

The Screening and Correlation of Trace Elements in the Blood and Urine of School-Aged Children (5–12 Years): A Pilot Biomonitoring Study
 , , , , , , ,
, , , , , , ,  , ,
, ,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Eligibility Criteria
2.4. Laboratory Methods
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CINVESTAV | Center for Research and Advanced Studies of the National Polytechnic Institute |
| EDTA | Ethylenediaminetetraacetic acid |
| LOD | Limit of detection |
| SECIHTI | Ministry of Science, Humanities, Technology, and Innovation |
References
- Lawal, K.K.; Ekeleme, I.K.; Onuigbo, C.M.; Ikpeazu, V.O.; Obiekezie, S.O. A review on the public health implications of heavy metals. World J. Adv. Res. Rev. 2021, 10, 255–265. [Google Scholar] [CrossRef]
- Heng, Y.Y.; Asad, I.; Coleman, B.; Menard, L.; Benki-Nugent, S.; Hussein Were, F.; Karr, C.J.; McHenry, M.S. Heavy metals and neurodevelopment of children in low and middle-income countries: A systematic review. PLoS ONE 2022, 17, e0265536. [Google Scholar] [CrossRef]
- Zheng, K.; Zeng, Z.; Tian, Q.; Huang, J.; Zhong, Q.; Huo, X. Epidemiological evidence for the effect of environmental heavy metal exposure on the immune system in children. Sci. Total Environ. 2023, 868, 161691. [Google Scholar] [CrossRef]
- Chen, Y.; Zhao, A.; Li, R.; Kang, W.; Wu, J.; Yin, Y.; Tong, S.; Li, S.; Chen, J. Independent and combined associations of multiple-heavy-metal exposure with lung function: A population-based study in US children. Environ. Geochem. Health 2023, 45, 5213–5230. [Google Scholar] [CrossRef]
- Parra, S.; de la Fuente-Mella, H.; González-Rojas, A.; Bravo, M.A. Exposure to Environmental Pollution in Schools of Puchuncaví, Chile: Characterization of Heavy Metals, Health Risk Assessment, and Effects on Children’s Academic Performance. Sustainability 2024, 16, 2518. [Google Scholar] [CrossRef]
- Witkowska, D.; Slowik, J.; Chilicka, K. Heavy Metals and Human Health: Possible Exposure Pathways and the Competition for Protein Binding Sites. Molecules 2021, 26, 6060. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.S.; Yesmin, M.; Jeba, F.; Hoque, M.S.; Jamee, A.R.; Salam, A. Risk assessment and evaluation of heavy metals concentrations in blood samples of plastic industry workers in Dhaka, Bangladesh. Toxicol. Rep. 2020, 7, 1373–1380. [Google Scholar] [CrossRef]
- Chen, G.; Chen, X.; Yan, C.; Wu, X.; Zeng, G. Surveying mercury levels in hair, blood and urine of under 7-year old children from a coastal city in China. Int. J. Environ. Res. Public Health 2014, 11, 12029–12041. [Google Scholar] [CrossRef] [PubMed]
- Surenbaatar, U.; Lee, S.; Kwon, J.Y.; Lim, H.; Kim, J.J.; Kim, Y.H.; Hong, Y.S. Bioaccumulation of Lead, Cadmium, and Arsenic in a Mining Area and Its Associated Health Effects. Toxics 2023, 11, 519. [Google Scholar] [CrossRef]
- Mattisson, K.; Tekavec, E.; Lundh, T.; Stroh, E. Cadmium and Lead Levels in Blood and Arsenic Levels in Urine among Schoolchildren Living in Contaminated Glassworks Areas, Sweden. Int. J. Environ. Res. Public Health 2020, 17, 7382. [Google Scholar] [CrossRef]
- Capelo, R.; Rohlman, D.S.; Jara, R.; Garcia, T.; Vinas, J.; Lorca, J.A.; Contreras Llanes, M.; Alguacil, J. Residence in an Area with Environmental Exposure to Heavy Metals and Neurobehavioral Performance in Children 9-11 Years Old: An Explorative Study. Int. J. Environ. Res. Public Health 2022, 19, 4732. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.M.; Hossain, D.; Al-Imran, A.; Khan, M.; Begum, M.; Osman, M. Environmental pollution with heavy metals: A public health concern. In Heavy Metals-Their Environmental Impacts and Mitigation; IntechOpen: Rijeka, Croatia, 2021; pp. 771–783. [Google Scholar]
- Mendoza-Cano, O.; Ríos-Silva, M.; Gonzalez-Curiel, I.; Camacho-Delacruz, A.A.; Romo-García, M.F.; Cuevas-Arellano, H.B.; Quintanilla-Montoya, A.L.; Martínez-Preciado, M.A.; Rincón-Avalos, P.; Hilerio-López, Á.G.; et al. Metal concentrations and KIM-1 levels in school-aged children: A crosssectional study. Sci. Rep. 2024, 14, 1–13. [Google Scholar] [CrossRef]
- Correia-Sa, L.; Fernandes, V.C.; Maia, M.L.; Pinto, E.; Norberto, S.; Almeida, A.; Santos, C.; Delerue-Matos, C.; Calhau, C.; Domingues, V.F. Trace Elements in Portuguese Children: Urinary Levels and Exposure Predictors. Toxics 2023, 11, 767. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Li, X.; Yu, L.; Wang, T.; Wang, J.; Liu, T. Review of soil heavy metal pollution in China: Spatial distribution, primary sources, and remediation alternatives. Resour. Conserv. Recycl. 2022, 181, 106261. [Google Scholar] [CrossRef]
- Fatoki, J.O.; Badmus, J.A. Arsenic as an environmental and human health antagonist: A review of its toxicity and disease initiation. J. Hazard. Mater. Adv. 2022, 5, 100052. [Google Scholar] [CrossRef]
- Chowdhury, U. Trace elements concentrations in biological samples and their correlation with urinary arsenic metabolites of chronic arsenic exposed people. Acad. Res. J. Nat. Public Health 2022, 1, 13–30. [Google Scholar] [CrossRef]
- EFSA Panel on Contaminants in the Food Chain (CONTAM); Schrenk, D.; Bignami, M.; Bodin, L.; Chipman, J.K.; del Mazo, J.; Grasl-Kraupp, B.; Hogstrand, C.; Hoogenboom, L.; Leblanc, J.C. Update of the risk assessment of inorganic arsenic in food. EFSA J. 2024, 22, e8488. [Google Scholar]
- Wang, X.; Huang, X.; Zhou, L.; Chen, J.; Zhang, X.; Xu, K.; Huang, Z.; He, M.; Shen, M.; Chen, X.; et al. Association of arsenic exposure and cognitive impairment: A population-based cross-sectional study in China. Neurotoxicology 2021, 82, 100–107. [Google Scholar] [CrossRef]
- Vega-Millan, C.B.; Devora-Figueroa, A.G.; Burgess, J.L.; Beamer, P.I.; Furlong, M.; Lantz, R.C.; Meza-Figueroa, D.; MK, O.R.; Garcia-Rico, L.; Meza-Escalante, E.R.; et al. Inflammation biomarkers associated with arsenic exposure by drinking water and respiratory outcomes in indigenous children from three Yaqui villages in southern Sonora, Mexico. Environ. Sci. Pollut. Res. Int. 2021, 28, 34355–34366. [Google Scholar] [CrossRef]
- Limón-Pacheco, J.H.; Jiménez-Córdova, M.I.; Cárdenas-González, M.; Retana, I.M.S.; Gonsebatt, M.E.; Del Razo, L.M. Potential co-exposure to arsenic and fluoride and biomonitoring equivalents for Mexican children. Ann. Glob. Health 2018, 84, 257–273. [Google Scholar] [CrossRef]
- Ciosek, Ż.; Kot, K.; Kosik-Bogacka, D.; Łanocha-Arendarczyk, N.; Rotter, I. The effects of calcium, magnesium, phosphorus, fluoride, and lead on bone tissue. Biomolecules 2021, 11, 506. [Google Scholar] [CrossRef] [PubMed]
- Adly, H.M.; Saati, A.A.; Khafagy, A.A.; Alandiyjany, M.N.; Saleh, S.A.K. Evaluation of School-Age Children’s Intelligence Quotient and Their Chronic Exposure to Trace Elements in Ambient Air. Cureus 2023, 15, e37532. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guideline for the Clinical Management of Lead Exposure. 2022. Available online: https://iris.who.int/bitstream/handle/10665/352382/9789240045880-spa.pdf (accessed on 12 May 2025). (In Spanish).
- Yasuda, H.; Tsutsui, T.; Suzuki, K. Metallomics Analysis for Assessment of Toxic Metal Burdens in Infants/Children and Their Mothers: Early Assessment and Intervention Are Essential. Biomolecules 2020, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Morata, I.; Sobel, M.; Tellez-Plaza, M.; Navas-Acien, A.; Howe, C.G.; Sanchez, T.R. A State-of-the-Science Review on Metal Biomarkers. Curr. Environ. Health Rep. 2023, 10, 215–249. [Google Scholar] [CrossRef]

{kind=link}
| Median (IQR), ng/mL | Rho (95% CI), | ||
|---|---|---|---|
| Blood | Urine | ||
| Aluminum | 327.9 (216.2–612.7) | 7.9 (4.7–13.3) | 0.11 (−0.10–0.31), 0.303 |
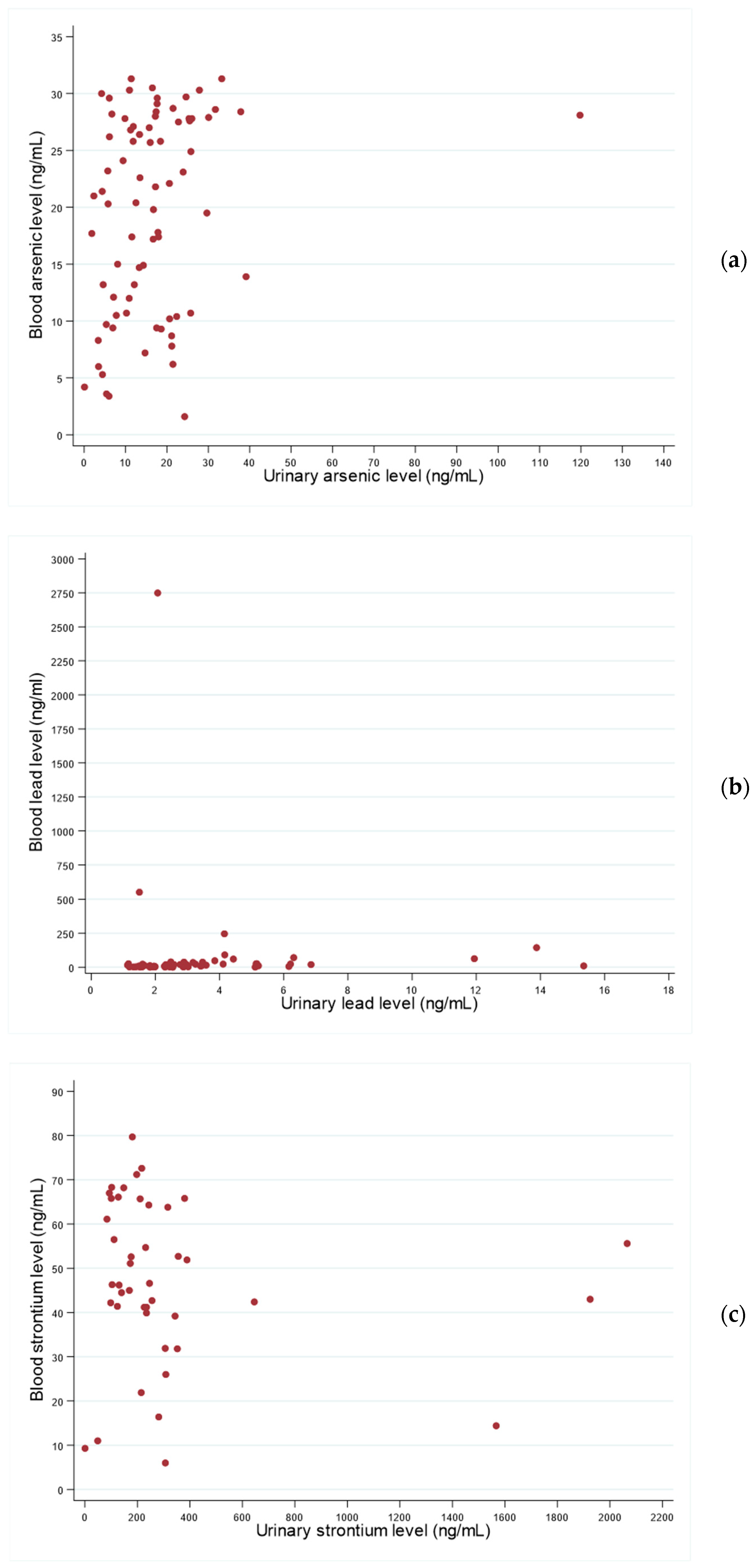
| Arsenic | 21.4 (10.6–27.8) | 13.4 (5.9–19.6) | 0.23 (0.01–0.44), 0.039 |
| Barium | 1.9 (1.1–3.9) | 1.8 (1.0–2.5) | 0.04 (−0.16–0.24), 0.688 |
| Cesium | 2.8 (2.3–3.3) | 8.0 (4.6–11.0) | 0.19 (−0.01–0.39), 0.066 |
| Cobalt | 0.6 (0.1–0.7) | 1.2 (0.8–1.6) | 0.20 (−0.02–0.41), 0.081 |
| Copper | 1083.4 (1055.8–1127.0) | 9.6 (4.3–19.0) | −0.01 (−0.23–0.21), 0.930 |
| Iodine | 53.0 (47.1–63.9) | 178.7 (118.9–255.3) | 0.08 (−0.12–0.29), 0.437 |
| Lead | 11.3 (4.0–23.8) | 1.8 (1.5–2.0) | 0.43 (0.24–0.61), <0.001 |
| Lithium | 2.1 (1.5–2.8) | 41.9 (30.6–53.6) | −0.19 (−0.40–0.01), 0.063 |
| Manganese | 15.5 (12.0–18.5) | 0.1 (0.1–0.6) | −0.11 (−0.33–0.11), 0.327 |
| Molybdenum | 5.0 (4.2–6.1) | 93.6 (63.4–131.2) | 0.10 (−0.12–0.32), 0.374 |
| Nickel | 5.6 (3.7–8.6) | 7.6 (4.8–9.1) | 0.01 (−0.19–0.20), 0.946 |
| Selenium | 161.0 (147.7–178.1) | 63.6 (56.7–87.4) | 0.20 (−0.01–0.41), 0.069 |
| Strontium | 46.2 (39.2–63.8) | 157.8 (111.1–257.5) | 0.22 (0.03–0.40), 0.023 |
| Tellurium | 0.3 (0.3–0.3) | 0.59 (0.58–0.61) | −0.01 (−0.23–0.22), 0.979 |
| Titanium | 23.3 (15.4–30.7) | 22.0 (15.4–35.7) | −0.05 (−0.27–0.17), 0.658 |
| Zinc | 5496 (5127–5784) | 604.8 (427.1–822.0) | −0.08 (−0.30–0.14), 0.474 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camacho-delaCruz, A.A.; Mendoza-Cano, O.; Trujillo, X.; Huerta, M.; Ríos-Silva, M.; Gonzalez-Curiel, I.E.; Lugo-Radillo, A.; Romo-García, M.F.; Cuevas-Arellano, H.B.; Hilerio-López, Á.G.; et al. The Screening and Correlation of Trace Elements in the Blood and Urine of School-Aged Children (5–12 Years): A Pilot Biomonitoring Study. Toxics 2025, 13, 431. https://doi.org/10.3390/toxics13060431
Camacho-delaCruz AA, Mendoza-Cano O, Trujillo X, Huerta M, Ríos-Silva M, Gonzalez-Curiel IE, Lugo-Radillo A, Romo-García MF, Cuevas-Arellano HB, Hilerio-López ÁG, et al. The Screening and Correlation of Trace Elements in the Blood and Urine of School-Aged Children (5–12 Years): A Pilot Biomonitoring Study. Toxics. 2025; 13(6):431. https://doi.org/10.3390/toxics13060431
Chicago/Turabian StyleCamacho-delaCruz, Arlette A., Oliver Mendoza-Cano, Xóchitl Trujillo, Miguel Huerta, Mónica Ríos-Silva, Irma Elizabeth Gonzalez-Curiel, Agustin Lugo-Radillo, María Fernanda Romo-García, Herguin Benjamin Cuevas-Arellano, Ángel Gabriel Hilerio-López, and et al. 2025. "The Screening and Correlation of Trace Elements in the Blood and Urine of School-Aged Children (5–12 Years): A Pilot Biomonitoring Study" Toxics 13, no. 6: 431. https://doi.org/10.3390/toxics13060431
APA StyleCamacho-delaCruz, A. A., Mendoza-Cano, O., Trujillo, X., Huerta, M., Ríos-Silva, M., Gonzalez-Curiel, I. E., Lugo-Radillo, A., Romo-García, M. F., Cuevas-Arellano, H. B., Hilerio-López, Á. G., Solano-Barajas, R., Bricio-Barrios, J. A., Uribe-Ramos, J. M., Ventura-Ramírez, J. F., Solano-Mendoza, A. A., Sánchez-Cárdenas, F., Benites-Godínez, V., Ríos-Bracamontes, E. F., Venegas-Ramírez, J., & Murillo-Zamora, E. (2025). The Screening and Correlation of Trace Elements in the Blood and Urine of School-Aged Children (5–12 Years): A Pilot Biomonitoring Study. Toxics, 13(6), 431. https://doi.org/10.3390/toxics13060431