
Risk Assessment of Phthalates and Their Metabolites in Hospitalized Patients: A Focus on Di- and Mono-(2-ethylhexyl) Phthalates Exposure from Intravenous Plastic Bags

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Sample Collection
2.3. Extraction Procedures
2.3.1. Plastic IV Bags for GC–MS Analysis
2.3.2. IV Bag Solutions for SPME-GC–MS/MS Analysis
2.4. Method Validation
2.4.1. Calibration Curve
2.4.2. Limit of Detection and Limit of Quantification
2.4.3. Instrumental Analysis
2.5. Analysis of Data
2.5.1. Content Calculation
2.5.2. Risk Assessment for Phthalate Exposure and Hazard Index
2.5.3. Risk Assessment for Simulated MEHP Exposure
3. Results
3.1. GC–MS Analysis of IV Bags
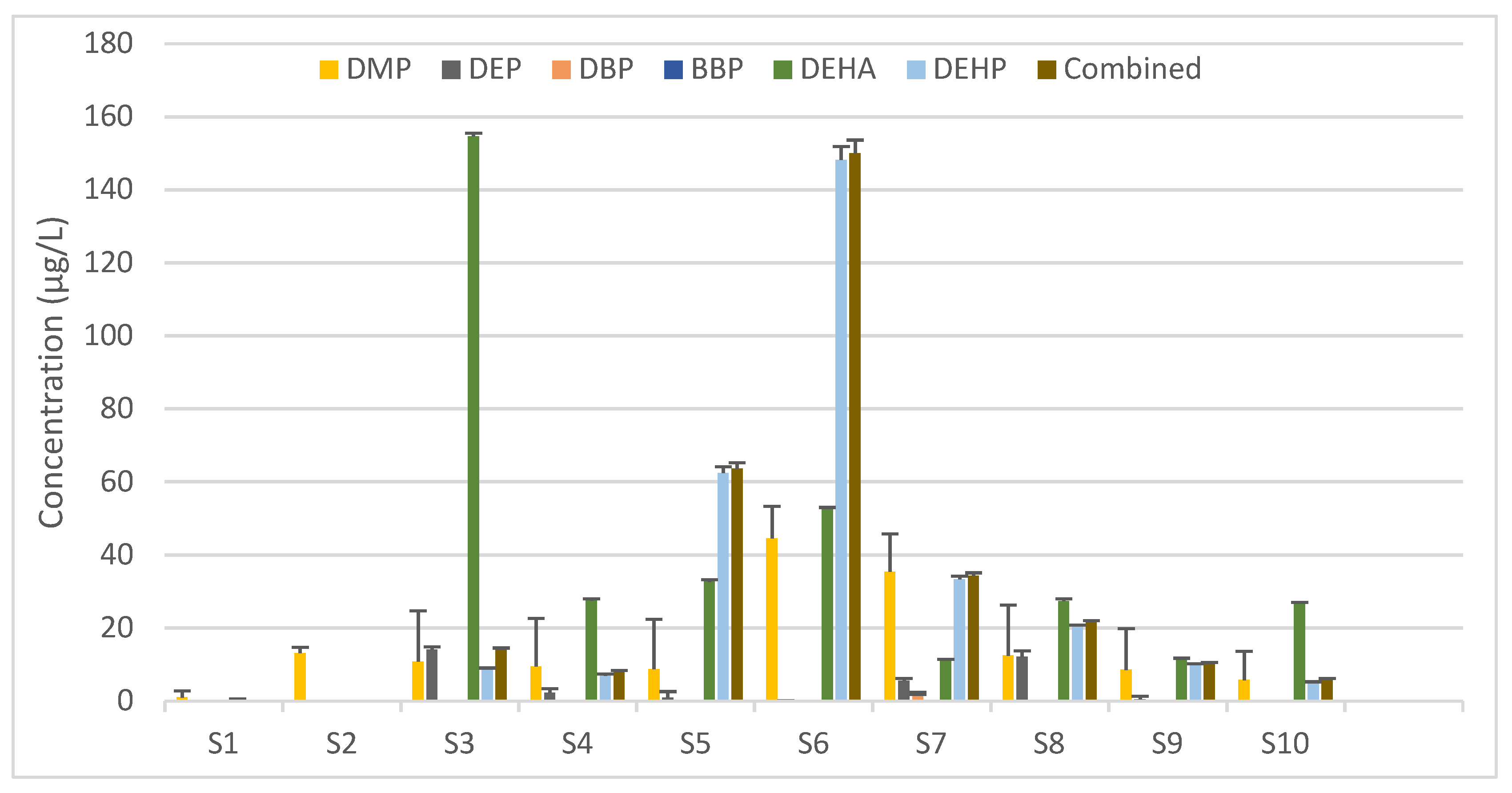
3.2. SPME-GC–MS/MS Analysis of IV Solutions
3.3. Risk Assessment for Phthalate Exposure
3.4. Risk Assessment for MEHP Exposure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Titow, W.V. PVC Plastics; Properties, Processing, and Applications. 1990. Available online: https://link.springer.com/content/pdf/bfm:978-94-011-3834-5/1.pdf (accessed on 16 May 2022).
- Grosu, E. Applications of Polyvinylchloride (PVC)/Thermoplastic Nano-, Micro-and Macroblends. In Polyvinylchloride-Based Blends; Springer: Berlin/Heidelberg, Germany, 2022; pp. 75–89. Available online: https://link.springer.com/chapter/10.1007/978-3-030-78455-3_4 (accessed on 16 May 2022).
- Chiellini, F.; Ferri, M.; Morelli, A.; Dipaola, L.; Latini, G. Perspectives on Alternatives to Phthalate Plasticized Poly (Vinyl Chloride) in Medical Devices Applications. Prog. Polym. Sci. 2013, 38, 1067–1088. [Google Scholar] [CrossRef]
- Rowdhwal, S.S.S.; Chen, J. Toxic Effects of Di-2-Ethylhexyl Phthalate: An Overview. BioMed Res. Int. 2018, 2018, 1750368. [Google Scholar] [CrossRef] [PubMed]
- Schettler, T.E.D. Human Exposure to Phthalates via Consumer Products. Int. J. Androl. 2006, 29, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Prasad, B. Phthalate Pollution: Environmental Fate and Cumulative Human Exposure Index Using the Multivariate Analysis Approach. Environ. Sci. Processes Impacts 2021, 23, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Kostić, S.I.; Andjelkovic, D.T.; Andjelkovic, H.D.; Cvetković, P.T.; Pavlović, D. Determination of Di(2-Ethylhexyl) Phthalate in Plastic Medical Devices. Hem. Ind. 2016, 70, 159–164. [Google Scholar] [CrossRef]
- Veiga, M.; Bohrer, D.; Nascimento, P.; Ramirez, A.; Carvalho, L.; Binotto, R. Migration of Phthalate-Based Plasticizers from PVC and Non-PVC Containers and Medical Devices. J. Braz. Chem. Soc. 2012, 23, 72–77. [Google Scholar] [CrossRef][Green Version]
- Karwacka, A.; Zamkowska, D.; Radwan, M.; Jurewicz, J. Exposure to Modern, Widespread Environmental Endocrine Disrupting Chemicals and Their Effect on the Reproductive Potential of Women: An Overview of Current Epidemiological Evidence. Hum. Fertil. 2019, 22, 2–25. [Google Scholar] [CrossRef] [PubMed]
- Kay, V.R.; Chambers, C.; Foster, W.G. Reproductive and Developmental Effects of Phthalate Diesters in Females. Crit. Rev. Toxicol. 2013, 43, 200–219. [Google Scholar] [CrossRef] [PubMed]
- Latini, G.; Del Vecchio, A.; Massaro, M.; Verrotti, A.; De Felice, C. Phthalate Exposure and Male Infertility. Toxicology 2006, 226, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Erkekoglu, P.; Kocer-Gumusel, B. Genotoxicity of Phthalates. Toxicol. Mech. Methods 2014, 24, 616–626. [Google Scholar] [CrossRef]
- Ferguson, K.K.; McElrath, T.F.; Meeker, J.D. Environmental Phthalate Exposure and Preterm Birth. JAMA Pediatrics 2014, 168, 61–67. [Google Scholar] [CrossRef]
- Qian, X.; Li, J.; Xu, S.; Wan, Y.; Li, Y.; Jiang, Y.; Zhao, H.; Zhou, Y.; Liao, J.; Liu, H.; et al. Prenatal Exposure to Phthalates and Neurocognitive Development in Children at Two Years of Age. Environ. Int. 2019, 131, 105023. [Google Scholar] [CrossRef] [PubMed]
- Toft, G.; Jönsson, B.A.G.; Lindh, C.H.; Jensen, T.K.; Hjollund, N.H.; Vested, A.; Bonde, J.P. Association between Pregnancy Loss and Urinary Phthalate Levels around the Time of Conception. Environ. Health Perspect 2012, 120, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Sathyanarayana, S.; Hauser, R. Phthalate Exposure and Children’s Health. Curr. Opin. Pediatrics 2013, 25, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.B.; Chen, H.Y.; Su, P.H.; Huang, P.C.; Sun, C.W.; Wang, C.J.; Hsiung, C.A.; Wang, S.L. Fetal and Childhood Exposure to Phthalate Diesters and Cognitive Function in Children Up to 12 Years of Age: Taiwanese Maternal and Infant Cohort Study. PLoS ONE 2015, 10, e0131910. [Google Scholar] [CrossRef]
- Calafat, A.M.; Ye, X.; Silva, M.J.; Kuklenyik, Z.; Needham, L.L. Human Exposure Assessment to Environmental Chemicals Using Biomonitoring. Int. J. Androl. 2006, 29, 166–171. [Google Scholar] [CrossRef]
- Frederiksen, H.; Skakkebaek, N.E.; Andersson, A.-M. Metabolism of Phthalates in Humans. Mol. Nutr. Food Res. 2007, 51, 899–911. [Google Scholar] [CrossRef]
- Guo, Y.; Wu, Q.; Kannan, K. Phthalate Metabolites in Urine from China, and Implications for Human Exposures. Environ. Int. 2011, 37, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, S.; Masai, E.; Kamimura, N.; Takahashi, K.; Anderson, R.C.; Faisal, P.A. Phthalates Impact Human Health: Epidemiological Evidences and Plausible Mechanism of Action. J. Hazard. Mater. 2017, 340, 360–383. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wu, D.; Guo, Y.; Mao, W.; Zhao, N.; Zhao, M.; Jin, H. Phthalate Metabolites in Paired Human Serum and Whole Blood. Sci. Total Environ. 2022, 824, 153792. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhou, Y.; Tang, C.; He, Y.; Wu, J.; Chen, Y.; Jiang, Q. Urinary Phthalate Metabolites Are Associated with Body Mass Index and Waist Circumference in Chinese School Children. PLoS ONE 2013, 8, e56800. [Google Scholar] [CrossRef] [PubMed]
- Hatch, E.E.; Nelson, J.W.; Qureshi, M.M.; Weinberg, J.; Moore, L.L.; Singer, M.; Webster, T.F. Association of Urinary Phthalate Metabolite Concentrations with Body Mass Index and Waist Circumference: A Cross-Sectional Study of NHANES Data, 1999–2002. Environ. Health 2008, 7, 27. [Google Scholar] [CrossRef]
- Dalgaard, M.; Nellemann, C.; Lam, H.R.; Sørensen, I.K.; Ladefoged, O. The Acute Effects of Mono(2-Ethylhexyl)Phthalate (MEHP) on Testes of Prepubertal Wistar Rats. Toxicol. Lett. 2001, 122, 69–79. [Google Scholar] [CrossRef]
- Miller, W.L.; Auchus, R.J. The Molecular Biology, Biochemistry, and Physiology of Human Steroidogenesis and Its Disorders. Endocr. Rev. 2011, 32, 81–151. [Google Scholar] [CrossRef] [PubMed]
- Conti, I.; Simioni, C.; Varano, G.; Brenna, C.; Costanzi, E.; Neri, L.M. Legislation to Limit the Environmental Plastic and Microplastic Pollution and Their Influence on Human Exposure. Environ. Pollut. 2021, 288, 117708. [Google Scholar] [CrossRef] [PubMed]
- Substances Restricted under REACH-ECHA. Available online: https://echa.europa.eu/substances-restricted-under-reach (accessed on 21 June 2022).
- Scientific Committee on Emerging and Newly-Identified Health Risks Opinion; The Safety of Medical Devices Containing Dehp-Plasticized Pvc or other Plasticizers on Neonates and other Groups Possibly At Risk. 2008. Available online: https://ec.europa.eu/health/archive/ph_risk/committees/04_scenihr/docs/scenihr_o_014.pdf (accessed on 16 May 2022).
- Scientific Committee on Emerging and Newly-Identified Health Risks Opinion; The Safety of Medical Devices Containing DEHP-Plasticized PVC or other Plasticizers on Neonates and Other Groups Possibly at Risk. 2015. Available online: https://ec.europa.eu/health/scientific_committees/emerging/docs/scenihr_o_047.pdf (accessed on 16 May 2022).
- Bernard, L.; Cueff, R.; Breysse, C.; Decaudin, B.; Sautou, V. Migrability of PVC Plasticizers from Medical Devices into a Simulant of Infused Solutions. Int. J. Pharm. 2015, 485, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Bourdeaux, D.; Yessaad, M.; Chennell, P.; Larbre, V.; Eljezi, T.; Bernard, L.; Sautou, V. Analysis of PVC Plasticizers in Medical Devices and Infused Solutions by GC–MS. J. Pharm. Biomed. Anal. 2016, 118, 206–213. [Google Scholar] [CrossRef]
- Bui, T.T.; Giovanoulis, G.; Cousins, A.P.; Magnér, J.; Cousins, I.T.; de Wit, C.A. Human Exposure, Hazard and Risk of Alternative Plasticizers to Phthalate Esters. Sci. Total Environ. 2016, 541, 451–467. [Google Scholar] [CrossRef]
- Consumer Products|Bimonthly Bulletin|. May 2021. Available online: https://www.eurofins.com/consumer-product-testing/media-centre/news/consumer-products-bimonthly-bulletin-may-2021/ (accessed on 21 June 2022).
- Zgheib, R.; Nakad, Z.; Saab, Y. Antibiotics in Lebanese Surface Waters: Estimation of Population Exposure and Identification of High-Risk Drugs. J. Environ. Pollut. Control 2021, 4, 1. [Google Scholar] [CrossRef]
- Saab, Y.; Nakad, Z.; Rahme, R. Chemotherapeutic Drugs in Lebanese Surface Waters: Estimation of Population Exposure and Identification of High-Risk Drugs. Sustain. Environ. Res. 2021, 31, 31. [Google Scholar] [CrossRef]
- Nassour, C.; Barton, S.J.; Nabhani-Gebara, S.; Saab, Y.; Barker, J. Occurrence of Anticancer Drugs in the Aquatic Environment: A Systematic Review. Env. Sci Pollut. Res. 2020, 27, 1339–1347. [Google Scholar] [CrossRef] [PubMed]
- Armbruster, D.A.; Pry, T. Limit of Blank, Limit of Detection and Limit of Quantitation. Clin. Biochem. Rev. 2008, 29 (Suppl. S1), S49–S52. [Google Scholar] [PubMed]
- Mani, D.R.; Abbatiello, S.E.; Carr, S.A. Statistical Characterization of Multiple-Reaction Monitoring Mass Spectrometry (MRM-MS) Assays for Quantitative Proteomics. BMC Bioinform. 2012, 13 (Suppl. S16), S9. [Google Scholar] [CrossRef] [PubMed]
- Nundy, S.; Kakar, A.; Bhutta, Z.A. How to Calculate an Adequate Sample Size? In How to Practice Academic Medicine and Publish from Developing Countries? A Practical Guide; Nundy, S., Kakar, A., Bhutta, Z.A., Eds.; Springer: Singapore, 2022; pp. 81–93. ISBN 9789811652486. [Google Scholar]
- Korfali, S.I.; Sabra, R.; Jurdi, M.; Taleb, R.I. Assessment of Toxic Metals and Phthalates in Children’s Toys and Clays. Arch. Env. Contam. Toxicol. 2013, 65, 368–381. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-J.; Guo, J.-L.; Xue, J.-C.; Bai, C.-L.; Guo, Y. Phthalate Metabolites: Characterization, Toxicities, Global Distribution, and Exposure Assessment. Env. Pollut. 2021, 291, 118106. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W.A.C.; Castle, L.; Hird, S.; Jeffery, J.; Scotter, M.J. A Twenty-Volunteer Study Using Deuterium Labelling to Determine the Kinetics and Fractional Excretion of Primary and Secondary Urinary Metabolites of Di-2-Ethylhexylphthalate and Di-Iso-Nonylphthalate. Food Chem. Toxicol. 2011, 49, 2022–2029. [Google Scholar] [CrossRef]
- Koch, H.M.; Bolt, H.M.; Preuss, R.; Angerer, J. New Metabolites of Di (2-Ethylhexyl) Phthalate (DEHP) in Human Urine and Serum after Single Oral Doses of Deuterium-Labelled DEHP. Arch. Toxicol. 2005, 79, 367–376. [Google Scholar] [CrossRef]
- Urine Output; CDC. Available online: https://www.cdc.gov/dengue/training/cme/ccm/page57297.html (accessed on 29 March 2022).
- European Union Directive. 2007. Available online: https://eur-lex.europa.eu/legal-content/en/ALL/?uri=CELEX%3A32007L0047 (accessed on 14 April 2021).
- Malarvannan, G.; Onghena, M.; Verstraete, S.; van Puffelen, E.; Jacobs, A.; Vanhorebeek, I.; Verbruggen, S.; Joosten, K.F.M.; Van den Berghe, G.; Jorens, P.G.; et al. Phthalate and Alternative Plasticizers in Indwelling Medical Devices in Pediatric Intensive Care Units. J. Hazard Mater. 2019, 363, 64–72. [Google Scholar] [CrossRef]
- Genay, S.; Luciani, C.; Décaudin, B.; Kambia, N.; Dine, T.; Azaroual, N.; Di Martino, P.; Barthélémy, C.; Odou, P. Experimental Study on Infusion Devices Containing Polyvinyl Chloride: To What Extent Are They Di(2-Ethylhexyl)Phthalate-Free? Int. J. Pharm. 2011, 412, 47–51. [Google Scholar] [CrossRef]
- Erythropel, H.C.; Maric, M.; Nicell, J.A.; Leask, R.L.; Yargeau, V. Leaching of the Plasticizer Di(2-Ethylhexyl)Phthalate (DEHP) from Plastic Containers and the Question of Human Exposure. Appl. Microbiol. Biotechnol. 2014, 98, 9967–9981. [Google Scholar] [CrossRef]
- Latini, G.; Ferri, M.; Chiellini, F. Materials Degradation in PVC Medical Devices, DEHP Leaching and Neonatal Outcomes. Curr. Med. Chem. 2010, 17, 2979–2989. [Google Scholar] [CrossRef] [PubMed]
- Arbin, A.; Östelius, J. Determination by Electron-Capture Gas Chromatography of Mono- and Di(2-Ethylhexyl) Phthalate in Intravenous Solutions Stored in Poly(Vinyl Chloride) Bags. J. Chromatogr. A 1980, 193, 405–412. [Google Scholar] [CrossRef]
- dos Santos, M.S.; Budziak, D.; Martendal, E.; Carasek, E. Determination of Phthalates and Adipate in Physiological Saline Solutions by Solid-Phase Microextraction and Gas Chromatography. Anal. Sci. 2009, 25, 865–868. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Strac, I.V.; Pušić, M.; Gajski, G.; Garaj-Vrhovac, V. Presence of Phthalate Esters in Intravenous Solution Evaluated Using Gas Chromatography-Mass Spectrometry Method. J. Appl. Toxicol. 2013, 33, 214–219. [Google Scholar] [CrossRef]
- Kambia, K.; Dine, T.; Gressier, B.; Bah, S.; Germe, A.F.; Luyckx, M.; Brunet, C.; Michaud, L.; Gottrand, F. Evaluation of Childhood Exposure to Di(2-Ethylhexyl) Phthalate from Perfusion Kits during Long-Term Parenteral Nutrition. Int. J. Pharm. 2003, 262, 83–91. [Google Scholar] [CrossRef]
- Allwood, M.C.; Martin, H. The Extraction of Diethylhexylphthalate (DEHP) from Polyvinyl Chloride Components of Intravenous Infusion Containers and Administration Sets by Paclitaxel Injection. Int. J. Pharm. 1996, 127, 65–71. [Google Scholar] [CrossRef]
- Bohrer, D. Contamination and Contamination Control. In Pharmaceutical Manufacturing Handbook: Regulations and Quality; Gad, S.C., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2008. [Google Scholar]
- Demoré, B.; Vigneron, J.; Perrin, A.; Hoffman, M.A.; Hoffman, M. Leaching of Diethylhexyl Phthalate from Polyvinyl Chloride Bags into Intravenous Etoposide Solution. J. Clin. Pharm. 2002, 27, 139–142. [Google Scholar] [CrossRef]
- Sautou-Miranda, V.; Brigas, F.; Vanheerswynghels, S.; Chopineau, J. Compatibility of Paclitaxel in 5% Glucose Solution with ECOFLAC Low-Density Polyethylene Containers-Stability under Different Storage Conditions. Int. J. Pharm. 1999, 178, 77–82. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, H.; Kannan, K. A Review of Biomonitoring of Phthalate Exposures. Toxics 2019, 7, 21. [Google Scholar] [CrossRef]
- Mallow, E.B.; Fox, M.A. Phthalates and Critically Ill Neonates: Device-Related Exposures and Non-Endocrine Toxic Risks. J. Perinatol. 2014, 34, 892–897. [Google Scholar] [CrossRef]
- Jenkins, R.; Tackitt, S.; Gievers, L.; Iragorri, S.; Sage, K.; Cornwall, T.; O’Riordan, D.; Merchant, J.; Rozansky, D. Phthalate-Associated Hypertension in Premature Infants: A Prospective Mechanistic Cohort Study. Pediatr. Nephrol. 2019, 34, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- von Rettberg, H.; Hannman, T.; Subotic, U.; Brade, J.; Schaible, T.; Waag, K.L.; Loff, S. Use of Di(2-Ethylhexyl)Phthalate-Containing Infusion Systems Increases the Risk for Cholestasis. Pediatrics 2009, 124, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Engel, S.M.; Zhu, C.; Berkowitz, G.S.; Calafat, A.M.; Silva, M.J.; Miodovnik, A.; Wolff, M.S. Prenatal Phthalate Exposure and Performance on the Neonatal Behavioral Assessment Scale in a Multiethnic Birth Cohort. Neurotoxicology 2009, 30, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Ha, E.-H.; Kim, E.-J.; Park, H.; Ha, M.; Kim, J.-H.; Hong, Y.-C.; Chang, N.; Kim, B.-N. Prenatal Exposure to Phthalates and Infant Development at 6 Months: Prospective Mothers and Children’s Environmental Health (MOCEH) Study. Env. Health Perspect 2011, 119, 1495–1500. [Google Scholar] [CrossRef]
- Park, S.; Kim, B.-N.; Cho, S.-C.; Kim, Y.; Kim, J.-W.; Lee, J.-Y.; Hong, S.-B.; Shin, M.-S.; Yoo, H.J.; Im, H.; et al. Association between Urine Phthalate Levels and Poor Attentional Performance in Children with Attention-Deficit Hyperactivity Disorder with Evidence of Dopamine Gene-Phthalate Interaction. Int. J. Env. Res. Public Health 2014, 11, 6743–6756. [Google Scholar] [CrossRef]
- Yolton, K.; Xu, Y.; Strauss, D.; Altaye, M.; Calafat, A.M.; Khoury, J. Prenatal Exposure to Bisphenol A and Phthalates and Infant Neurobehavior. Neurotoxicol. Teratol. 2011, 33, 558–566. [Google Scholar] [CrossRef]
- Itoh, H.; Iwasaki, M.; Hanaoka, T.; Sasaki, H.; Tanaka, T.; Tsugane, S. Urinary Phthalate Monoesters and Endometriosis in Infertile Japanese Women. Sci. Total Env. 2009, 408, 37–42. [Google Scholar] [CrossRef]
- Silva, M.J.; Barr, D.B.; Reidy, J.A.; Malek, N.A.; Hodge, C.C.; Caudill, S.P.; Brock, J.W.; Needham, L.L.; Calafat, A.M. Urinary Levels of Seven Phthalate Metabolites in the U.S. Population from the National Health and Nutrition Examination Survey (NHANES) 1999–2000. Env. Health Perspect 2004, 112, 331–338. [Google Scholar] [CrossRef]
- Calafat, A.M.; Needham, L.L.; Silva, M.J.; Lambert, G. Exposure to Di-(2-Ethylhexyl) Phthalate among Premature Neonates in a Neonatal Intensive Care Unit. Pediatrics 2004, 113, e429–e434. [Google Scholar] [CrossRef]
- Weuve, J.; Sánchez, B.N.; Calafat, A.M.; Schettler, T.; Green, R.A.; Hu, H.; Hauser, R. Exposure to Phthalates in Neonatal Intensive Care Unit Infants: Urinary Concentrations of Monoesters and Oxidative Metabolites. Env. Health Perspect 2006, 114, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Ondusko, D.; Montrose, L.; Forbush, R.; Rozansky, D. Phthalate Exposures in the Neonatal Intensive Care Unit. Toxics 2021, 9, 90. [Google Scholar] [CrossRef] [PubMed]
- Vetrano, A.M.; Laskin, D.L.; Archer, F.; Syed, K.; Gray, J.P.; Laskin, J.D.; Nwebube, N.; Weinberger, B. Inflammatory Effects of Phthalates in Neonatal Neutrophils. Pediatr Res. 2010, 68, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.M.; Parastar, S.; Ebrahimpour, K.; Shoshtari-Yeganeh, B.; Hashemi, M.; Mansourian, M.; Kelishadi, R. Association of Urinary Phthalate Metabolites Concentrations with Body Mass Index and Waist Circumference. Env. Sci. Pollut. Res. Int. 2018, 25, 11143–11151. [Google Scholar] [CrossRef] [PubMed]
- Rattan, S.; Brehm, E.; Gao, L.; Flaws, J.A. Di(2-Ethylhexyl) Phthalate Exposure During Prenatal Development Causes Adverse Transgenerational Effects on Female Fertility in Mice. Toxicol. Sci. 2018, 163, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Bulgheroni, A.; Kinsner-Ovaskainen, A.; Hoffmann, S.; Hartung, T.; Prieto, P. Estimation of Acute Oral Toxicity Using the No Observed Adverse Effect Level (NOAEL) from the 28 Day Repeated Dose Toxicity Studies in Rats. Regul. Toxicol. Pharm. 2009, 53, 16–19. [Google Scholar] [CrossRef]


{kind=link}
| Hazard Quotient (HQ) | Neonates (kg) | Adults (kg) | |||||||||
| 1 | 2 | 3 | 4 | 5 | 50 | 60 | 70 | 80 | 90 | ||
| Sample 1 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| Sample 2 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| Sample 3 | 3.71 * | 1.85 * | 1.24 * | 0.926 | 0.741 | 0.371 | 0.309 | 0.265 | 0.232 | 0.206 | |
| Sample 4 | 0.832 | 0.416 | 0.277 | 0.208 | 0.166 | 0.0832 | 0.0693 | 0.0594 | 0.0520 | 0.0462 | |
| Sample 5 | 1.56 * | 0.780 | 0.520 | 0.390 | 0.312 | 0.156 | 0.130 | 0.111 | 0.0975 | 0.087 | |
| Sample 6 | 0.221 | 0.110 | 0.0740 | 0.0552 | 0.0442 | 0.0221 | 0.0184 | 0.0160 | 0.0138 | 0.0123 | |
| Sample 7 | 0.172 | 0.0860 | 0.0573 | 0.0429 | 0.0344 | 0.0172 | 0.0143 | 0.0123 | 0.0107 | 0.00954 | |
| Sample 8 | 0.510 | 0.255 | 0.170 | 0.128 | 0.102 | 0.0510 | 0.0425 | 0.0365 | 0.0319 | 0.0284 | |
| Sample 9 | 0.248 | 0.124 | 0.0825 | 0.0619 | 0.0495 | 0.0247 | 0.0206 | 0.0177 | 0.0155 | 0.0138 | |
| Sample 10 | 0.124 | 0.0619 | 0.0413 | 0.0310 | 0.0248 | 0.0124 | 0.0103 | 0.00885 | 0.00774 | 0.00688 | |
| UEmin (µg/L) | UEmax (µg/L) | ||
|---|---|---|---|
| Neonates (kg) | 1 | 86.6 | 273 |
| 2 | 21.6 | 68.2 | |
| 3 | 9.62 | 30.3 | |
| 4 | 5.41 | 17.1 | |
| 5 | 3.46 | 10.9 | |
| Adults (kg) | 50 | 0.173 | 0.546 |
| 60 | 0.120 | 0.379 | |
| 70 | 0.0883 | 0.278 | |
| 80 | 0.0676 | 0.213 | |
| 90 | 0.0534 | 0.168 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saab, Y.; Oueis, E.; Mehanna, S.; Nakad, Z.; Stephan, R.; Khnayzer, R.S. Risk Assessment of Phthalates and Their Metabolites in Hospitalized Patients: A Focus on Di- and Mono-(2-ethylhexyl) Phthalates Exposure from Intravenous Plastic Bags. Toxics 2022, 10, 357. https://doi.org/10.3390/toxics10070357
Saab Y, Oueis E, Mehanna S, Nakad Z, Stephan R, Khnayzer RS. Risk Assessment of Phthalates and Their Metabolites in Hospitalized Patients: A Focus on Di- and Mono-(2-ethylhexyl) Phthalates Exposure from Intravenous Plastic Bags. Toxics. 2022; 10(7):357. https://doi.org/10.3390/toxics10070357
Chicago/Turabian StyleSaab, Yolande, Emilia Oueis, Stephanie Mehanna, Zahi Nakad, Rita Stephan, and Rony S. Khnayzer. 2022. "Risk Assessment of Phthalates and Their Metabolites in Hospitalized Patients: A Focus on Di- and Mono-(2-ethylhexyl) Phthalates Exposure from Intravenous Plastic Bags" Toxics 10, no. 7: 357. https://doi.org/10.3390/toxics10070357
APA StyleSaab, Y., Oueis, E., Mehanna, S., Nakad, Z., Stephan, R., & Khnayzer, R. S. (2022). Risk Assessment of Phthalates and Their Metabolites in Hospitalized Patients: A Focus on Di- and Mono-(2-ethylhexyl) Phthalates Exposure from Intravenous Plastic Bags. Toxics, 10(7), 357. https://doi.org/10.3390/toxics10070357