
11-Nor-9-Carboxy Tetrahydrocannabinol Distribution in Fluid from the Chest Cavity in Cannabis-Related Post-Mortem Cases

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Speciemns Selection
2.2. Specimens Collection
2.3. Bodily and Tissues Sample Preparation
2.3.1. Non-Hydrolyzed Specimens
2.3.2. Hydrolyzed Specimens
2.3.3. Solid Phase Extraction
2.4. LC-MS/MS Conditions
2.5. Method Validation
2.6. Statistical Analysis
3. Results
3.1. Demographic Profile
3.2. Case Samples
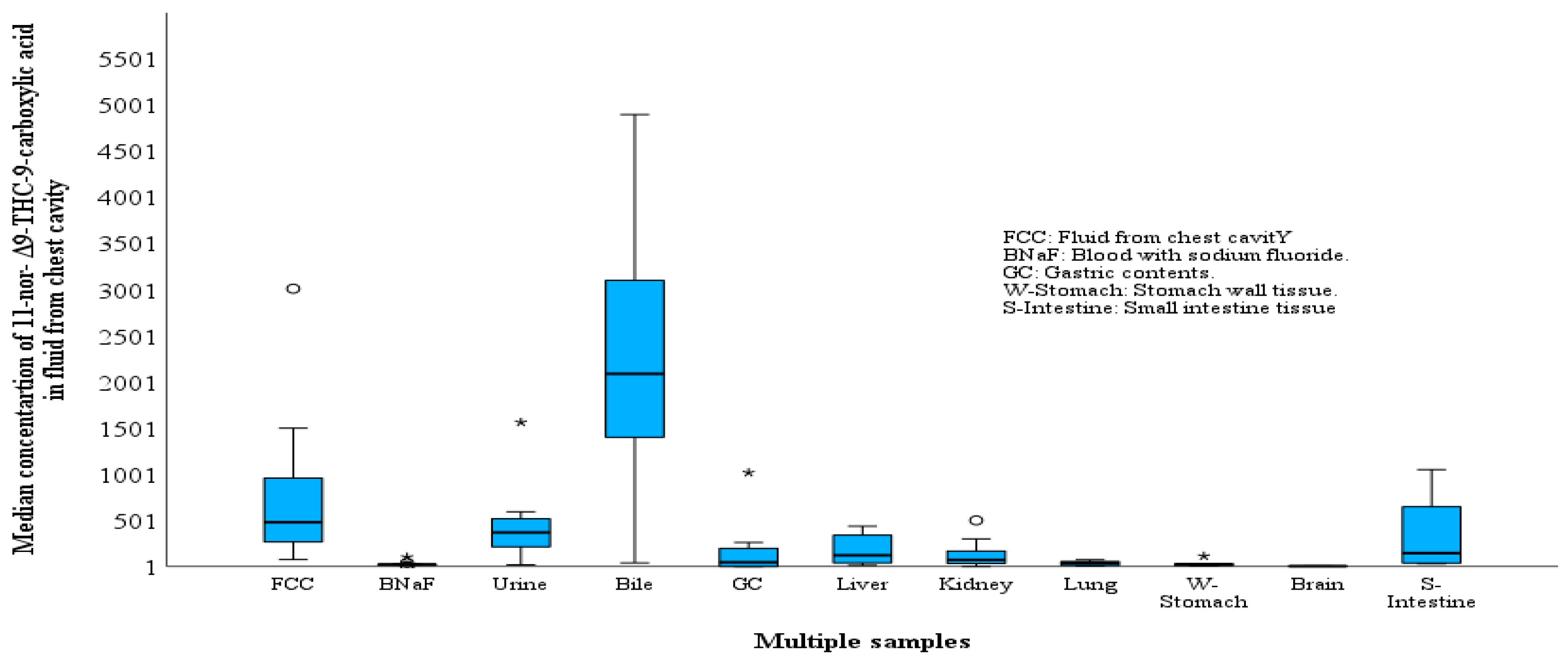
3.2.1. THC-COOH in FCC
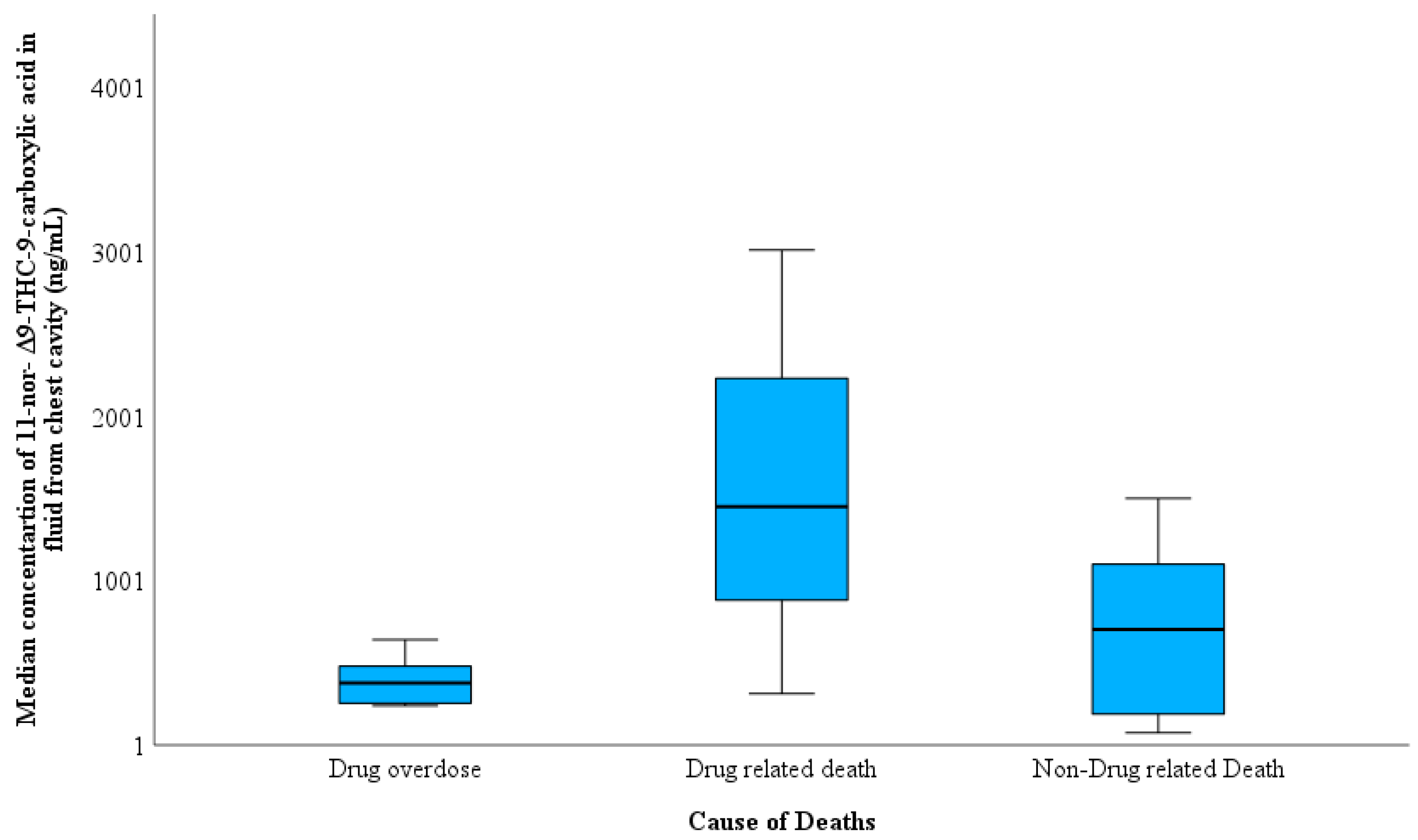
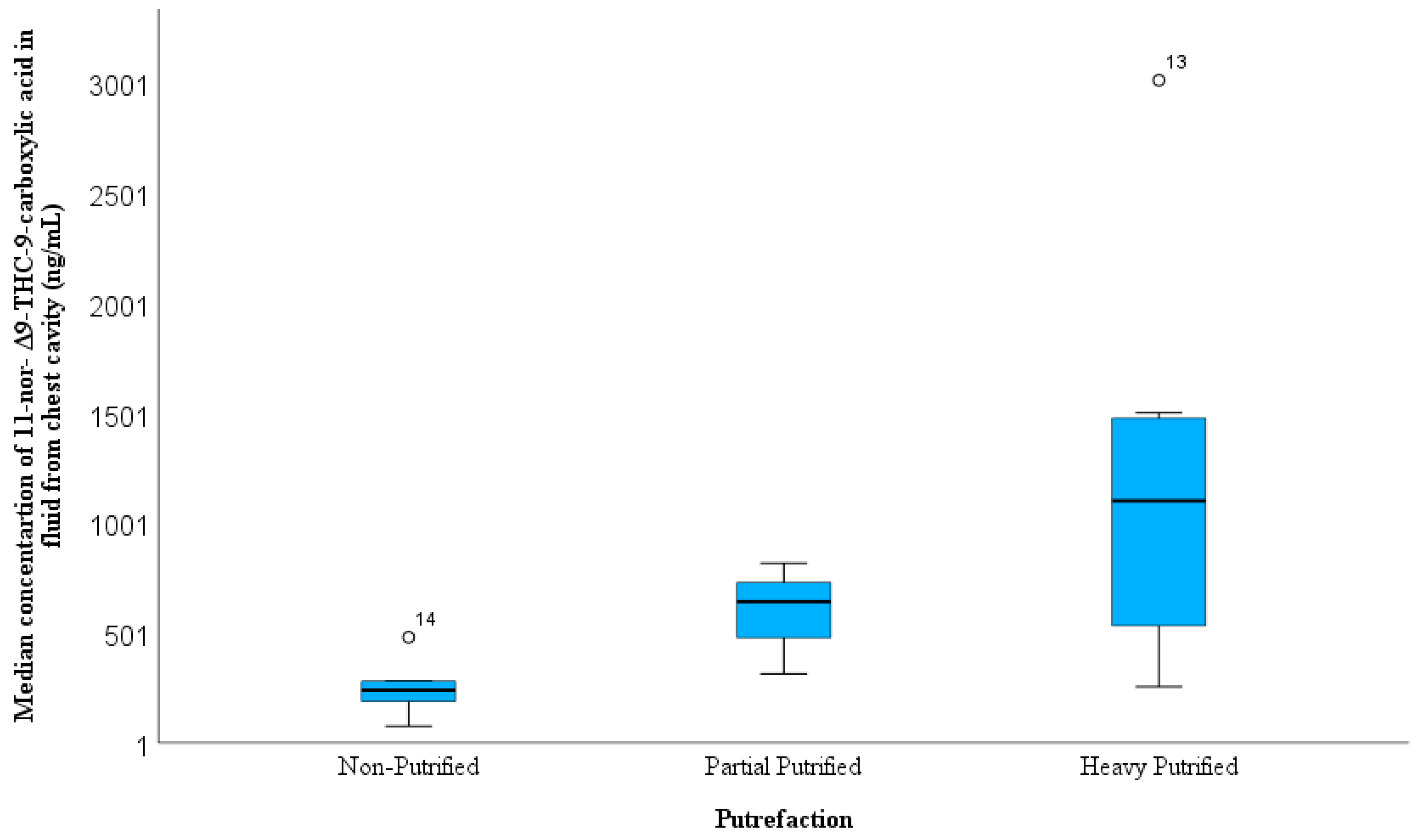
3.2.2. Cause and Manner of Death
3.2.3. History of Drug Abuse, PMIs, and BMI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chandra, S.; Radwan, M.M.; Majumdar, C.G.; Church, J.C.; Freeman, T.P.; ElSohly, M.A. New Trends in Cannabis Potency in USA and Europe during the Last Decade (2008–2017). Eur. Arch. Psychiatry Clin. Neurosci. 2019, 269, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Cliburn, K.D.; Huestis, M.A.; Wagner, J.R.; Kemp, P.M. Cannabinoid Distribution in Fatally-Injured Pilots’ Postmortem Fluids and Tissues. Forensic Sci. Int. 2021, 329, 111075. [Google Scholar] [CrossRef]
- Lewis, B.; Fleeger, T.; Judge, B.; Riley, B.; Jones, J.S. Acute Toxicity Associated with Cannabis Edibles Following Decriminalization of Marijuana in Michigan. Am. J. Emerg. Med. 2021, 46, 732–735. [Google Scholar] [CrossRef] [PubMed]
- Wickens, C.M.; Ialomiteanu, A.R.; di Ciano, P.; Stoduto, G.; Mann, R.E. Use of Cannabis and/or Prescription Opioids among Adult Drivers in Ontario, Canada: Prevalence and Association with Motor Vehicle Collisions. J. Transp. Health 2021, 22, 101091. [Google Scholar] [CrossRef]
- Shirah, B.H.; Ahmed, M.M. The Use of Cannabis for Medical Purposes in the Arab World. Med. Cannabis Cannabinoids 2021, 4, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Al-Asmari, A.I.; Alharbi, H.; Al-Zahrani, A.E.; Zughaibi, T.A. Heroin-Related Fatalities in Jeddah, Saudi Arabia, between 2008 and 2018. Toxics 2023, 11, 248. [Google Scholar] [CrossRef]
- Al-Asmari, A.I. Methamphetamine-Related Postmortem Cases in Jeddah, Saudi Arabia. Forensic Sci. Int. 2021, 321, 110746. [Google Scholar] [CrossRef]
- Cliburn, K.D.; Huestis, M.A.; Wagner, J.R.; Kemp, P.M. Identification and Quantification of Cannabinoids in Postmortem Fluids and Tissues by Liquid Chromatography-Tandem Mass Spectrometry. J. Chromatogr. A 2021, 1652, 462345. [Google Scholar] [CrossRef] [PubMed]
- Al-Asmari, A.I. Method for Postmortem Quantification of Δ9-Tetrahydrocannabinol and Metabolites Using LC-MS-MS. J. Anal. Toxicol. 2019, 43, 703–719. [Google Scholar] [CrossRef]
- Ashton, C.H. Pharmacology and Effects of Cannabis: A Brief Review. Br. J. Psychiatry 2001, 178, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Saenz, S.R.; Lewis, R.J.; Angier, M.K.; Wagner, J.R. Postmortem Fluid and Tissue Concentrations of THC, 11-OH-THC and THC-COOH. J. Anal. Toxicol. 2017, 41, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Fabritius, M.; Staub, C.; Mangin, P.; Giroud, C. Distribution of Free and Conjugated Cannabinoids in Human Bile Samples. Forensic Sci. Int. 2012, 223, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Lemos, N.P.; Ingle, E.A. Cannabinoids in Postmortem Toxicology. J. Anal. Toxicol. 2011, 35, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Gronewold, A.; Skopp, G. A Preliminary Investigation on the Distribution of Cannabinoids in Man. Forensic Sci. Int. 2011, 210, e7–e11. [Google Scholar] [CrossRef] [PubMed]
- Al-Asmari, A.I. Method for Postmortem Tissue Quantification of Δ9-Tetrahydrocannabinol and Metabolites Using LC–MS-MS. J. Anal. Toxicol. 2020, 44, 718–733. [Google Scholar] [CrossRef]
- Kemp, P.M.; Cardona, P.S.; Chaturvedi, A.K.; Soper, J.W. Distribution of Δ9-Tetrahydrocannabinol and 11-Nor-9-Carboxy-Δ9-Tetrahydrocannabinol Acid in Postmortem Biological Fluids and Tissues From Pilots Fatally Injured in Aviation Accidents. J. Forensic Sci. 2015, 60, 942–949. [Google Scholar] [CrossRef]
- Zughaibi, T.A.; Al-Qumsani, L.; Mirza, A.A.; Almostady, A.; Basrawi, J.; Tabrez, S.; Alsolami, F.; Al-Makki, R.; Al-Ghamdi, S.; Al-Ghamdi, A.; et al. Comparison between Blood, Non-Blood Fluids and Tissue Specimens for the Analysis of Cannabinoid Metabolites in Cannabis-Related Post-Mortem Cases. Forensic Sci. 2023, 3, 330–344. [Google Scholar] [CrossRef]
- Matuszewski, B.K.; Constanzer, M.L.; Chavez-Eng, C.M. Strategies for the Assessment of Matrix Effect in Quantitative Bioanalytical Methods Based on HPLC-MS/MS. Anal. Chem. 2003, 75, 3019–3030. [Google Scholar] [CrossRef]
- ANSI/ASB Standard 036; Method Validation in Forensic Toxicology. American Academy of Forensic Sciences Standards Board: Colorado Springs, CO, USA, 2019.
- Kemp, P.M.; Abukhalaf, I.K.; Manno, J.E.; Manno, B.R.; Alford, D.D.; Mc Williams, M.E.; Nixon, F.E.; Fitzgerald, M.J.; Reeves, R.R.; Wood, M.J. Cannabinoids in Humans. Ii. the Influence of Three Methods of Hydrolysis on the Conentration of Thc and Two Metabolites in Urine. J. Anal. Toxicol. 1995, 19, 292–298. [Google Scholar] [CrossRef]
- Duflou, J.; Darke, S.; Easson, J. Morphine Concentrations in Stomach Contents of Intravenous Opioid Overdose Deaths. J. Forensic Sci. 2009, 54, 1181–1184. [Google Scholar] [CrossRef]
- Moriya, F.; Hashimoto, Y. Distribution of Free and Conjugated Morphine in Body Fluids and Tissues in a Fatal Heroin Overdose: Is Conjugated Morphine Stable in Postmortem Specimens? J. Forensic Sci. 1997, 42, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Skopp, G. Preanalytic Aspects in Postmortem Toxicology. Forensic Sci. Int. 2004, 142, 75–100. [Google Scholar] [CrossRef]
- Karschner, E.L.; Schwilke, E.W.; Lowe, R.H.; Darwin, W.D.; Pope, H.G.; Herning, R.; Cadet, J.L.; Huestis, M.A. Do Δ9-Tetrahydrocannabinol Concentrations Indicate Recent Use in Chronic Cannabis Users? Addiction 2009, 104, 2041–2048. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Case Information | Age | PMI | Sign of Putrefaction | Co-Ingested Substances | Location | Manner of Death | Cause of Death |
|---|---|---|---|---|---|---|---|---|
| 1. | Deceased with history of chronic drug used was found dead in a car. | 36 | 24 | Heavily decomposed | Amphetamine | Outdoor | Accidental injury | Non-Drug related Death |
| 2. | Fall from height, died at hospital | 33 | 24 | Non-putrefied | None | Outdoor | Accidental injury | Non-Drug related Death |
| 3. | Poly drug intoxication, history of drug abuse | 23 | 48 | Non-putrefied | Heroin metabolites (6-monoacetylmorphine, morphine and codeine) | Indoor | Accidental overdose | Drug overdose |
| Cocaine metabolites (Benzoylecgonine, ecgonine methyl ester), | ||||||||
| Alprazolam | ||||||||
| Pregabalin | ||||||||
| 4. | Poly drug intoxication, history of drug abuse | 23 | 48 | Non-putrefied | Heroin metabolites (6-monoacetylmorphine, morphine and codeine) | Indoor | Accidental overdose | Drug overdose |
| Ethanol | ||||||||
| Alprazolam, | ||||||||
| Tramadol | ||||||||
| 5. | Gun shooting | 18 | 24 | Partially putrefied | None | Indoor | Homicidal | Non-Drug related Death |
| 6. | Fall from height | 26 | 72 | Heavily decomposed | Methamphetamine | Outdoor | Homicidal | Non-Drug related Death |
| Amphetamine | ||||||||
| Alprazolam | ||||||||
| Tramadol | ||||||||
| 7. | Found dead on the street | 40 | 96 | Heavily decomposed | Amphetamine | Outdoor | Suicidal | Non-Drug related Death |
| 8. | Found dead in his car | 22 | 24 | Heavily decomposed | Heroin metabolites (6-monoacetylmorphine, morphine and codeine) | Outdoor | Accidental overdose | Drug overdose |
| Acetone | ||||||||
| 9. | Drug overdose | 21 | 130 | Partially putrefied | Ethanol | Indoor | Accidental overdose | Drug overdose |
| Barbiturates | ||||||||
| Clonazepam | ||||||||
| 10. | The deceased was found hanging | 22 | 24 | Non-putrefied | Amphetamine | Indoor | Suicidal | Non-Drug related Death |
| Gabapentin | ||||||||
| Alprazolam | ||||||||
| 11. | Drug overdose | 50 | 320 | Heavily decomposed | Amphetamine | Indoor | Accidental overdose | Drug overdose |
| Ethanol | ||||||||
| Tramadol | ||||||||
| Lidocaine | ||||||||
| 12. | Car accident | 42 | 72 | Partially putrefied | Amphetamine | Outdoor | Accidental injury | Drug related death |
| 13. | Found dead in his car, heavily decomposed | 47 | 24 | Heavily decomposed | Ethanol | Indoor | Accidental overdose | Drug related death |
| Amphetamine | ||||||||
| 14. | Polydrug intoxication, history of drug abuse | 21 | 48 | Non-putrefied | Heroin metabolites (6-monoacetylmorphine, morphine and codeine) | Indoor | Accidental overdose | Drug overdose |
| Ethanol | ||||||||
| Alprazolam | ||||||||
| Tramadol | ||||||||
| 15. | Fall from height. | 37 | 120 | Heavily decomposed | Amphetamine, | Indoor | Accidental injury | Drug related death |
| Tadalafil |
| Number of Cases | Median | Minimum | Maximum | ||
|---|---|---|---|---|---|
| Blood with Sodium Fluoride | Δ9-tetrahydrocannabinol (THC) | 10 | 10 | 102 | 20.0 |
| 11-norΔ9-THC-9-carboxylic acid | 11 | 20.0 | 2.0 | 100.0 | |
| 11-hydroxy-Δ9-THC | 9 | 3.0 | 1.0 | 10.0 | |
| Fluid from Chest Cavity | THC | 0 | n.a. & | n.a. | n.a. |
| 11-nor-Δ9-THC-9-carboxylic acid | 15 | 480.0 | 80.0 | 3010.0 | |
| 11-hydroxy-Δ9-THC | 0 | n.a. | n.a. | n.a. | |
| Urine | THC | 4 | 3.0 | 2.0 | 10.0 |
| 11-nor-Δ9-THC-9-carboxylic acid | 10 | 370.0 | 20.0 | 1560.0 | |
| 11-hydroxy-Δ9-THC | 6 | 2.0 | Tr # | 4.0 | |
| Bile | THC | 8 | 120.0 | 6.0 | 250.0 |
| 11-nor-Δ9-THC-9-carboxylic acid | 13 | 210.0 | 40.0 | 33,000.0 | |
| 11-hydroxy-Δ9-THC | 13 | 110.0 | 3.0 | 1350.0 | |
| Gastric Contents | THC | 10 | 80.0 | 5.0 | 280.0 |
| 11-nor-Δ9-THC-9-carboxylic acid | 9 | 50.0 | 1.0 | 1020.0 | |
| 11-hydroxy-Δ9-THC | 4 | 4.0 | 1.0 | 30.0 | |
| Liver | THC | 4 | 2.0 | 1.0 | 30.0 |
| 11-nor-Δ9-THC-9-carboxylic acid | 14 | 120.0 | 14.0 | 440.0 | |
| 11-hydroxy-Δ9-THC | 2 | 1.0 | Tr | 1.0 | |
| Kidney | THC | 7 | 2.0 | 1.0 | 70.0 |
| 11-nor-Δ9-THC-9-carboxylic acid | 14 | 70.0 | 1.0 | 500.0 | |
| 11-hydroxy-Δ9-THC | 3 | 1.0 | 1.0 | 140.0 | |
| Brain | THC | 3 | 20.0 | 14.0 | 20.0 |
| 11-nor-Δ9-THC-9-carboxylic acid | 3 | 4.0 | 4.0 | 10.0 | |
| 11-hydroxy-Δ9-THC | 4 | 2.0 | 1.0 | 10.5 | |
| Stomach Wall Tissue | THC | 6 | 30.0 | 4.0 | 470.0 |
| 11-nor-Δ9-THC-9-carboxylic acid | 5 | 30.0 | 6.0 | 110.0 | |
| 11-hydroxy-Δ9-THC | 0 | n.a. | n.a. | n.a. | |
| Lung | THC | 5 | 20.0 | 3.0 | 40.0 |
| 11-nor-Δ9-THC-9-carboxylic acid | 5 | 40.0 | 4.0 | 75.0 | |
| 11-hydroxy-Δ9-THC | 1 | n.a. | n.a. | n.a. | |
| Small Intestine tissue | THC | 0 | n.a. | n.a. | n.a. |
| 11-nor-Δ9-THC-9-carboxylic acid | 4 | 145.0 | 30.0 | 1050.0 | |
| 11-hydroxy-Δ9-THC | 2 | 38.5 | 20.0 | 60.0 |
| Blood with Sodium Fluoride | Fluid from Chest Cavity | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Δ9-Tetrahydrocannabinol | 11-Nor-Δ9-THC-9-Carboxylic Acid | 11-hydroxy-Δ9-THC | 11-nor-Δ9-THC-9-Carboxylic Acid | ||||||||||
| NS * | Median | Range | NS * | Median | Range | NS * | Median | Range | NS * | Median | Range | ||
| Cause of Death | Drug overdose | 2 | 15 | 10.0–19 | 3 | 24 | 17.0–103.0 | 2 | 5 | 3.0–10 | 6 | 378 | 240.0–1100.0 |
| Drug related death | 3 | 7 | 2.0–10 | 3 | 18 | 2.0–40.0 | 2 | 1 | 0.5–1 | 3 | 1450 | 314.0–3010.0 | |
| Non-Drug related Death | 5 | 6 | 1.0–20 | 5 | 22 | 6.0–26.0 | 5 | 3 | 0.5–8 | 6 | 703 | 76.0–1500.0 | |
| Manner of Death | Accidental Overdose | 3 | 10 | 7.0–20 | 4 | 32 | 17.0–103.0 | 3 | 3 | 1–7 | 7 | 476 | 240.0–3010.0 |
| Accidental injury | 3 | 10 | 2.0–20 | 3 | 18 | 2.0–22.0 | 2 | 4 | 1–10 | 4 | 452 | 76.0–1450.0 | |
| Homicidal | 2 | 9 | 4.0–13 | 2 | 16 | 6.0–26.0 | 2 | 3 | n.a | 2 | 1158 | 816.2–1500.0 | |
| Suicidal | 2 | 3 | 1.2–6 | 2 | 22 | n.a | 2 | 1 | n.a | 2 | 645 | n.a. | |
| Location of death | Indoor | 6 | 9 | 1.2–20 | 7 | 21 | 6.0–103.0 | 5 | 3 | 1–7 | 8 | 461 | 189.0–3010.0 |
| Outdoor | 4 | 9 | 1.7–20 | 4 | 23 | 2.0–26.0 | 4 | 3 | 1–10 | 7 | 480 | 76.0–1500.0 | |
| Putrefaction | Non-putrefied | 4 | 15 | 1.2–20 | 4 | 22 | 17.0–103.0 | 4 | 5 | 0.5–8 | 5 | 240 | 76.0–480.0 |
| Partially putrefied | 2 | 3 | 1.7–4 | 3 | 6 | 2.0–24.0 | 2 | 2 | n.a | 3 | 642 | 314.0–816.2 | |
| Heavy putrefied | 4 | 9 | 6–13 | 4 | 25 | 18.0–40.0 | 3 | 2 | 0.5–3 | 7 | 1100 | 255.0–3010.0 | |
| Poly drug used | No | 2 | 12 | 4.0–20 | 2 | 14 | 6.0–22.0 | 2 | 6 | 3.0–8 | 2 | 446 | 76.0–816.2 |
| Yes | 8 | 9 | 1.2–20 | 9 | 23 | 2.0–103.0 | 7 | 2 | 0.5–7 | 13 | 480 | 189.0–3010.0 | |
| History of drug of abuse | No | 4 | 9 | 1.2–20 | 4 | 22 | 6.0–26.0 | 4 | 3 | 1–8 | 6 | 535 | 76.0–1500.0 |
| Yes | 6 | 9 | 1.7–19 | 7 | 23 | 2.0–103.0 | 5 | 2 | 1–7 | 9 | 476 | 240.0–3010.0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zughaibi, T.A.; Alharbi, H.; Al-Saadi, A.; Alzahrani, A.E.; Al-Asmari, A.I. 11-Nor-9-Carboxy Tetrahydrocannabinol Distribution in Fluid from the Chest Cavity in Cannabis-Related Post-Mortem Cases. Toxics 2023, 11, 740. https://doi.org/10.3390/toxics11090740
Zughaibi TA, Alharbi H, Al-Saadi A, Alzahrani AE, Al-Asmari AI. 11-Nor-9-Carboxy Tetrahydrocannabinol Distribution in Fluid from the Chest Cavity in Cannabis-Related Post-Mortem Cases. Toxics. 2023; 11(9):740. https://doi.org/10.3390/toxics11090740
Chicago/Turabian StyleZughaibi, Torki A., Hassan Alharbi, Adel Al-Saadi, Abdulnasser E. Alzahrani, and Ahmed I. Al-Asmari. 2023. "11-Nor-9-Carboxy Tetrahydrocannabinol Distribution in Fluid from the Chest Cavity in Cannabis-Related Post-Mortem Cases" Toxics 11, no. 9: 740. https://doi.org/10.3390/toxics11090740
APA StyleZughaibi, T. A., Alharbi, H., Al-Saadi, A., Alzahrani, A. E., & Al-Asmari, A. I. (2023). 11-Nor-9-Carboxy Tetrahydrocannabinol Distribution in Fluid from the Chest Cavity in Cannabis-Related Post-Mortem Cases. Toxics, 11(9), 740. https://doi.org/10.3390/toxics11090740