

Impact of Heated Tobacco Products, E-Cigarettes, and Combustible Cigarettes on Small Airways and Arterial Stiffness
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
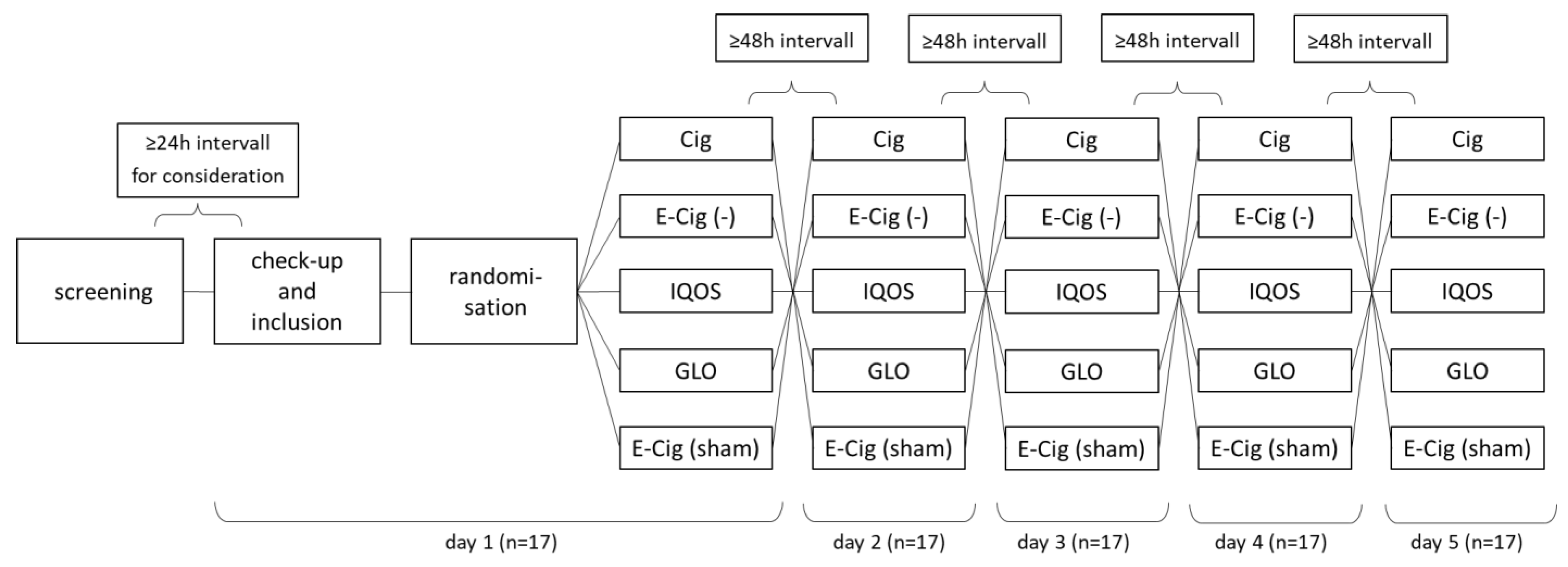
2.1. Study Cohort and Design
2.2. Measurement of Resistance and Reactance in Central and Small Airways
2.3. Measurement of Peripheral and Central Blood Pressure and Arterial Stiffness
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
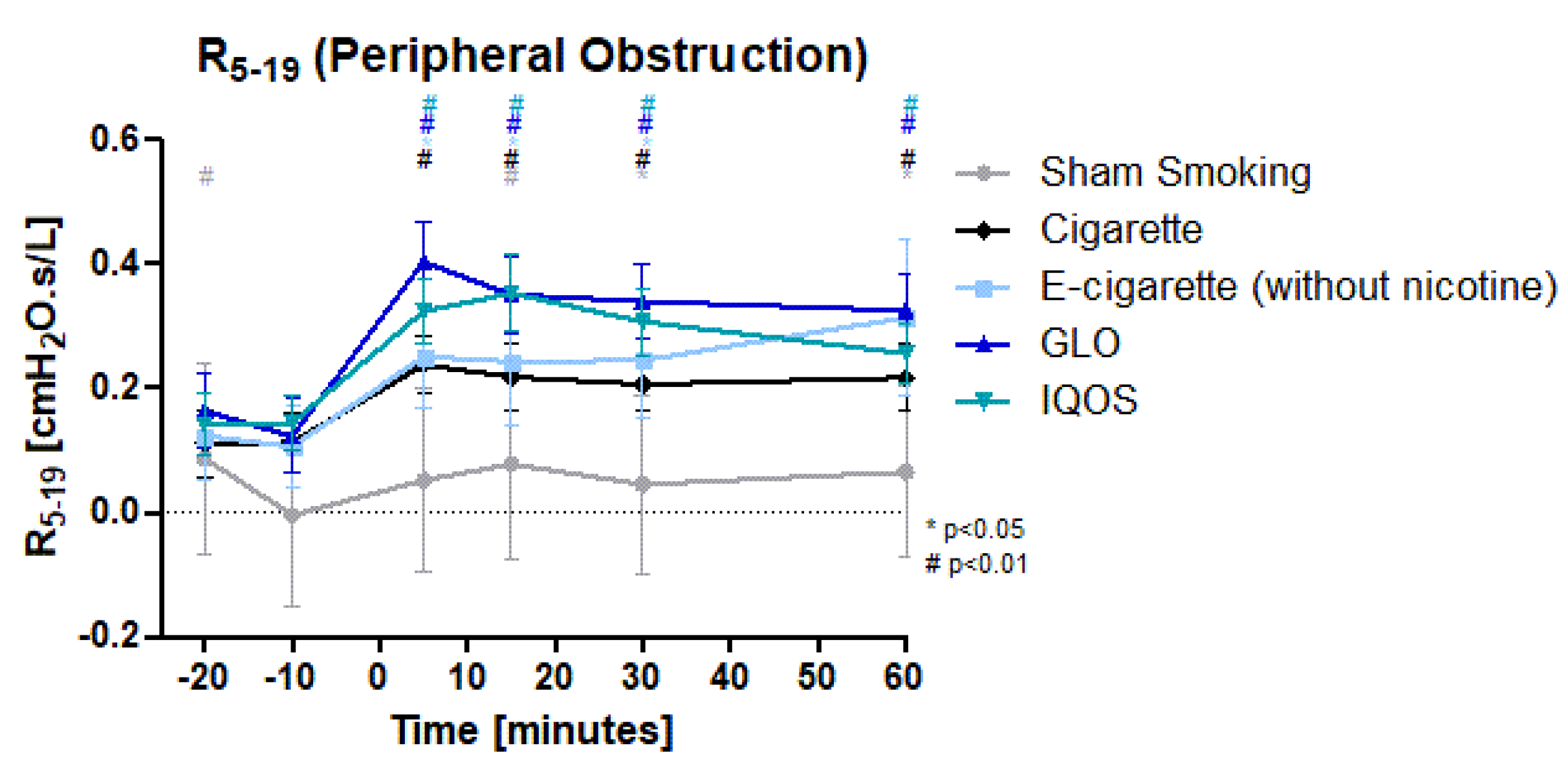
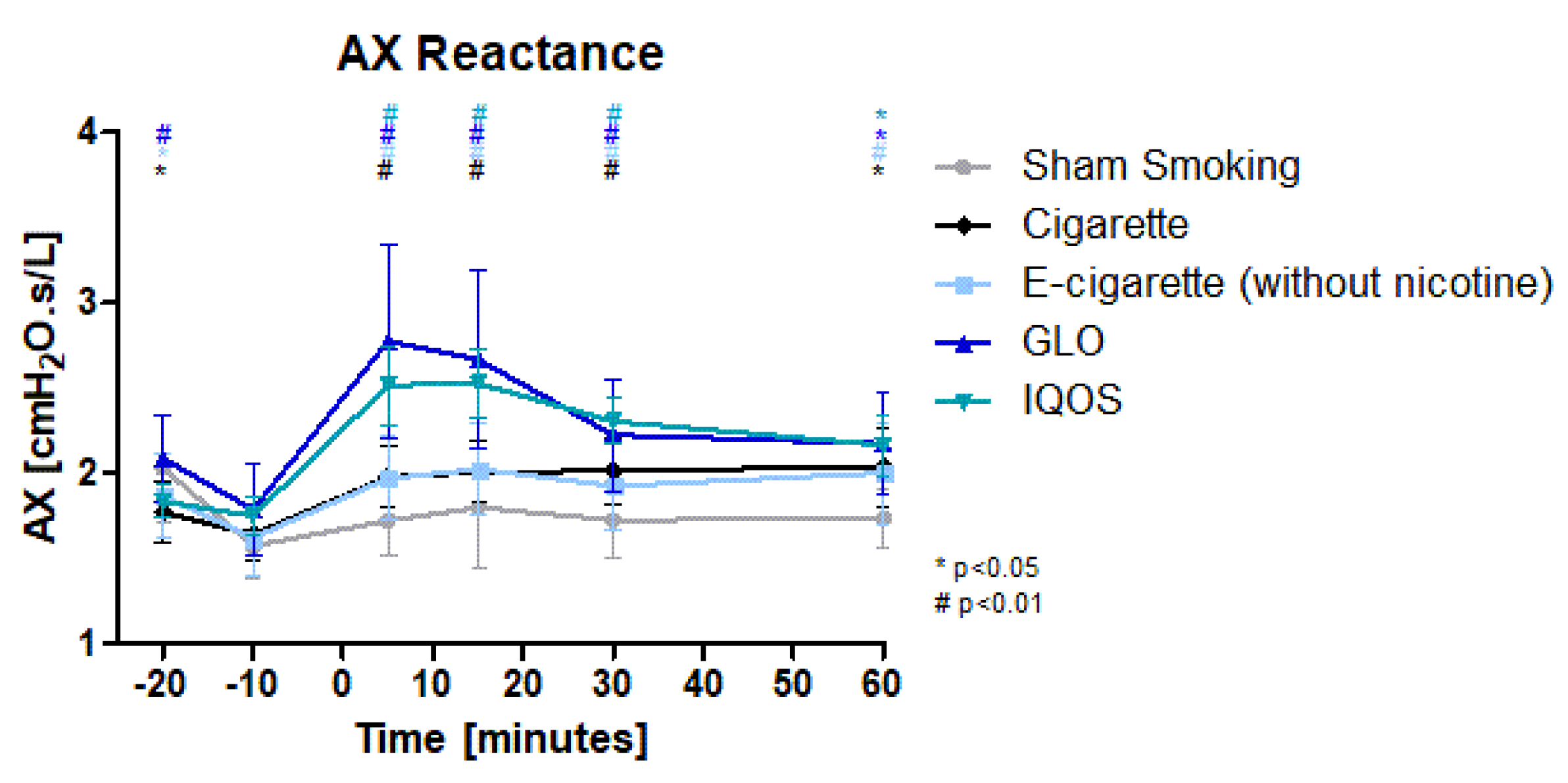
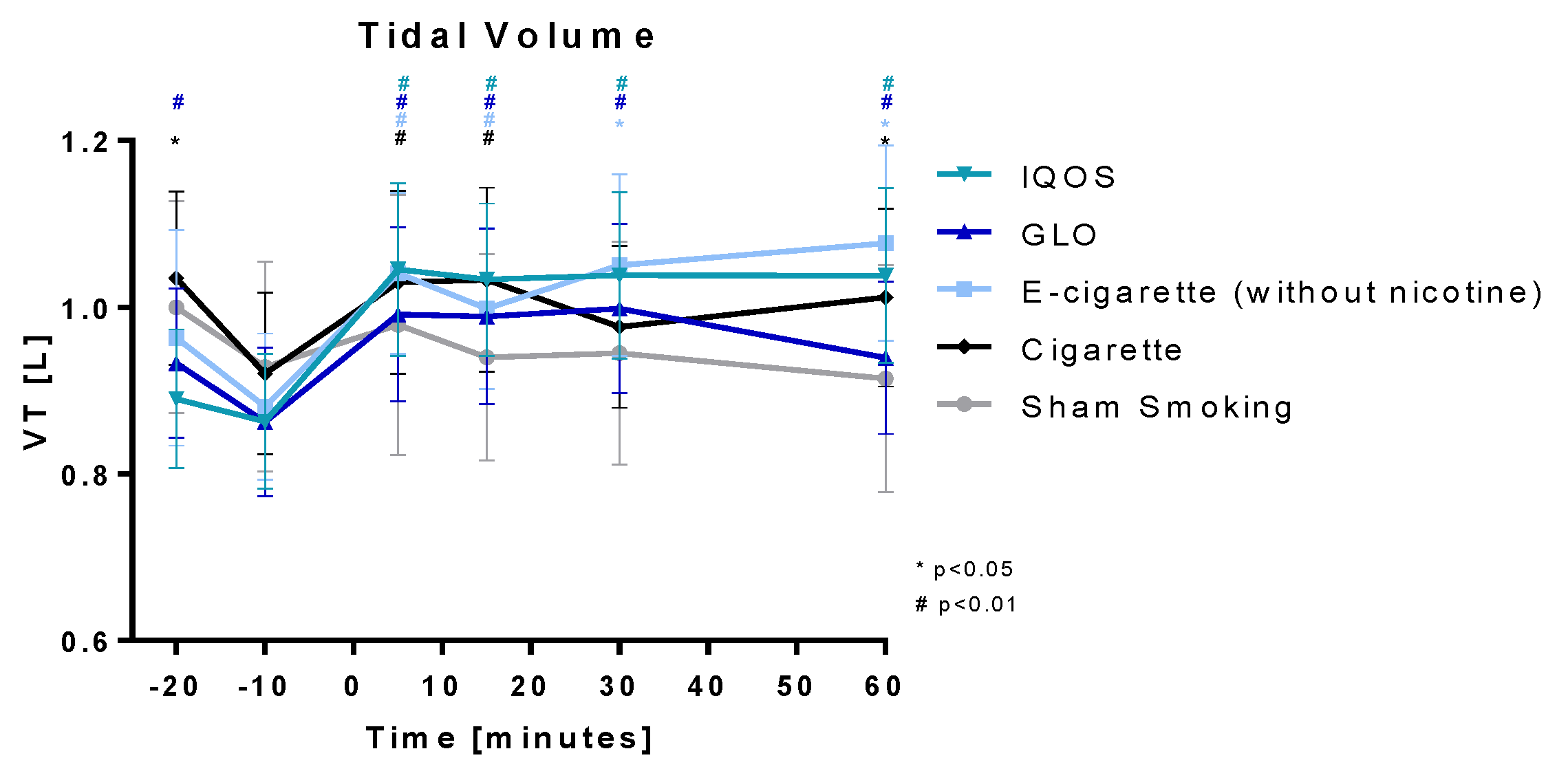
3.2. Respiratory Parameters
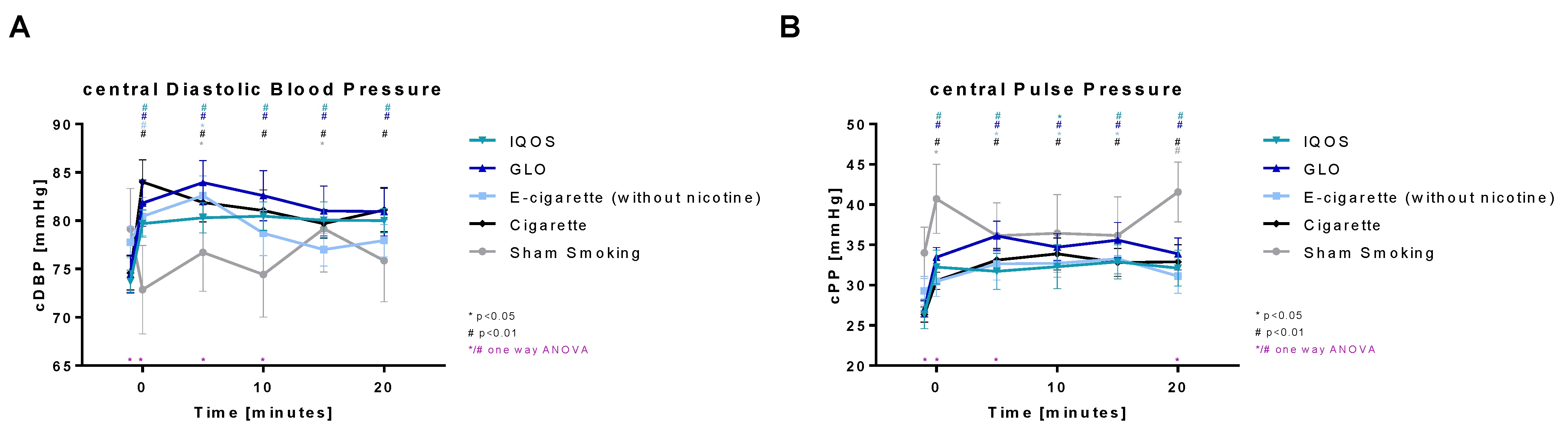
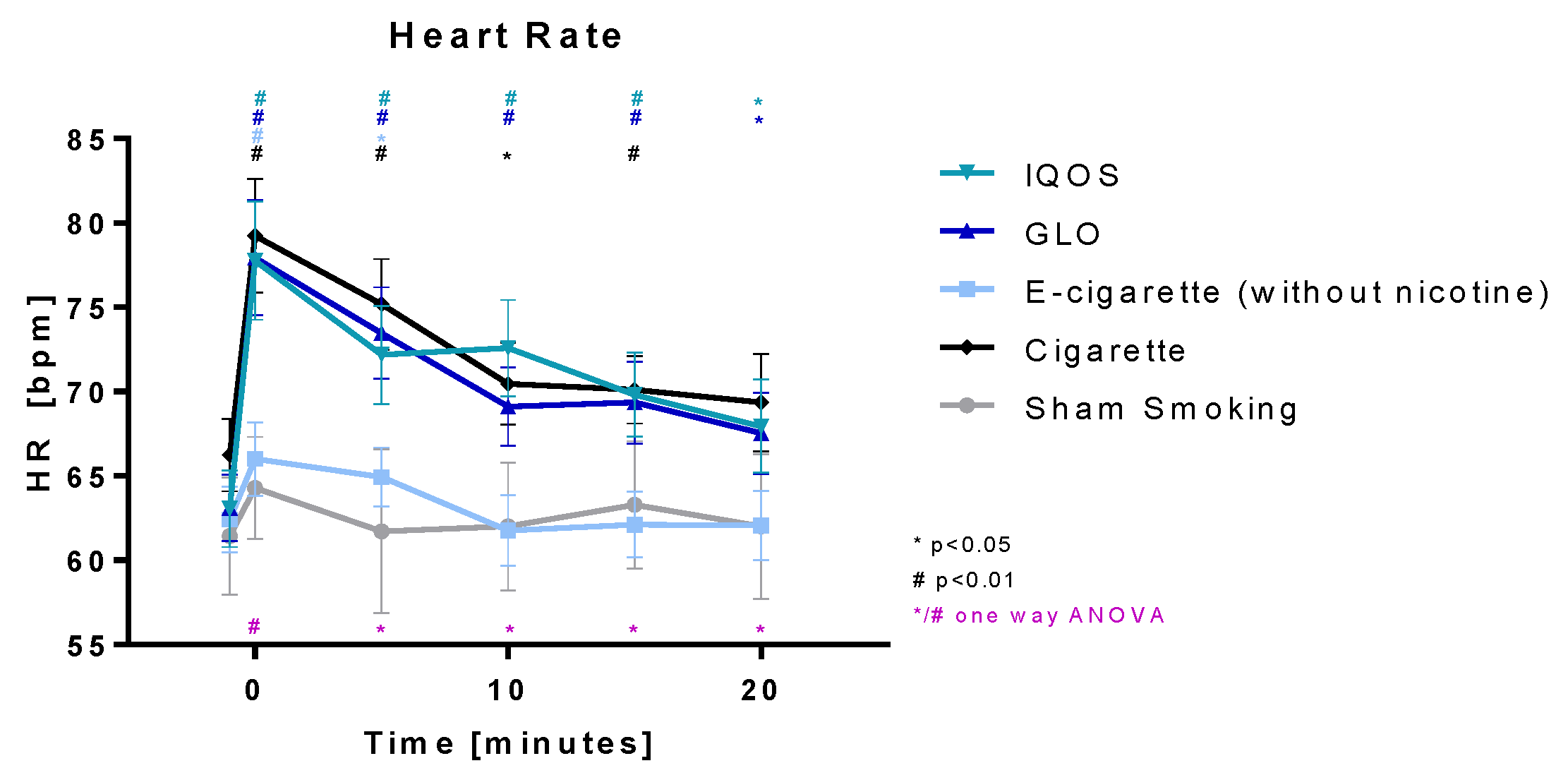
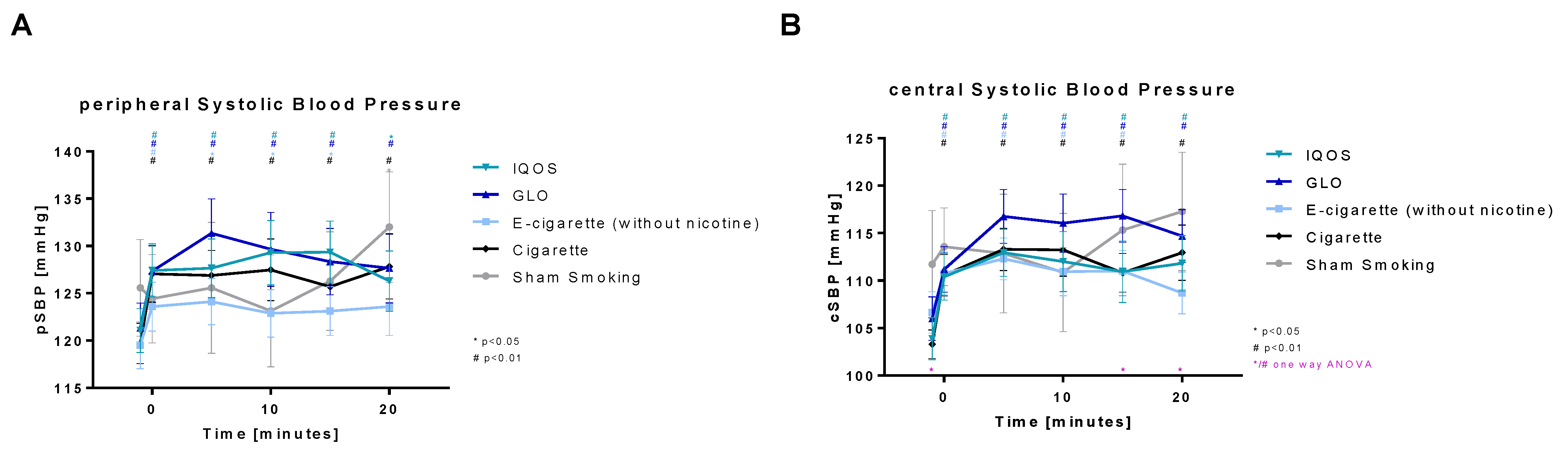
3.3. Heart Rate, Peripheral, and Central Blood Pressure and Pulse Pressure
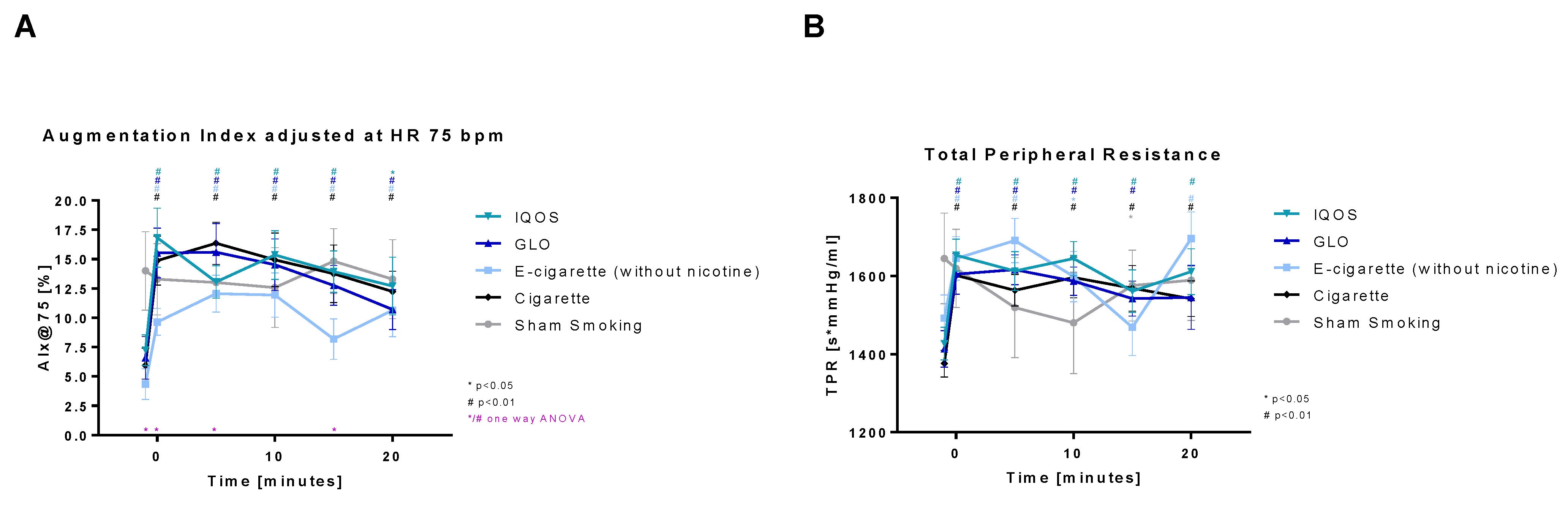
3.4. Parameters of Arterial Stiffness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bundesministerium für Gesundheit. Rauchen. Available online: https://www.bundesgesundheitsministerium.de/service/begriffe-von-a-z/r/rauchen.html (accessed on 29 March 2023).
- Institute of General Practice, Addiction Research and Clinical Epidemiology Unit. DEBRA Study. Prävalenz Aktueller Tabak-Raucher*innen in Deutschland. Available online: https://www.debra-study.info/ (accessed on 28 March 2023).
- Pashutina, Y.; Kastaun, S.; Kotz, D. DEBRA Factsheet 5; Die Motivation zum Rauchstopp Skala. Düsseldorf, Germany. Available online: https://www.google.com.tw/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwiL16mRu5WBAxU5o1YBHRuGB9UQFnoECBYQAQ&url=https%3A%2F%2Fwww.debra-study.info%2Fwp-content%2Fuploads%2F2022%2F02%2FFactsheet-05-v7-1.pdf&usg=AOvVaw0PqllTq-Dz1zFksTZjBw2M&opi=89978449 (accessed on 28 March 2023).
- Hughes, J.R.; Keely, J.; Naud, S. Shape of the relapse curve and long-term abstinence among untreated smokers. Addiction 2004, 99, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Stead, L.F.; Perera, R.; Bullen, C.; Mant, D.; Hartmann-Boyce, J.; Cahill, K.; Lancaster, T. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst. Rev. 2018, 11, CD000146. [Google Scholar]
- Hartmann-Boyce, J.; McRobbie, H.; Lindson, N.; Bullen, C.; Bergh, R.; Theodoulou, A.; Notley, C.; Rigotti, N.A.; Turner, T.; Butler, A.R.; et al. Electronic cigarettes for smoking cessation. Cochrane Database Syst. Rev. 2022, 11, CD010216. [Google Scholar]
- Kotz, D.; Jackson, S.; Brown, J.; Kastaun, S. The Effectiveness of E-Cigarettes for Smoking Cessation. Dtsch. Arztebl. Int. 2022, 119, 297–301. [Google Scholar] [PubMed]
- Bhatt, J.M.; Ramphul, M.; Bush, A. An update on controversies in e-cigarettes. Paediatr. Respir. Rev. 2020, 36, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Gotts, J.E.; Jordt, S.-E.; McConnell, R.; Tarran, R. What are the respiratory effects of e-cigarettes? BMJ 2019, 366, l5275. [Google Scholar] [CrossRef] [PubMed]
- Chun, L.F.; Moazed, F.; Calfee, C.S.; Matthay, M.; Gotts, J. Pulmonary toxicity of e-cigarettes. Am. J. Physiol. Lung Cell Mol. Physiol. 2017, 313, L193–L206. [Google Scholar] [CrossRef]
- Lüdicke, F.; Picavet, P.; Baker, G.; Haziza, C.; Poux, V. Effects of Switching to the Menthol Tobacco Heating System 2.2, Smoking Abstinence, or Continued Cigarette Smoking on Clinically Relevant Risk Markers: A Randomized, Controlled, Open-Label, Multicenter Study in Sequential Confinement and Ambulatory Settings (Part 2). Nicotine Tob. Res. 2018, 20, 173–182. [Google Scholar] [PubMed]
- Goodall, S.; Gale, N.; Thorne, D.; Haziza, C.; Hadley, S.; Prasad, K.; Gilmour, I.; Miazzi, F.; Proctor, C. Evaluation of behavioural, chemical, toxicological and clinical studies of a tobacco heated product glo™ and the potential for bridging from a foundational dataset to new product iterations. Toxicol. Rep. 2022, 9, 1426–1442. [Google Scholar] [CrossRef]
- WHO. Heated Tobacco Products Information Sheet. Available online: https://www.who.int/publications/i/item/WHO-HEP-HPR-2020.2 (accessed on 20 February 2023).
- Centers for Disease Control and Prevention (US); National Center for Chronic Disease Prevention and Health Promotion; Office on Smoking and Health (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General; Chemistry and Toxicology of Cigarette Smoke and Biomarkers of Exposure and Harm; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2010.
- Başaran, R.; Güven, N.M.; Eke, B.C. An Overview of iQOS® as a New Heat-Not-Burn Tobacco Product and Its Potential Effects on Human Health and the Environment. Turk. J. Pharm. Sci. 2019, 16, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Schaller, K.; Kahnert, D.-B.S.; Mons, U. E-Zigaretten und Tabakerhitzer—Ein Überblick; Deutsches Krebsforschungszentrum: Heidelberg, Germany, 2020. [Google Scholar]
- Dusautoir, R.; Zarcone, G.; Verriele, M.; Garcon, G.; Fronval, I.; Beauval, N.; Allorge, D.; Riffault, V.; Locoge, N.; Lo-Guidic, J.-M.; et al. Comparison of the chemical composition of aerosols from heated tobacco products, electronic cigarettes and tobacco cigarettes and their toxic impacts on the human bronchial epithelial BEAS-2B cells. J. Hazard. Mater. 2021, 401, 123417. [Google Scholar] [CrossRef] [PubMed]
- Tattan-Birch, H.; Jackson, S.E.; Dockrell, M.; Brown, J. Tobacco-free Nicotine Pouch Use in Great Britain: A Representative Population Survey 2020–2021. Nicotine Tob. Res. 2022, 24, 1509–1512. [Google Scholar] [CrossRef] [PubMed]
- Znyk, M.; Jurewicz, J.; Kaleta, D. Exposure to Heated Tobacco Products and Adverse Health Effects, a Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6651. [Google Scholar] [CrossRef]
- Vivarelli, F.; Canistro, D.; Cirillo, S.; Elias, R.; Granata, S.; Mussoni, M.; Burattini, S.; Falcieri, E.; Turrini, E.; Fimognari, C.; et al. Unburned Tobacco Cigarette Smoke Alters Rat Ultrastructural Lung Airways and DNA. Nicotine Tob. Res. 2021, 23, 2127–2134. [Google Scholar] [CrossRef]
- Nitta, N.A.; Sato, T.; Komura, M.; Yoshikawa, H.; Suzuki, Y.; Mitsui, A.; Kuwasaki, E.; Takahashi, F.; Kodama, Y.; Seyama, K.; et al. Exposure to the heated tobacco product IQOS generates apoptosis-mediated pulmonary emphysema in murine lungs. Am. J. Physiol. Lung Cell Mol. Physiol. 2022, 322, L699–L711. [Google Scholar] [CrossRef] [PubMed]
- Bhat, T.A.; Kalathil, S.G.; Leigh, N.; Muthumalage, T.; Rahman, I.; Goniewicz, M.; Thanvala, Y. Acute Effects of Heated Tobacco Product (IQOS) Aerosol Inhalation on Lung Tissue Damage and Inflammatory Changes in the Lungs. Nicotine Tob. Res. 2021, 23, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Franzen, K.F.; Belkin, S.; Goldmann, T.; Reppel, M.; Watz, H.; Mortensen, K.; Drömann, D. The impact of heated tobacco products on arterial stiffness. Vasc. Med. 2020, 25, 572–574. [Google Scholar] [CrossRef]
- Benthien, J.; Meusel, M.; Cayo Talavera, S.; Eitel, I.; Drömann, D.; Franzen, K. JUUL™ ing and Heating Lead to a Worsening of Arterial Stiffness. Medicines 2022, 9, 28. [Google Scholar] [CrossRef] [PubMed]
- van Bortel, L.M.; Duprez, D.; Starmans-Kool, M.J.; E Safar, M.; Giannattasio, C.; Cockcroft, J.; Kaiser, D.; Thuillez, C. Clinical applications of arterial stiffness, Task Force III: Recommendations for user procedures. Am. J. Hypertens. 2002, 15, 445–452. [Google Scholar] [CrossRef]
- Philip Morris Products, S.A. User Guide IQOS 2.4 PLUS. Available online: www.iqos.com/gb/en/get-support/iqos-2-4-plus-guide.html (accessed on 30 March 2023).
- British American Tobacco, S.A. Instruction Manual GLO. Available online: https://www.discoverglo.com/de/de/blog/tabak-erhitzen-anfaengerfehler/ (accessed on 30 March 2023).
- Farsalinos, K.E.; Romagna, G.; Tsiapras, D.; Kyrzopoulos, S.; Voudris, V. Evaluation of electronic cigarette use (vaping) topography and estimation of liquid consumption: Implications for research protocol standards definition and for public health authorities’ regulation. Int. J. Environ. Res. Public Health 2013, 10, 2500–2514. [Google Scholar] [CrossRef]
- Thoracic Medical Systems Inc. Tremoflo C-100 Airwave Oscillometry System User Manual English; THORASYS Thoracic Medical System Inc.: Montreal, QC, Canada, 2018. [Google Scholar]
- Porojan-Suppini, N.; Fira-Mladinescu, O.; Marc, M.; Tudorache, E.; Oancea, C. Lung Function Assessment by Impulse Oscillometry in Adults. Ther. Clin. Risk Manag. 2020, 16, 1139–1150. [Google Scholar] [CrossRef] [PubMed]
- Hallett, S.; Toro, F.; Ashurst, J.V. Physiology, Tidal Volume; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Weber, T.; Wassertheurer, S.; Rammer, M.; Maurer, E.; Hametner, B.; Mayer, C.; Kropf, J.; Eber, B. Validation of a brachial cuff-based method for estimating central systolic blood pressure. Hypertension 2011, 58, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Wassertheurer, S.; Kropf, J.; Weber, T.; van der Giet, M.; Baulmann, J.; Ammer, M.; Hametner, B.; Mayer, C.; Eber, B.; Magometschnigg, D. A new oscillometric method for pulse wave analysis: Comparison with a common tonometric method. J. Hum. Hypertens. 2010, 24, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Hukkanen, J.; Jacob, P.; Benowitz, N.L. Metabolism and disposition kinetics of nicotine. Pharmacol. Rev. 2005, 57, 79–115. [Google Scholar] [CrossRef]
- Philip Morris Products, S.A. Philip Morris International, Website. Unsere Visionen, eine Rauchfreie Zukunft Gestalten. Available online: https://www.pmi.com/markets/germany/de/%C3%BCber-uns/our-vision (accessed on 30 March 2023).
- British American Tobacco (Germany) GmbH. glo Website. Available online: https://www.discoverglo.com/de/de/ (accessed on 30 March 2023).
- Simonavicius, E.; McNeill, A.; Shahab, L.; Brose, L. Heat-not-burn tobacco products: A systematic literature review. Tob. Control 2019, 28, 582–594. [Google Scholar] [CrossRef]
- Desiraju, K.; Agrawal, A. Impulse oscillometry: The state-of-art for lung function testing. Lung India 2016, 33, 410–416. [Google Scholar]
- Christenson, S.A.; Smith, B.M.; Bafadhel, M.; Putcha, N. Chronic obstructive pulmonary disease. Lancet 2022, 399, 2227–2242. [Google Scholar] [CrossRef]
- Sohal, S.S.; Eapen, M.S.; Naidu, V.G.M.; Sharma, P. IQOS exposure impairs human airway cell homeostasis: Direct comparison with traditional cigarette and e-cigarette. ERJ Open Res. 2019, 5, 00159–2018. [Google Scholar] [CrossRef]
- Pataka, A.; Kotoulas, S.; Chatzopoulos, E.; Grigoriou, I.; Sapalidis, K.; Kosmidis, C.; Vagionas, A.; Perdikouri, E.-I. Acute Effects of a Heat-Not-Burn Tobacco Product on Pulmonary Function. Medicina 2020, 56, 292. [Google Scholar] [CrossRef]
- Leigh, N.J.; Tran, P.L.; O’Connor, R.J.; Goniewicz, M. Cytotoxic effects of heated tobacco products (HTP) on human bronchial epithelial cells. Tob. Control 2018, 27, s26–s29. [Google Scholar] [CrossRef]
- Madison, M.C.; Landers, C.T.; Gu, B.-H.; Chang, C.-Y.; Tung, H.-Y.; You, R.; Hong, M.; Baghaei, N.; Song, L.-Z.; Porter, P. Electronic cigarettes disrupt lung lipid homeostasis and innate immunity independent of nicotine. J. Clin. Investig. 2019, 129, 4290–4304. [Google Scholar] [CrossRef]
- Szafran, B.N.; Pinkston, R.; Perveen, Z.; Ross, M.; Morgan, T.; Paulsen, D.B.; Penn, A.; Kaplan, B.; Noel, A. Electronic-Cigarette Vehicles and Flavoring Affect Lung Function and Immune Responses in a Murine Model. Int. J. Mol. Sci. 2020, 21, 6022. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Anagnostopoulos, N.; Kougias, M.; Evangelopoulou, V.; Connoly, G.; Behrakis, P. Short-term pulmonary effects of using an electronic cigarette: Impact on respiratory flow resistance, impedance, and exhaled nitric oxide. Chest 2012, 141, 1400–1406. [Google Scholar] [CrossRef]
- Flouris, A.D.; Chorti, M.S.; Poulianiti, K.P.; Jamurtas, A.Z.; Kostikas, K.; Tzatzarakis, M.; Hayes, A.; Tsatsaki, A. Acute impact of active and passive electronic cigarette smoking on serum cotinine and lung function. Inhal. Toxicol. 2013, 25, 91–101. [Google Scholar] [CrossRef]
- Unverdorben, M.; Mostert, A.; Munjal, S.; van der Bijl, A.; Potgieter, L.; Venter, C.; Liang, Q.; Meyer, B.; Roethig, H.-J. Acute effects of cigarette smoking on pulmonary function. Regul. Toxicol. Pharmacol. 2010, 57, 241–246. [Google Scholar] [CrossRef]
- Ferrari, M.; Zanasi, A.; Nardi, E.; Labate, A.; Ceriana, P.; Balestrino, A.; Pisani, L.; Corcione, N.; Nava, S. Short-term effects of a nicotine-free e-cigarette compared to a traditional cigarette in smokers and non-smokers. BMC Pulm. Med. 2015, 15, 120. [Google Scholar] [CrossRef]
- Benowitz, N.L. The role of nicotine in smoking-related cardiovascular disease. Prev. Med. 1997, 26, 412–417. [Google Scholar] [CrossRef]
- Omvik, P. How smoking affects blood pressure. Blood Press. 1996, 5, 71–77. [Google Scholar] [CrossRef]
- Adamopoulos, D.; Argacha, J.-F.; Gujic, M.; Preumont, N.; Degaute, J.-P.; van de Borne, P. Acute effects of nicotine on arterial stiffness and wave reflection in healthy young non-smokers. Clin. Exp. Pharmacol. Physiol. 2009, 36, 784–789. [Google Scholar] [CrossRef]
- Mahmud, A.; Feely, J. Effects of passive smoking on blood pressure and aortic pressure waveform in healthy young adults--influence of gender. Br. J. Clin. Pharmacol. 2004, 57, 37–43. [Google Scholar] [CrossRef]
- Jatoi, N.A.; Jerrard-Dunne, P.; Feely, J.; Mahmud, A. Impact of smoking and smoking cessation on arterial stiffness and aortic wave reflection in hypertension. Hypertension 2007, 49, 981–985. [Google Scholar] [CrossRef]
- Majek, P.; Jankowski, M.; Brożek, G.M. Acute health effects of heated tobacco products: Comparative analysis with traditional cigarettes and electronic cigarettes in young adults. ERJ Open Res. 2023, 9, 00595–2022. [Google Scholar] [CrossRef]
- Yaman, B.; Akpınar, O.; Kemal, H.S.; Cerit, L.; Yüksek, Ü.; Söylemez, N.; Duygu, H. Comparison of IQOS (heated tobacco) and cigarette smoking on cardiac functions by two-dimensional speckle tracking echocardiography. Toxicol. Appl. Pharmacol. 2021, 423, 115575. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; Simone, G.; Dominiczak, A. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 2001, 37, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Baulmann, J.; Nürnberger, J.; Slany, J.; Schmieder, R.; Schmidt-Trucksäss, A.; Baumgart, D.; Cremerius, P.; Hess, O.; Mortensen, K.; Weber, T. Arterielle Gefässsteifigkeit und Pulswellenanalyse. Dtsch. Med. Wochenschr. 2010, 135 (Suppl. 1), S4–S14. [Google Scholar] [CrossRef] [PubMed]
- Antoniewicz, L.; Brynedal, A.; Hedman, L.; Lundbäck, M.; Bosson, J. Acute Effects of Electronic Cigarette Inhalation on the Vasculature and the Conducting Airways. Cardiovasc. Toxicol. 2019, 19, 441–450. [Google Scholar] [CrossRef]
- Gonzalez, J.E.; Cooke, W.H. Acute effects of electronic cigarettes on arterial pressure and peripheral sympathetic activity in young nonsmokers. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H248–H255. [Google Scholar] [CrossRef]
- Flint, A.C.; Conell, C.; Ren, X.; Banki, N.M.; Chan, S.L.; Rao, V.; Melles, R.; Bhatt, D. Effect of Systolic and Diastolic Blood Pressure on Cardiovascular Outcomes. N. Engl. J. Med. 2019, 381, 243–251. [Google Scholar] [CrossRef]
- Hajek, P.; Pittaccio, K.; Pesola, F.; Smith, K.; Phillips-Waller, A.; Przulj, D. Nicotine delivery and users’ reactions to Juul compared with cigarettes and other e-cigarette products. Addiction 2020, 115, 1141–1148. [Google Scholar] [CrossRef]
- Staudt, M.R.; Salit, J.; Kaner, R.J.; Hollmann, C.; Crystal, R. Altered lung biology of healthy never smokers following acute inhalation of E-cigarettes. Respir. Res. 2018, 19, 78. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, M.L.; Delucchi, K.; Benowitz, N.L.; Ramo, D. Adolescent Exposure to Toxic Volatile Organic Chemicals From E-Cigarettes. Pediatrics 2018, 141, e20173557. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | All (n = 17) | Male (n = 9) | Female (n = 8) | p-Value |
|---|---|---|---|---|
| Age [years] | 24.2 ± 1.1 | 25.2 ± 4.6 | 23 ± 4.4 | 0.329 |
| Weight [kg] | 71.3 ± 3.8 | 82.9 ± 11.5 | 58.3 ± 5.6 | <0.01 |
| Height [cm] | 177 ± 2.7 | 184.8 ± 9.0 | 168.4 ± 5.7 | <0.01 |
| BMI [kg/m2] | 22.5 ± 0.6 | 24.2 ± 1.9 | 20.5 ± 1.6 | 0.01 |
| Waist [cm] | 77.5 ± 2.7 | 86.1 ± 5.5 | 67.9 ± 7.0 | <0.01 |
| Hip [cm] | 91.2 ± 2.1 | 96.7 ± 5.5 | 85.1 ± 7.1 | 0.02 |
| Cigarettes per day | 1.12 ± 0.8 | 1.2 ± 0.7 | 1.0 ± 1.0 | 0.687 |
| Fagerström Test for Nicotine Dependence [points] | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goebel, I.; Mohr, T.; Axt, P.N.; Watz, H.; Trinkmann, F.; Weckmann, M.; Drömann, D.; Franzen, K.F. Impact of Heated Tobacco Products, E-Cigarettes, and Combustible Cigarettes on Small Airways and Arterial Stiffness. Toxics 2023, 11, 758. https://doi.org/10.3390/toxics11090758
Goebel I, Mohr T, Axt PN, Watz H, Trinkmann F, Weckmann M, Drömann D, Franzen KF. Impact of Heated Tobacco Products, E-Cigarettes, and Combustible Cigarettes on Small Airways and Arterial Stiffness. Toxics. 2023; 11(9):758. https://doi.org/10.3390/toxics11090758
Chicago/Turabian StyleGoebel, Isabel, Theresa Mohr, Paul N. Axt, Henrik Watz, Frederik Trinkmann, Markus Weckmann, Daniel Drömann, and Klaas F. Franzen. 2023. "Impact of Heated Tobacco Products, E-Cigarettes, and Combustible Cigarettes on Small Airways and Arterial Stiffness" Toxics 11, no. 9: 758. https://doi.org/10.3390/toxics11090758
APA StyleGoebel, I., Mohr, T., Axt, P. N., Watz, H., Trinkmann, F., Weckmann, M., Drömann, D., & Franzen, K. F. (2023). Impact of Heated Tobacco Products, E-Cigarettes, and Combustible Cigarettes on Small Airways and Arterial Stiffness. Toxics, 11(9), 758. https://doi.org/10.3390/toxics11090758