
Spatiotemporal Patterns of Indoor Air Pollution and Its Association with Depressive Symptoms Among Schoolchildren in China

 , , , , , and
, , , , , and 
Abstract

1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements of Indoor Exposure to Air Pollutants
2.3. Assessment of Depressive Symptoms
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics of the Participants
3.2. Levels of Exposure to Seven Indoor Environmental Factors Cross Different Exposure Settings and Time Periods
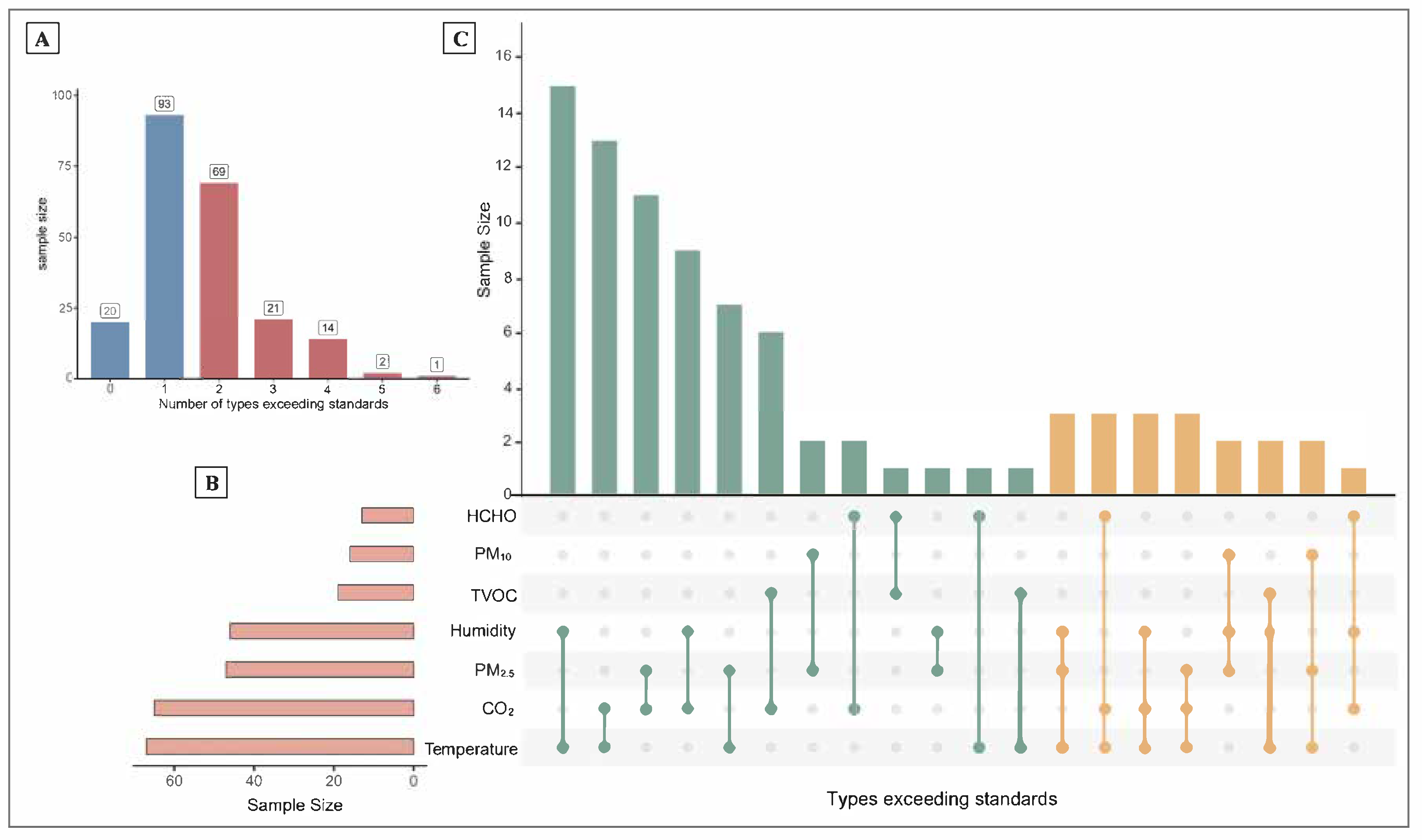
3.3. Distribution of Types of Exceedances Among Seven Indoor Environmental Indicators
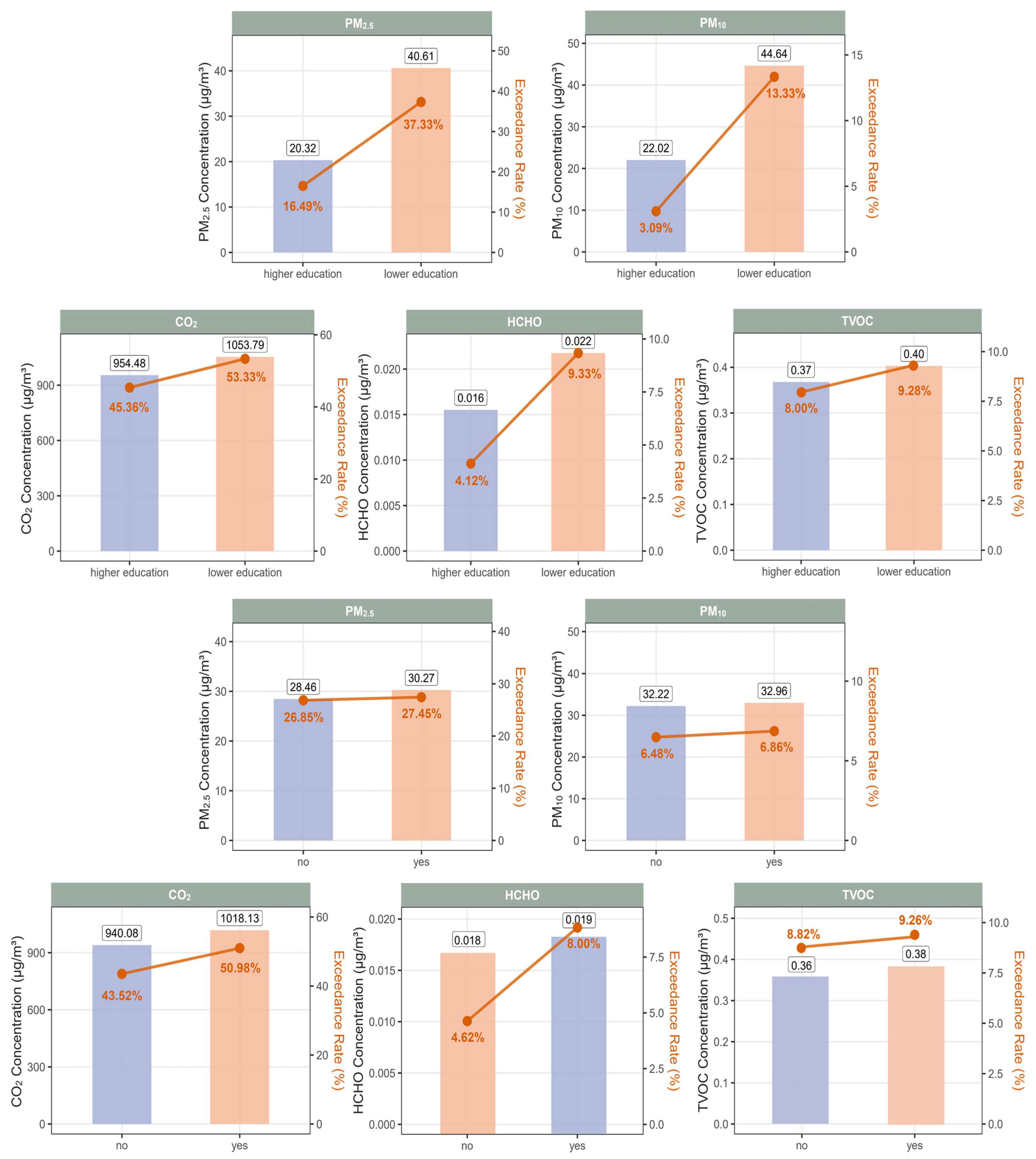
3.4. Levels of Exposure to Seven Indoor Environmental Factors Across Different Subgroups
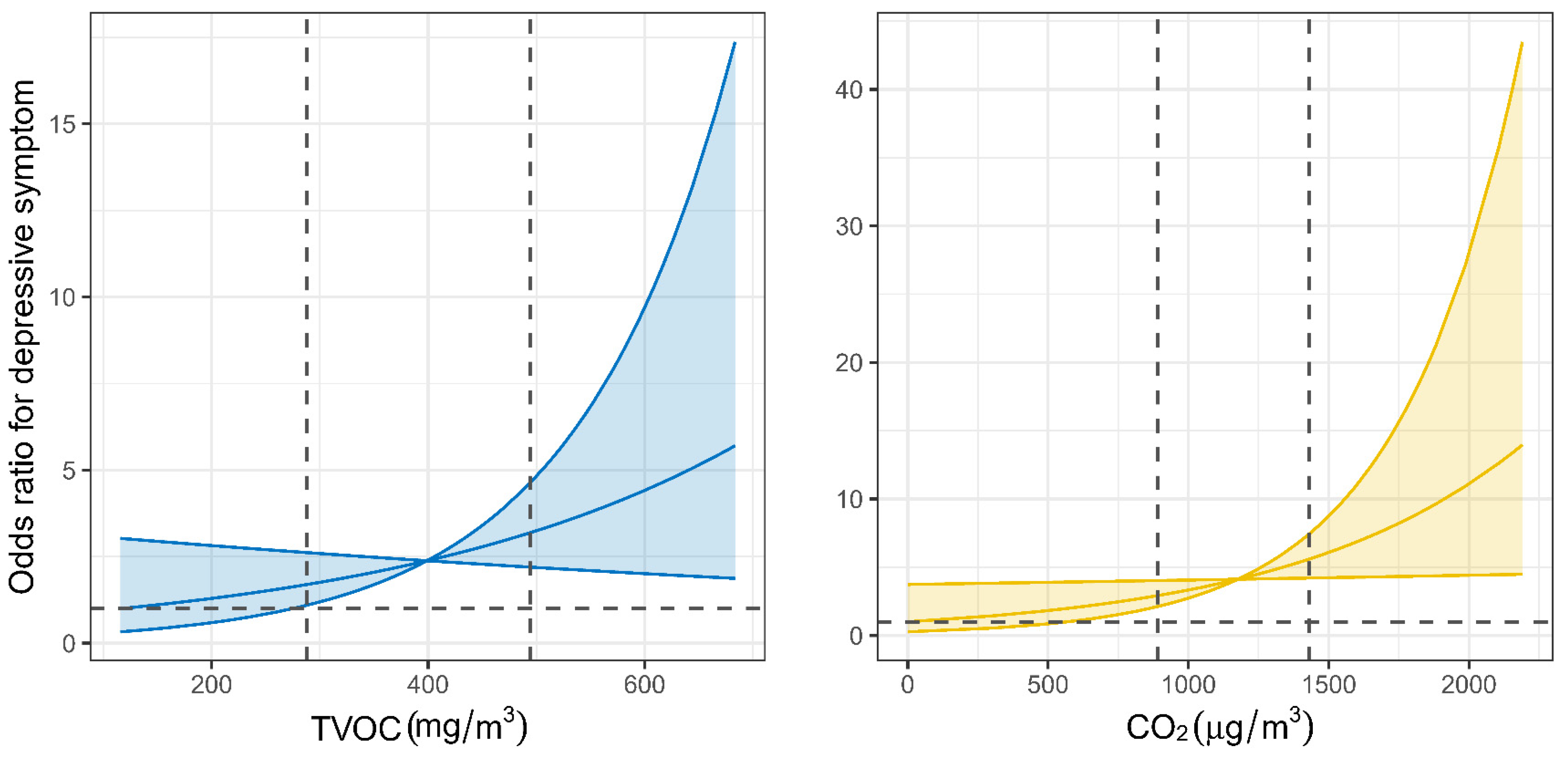
3.5. Association of Exposure to Five Indoor Air Pollutants with Depressive Symptoms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bozkurt, Z.; Doğan, G.; Arslanbaş, D.; Pekey, B.; Pekey, H.; Dumanoğlu, Y.; Bayram, A.; Tuncel, G. Determination of the personal, indoor and outdoor exposure levels of inorganic gaseous pollutants in different microenvironments in an industrial city. Environ. Monit. Assess. 2015, 187, 590. [Google Scholar] [CrossRef]
- Branco, P.T.; Alvim-Ferraz, M.C.; Martins, F.G.; Sousa, S.I. The microenvironmental modelling approach to assess children’s exposure to air pollution—A review. Environ. Res. 2014, 135, 317–332. [Google Scholar] [CrossRef]
- Rivas, I.; Donaire-Gonzalez, D.; Bouso, L.; Esnaola, M.; Pandolfi, M.; de Castro, M.; Viana, M.; Àlvarez-Pedrerol, M.; Nieuwenhuijsen, M.; Alastuey, A.; et al. Spatiotemporally resolved black carbon concentration, schoolchildren’s exposure and dose in Barcelona. Indoor Air 2016, 26, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.T.; Li, X.M.; Liu, E.M.; Xiong, W.K.; Wang, S.; Zhu, R.; Ding, Y.B.; Zhong, Z.H. Associations of early-life factors and indoor environmental exposure with asthma among children: A case-control study in Chongqing, China. World J. Pediatr. 2022, 18, 186–195. [Google Scholar] [CrossRef]
- Liu, S.; Huang, Q.; Chen, C.; Song, Y.; Zhang, X.; Dong, W.; Zhang, W.; Zhao, B.; Nan, B.; Zhang, J.; et al. Joint effect of indoor size-fractioned particulate matters and black carbon on cardiopulmonary function and relevant metabolic mechanism: A panel study among school children. Environ. Pollut. 2022, 307, 119533. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Bagkeris, E.; Mumovic, D. The combined impacts of indoor temperature and total volatile organic compounds on cognitive performance of university students: A controlled exposure study. Sci. Total Environ. 2025, 966, 178652. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Lian, X.; Wang, Y.; Wang, H.; Guo, J.; Tang, Z.; Shi, D.; Song, Y.; Zou, Z.; Chen, Y.; et al. Short-term exposure to PM2.5 and high pollution events on depressive symptoms among adolescents. J. Hazard. Mater. 2025, 492, 138131. [Google Scholar] [CrossRef]
- Zundel, C.G.; Ryan, P.; Brokamp, C.; Heeter, A.; Huang, Y.; Strawn, J.R.; Marusak, H.A. Air pollution, depressive and anxiety disorders, and brain effects: A systematic review. Neurotoxicology 2022, 93, 272–300. [Google Scholar] [CrossRef]
- Cui, X.; Li, Z.; Teng, Y.; Barkjohn, K.K.; Norris, C.L.; Fang, L.; Daniel, G.N.; He, L.; Lin, L.; Wang, Q.; et al. Association Between Bedroom Particulate Matter Filtration and Changes in Airway Pathophysiology in Children with Asthma. JAMA Pediatr. 2020, 174, 533–542. [Google Scholar] [CrossRef]
- He, L.; Li, Z.; Teng, Y.; Cui, X.; Barkjohn, K.K.; Norris, C.; Fang, L.; Lin, L.; Wang, Q.; Zhou, X.; et al. Associations of personal exposure to air pollutants with airway mechanics in children with asthma. Environ. Int. 2020, 138, 105647. [Google Scholar] [CrossRef]
- He, L.; Norris, C.; Cui, X.; Li, Z.; Barkjohn, K.K.; Brehmer, C.; Teng, Y.; Fang, L.; Lin, L.; Wang, Q.; et al. Personal Exposure to PM2.5 Oxidative Potential in Association with Pulmonary Pathophysiologic Outcomes in Children with Asthma. Environ. Sci. Technol. 2021, 55, 3101–3111. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Hama, S.; Abbass, R.A.; Nogueira, T.; Brand, V.S.; Wu, H.-W.; Abulude, F.O.; Adelodun, A.A.; de Fatima Andrade, M.; Asfaw, A.; et al. CO2 exposure, ventilation, thermal comfort and health risks in low-income home kitchens of twelve global cities. J. Build. Eng. 2022, 61, 105254. [Google Scholar] [CrossRef]
- Guo, J.; Garshick, E.; Si, F.; Tang, Z.; Lian, X.; Wang, Y.; Li, J.; Koutrakis, P. Environmental Toxicant Exposure and Depressive Symptoms. JAMA Netw. Open 2024, 7, e2420259. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Ohtani, K.; Imajo, A.; Izu, H.; Nakamura, H.; Shiraishi, K. Comparison of the neurotoxicities between volatile organic compounds and fragrant organic compounds on human neuroblastoma SK-N-SH cells and primary cultured rat neurons. Toxicol. Rep. 2015, 2, 729–736. [Google Scholar] [CrossRef]
- GB/T 18883–2022; Standards for Indoor Air Quality. Standardization Administration of China, State Administration for Market Regulation of China: Beijing, China, 2022.
- Wang, X.; Dang, J.; Liu, J.; Liu, Y.; Wang, Y.; Shi, D.; Chen, Z.; Yuan, W.; Cai, S.; Mi, J.; et al. A cluster randomized trial of a comprehensive intervention nesting family and clinic into school centered implementation to reduce myopia and obesity among children and adolescents in Beijing, China: Study protocol. BMC Public Health 2023, 23, 1435. [Google Scholar] [CrossRef] [PubMed]
- T/CECS 698-2020; Performance Test Standard of Measurement Device for Indoor PM2.5 Concentration. Professional Committee on Building Environment and Energy Conservation, China Engineering Construction Standardization Association: Beijing, China, 2020.
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Beekman, A.T.F.; Deeg, D.J.H.; Van Limbeek, J.; Braam, A.W.; De Vries, M.Z.; Van Tilburg, W. BRIEF COMMUNICATION.: Criterion validity of the Center for Epidemiologic Studies Depression scale (CES-D): Results from a community-based sample of older subjects in the Netherlands. Psychol. Med. 1997, 27, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.F.; Liu, Z.J.; Ouyang, S.; Dong, Q.; Yan, W.J.; Xu, D.W. Machine learning-driven development of a stratified CES-D screening system: Optimizing depression assessment through adaptive item selection. BMC Psychiatry 2025, 25, 286. [Google Scholar] [CrossRef]
- Huang, F.; Wang, Y.; Xue, H.; Zhang, X.; Tian, Y.; Du, W.; Fan, L.; Yang, J. Are Rural–Urban Differences in Bullying and Poly-Bullying Victimization Associated with Internet Addiction or Depressive Symptoms among Adolescents in Jiangsu Province of China. Future 2024, 2, 1–15. [Google Scholar] [CrossRef]
- Dardas, L.A.; Xu, H.; Shawashreh, A.; Franklin, M.S.; Wainwright, K.; Pan, W. Psychometric Properties and Factor Structure of the Center for Epidemiologic Studies Depression Scale in a National Sample of Arab Adolescents. Issues Ment. Health Nurs. 2019, 40, 437–443. [Google Scholar] [CrossRef]
- Kandola, A.; Lewis, G.; Osborn, D.P.J.; Stubbs, B.; Hayes, J.F. Depressive symptoms and objectively measured physical activity and sedentary behaviour throughout adolescence: A prospective cohort study. Lancet Psychiatry 2020, 7, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Zhang, E.; Chen, J.; Liu, Y.; Li, H.; Li, Y.; Kuwahara, K.; Xiang, M. Associations between joint lifestyle behaviors and depression among children and adolescents: A large cross-sectional study in China. J. Affect. Disord. 2024, 352, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Chang, F.C.; Chiu, C.H.; Chen, P.H.; Chiang, J.T.; Miao, N.F.; Chuang, H.Y.; Huang, W.Q.; Tseng, C.C. Smartphone addiction and victimization predicts sleep problems and depression among children. J. Pediatr. Nurs. 2022, 64, e24–e31. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, A.; Quirk, S.E.; Housden, S.; Brennan, S.L.; Williams, L.J.; Pasco, J.A.; Berk, M.; Jacka, F.N. Relationship between diet and mental health in children and adolescents: A systematic review. Am. J. Public Health 2014, 104, e31–e42. [Google Scholar] [CrossRef]
- Marino, C.; Andrade, B.; Campisi, S.C.; Wong, M.; Zhao, H.; Jing, X.; Aitken, M.; Bonato, S.; Haltigan, J.; Wang, W.; et al. Association Between Disturbed Sleep and Depression in Children and Youths: A Systematic Review and Meta-analysis of Cohort Studies. JAMA Netw. Open 2021, 4, e212373. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 14 July 2022).
- Fromme, H.; Twardella, D.; Dietrich, S.; Heitmann, D.; Schierl, R.; Liebl, B.; Rüden, H. Particulate matter in the indoor air of classrooms—Exploratory results from Munich and surrounding area. Atmos. Environ. 2007, 41, 854–866. [Google Scholar] [CrossRef]
- Andamon, M.M.; Rajagopalan, P.; Woo, J. Evaluation of ventilation in Australian school classrooms using long-term indoor CO2 concentration measurements. Build. Environ. 2023, 237, 110313. [Google Scholar] [CrossRef]
- Stinson, B.; Laguerre, A.; Gall, E.T. Per-Person and Whole-Building VOC Emission Factors in an Occupied School with Gas-Phase Air Cleaning. Environ. Sci. Technol. 2022, 56, 3354–3364. [Google Scholar] [CrossRef]
- Molinier, B.; Arata, C.; Katz, E.F.; Lunderberg, D.M.; Ofodile, J.; Singer, B.C.; Nazaroff, W.W.; Goldstein, A.H. Bedroom Concentrations and Emissions of Volatile Organic Compounds during Sleep. Environ. Sci. Technol. 2024, 58, 7958–7967. [Google Scholar] [CrossRef]
- Zhang, D.; Bluyssen, P.M. Exploring the possibility of using CO2 as a proxy for exhaled particles to predict the risk of indoor exposure to pathogens. Indoor Built Environ. 2022, 32, 1958–1972. [Google Scholar] [CrossRef]
- Arendt, J.N.; Christensen, M.L.; Hjorth-Trolle, A. Maternal education and child health: Causal evidence from Denmark. J. Health Econ. 2021, 80, 102552. [Google Scholar] [CrossRef] [PubMed]
- Green, C.M.; Berkule, S.B.; Dreyer, B.P.; Fierman, A.H.; Huberman, H.S.; Klass, P.E.; Tomopoulos, S.; Yin, H.S.; Morrow, L.M.; Mendelsohn, A.L. Maternal literacy and associations between education and the cognitive home environment in low-income families. Arch. Pediatr. Adolesc. Med. 2009, 163, 832–837. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, L.; Taylor, J.; Davies, M.; Shrubsole, C.; Symonds, P.; Dimitroulopoulou, S. Exposure to indoor air pollution across socio-economic groups in high-income countries: A scoping review of the literature and a modelling methodology. Environ. Int. 2020, 143, 105748. [Google Scholar] [CrossRef]
- Elia, E.A.; Stylianou, M.; Agapiou, A. Investigation on the source of VOCs emission from indoor construction materials using electronic sensors and TD-GC-MS. Environ. Pollut. 2024, 348, 123765. [Google Scholar] [CrossRef]
- Liu, X.; Buddhi, P.; Rohan, J.; Phong, T.; Bryce, C.; Isak, Z.; Riki, L.; Matthew, D.; Hao, W.; Jian, G.; et al. Response of low-cost sensors to high PM2.5 concentrations during bushfire and haze events. Aerosol Sci. Technol. 2024, 58, 978–990. [Google Scholar] [CrossRef]
- Williams, C.R.; Dittman, A.H.; McElhany, P.; Busch, D.S.; Maher, M.T.; Bammler, T.K.; MacDonald, J.W.; Gallagher, E.P. Elevated CO2 impairs olfactory-mediated neural and behavioral responses and gene expression in ocean-phase coho salmon (Oncorhynchus kisutch). Glob. Change Biol. 2019, 25, 963–977. [Google Scholar] [CrossRef]
- Yoon, S.; Zuccarello, M.; Rapoport, R.M. pCO2 and pH regulation of cerebral blood flow. Front. Physiol. 2012, 3, 365. [Google Scholar] [CrossRef]
- Gao, C.; Zhao, X.; Li, T. Effects of indoor VOCs from paint on human brain activities during working memory tasks: An electroencephalogram study. Indoor Air 2022, 32, e13062. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, J.; Wang, J.; Guo, D.; Pei, J.; Zhao, L.; Zhang, X.; Liu, J.; Li, Y.; Deng, M.; et al. Effect of low concentrations of indoor toluene on cognitive performance: EEG-based evidence. Build. Environ. 2022, 224, 109494. [Google Scholar] [CrossRef]
- López, L.R.; Dessì, P.; Cabrera-Codony, A.; Rocha-Melogno, L.; Kraakman, B.; Naddeo, V.; Balaguer, M.D.; Puig, S. CO2 in indoor environments: From environmental and health risk to potential renewable carbon source. Sci. Total Environ. 2023, 856, 159088. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (N = 219) |
|---|---|
| Age, mean ± SD | 9.9 ± 2.1 |
| Sex, n (%) | |
| Boys | 115 (52.5%) |
| Girls | 104 (47.5%) |
| Grade, n (%) | |
| Grade 1 | 9 (4.1%) |
| Grade 2 | 38 (17.4%) |
| Grade 3 | 45 (20.5%) |
| Grade 4 | 53 (24.2%) |
| Grade 7 | 74 (33.8%) |
| District, n (%) | |
| Dongcheng | 27 (12.3%) |
| Tongzhou | 121 (55.3%) |
| Changping | 71 (32.4%) |
| Season a, n (%) | |
| Warm | 121 (55.3%) |
| Cool | 98 (44.7%) |
| Maternal education, n (%) | |
| Bachelor’s degree or above | 97 (44.3%) |
| High school or below | 75 (34.2%) |
| Unknown | 47 (21.5%) |
| Home decoration within one year, n (%) | |
| Yes | 75 (34.2%) |
| No | 132 (60.3%) |
| Unknown | 12 (5.5%) |
| Exposure | Units | Mean ± SD | Median (Q25–Q75) | Min | Max |
|---|---|---|---|---|---|
| Classroom a | |||||
| PM2.5 | μg/m3 | 41.82 ± 33.37 | 35.55 (22.05–53.36) | 2.23 | 131.13 |
| PM10 | μg/m3 | 46.32 ± 36.79 | 39.24 (24.67–57.79) | 2.7 | 145.12 |
| CO2 | PPM | 644.77 ± 364.05 | 595.30 (549.09–741.57) | 10.11 | 1819.3 |
| HCHO | mg/m3 | 0.02 ± 0.01 | 0.01 (0.01–0.02) | 0.01 | 0.04 |
| TVOC | mg/m3 | 0.31 ± 0.16 | 0.30 (0.20–0.44) | 0.10 | 0.58 |
| Temperature | °C | 23.01 ± 5.43 | 24.03 (21.18–25.54) | 11.84 | 33.92 |
| Humidity | % | 32.94 ± 9.50 | 32.66 (25.01–39.76) | 19.48 | 49.85 |
| Bedroom b | |||||
| PM2.5 | μg/m3 | 40.10 ± 49.61 | 27.89 (12.19–50.78) | 0.47 | 494.26 |
| PM10 | μg/m3 | 44.40 ± 56.52 | 31.42 (14.07–55.35) | 0.71 | 589.18 |
| CO2 | PPM | 1031.51 ± 527.11 | 919.21 (667.95–1293.89) | 0.00 | 3109.33 |
| HCHO | mg/m3 | 0.03 ± 0.07 | 0.01 (0.01–0.03) | 0.00 | 0.87 |
| TVOC | mg/m3 | 0.39 ± 0.16 | 0.39 (0.28–0.48) | 0.10 | 0.94 |
| Temperature | °C | 25.51 ± 3.13 | 25.45 (23.19–27.63) | 15.5 | 33.52 |
| Humidity | % | 40.07 ± 9.48 | 39.07 (33.66–47.32) | 18.55 | 64.19 |
| Overall c | |||||
| PM2.5 | μg/m3 | 41.36 ± 48.85 | 29.97 (12.90–52.52) | 0.59 | 383.21 |
| PM10 | μg/m3 | 45.90 ± 55.42 | 32.96 (14.87–57.86) | 0.79 | 453.3 |
| CO2 | PPM | 1037.86 ± 490.70 | 965.87 (699.60–1295.92) | 0.00 | 3025.33 |
| HCHO | mg/m3 | 0.03 ± 0.08 | 0.02 (0.01–0.03) | 0.00 | 0.77 |
| TVOC | mg/m3 | 0.39 ± 0.14 | 0.38 (0.29–0.47) | 0.12 | 1.09 |
| Temperature | °C | 25.34 ± 3.20 | 25.10 (23.16–27.42) | 14.99 | 33.99 |
| Humidity | % | 39.84 ± 8.93 | 39.39 (33.43–47.57) | 18.63 | 57.59 |
| Exposure a | Increment (IQR) | ORs (95% CIs) b | p Values |
|---|---|---|---|
| PM2.5 | 39.44 μg/m3 | 1.08 (0.73, 1.58) | 0.70 |
| PM10 | 43.83 μg/m3 | 1.08 (0.75, 1.57) | 0.67 |
| CO2 | 552.38 PPM | 2.10 (1.07, 4.10) | 0.03 * |
| HCHO | 0.02 mg/m3 | 1.12 (0.79, 1.58) | 0.17 |
| TVOC | 0.21 mg/m3 | 1.83 (1.01, 3.35) | 0.04 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Shi, D.; Ye, X.; Dang, J.; Guo, J.; Lian, X.; Wang, S.; Song, J.; Dong, Y.; Li, J.; et al. Spatiotemporal Patterns of Indoor Air Pollution and Its Association with Depressive Symptoms Among Schoolchildren in China. Toxics 2025, 13, 563. https://doi.org/10.3390/toxics13070563
Wang Y, Shi D, Ye X, Dang J, Guo J, Lian X, Wang S, Song J, Dong Y, Li J, et al. Spatiotemporal Patterns of Indoor Air Pollution and Its Association with Depressive Symptoms Among Schoolchildren in China. Toxics. 2025; 13(7):563. https://doi.org/10.3390/toxics13070563
Chicago/Turabian StyleWang, Yaqi, Di Shi, Xinyao Ye, Jiajia Dang, Jianhui Guo, Xinyao Lian, Shaoguan Wang, Jieyun Song, Yanhui Dong, Jing Li, and et al. 2025. "Spatiotemporal Patterns of Indoor Air Pollution and Its Association with Depressive Symptoms Among Schoolchildren in China" Toxics 13, no. 7: 563. https://doi.org/10.3390/toxics13070563
APA StyleWang, Y., Shi, D., Ye, X., Dang, J., Guo, J., Lian, X., Wang, S., Song, J., Dong, Y., Li, J., & Song, Y. (2025). Spatiotemporal Patterns of Indoor Air Pollution and Its Association with Depressive Symptoms Among Schoolchildren in China. Toxics, 13(7), 563. https://doi.org/10.3390/toxics13070563