic Sci. Int. 2020, 310, 110237. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.; Krew, M.D.; Vazirian MD Jerry, J.; Sola, C. Novel ways to acquire designer benzodiazepines: A case report and discussion of the changing role of the internet. Psychosomatics 2019, 60, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Liu, C.; Huang, J.; Deng, Q.; Hua, Z. Identification of the designer benzodiazepine 8-chloro-6-(2-fluorophenyl)-1-methyl-4H-[1,2,4]triazolo[4,3-a][1,4] benzodiazepine (flualprazolam) in an anesthesia robbery case. Forensic Toxicol. 2020, 38, 269–276. [Google Scholar] [CrossRef]
- United Nations Office on Drugs and Crime. The Non-Medical Use of Prescription Drugs; United Nations on Drugs and Crime: Vienna, Austria, 2017. [Google Scholar]
- Jacques, B.; Gurinder, S.; Kuo, Y.; Mukaila, A.; Jordan, W.; Gulshan, S. Association of opioid and benzodazepine use with adverse respiratory events in older adults with chronic obstructive pulmonary disease. Ann. Am. Thorac. Soc. 2019, 16, 1245–1251. [Google Scholar]
- Nagatomo, K.N.; Abe, H.; Ryuji, A.; Funahashi, H.; Takeda, R.; Taniguchi, H.; Ishida, Y. A survey of the effects of ramelteon on benzodiazepine-dependence: Comparison between a ramelteon add-on group and a continuous benzodiazepine administration group. Asian J. Psychiatry 2018, 36, 20–24. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, G.K. Benzodiazepines. Am. J. Health Syst. Pharm. 1996, 53, 1694–1719. [Google Scholar]
- Lader, M. Benzodiazepines revisited-will we ever learn? Addiction 2011, 106, 2086–2109. [Google Scholar] [CrossRef]
- World Health Organization. Medicines Used in Generalized Anxiety and Sleep Disorders. In Pharmacological Treatment of Mental Disorders in Primary Health Care; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Hernández, P. Adverse Drug Reactions and Addiction to Other Substances. In Farmacología General; Rodriguez, F.G., Rodriguez, L., Eds.; Editorial Ciencias Médicas: La Habana, Cuba, 2002; pp. 70–90. [Google Scholar]
- Keun, S.; Shobha, D.; Moon, E.; Chari, M.; Mukkanti, K.; Kim, S.-H.; Ahn, K.-H.; Kim, S.Y. Anti-neuroinflammatory activity of 1,5-benzodiazepine derivatives. Bioorg. Med. Chem. Lett. 2010, 20, 3969–3971. [Google Scholar]
- Calcaterra, N.; Barrow, J. Classics in chemical neuroscience: Diazepam (Valium). ACS Chem. Neurosci. 2014, 5, 253–260. [Google Scholar] [CrossRef]
- Aronson, J.K. Meyler´s Side Effects of Drugs. In The International Encyclopedia of Adverse Drug Reactions and Interactions, 16th ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 930–937. [Google Scholar]
- March, K.L.; Twilla, J.D.; Reaves, A.B.; Self, M.M.S.; Bergeron, J.B.; Sakaan, S.A. Lorazepam versus chlordiazepoxide for the treatment of alcohol withdrawal syndrome and prevention of delirium tremens in general medicine ward patients. Alcohol 2019, 81, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Syed, A.; Guru, G.; Jaisoorya, T.S.; Suresh, M. Resurgense of catatonia following tapering or stoppage of lorazepam case series and implications. Asian J. Psychiatry 2017, 28, 102–105. [Google Scholar]
- Nelson, A.C.; Kehoe, J.; Sankoff, J.; Mintzer, D.; Taub, J.; Kaucher, K. Benzodiazepines vs barbiturates for alcohol withdrawal: Analysis of 3 different treatment protocols. Am. J. Emerg. Med. 2019, 37, 733–736. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, L.-N. Baclofen for alcohol withdrawal. Cochrane Syst. Rev. 2019, 008502. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.C.; Di Filippo, C.; Enjuanes, F. Diagnosis and treatment of catatonia: Presentation of a case. Psiquiatr. Biol. 2013, 20, 40–43. [Google Scholar] [CrossRef]
- Massah, A.R.; Gharaghani, S.; Lordejani, H.A.; Asakere, N. New and mild method for the synthesis of alprazolam and diazepam and computational study of their binding mode to GABAA receptor. Med. Chem. Res. 2016, 25, 1538–1550. [Google Scholar] [CrossRef]
- Mendoca, J.; Scotti, L.; Ishiki, H.; Botelho, S.P.S.; Da Silva, M.S.; Scotti, M.T. Benzo-and thienobenzo-diazepines:multitarget drugs for CNS disorders. Mini Rev. Med. Chem. 2015, 15, 630–647. [Google Scholar]
- Frias, A.; Fernades, G.; Zangrossi, H. GABAA/benzodiazepine receptors in the dorsal periaqueductal gray mediate the panicolytic but not the anxiolytic effect of alprazolam in rats. Behav. Brain Res. 2019, 364, 99–105. [Google Scholar] [CrossRef]
- Perna, G.; Dacco, S.; Menotti, R.; Caldirola, D. Antianxiety medications for the treatment of compex agoraphobia: Pharmacological interventions for a behavioral condition. Neuropsychiatr. Dis. Treat. 2011, 7, 621–637. [Google Scholar]
- Bolli, M.H.; Marfurt, J.; Grisostomi, C.; Boss, C.; Binlcert, C.; Hess, P.; Treiber, E.; Thorin, A.; Morrison, K.; Buchmann, S.; et al. Novel benzo [1,4] diazepin-2-one derivatives as endothelin receptor antagonists. J. Med. Chem. 2004, 47, 2776–2795. [Google Scholar] [CrossRef]
- Alprazolam (Xanax, and others) revisited. Med. Lett. Drugs Ther. 2005, 47, 5–7.
- Kumar, N.; Rao, S.; Kumar, S.; Kumar, P. Potential impurities of anxiolytic drug, clobazam: Identification, synthesis and characterization using HPLC, LC-ESI/MSn and NMR. J. Pharmaceut. BioMed 2017, 137, 268–278. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, M.M. Overview of drugs used for epilepsy and seizures. Etiology, diagnosis and treatment. Pharm. Ther. 2010, 35, 392–415. [Google Scholar]
- Gauthier, A.C.; Mattson, R.H. Clobazam: A safe, efficacious, and newly rediscovered therapeutic for epilepsy. Neurosci. Ther. 2015, 21, 543–548. [Google Scholar] [CrossRef]
- Nakajima, H. A pharmacological profile of clobazam (Mystan), a new antiepileptic drug. Folia Pharmacol. Japon. 2001, 118, 117–122. [Google Scholar] [CrossRef][Green Version]
- Redondo, P.; Vicente, J.; España, A.; Subira, M.; De Felipe, I.; Quintanilla, E. Photo-induced toxic epidermal necrolysis caused by clobazam. Br. J. Dermatol. 1996, 135, 999–1002. [Google Scholar] [CrossRef]
- Menezes, C.M.S.; Rivera, G.; Alves, M.A.; do Amaral, D.N.; Thibaut, J.P.; Barreiro, E.J.; Lima, L.M. Synthesis, biological evaluation, and structure-activity relationship of clonazepam, meclonazepam, and 1,4-benzodiazepine compounds with schistosomicidal activity. Chem. Biol. Drug. Des. 2012, 79, 943–949. [Google Scholar] [CrossRef]
- Toth, K.; Csukly, G.; Sirok, D.; Belic, A.; Kiss, A.; Hafra, E.; Deri, M.; Menus, A.; Bitter, I.; Monostory, K. Optimization of clonazepam therapy adjusted to patient’s CYP3A status and NAT2” genotype. Int. J. Neuropsychopharmacol. 2016, 19, pyw083. [Google Scholar] [CrossRef]
- Min, W.S.; Bun, K.J.; Jeong, S.; Suk, S.H.; Kang, S.; Min, W.J.; Woo, Y.S.; San, L.; Yeol, L.S.; Won, L.S.; et al. The efficacy and safety of clonazepam in patients with anxiety disorder taking newer antidepressants: A multicenter naturalistic study. Clin. Psychopharmacol. Neurosci. 2016, 14, 177–183. [Google Scholar]
- Sirajul, I.; Banik, D.; Akhtaruzzaman, A.; Chandra, P.; Mesbahuddin, K. Use of oral bromazepam as premedicant and its effects in peri-operative period-A comparative study with oral diazepam. J. BSA 2005, 18, 22–30. [Google Scholar]
- Attia, M.S. Spectrofluorimetric quantification of bromazepam using a highly selective optical probe based on Eu3+-bromazepam complex in pharmaceutical and serum samples. Spectrochim. Acta Part A 2009, 74, 972–976. [Google Scholar] [CrossRef] [PubMed]
- Minc, D.; Machado, S.; Bastos, V.; Machado, D.; Cunha, M.; Cagy, M.; Budde, H.; Basile, L.; Piedade, R.; Ribeiro, P. Gamma band oscillations under influence of bromazepam during a sensorimotor integration task: An EEG coherence study. Neurosci. Lett. 2010, 469, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Bohorquez, A.; Gomez, C.; Garcia, V.; Jaramillo, L.E.; de la Hoz, A.M.; Arenas, A.; Tamayo, N. Antipsychotic treatment of the adult patient in the acute phase of Schizophrenia. Rev. Col. Psiquiatr. 2014, 44, 13–28. [Google Scholar]
- Fortunato, S.; Guaraci, K.; Assis, F.; Bittencourt, J.; Aprigio, D.; Gongora, M.; Teixeira, S.; Monteiro, F.; Cagy, P.; Hindi, L.F.; et al. The effects of bromazepam over the central and frontal areas during a motor task: An EEG study. Arq. Neuro Psiquiatr. 2015, 73, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Puga, F.; Veiga, H.; Cagy, M.; McDowell, K.; Piedade, R.; Ribeiro, P. Analysis of the influence of bromazepam on cognitive performance through the visual evoked potential (P300). Arq. Neuro Psiquiatr. 2005, 63, 228–234. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Murphy, S. A double-blind comparison of the effects of gradual withdrawal of lorazepam, diazepam and bromazepam in benzodiazepine dependence. Br. J. Psychiatry 1991, 158, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Ulusoy, E.; Duman, M.; Didem, H.; Caglar, A.; Er, A.; Akgul, F.; Citlenbik, H.; Ozturk, A.; Yilmaz, D. The effect of early midazolam infusion on the duration of pediatric status epilepticus patients. Seizure Eur. J. Epilep. 2019, 71, 50–55. [Google Scholar] [CrossRef]
- Li, S.-P.; Zhou, X.-L.; Zhao, Y. Sedation with midazolam worsens the diaphragm function than dexmedetomidine and propofol during mechanical ventilation in rats. BioMed Pharmacother. 2020, 121, 109405–109414. [Google Scholar] [CrossRef] [PubMed]
- Epilepsy Society. List of Anti-Epileptic Drugs. Available online: https://www.epilepsysociety.org.uk/list-anti-epileptic-drugs (accessed on 14 July 2020).
- Rech, M.; Barbas, B.; Chaney, W.; Greenhalgh, E.; Turck, C. When to pick the nose: Out-of-hospital and emergency department intranasal Administration of medications. Ann. Emerg. Med. 2017, 70, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, T.; Maurer, H. Sedatives and hypnotic. Handb. Anal. Sep. 2000, 2, 197–227. [Google Scholar]
- Druid, H.; Holmgren, P.; Ahlner, J. Flunitrazepam: An evaluation of use, abuse and toxicity. Forensic Sci. Int. 2001, 122, 136–141. [Google Scholar] [CrossRef]
- Aronson, J.K. Meyler’s Side Effects of Drugs. In The International Encyclopedia of Adverse Drug Reactions and Interactions, 16th ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 364–681. [Google Scholar]
- Bruce, S.E.; Vasile, R.G.; Goisman, R.M. Are benzodiazepines still the medication of choice for patients with panic disorder with or without agoraphobia? Am. J. Psychiatry 2003, 160, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Liégeois, J.F.; Bruhwyler, J.; Damas, J.; Nguyen, T.P.; Chleide, E.M.; Mercier, M.G.; Rogister, F.A.; Delarge, J.E. New pyridobenzodiazepine derivatives as potential antipsychotics: Synthesis and neurochemical study. J. Med. Chem. 1993, 36, 2107–2114. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, I.R.; Arceo, K.S.; Mercado, F. Cellular and molecular mechanism of the boenzodiazepines addiction. Salud Ment. 2013, 36, 325–329. [Google Scholar]
- Cherif, W.B.; Gharbi, R.; Sebai, H.; Dridi, D.; Boughattas, N.A.; Attia, M.B. Neuropharmacological screening of two 1,5-benzodiazepine compounds in mice. C. R. Biol. 2010, 333, 214–219. [Google Scholar] [CrossRef]
- Guerrero, F.A.; Reyna, L.V.; Taboada, J.; Martinez, E.; Cortés, E. Effect of a derivative of 1,5-benzodiazepine on slepp. Gac. Med. Mex. 1990, 126, 519–522. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Benzodiazepine Name | Some Medical Use | Other Medicines Used for the Same Purpose | Advantages and Disadvantages of Benzodiazepines |
|---|---|---|---|
| Diazepam | Anxiety disorders, epilepsy, alcohol withdrawal symptoms (AWS), muscle spasms [67] | Fluoxetina (Prozac, Sarafem, Fontex), Escitalopram (Lexapro), Paroxetina (Paxil) (selective serotonin reuptake inhibitors) [67] | The clinical efficacy of Diazepam is recognized because it rapidly reaches its potency of action, by its safety, and high bioavailability. Among its disadvantages is that it can cause urinary retention and compartment syndrome [68] |
| Lorazepam | Treatment of alcohol withdrawal symptoms (AWS) [69], treatment of catatonia [70] | Benzodiazepines are the standard although other alternative agents as phenobarbital also are used frequently for the treatment of AWS [71,72], whereas for catatonia, electroconvulsive therapy is usually used [73] | Lorazepam is attractive for treatment of AWS because it is likely to accumulate in liver less than other substances [69]. For the treatment of catatonia, Lorazepam is considered safe and effective (recovery rates >80%). Independent of the blood concentration, the lorazepam can cause significant impairment of driving and psychomotor abilities [68] |
| Alprazolam | Treatment of panic disorder (PD), agoraphobia [74], and depression [75]. In addition, it is used as an anxiolytic agent | For PD, fluoxetine and escitalopram (selective serotonin reuptake inhibitors) are also used [76]. For agoraphobia, the treatment with paroxetine, sertraline, citalopram, escitalopram, and clomipramine showed good results [77] | Alprazolam is a high potency BDZ and, due to its effectiveness, it is the most widely used in the pharmacological treatment of panic disorders [76]. It has a recognized efficacy for the treatment of agoraphobia [78]. Its disadvantages include sedation, withdrawal symptoms, and abuse [79] |
| Clobazam | It is used as anxiolytic, anticonvulsant and antiepileptic agent [80] | In the treatment of seizures valproic acid, lamotrigine, and topiramate, among others, are used [81] | Clobazam has shown great efficacy and high safety in the treatment of refractory epilepsy in both children and adults; in general, it has shown great benefits for epileptic patients [82]. Moreover, Clobazam (1,5-benzodiazepine) exhibits a better pharmacological profile in both short and long-term seizures treatments than 1,4-benzodiazepine [83]. One case of photo-induced toxic epidermal necrolysis caused by clobazam was reported [84] |
| Clonazepam | Treatment of schistosomiasis, a disease considered to be a serious public health problem [85] | Praziquantel can also be used to treat schistosomiasis, although its use can cause resistance to parasites [85] | Methyl-clonazepam has a schistosomicidal effect in humans and could be an alternative to Praziquantel [85], but it can cause adverse effects on the central nervous systems derived from differences in Clonazepam metabolism [86]. Among the adverse effects is that it can cause drowsiness [87] |
| Bromazepam | Bromazepam is a BDZ used clinically as anxiolytic [88,89,90] | Dexmedetomidine is a pharmacological option as an anxiolytic to bromazepam [91] | Studies on psychiatric patients suggest that it is better as anxiolytic than diazepam and lorazepam [88]. In addition, it does not produce negative effects on cognitive and motor response [92,93]. Its main point again is that it produces dependency [94] |
| Midazolam | Midazolam is used for the treatment of the epileptic state [95] and as a sedative [96] | For the treatment of epilepsy, Sodium Valproate, Cannabidiol, Ethosuximide, Lamotrigine, among others, can also be used [97] | The use of Midazolam for the treatment of epilepsy is associated with a shorter seizure duration [95]. Some adverse effects of intranasal medication are nasal burning and bitter taste [98] |
| Flunitrazepam | The use of Flunitrazepam is licensed in Europe, Asia, and Latin America for the treatment of insomnia, as pre-anesthetic and as sedative-hypnotic agent. Nevertheless, its use has not been approved in the U.S. [98] | Other drugs used as hypnotic-sedatives are Barbiturates, Diphenhydramine and receptor agonists such as Zopiclone, Zolpidem, Zaleplon, and Eszopiclone [99] | Flunitrazepam has no advantages over other BDZs. However, it is very popular among alcohol and drug abusers and it may produce violent behaviors [100] including being implicated in sexual assault [101] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanabria, E.; Cuenca, R.E.; Esteso, M.Á.; Maldonado, M. Benzodiazepines: Their Use either as Essential Medicines or as Toxics Substances. Toxics 2021, 9, 25. https://doi.org/10.3390/toxics9020025
Sanabria E, Cuenca RE, Esteso MÁ, Maldonado M. Benzodiazepines: Their Use either as Essential Medicines or as Toxics Substances. Toxics. 2021; 9(2):25. https://doi.org/10.3390/toxics9020025
Chicago/Turabian StyleSanabria, Edilma, Ronald Edgardo Cuenca, Miguel Ángel Esteso, and Mauricio Maldonado. 2021. "Benzodiazepines: Their Use either as Essential Medicines or as Toxics Substances" Toxics 9, no. 2: 25. https://doi.org/10.3390/toxics9020025
APA StyleSanabria, E., Cuenca, R. E., Esteso, M. Á., & Maldonado, M. (2021). Benzodiazepines: Their Use either as Essential Medicines or as Toxics Substances. Toxics, 9(2), 25. https://doi.org/10.3390/toxics9020025