
Human Biomonitoring Initiative (HBM4EU): Human Biomonitoring Guidance Values Derived for Dimethylformamide

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Methodology to Derive HBM-GVs in the Framework of the HBM4EU Project
- Selection of the relevant biomarker(s): a biomarker is defined as any substance, structure, or process that can be measured in the body or its degradation product(s) which influences or predicts the incidence of outcome or disease. Biomarkers can be classified into biomarkers of exposure (BME), biomarkers of effects, or biomarkers of susceptibility [2]. This first step consists of the data collection on the substance and its metabolites (i.e., toxicokinetic and toxicodynamic data). Based on these data, biomarkers of exposure and/or effect are identified and then chosen according to defined criteria: specificity, sensitivity, half-life, sampling conditions, invasiveness, background level, and analytical methods [15].
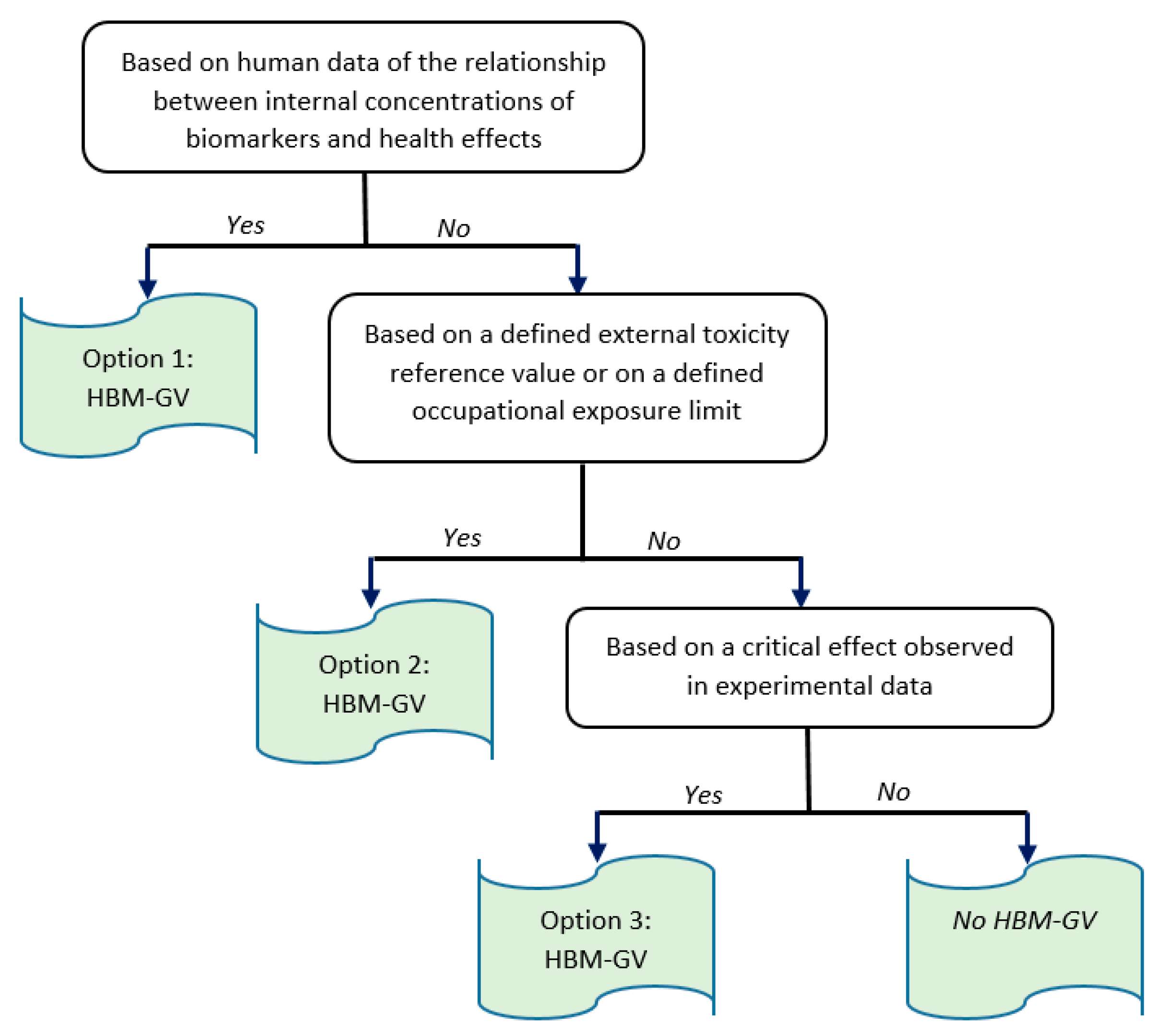
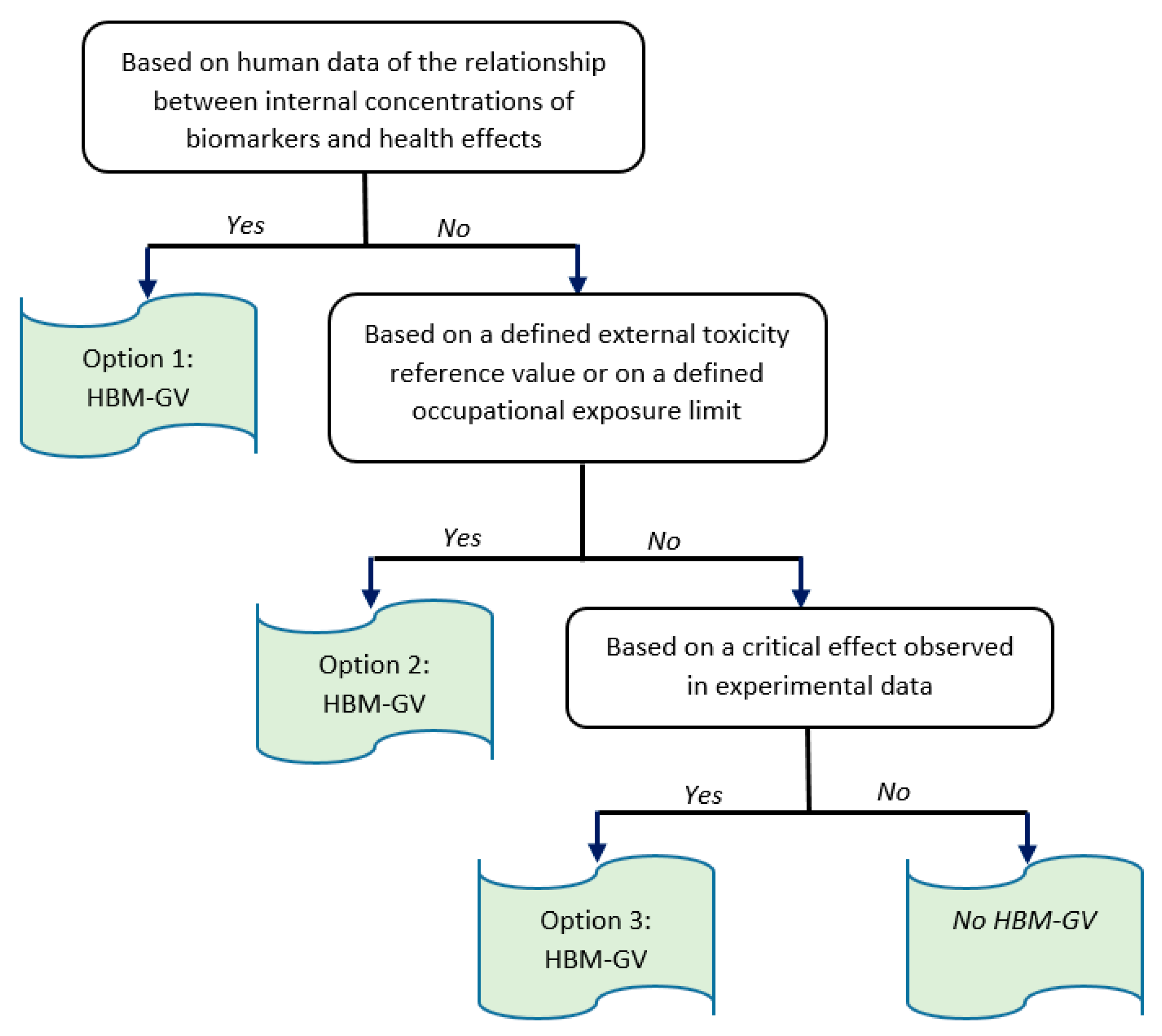
- The derivation of HBM-GVs for the selected biomarkers can then be conducted through three possible options (decision tree described in Figure 1). When the corresponding data are available, the preferred option is to base HBM-GV(s) identification on the relationship between internal concentrations of the selected biomarker(s) and the occurrence of adverse effects. The second possible option is to derive HBM-GVs from external limit values (i.e., Occupational Exposure Levels [OEL] or Toxicity Reference Values [TRV]) proposed by relevant European or non-European bodies. The last option consists of the derivation of HBM-GVs on the basis of critical effects observed in animal toxicological studies. These options are described in more detail in Apel et al. (2020) [2].
- Choice of the critical effect which is considered to be the most sensitive among all adverse effects that may arise from exposure to the substance (e.g., changes in morphology, physiology, growth, development, reproduction, or life span resulting in an impairment of functional capacity, an impairment of the capacity to offset additional stress, or an increase in sensitivity).
- Selection of the key study and identification of a point of departure (POD) with the most informative studies, i.e., well-conducted human studies adequately reporting measured internal concentration levels of a substance, sampling times, analytical methods used, and the relationships between concentrations of a substance or its metabolites in human biological media and the occurrence of adverse effects. If relevant and qualitatively acceptable human studies are available, a key human study together with a Point of Departure (POD) is selected.
- Application of assessment factors (AFs), when necessary, to obtain the HBM-GVs. These can be divided into an AFH for the intraspecies variability or possible other AFs to compensate for the potential remaining uncertainties in the derived HBM-GV, especially regarding the possible deficiencies or data gaps in the available data sets [2].
2.2. Methodology Used for Deriving HBM-GVWorker for DMF
- the reports by the American Conference of Governmental Industrial Hygienists (ACGIH) [16,17], the German Research Foundation or Deutsche Forschungsgemeinschaft (DFG) [18,19], the European Chemicals Agency (ECHA) [7], the International Agency for Research on Cancer (IARC) ([10]), and the Scientific committee for occupational exposure limits (SCOEL) [20];
- for more recent and specific publications, a bibliographical research, which was conducted in Medline and Scopus until 2021 with the following keywords: Dimethylformamide, DMF, guidance value, toxicity reference value (TRV), biomarker of exposure, biomonitoring, toxicokinetic, health effects, liver, carcinogenicity, and reprotoxic effects.
3. Results
3.1. Identification of Possible Biomarkers of Exposure
- -
- Unchanged DMF in urine;
- -
- total NMF or tNMF (which is the sum of HMMF and NMF) in urine;
- -
- AMCC in urine;
- -
- MCVal in blood; and
- -
- formamide in urine.
3.2. Identification and Characterization of the Dangers Associated with DMF Exposure

{kind=link}
{kind=link}
| Reference | Subjects | Exposure DMF in the Air (DMFa) Metabolites * | Results/Observations | |
|---|---|---|---|---|
| Lyle et al., 1979 [52] England | Workers (DMF used as solvent) N = 102) 3-year follow-up | DMFa Range: <10 to 200 ppm (30–600 mg·m−3) tNMF (tNMFu) Range: <10 to 77 µL/L (probable error in the unit) | Alcohol intolerance reactions Facial flushing and other symptoms in 19 workers 26 of the 34 episodes occurred after the workers had consumed alcoholic drinks Liver function not investigated | |
| Yonemoto and Suzuki, 1980 [53] Japan | Workers (synthetic leather factory) N = 11 (biomonitoring data for 9 of them) | DMFa Range: 0–5 ppm (0–15 mg·m−3) (TWA) Post-Shift (PS) tNMFu Range: 0.4–19.56 mg·d−1 | No effect on serum biochemistry (liver enzymes) Alcohol intolerance: 6/11 workers said to be less tolerant than before | |
| Lauwerys et al., 1980 [27] Belgium | Workers in an acrylic fiber factory N = 22 (+28 controls) | DMFa Mean: 13 (1.3–46.6) mg·m−3 (4.5 (0.4–15.3) ppm) Stationary sampling tNMFu <40–50 mg·g−1 cr (PS) | No effects on serum biochemistry (liver enzymes not elevated) Signs of alcohol intolerance in some workers | |
| Catenacci et al., 1984 [54] Italy Quoted by SCOEL (2006) [20] | N = 54 (employed > 5 y) acrylic fiber plant 2 groups exposed and 54 controls) | Group 1 (N = 28) DMFa Mean (range): 6 (4–8) ppm (18 (12–24) mg·m−3) tNMFu 22.3 mg·L−1 | Group 2 (N = 26) DMFa Mean (range): 1 (0.6–1.6) ppm (3 (1.8–4.8) mg·m−3) tNMFu: 7 mg·L−1 | No significant effects on liver enzymes in the 2 groups |
| Sakai et al., 1995 [55] Japan | Workers (N = 10) Polyurethane production 2.5-year follow-up | DMFa Geometric mean (GM): 2.5–10.4 ppm (7.5–31.2 mg·m−3) PS tNMFu Mean: 24.7 mg·g−1 cr AMCCu Mean: 22.0 mg·g−1 cr | No effects on liver enzymes | |
| Fiorito et al., 1997 [50] Italy | N = 75 (employed) synthetic leather production and 75 controls (unexposed workers) | DMFa Group 1 (Washing) N = 10 GM: 21.5 mg·m−3 (7.2 ppm) Range: 5–40 mg·m−3 Group 2 (Production) N = 12 GM: 18.7 mg·m−3 (6.2 ppm) Range: 5–40 mg·m−3 tNMFu (N = 22): GM: 13.6 mg·L−1 or 13.4 mg·g−1 cr PS | Elevation of liver enzymes (12/75) [p < 0.01] Alcohol intolerance in 50% of exposed workers and facial flushing (38%), palpitations (30%), headache (22%), body flushing (15%), and tremors (14%) Gastrointestinal symptoms (stomach pain, nausea, loss of appetite) in 50% of exposed workers | |
| Wrbitzky and Angerer, (1998) [47]; Wrbitzky, (1999) [48] Germany | Polyacrylic fiber production N = 126 (total of exposed workers) | DMFa Mean (SD): 4.1 ± 7.4 (<0.1–37.9) ppm (12.3 ± 22.2 mg·m−3) tNMFu Mean (SD): 14.9 ± 18.7 (0.9–100) mg·L−1 9.1 ± 11.4 (0.5–62.3) mg·g−1 cr | Effects on liver enzymes Synergetic effect of alcohol consumption on liver enzymes activity | |
| Finishing N = 55 | DMFa Mean (SD): 14.2 ± 2.2 (>0.1–13.7) ppm (42.6 ± 6.6 mg·m−3) tNMFu Mean (SD): 4.5 ± 4.3 mg·g−1 cr | Effects on liver enzymes in alcohol consumers | ||
| Dyeing N = 12 | DMFa Mean (SD): 2.5 ± 3.1 (0.1–9.8) ppm (7.5 ± 9.3 mg·m−3) tNMFu Mean (SD): 6.7 ± 5.4 (0.8–17.2) mg·g−1 cr | No effects on liver enzymes in workers not drinking alcohol Reduced alcohol consumption in workers drinking alcohol | ||
| Dry spinning N = 28 | DMFa Mean (SD): 6.4–9.6 (0.8–36.9) ppm (19.2 ± 28.8 mg·m−3) tNMFu Mean (SD): 11.6 ± 13.1 (0.9–62.3 mg·g−1 cr) | |||
| Wet spinning N = 30 | DMFa Mean (SD): 7.3 ± 10.2 (0.3–37.9) ppm (21.9 ± 30.6 mg·m−3) tNMFu Mean (SD): 16.0 ± 15.9 (0.4–54.0) mg·g−1 cr | |||
| He et al., 2010 [45] China | Synthetic leather and other resins production N = 79 (58 men and 21 women) | Group 1 (N = 33): Low exposure DMFa Min-Max: Not detected- <4.55 mg·m−3 (1.6 ppm) DMFu GM: 0.26 mg·g−1 creatinine tNMFu GM: 1.80 mg·g−1 creatinine AMCCu GM: 4.25 mg·g−1 creatinine Group 2 (N = 24): Medium exposure DMFa (Mean): 9 mg·m−3 (3 ppm) DMFu (GM): 0.53 mg·g−1 creatinine tNMFu (GM): 9.6 mg·g−1 creatinine AMCCu (GM): 25.4 mg·g−1 creatinine Group 3 (N = 22): High exposure DMFa (Mean): 36 mg·m−3 (12 ppm) DMFu (GM): 1.78 mg·g−1 creatinine tNMFu (GM): 26.5 mg·g−1 creatinine AMCCu (GM): 45.5 mg·g−1 creatinine | About 60% of subjects with urine AMCC concentration above 40 mg·g−1 cr had raised liver enzyme activities Statistically more workers with raised liver enzymes in group 3 (high exposure group) than in group 1 (administrative staff of the factory); p < 0.05 | |
| Kilo et al., 2016 [51] Germany | Synthetic fiber production N = 220 workers and 175 Controls | Mean ± SD DMFa: 6.2 ± 7.6 mg·m−3; 2.1 ± 2.5 ppm tNMFu: 7.75 (±8.82) mg·L−1 AMCCu: 9.42 (±10.42) mg·g−1 cr McVal: 83.3 (±83.1) nmol·g−1 globin | None of the tested liver enzyme activities showed a positive association with any of the three exposure markers Alcohol intolerance reactions (not influencing alcohol consumption behavior) | |
| Wu et al., 2017 [46] China | Synthetic leather production N = 698 And 188 controls | 3 exposure groups: Median (range) Low exposure group tNMFu (N = 228): 0.0025 mg·L−1 (ND-0.11) AMCCu (N = 227): 2.18 mg·L−1 (ND-16,95) MCVal (N = 232): 15.19 nmol·mol−1 globin (ND-29.37) Moderate exposure groups tNMFu (N = 227): 1.78 mg·L−1 (0.11–3.88) AMCCu (N = 228): 44.9 mg·L−1 (16.95–86.62) MCVal (N = 234): 46.00 (29.37–63.95) nmol·mol−1 globin High exposure groups tNMFu (N = 227): 9.59 mg·L−1 (>3.88) AMCCu (N = 227): 148.01 mg·L−1 (>86.62) MCVal (N = 232): 87.01 (63.95–) nmol/mol globin | Liver injury assessed by measurement of liver enzyme levels and compared to reference value ranges (AST and ALT: 0–45, γGT: 8–58U/L) Statistically more workers with raised liver enzymes only in high-exposure group for tNMF, in both moderate- and high-exposure groups for AMCCu and MCVal (p < 0.05) | |
3.3. Choice of the Critical Effect
3.4. Choice of Relevant Biomarkers
3.4.1. Unchanged DMF in Urine
3.4.2. Total NMF in Urine
3.4.3. AMCC in Urine
3.4.4. MCVal Adducts to Globin in Blood
3.4.5. Formamide in Urine
3.4.6. Conclusion on BME Selection
3.4.7. Analytical Methods
3.5. Published Limit Values for Urine tNMF and AMCC in Occupational Setting
3.6. Choice of Key Studies and Identification of a POD for tNMF in Urine
- -
- Lauwerys et al. (1980) [27] observed no effect on liver enzymes up to 40–50 mg·g−1 creatinine (cr) tNMF in urine of 22 workers exposed to DMF during five consecutive days. The authors underlined that in the factory, the selection criteria (not disclosed) at the beginning of employment were rather severe and could have led to recruitment bias so that the results obtained may not reflect responses in any worker [16];
- -
- The two publications by Wrbitzky and Angerer (1998) and Wrbitzky (1999) reporting on the same study conducted in a cohort of 126 workers showed that liver damage was significantly more frequent in the exposed group than in controls. Mean tNMF concentration in the exposed group was 9.1 mg·g−1 creatinine (14.9 mg·L−1). However, considering the working areas, it was observed that liver damage was unexpectedly associated with the lowest exposure group (mean urine tNMF: 4.5 mg·g−1 creatinine) and could be explained by a higher alcohol consumption. In the other three areas, no excess of liver damage was observed for mean urine tNMF concentrations of 6.7, 11.6, and 16 mg·g−1 creatinine [47,48].
- -
- In a recent European study by Kilo et al. (2017), no excess risk of liver damage was observed in a cohort of 220 workers exposed to DMF with a mean concentration of 7.75 mg·L−1 tNMF in urine, compared with 175 controls [51].
- -
- The other three studies were conducted in Asian people:
- -
- Sakai et al. (1995) reported no effects on liver enzymes of DMF exposure in 10 workers during à 2.5-year-follow-up. The mean tNMF concentration in the urine of these workers was 24.47 mg·g−1·cr [55];
- -
- He et al. (2010) also reported that, when their cohort of 79 workers was divided into three groups, a significantly elevated risk of liver damage (liver enzyme elevation) according to DMF exposure was observed only in the group with the highest exposure (mean tNMF concentration: 26.5 mg·g−1·cr) [45]; and
- -
- Wu et al. (2017) measured liver enzyme activity in a cohort of 698 workers exposed to DMF and in 188 controls. They also measured tNMF urine concentration in exposed workers. A significantly elevated risk of liver damage was observed only for the third tertile of tNMF distribution (median tNMF concentration: 9.59 mg·L−1). The lower limit for the benchmark dose with a benchmark response of 10% above the adverse response rate of liver injury seen in the control group (BMDL10) was 14 mg·L−1 (tNMF) [46].
3.7. Choice of the Key Study and POD for AMCC in Urine
- -
- In the German study by Kilo et al. (2016), no effects on liver enzymes were observed in a cohort of 220 workers with a mean AMCC urine concentration of 9.42 mg·g−1 cr when they were compared to 175 controls; however, the range of the measured AMCC urine concentrations was very large (standard deviation: 10.42 mg·g−1 cr) [51];
- -
- in the Japanese study by Sakaï et al. (1995), no effects on liver enzymes were observed in 10 workers exposed to DMF during à 2.5-year follow-up. The mean AMCC concentration in the urine of these workers was 22 mg·g−1·cr [55];
- -
- in the study from China, He et al. (2010) also reported that, when their cohort of 79 workers was divided into three groups, a significantly elevated risk of liver damage (liver enzyme elevation) according to DMF exposure was observed only in the group with the highest exposure (mean AMCC concentration in urine: 45.5 mg·g−1 cr). Geometric mean values for the concentration of AMCC in urine of workers from the low and medium exposure groups were 4.25 mg·g−1·cr and 25.4 mg·g−1·cr, respectively [45];
- -
- a second Chinese study by Wu et al. (2017) measured liver enzyme activity in a cohort of 698 workers exposed to DMF and in 188 controls. They also measured AMCC urine concentration in exposed workers. A significantly elevated risk of liver damage was observed only for the second and the third tertiles of the AMCC distribution (median AMCC concentrations: 44.09 mg·L−1 and 148.01 mg·L−1, respectively). The median and maximal AMCC concentrations in the low exposure group (1st tertile), with no detectable liver damage excess, were 2.18 mg·L−1 and 16.95 mg·L−1, respectively. The lower limit for the benchmark dose with a benchmark response of 10% above the adverse response rate of liver injury seen in the control group (BMDL10) was 155 mg·L−1 (AMCC) [46].
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ganzleben, C.; Antignac, J.-P.; Barouki, R.; Castaño, A.; Fiddicke, U.; Klánová, J.; Lebret, E.; Olea, N.; Sarigiannis, D.; Schoeters, G.R.; et al. Human Biomonitoring as a Tool to Support Chemicals Regulation in the European Union. Int. J. Hyg. Environ. Health 2017, 220, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Apel, P.; Rousselle, C.; Lange, R.; Sissoko, F.; Kolossa-Gehring, M.; Ougier, E. Human Biomonitoring Initiative (HBM4EU)—Strategy to Derive Human Biomonitoring Guidance Values (HBM-GVs) for Health Risk Assessment. Int. J. Hyg. Environ. Health 2020, 230, 113622. [Google Scholar] [CrossRef] [PubMed]
- Lamkarkach, F.; Ougier, E.; Garnier, R.; Viau, C.; Kolossa-Gehring, M.; Lange, R.; Apel, P. Human Biomonitoring Initiative (HBM4EU): Human Biomonitoring Guidance Values (HBM-GVs) Derived for Cadmium and Its Compounds. Environ. Int. 2021, 147, 106337. [Google Scholar] [CrossRef] [PubMed]
- Ougier, E.; Zeman, F.; Antignac, J.-P.; Rousselle, C.; Lange, R.; Kolossa-Gehring, M.; Apel, P. Human Biomonitoring Initiative (HBM4EU): Human Biomonitoring Guidance Values (HBM-GVs) Derived for Bisphenol A. Environ. Int. 2021, 154, 106563. [Google Scholar] [CrossRef]
- Lange, R.; Apel, P.; Rousselle, C.; Charles, S.; Sissoko, F.; Kolossa-Gehring, M.; Ougier, E. The European Human Biomonitoring Initiative (HBM4EU): Human Biomonitoring Guidance Values for Selected Phthalates and a Substitute Plasticizer. Int. J. Hyg. Environ. Health 2021, 234, 113722. [Google Scholar] [CrossRef]
- David, M.; Gerofke, A.; Lange, R.; Kolossa-Gehring, M.; Apel, P. The European Human Biomonitoring Initiative (HBM4EU): Human Biomonitoring Guidance Values (HBM-GVs) for the Aprotic Solvents N-Methyl-2-Pyrrolidone (NMP) and N-Ethyl-2-Pyrrolidone (NEP). Int. J. Hyg. Environ. Health 2021, 238, 113856. [Google Scholar] [CrossRef]
- European Chemical Agency (ECHA). Opinion of the Committee for Risk Assessment and Opinion of the Committee for Socio-Economic Analysis on an Annex XV Dossier Proposing Restrictions of the Manufacture, Placing on the Market or Use of a Substance within the EU; European Chemical Agency (ECHA): Helsinki, Finland, 2019.
- European Chemical Agency (ECHA). Background Document for N,N-Dimethylformamide (DMF); Document Developed in the Context of ECHA’s Fifth Recommendation for the Inclusion of Substances in Annex XIV; European Chemical Agency (ECHA): Helsinki, Finland, 2014.
- International Agency for Research on Cancer (IARC). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; World Health Organization: Lyon, France, 1999; Volume 71, Part Two. [Google Scholar]
- International Agency for Research on Cancer (IARC). Some Chemicals. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; World Health Organization: Lyon, France, 2018; Volume 115. [Google Scholar]
- Kommission HBM des Umweltbundesamtes. Grundsatzpapier Zur Ableitung von HBM-Werten. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz. 2014, pp. 138–147. Available online: https://www.umweltbundesamt.de/sites/default/files/medien/377/dokumente/art_10.1007_s00103-013-1867-2-2.pdf (accessed on 20 April 2022).
- Apel, P.; Angerer, J.; Wilhelm, M.; Kolossa-Gehring, M. New HBM Values for Emerging Substances, Inventory of Reference and HBM Values in Force, and Working Principles of the German Human Biomonitoring Commission. Int. J. Hyg. Environ. Health 2017, 220, 152–166. [Google Scholar] [CrossRef] [Green Version]
- Hays, S.M.; Becker, R.A.; Leung, H.W.; Aylward, L.L.; Pyatt, D.W. Biomonitoring Equivalents: A Screening Approach for Interpreting Biomonitoring Results from a Public Health Risk Perspective. Regul. Toxicol. Pharmacol. 2007, 47, 96–109. [Google Scholar] [CrossRef]
- Hays, S.M.; Aylward, L.L.; LaKind, J.S.; Bartels, M.J.; Barton, H.A.; Boogaard, P.J.; Brunk, C.; DiZio, S.; Dourson, M.; Goldstein, D.A.; et al. Guidelines for the Derivation of Biomonitoring Equivalents: Report from the Biomonitoring Equivalents Expert Workshop. Regul. Toxicol. Pharmacol. 2008, 51, S4–S15. [Google Scholar] [CrossRef]
- ANSES. Document de Référence Pour l’élaboration de Valeurs Limites d’exposition à Des Agents Chimiques En Milieu Professionnel; Agence Nationale de Sécurité Sanitaire Pour l’Alimentation, l’Environnement et Le Travail: Paris, France, 2017; 142p. [Google Scholar]
- American Conference of Governmental Industrial Hygienists (ACGIH). Biological Exposure Index Documentation for N,N-Dimethylformamide; American Conference of Governmental Industrial Hygienists: Washington, DC, USA, 2017. [Google Scholar]
- American Conference of Governmental Industrial Hygienists (ACGIH). N,N-Dimethylformamide; American Conference of Governmental Industrial Hygienists: Washington, DC, USA, 2018. [Google Scholar]
- Käfferlein, H.U. Addendum Zu N,N-Dimethylformamid. In Biologische Arbeitsstoff-Toleranz-Werte (BAT-Werte) und Expositionsäquivalente für Krebs-Erzeugende Arbeitsstoffe (EKA) und Biologische Leitwerte (BLW); Drexler, H., Greim, H., Eds.; DFG MAK Commission: Germany, 2006. [Google Scholar]
- Göen, T.; Drexler, H.; Hartwig, A. Addendum to N,N-Dimethylformamide [N,N-Dimethylformamid, Addendum] BAT Value Documentation in German; DFG MAK Commission: Germany, 2019. [Google Scholar]
- SCOEL/SUM/121; Recommendation from the Scientific Committee for Occupational Exposure Limits on N,N-Dimethylformamide. The Scientific Committee on Occupational Exposure Limits (SCOEL), 2006.
- Brugnone, F.; Perbellini, L.; Gaffuri, E.; Apostoli, P. Biomonitoring of Industrial Solvent Exposures in Workers’ Alveolar Air. Int. Arch. Occup. Environ. Health 1980, 47, 245–261. [Google Scholar] [CrossRef]
- Mráz, J.; Nohová, H. Absorption, Metabolism and Elimination of N,N-Dimethylformamide in Humans. Int. Arch. Occup. Environ. Health 1992, 64, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Maxfield, M.E.; Barnes, J.R.; Azar, A.; Trochimowicz, H.T. Urinary Excretion of Metabolite Following Experimental Human Exposures to DMF or to DMAC. J. Occup. Med. 1975, 17, 506–511. [Google Scholar] [PubMed]
- Mráz, J.; Nohová, H. Percutaneous Absorption of N,N-Dimethylformamide in Humans. Int. Arch. Occup. Environ. Health 1992, 64, 79–83. [Google Scholar] [CrossRef]
- Tsuda, Y.; Miyauchi, H.; Minozoe, A.; Tanaka, S.; Arito, H.; Tsukahara, T.; Nomiyama, T. Seasonal Difference in Percutaneous Absorption of N,N-Dimethylformamide as Determined Using Two Urinary Metabolites. J. Occup. Health 2014, 56, 252–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nomiyama, T.; Nakashima, H.; Chen, L.L.; Tanaka, S.; Miyauchi, H.; Yamauchi, T.; Sakurai, H.; Omae, K. N,N-Dimethylformamide: Significance of Dermal Absorption and Adjustment Method for Urinary N-Methylformamide Concentration as a Biological Exposure Item. Int. Arch. Occup. Environ. Health 2001, 74, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Lauwerys, R.R.; Kivits, A.; Lhoir, M.; Rigolet, P.; Houbeau, D.; Buchet, J.P.; Roels, H.A. Biological Surveillance of Workers Exposed to Dimethylformamide and the Influence of Skin Protection on Its Percutaneous Absorption. Int. Arch. Occup. Environ. Health 1980, 45, 189–203. [Google Scholar] [CrossRef]
- World Health Organization. N,N-Dimethylformamide; World Health Organization (WHO): Geneva, Switzerland, 2001. [Google Scholar]
- Saillenfait, A.M.; Payan, J.P.; Beydon, D.; Fabry, J.P.; Langonne, I.; Sabate, J.P.; Gallissot, F. Assessment of the Developmental Toxicity, Metabolism, and Placental Transfer of N,N-Dimethylformamide Administered to Pregnant Rats. Fundam. Appl. Toxicol. 1997, 39, 33–43. [Google Scholar] [CrossRef]
- Mráz, J.; Jheeta, P.; Gescher, A.; Hyland, R.; Thummel, K.; Threadgill, M.D. Investigation of the Mechanistic Basis of N,N-Dimethylformamide Toxicity. Metabolism of N,N-Dimethylformamide and Its Deuterated Isotopomers by Cytochrome P450 2E1. Chem. Res. Toxicol. 1993, 6, 197–207. [Google Scholar] [CrossRef]
- Scailteur, V.; de Hoffmann, E.; Buchet, J.P.; Lauwerys, R. Study on in Vivo and in Vitro Metabolism of Dimethylformamide in Male and Female Rats. Toxicology 1984, 29, 221–234. [Google Scholar] [CrossRef]
- Kawai, T.; Yasugi, T.; Mizunuma, K.; Watanabe, T.; Cai, S.X.; Huang, M.Y.; Xi, L.Q.; Qu, J.B.; Yao, B.Z.; Ikeda, M. Occupational Dimethylformamide Exposure. 2. Monomethylformamide Excretion in Urine after Occupational Dimethylformamide Exposure. Int. Arch. Occup. Environ. Health 1992, 63, 455–460. [Google Scholar] [CrossRef]
- Mráz, J.; Turecek, F. Identification of N-Acetyl-S-(N-Methylcarbamoyl)Cysteine, a Human Metabolite of N,N-Dimethylformamide and N-Methylformamide. J. Chromatogr. 1987, 414, 399–404. [Google Scholar] [CrossRef]
- Mráz, J.; Cross, H.; Gescher, A.; Threadgill, M.D.; Flek, J. Differences between Rodents and Humans in the Metabolic Toxification of N,N-Dimethylformamide. Toxicol. Appl. Pharmacol. 1989, 98, 507–516. [Google Scholar] [CrossRef]
- Käfferlein, H.U.; Angerer, J. N-Methylcarbamoylated Valine of Hemoglobin in Humans after Exposure to N,N-Dimethylformamide: Evidence for the Formation of Methyl Isocyanate? Chem. Res. Toxicol. 2001, 14, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Angerer, J.; Göen, T.; Krämer, A.; Käfferlein, H.U. N-Methylcarbamoyl Adducts at the N-Terminal Valine of Globin in Workers Exposed to N,N-Dimethylformamide. Arch. Toxicol. 1998, 72, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Mráz, J.; Cimlová, J.; Stránský, V.; Nohová, H.; Kicová, R.; Simek, P. N-Methylcarbamoyl-Lysine Adduct in Globin: A New Metabolic Product and Potential Biomarker of N, N-Dimethylformamide in Humans. Toxicol. Lett. 2006, 162, 211–218. [Google Scholar] [CrossRef]
- Hundley, S.G.; Lieder, P.H.; Valentine, R.; Malley, L.A.; Kennedy, G.L. Dimethylformamide Pharmacokinetics Following Inhalation Exposures to Rats and Mice. Drug Chem. Toxicol. 1993, 16, 21–52. [Google Scholar] [CrossRef]
- Hundley, S.G.; McCooey, K.T.; Lieder, P.H.; Hurtt, M.E.; Kennedy, G.L. Dimethylformamide Pharmacokinetics Following Inhalation Exposure in Monkeys. Drug Chem. Toxicol. 1993, 16, 53–79. [Google Scholar] [CrossRef]
- Henschler, D. Occupational Toxicants: Critical Data Evaluation for MAK Values and Classification of Carcinogens; Greim, H., Ed.; Wiley-VCH: Weinheim, Germany, 1998; Volume 8. [Google Scholar]
- Eben, A.; Kimmerle, G. Metabolism Studies of N, N-Dimethylformamide. III. Studies about the Influence of Ethanol in Persons and Laboratory Animals. Int. Arch. Occup. Environ. Health 1976, 34, 109–126. [Google Scholar] [CrossRef]
- Kim, K.-W.; Chung, Y.H. Hepatotoxicity in Rats Treated with Dimethylformamide or Toluene or Both. Toxicol. Res. 2013, 29, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Garnier, R.; Chataigner, D.; Perez-Trigalou, B.; Efthymiou, M.L. Intoxications professionnelles par le diméthylformamide. Arch. Mal. Prof. 1992, 53, 111–120. [Google Scholar]
- Li, M.-J.; Zeng, T. The Deleterious Effects of N,N-Dimethylformamide on Liver: A Mini-Review. Chem. Biol. Interact. 2019, 298, 129–136. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Wang, P.; Zhu, J.; Wu, G.; Ji, J.; Xue, Y. Role of Urinary Biomarkers of N,N-Dimethylformamide in the Early Detection of Hepatic Injury among Occupational Exposed Workers. Int. Arch. Occup. Environ. Health 2010, 83, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Liu, Q.; Wang, C.; Xu, B.; Guan, M.; Ye, M.; Jiang, H.; Zheng, M.; Zhang, M.; Zhao, W.; et al. A Comparative Benchmark Dose Study for N, N-Dimethylformamide Induced Liver Injury in a Chinese Occupational Cohort. Toxicol. Sci. 2017, 158, 140–150. [Google Scholar] [CrossRef] [Green Version]
- Wrbitzky, R.; Angerer, J. N,N-Dimethylformamide--Influence of Working Conditions and Skin Penetration on the Internal Exposure of Workers in Synthetic Textile Production. Int. Arch. Occup. Environ. Health 1998, 71, 309–316. [Google Scholar] [CrossRef]
- Wrbitzky, R. Liver Function in Workers Exposed to N,N-Dimethylformamide during the Production of Synthetic Textiles. Int. Arch. Occup. Environ. Health 1999, 72, 19–25. [Google Scholar] [CrossRef]
- Cai, S.X.; Huang, M.Y.; Xi, L.Q.; Li, Y.L.; Qu, J.B.; Kawai, T.; Yasugi, T.; Mizunuma, K.; Watanabe, T.; Ikeda, M. Occupational Dimethylformamide Exposure. 3. Health Effects of Dimethylformamide after Occupational Exposure at Low Concentrations. Int. Arch. Occup. Environ. Health 1992, 63, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Fiorito, A.; Larese, F.; Molinari, S.; Zanin, T. Liver Function Alterations in Synthetic Leather Workers Exposed to Dimethylformamide. Am. J. Ind. Med. 1997, 32, 255–260. [Google Scholar] [CrossRef]
- Kilo, S.; Göen, T.; Drexler, H. Cross-Sectional Study on N,N-Dimethylformamide (DMF); Effects on Liver and Alcohol Intolerance. Int. Arch. Occup. Environ. Health 2016, 89, 1309–1320. [Google Scholar] [CrossRef]
- Lyle, W.H.; Spence, T.W.; McKinneley, W.M.; Duckers, K. Dimethylformamide and Alcohol Intolerance. Br. J. Ind. Med. 1979, 36, 63–66. [Google Scholar] [CrossRef] [Green Version]
- Yonemoto, J.; Suzuki, S. Relation of Exposure to Dimethylformamide Vapor and the Metabolite, Methylformamide, in Urine of Workers. Int. Arch. Occup. Environ. Health 1980, 46, 159–165. [Google Scholar] [CrossRef]
- Catenacci, G.; Grampella, D.; Terzi, R.; Sala, A.; Pollini, G. Hepatic Function in Subjects Exposed to Environmental Concentrations of DMF Lower than the Actually Proposed TLV. G. Ital. Med. Lav. 1984, 6, 157–158. [Google Scholar] [PubMed]
- Sakai, T.; Kageyama, H.; Araki, T.; Yosida, T.; Kuribayashi, T.; Masuyama, Y. Biological Monitoring of Workers Exposed to N,N-Dimethylformamide by Determination of the Urinary Metabolites, N-Methylformamide and N-Acetyl-S-(N-Methylcarbamoyl) Cysteine. Int. Arch. Occup. Environ. Health 1995, 67, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Hanasono, G.K.; Fuller, R.W.; Broddle, W.D.; Gibson, W.R. Studies on the Effects on N,N’-Dimethylformamide on Ethanol Disposition and on Monoamine Oxidase Activity in Rats. Toxicol. Appl. Pharmacol. 1977, 39, 461–472. [Google Scholar] [CrossRef]
- Wolff, P.H. Ethnic Differences in Alcohol Sensitivity. Science 1972, 175, 449–450. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W. Racial Differences in Alcohol Sensitivity. Alcohol Alcohol. 1986, 21, 93–104. [Google Scholar]
- Hennebrüder, K.; Angerer, J. Determination of DMF Modified DNA Base N4-Methylcarbamoylcytosine in Human Urine Using off-Line Sample Clean-up, Two-Dimensional LC and ESI-MS/MS Detection. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2005, 822, 124–132. [Google Scholar] [CrossRef]
- Chen, Y. Induction of DNA strand breakage of human peripheral blood cells by N,N-dimethylformamide. Chin. J. Health Lab. Technol. 2014, 14, 166–168. [Google Scholar]
- Shieh, D.-B.; Chen, C.-C.; Shih, T.-S.; Tai, H.-M.; Wei, Y.-H.; Chang, H.-Y. Mitochondrial DNA Alterations in Blood of the Humans Exposed to N,N-Dimethylformamide. Chem. Biol. Interact. 2007, 165, 211–219. [Google Scholar] [CrossRef]
- Major, J.; Hudák, A.; Kiss, G.; Jakab, M.G.; Szaniszló, J.; Náray, M.; Nagy, I.; Tompa, A. Follow-up Biological and Genotoxicological Monitoring of Acrylonitrile- and Dimethylformamide-Exposed Viscose Rayon Plant Workers. Environ. Mol. Mutagenesis 1998, 31, 301–310. [Google Scholar] [CrossRef]
- Cheng, T.J.; Hwang, S.J.; Kuo, H.W.; Luo, J.C.; Chang, M.J. Exposure to Epichlorohydrin and Dimethylformamide, Glutathione S-Transferases and Sister Chromatid Exchange Frequencies in Peripheral Lymphocytes. Arch. Toxicol. 1999, 73, 282–287. [Google Scholar] [CrossRef]
- McQueen, C.A.; Way, B.M.; Williams, G.M. Genotoxicity of Carcinogens in Human Hepatocytes: Application in Hazard Assessment. Toxicol. Appl. Pharmacol. 1988, 96, 360–366. [Google Scholar] [CrossRef]
- Antoine, J.L.; Arany, J.; Léonard, A.; Henrotte, J.; Jenar-Dubuisson, G.; Decat, G. Lack of Mutagenic Activity of Dimethylformamide. Toxicology 1983, 26, 207–212. [Google Scholar] [CrossRef]
- Koudela, K.; Spazier, K. Results of Cytogenetic Examination of Persons Working in an Environment of Increased Concentration of Dimethylformamide Vapors in the Atmosphere. Prac. Lèk. 1981, 33, 121–123. [Google Scholar]
- Senoh, H.; Aiso, S.; Arito, H.; Nishizawa, T.; Nagano, K.; Yamamoto, S.; Matsushima, T. Carcinogenicity and Chronic Toxicity after Inhalation Exposure of Rats and Mice to N,N-Dimethylformamide. J. Occup. Health 2004, 46, 429–439. [Google Scholar] [CrossRef] [Green Version]
- Malley, L.A.; Slone, T.W.; Van Pelt, C.; Elliott, G.S.; Ross, P.E.; Stadler, J.C.; Kennedy, G.L. Chronic Toxicity/Oncogenicity of Dimethylformamide in Rats and Mice Following Inhalation Exposure. Fundam. Appl. Toxicol. 1994, 23, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Ohbayashi, H.; Umeda, Y.; Senoh, H.; Kasai, T.; Kano, H.; Nagano, K.; Arito, H.; Fukushima, S. Enhanced Hepatocarcinogenicity by Combined Inhalation and Oral Exposures to N,N-Dimethylformamide in Male Rats. J. Toxicol. Sci. 2009, 34, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Ducatman, A.M.; Conwill, D.E.; Crawl, J. Germ Cell Tumors of the Testicle among Aircraft Repairmen. J. Urol 1986, 136, 834–836. [Google Scholar] [CrossRef]
- Levin, S.M.; Baker, D.B.; Landrigan, P.J.; Monaghan, S.V.; Frumin, E.; Braithwaite, M.; Towne, W. Testicular Cancer in Leather Tanners Exposed to Dimethylformamide. Lancet 1987, 2, 1153. [Google Scholar] [CrossRef]
- Chen, J.L.; Fayerweather, W.E.; Pell, S. Cancer Incidence of Workers Exposed to Dimethylformamide and/or Acrylonitrile. J. Occup. Med. 1988, 30, 813–818. [Google Scholar] [CrossRef]
- Walrath, J.; Fayerweather, W.E.; Gilby, P.G.; Pell, S. A Case-Control Study of Cancer among Du Pont Employees with Potential for Exposure to Dimethylformamide. J. Occup. Med. 1989, 31, 432–438. [Google Scholar]
- Yoon, J.-H.; Yoo, C.-I.; Ahn, Y.-S. N,N-Dimethylformamide: Evidence of Carcinogenicity from National Representative Cohort Study in South Korea. Scand. J. Work Environ. Health 2019, 45, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.-Y.; Tsai, C.-Y.; Lin, Y.-Q.; Shih, T.-S.; Lin, Y.-C. Urinary Biomarkers of Occupational N,N-Dimethylformamide (DMF) Exposure Attributed to the Dermal Exposure. J. Expo. Anal. Environ. Epidemiol. 2004, 14, 214–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellwig, J.; Merkle, J.; Klimisch, H.J.; Jäckh, R. Studies on the Prenatal Toxicity of N,N-Dimethylformamide in Mice, Rats and Rabbits. Food Chem. Toxicol. 1991, 29, 193–201. [Google Scholar] [CrossRef]
- Fail, P.A.; George, J.D.; Grizzle, T.B.; Heindel, J.J. Formamide and Dimethylformamide: Reproductive Assessment by Continuous Breeding in Mice. Reprod. Toxicol. 1998, 12, 317–332. [Google Scholar] [CrossRef]
- Merkle, J.; Zeller, H. [Studies on acetamides and formamides for embryotoxic and teratogenic activities in the rabbit (author’s transl)]. Arzneimittelforschung 1980, 30, 1557–1562. [Google Scholar]
- Käfferlein, H.U.; Göen, T.; Müller, J.; Wrbitzky, R.; Angerer, J. Biological Monitoring of Workers Exposed to N,N-Dimethylformamide in the Synthetic Fibre Industry. Int. Arch. Occup. Environ. Health 2000, 73, 113–120. [Google Scholar] [CrossRef]
- Yang, J.S.; Kim, E.A.; Lee, M.Y.; Park, I.J.; Kang, S.K. Biological Monitoring of Occupational Exposure to N,N-Dimethylformamide--the Effects of Co-Exposure to Toluene or Dermal Exposure. Int. Arch. Occup. Environ. Health 2000, 73, 463–470. [Google Scholar] [CrossRef]
- Imbriani, M.; Maestri, L.; Marraccini, P.; Saretto, G.; Alessio, A.; Negri, S.; Ghittori, S. Urinary Determination of N-Acetyl- S-( N-Methylcarbamoyl)Cysteine and N-Methylformamide in Workers Exposed to N, N-Dimethylformamide. Int. Arch. Occup. Environ. Health 2002, 75, 445–452. [Google Scholar] [CrossRef]
- Seitz, M.; Kilo, S.; Eckert, E.; Müller, J.; Drexler, H.; Göen, T. Validity of Different Biomonitoring Parameters for the Assessment of Occupational Exposure to N,N-Dimethylformamide (DMF). Arch. Toxicol. 2018, 92, 2183–2193. [Google Scholar] [CrossRef]
- Will, W.; Schulz, G. N,N-Dimethylformamide (DMF) [Biomonitoring Methods, 1996]. In The MAK-Collection for Occupational Health and Safety; John Wiley & Sons, Ltd: Hoboken, NJ, USA, 2012; pp. 97–108. ISBN 978-3-527-60041-0. [Google Scholar]
- Käfferlein, H.U.; Angerer, J. Determination of N-Acetyl-S-(N-Methylcarbamoyl)Cysteine (AMCC) in the General Population Using Gas Chromatography-Mass Spectrometry. J. Environ. Monit. 1999, 1, 465–469. [Google Scholar] [CrossRef]
- Schettgen, T.; Musiol, A.; Kraus, T. Simultaneous Determination of Mercapturic Acids Derived from Ethylene Oxide (HEMA), Propylene Oxide (2-HPMA), Acrolein (3-HPMA), Acrylamide (AAMA) and N,N-Dimethylformamide (AMCC) in Human Urine Using Liquid Chromatography/Tandem Mass Spectrometry. Rapid. Commun. Mass Spectrom. 2008, 22, 2629–2638. [Google Scholar] [CrossRef] [PubMed]
- Kenwood, B.M.; Bagchi, P.; Zhang, L.; Zhu, W.; Chambers, D.M.; Blount, B.C.; De Jesús, V.R. Characterization of US Population Levels of Urinary Methylcarbamoyl Mercapturic Acid, a Metabolite of N,N-Dimethylformamide and Methyl Isocyanate, in the National Health and Nutrition Examination Survey (NHANES) 2005–2006 and 2011–2016. Environ. Sci. Pollut. Res. 2021, 28, 16781–16791. [Google Scholar] [CrossRef] [PubMed]
- HBM4EU. Deliverable 9.5 Prioritised List of Biomarkers, Matrices and Analytical Methods for the 2nd Prioritisation Round of Substances; HBM4EU, 2022. [Google Scholar]
- Alwis, K.U.; Blount, B.C.; Britt, A.S.; Patel, D.; Ashley, D.L. Simultaneous Analysis of 28 Urinary VOC Metabolites Using Ultra High Performance Liquid Chromatography Coupled with Electrospray Ionization Tandem Mass Spectrometry (UPLC-ESI/MSMS). Anal. Chim. Acta 2012, 750, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Wang, V.-S.; Shih, T.-S.; Cheng, C.-C.; Chang, H.-Y.; Lai, J.-S.; Lin, C.-C. Evaluation of Current Biological Exposure Index for Occupational N, N-Dimethylformamide Exposure from Synthetic Leather Workers. J. Occup. Environ. Med. 2004, 46, 729–736. [Google Scholar] [CrossRef]
- Kim, H.-A.; Kim, K.; Heo, Y.; Lee, S.-H.; Choi, H.-C. Biological Monitoring of Workers Exposed to N, N-Dimethylformamide in Synthetic Leather Manufacturing Factories in Korea. Int. Arch. Occup. Environ. Health 2004, 77, 108–112. [Google Scholar] [CrossRef]
- Tomasini, M.; Todaro, A.; Piazzoni, M.; Peruzzo, G.F. Exposure to dimethylformamide: Study of 14 cases. Med. Lav. 1983, 74, 217–220. [Google Scholar]
- Cirla, A.M.; Pisati, G.; Invernizzi, E.; Torricelli, P. Epidemiological Study on Workers Exposed to Low Dimethylformamide Concentrations. G. Ital. Med. Lav. 1984, 6, 149–156. [Google Scholar]
- Wang, C.; Huang, C.; Wei, Y.; Zhu, Q.; Tian, W.; Zhang, Q. Short-Term Exposure to Dimethylformamide and the Impact on Digestive System Disease: An Outdoor Study for Volatile Organic Compound. Environ. Pollut. 2014, 190, 133–138. [Google Scholar] [CrossRef]
| Route | Effects on Liver | Reproductive Effects | Carcinogenic Effects on Liver |
|---|---|---|---|
| Inhalation | NOAEL: 25 ppm LOAEL: 100 ppm (Rats and mice) [68] | NOAEL: 25 ppm LOAEC: 150 ppm (Rabbits) [76] | LOAEC: 200 ppm (mice) LOAEC: 400 ppm (rats) [67] |
| Oral | NOAEL = 238 mg/kg bw/d LOAEL = 475 mg/kg bw/d (Rats) (BASF (1977) unpublished data, quoted by ECHA [7]) | NOAEL = 166 mg/kg bw/d LOAEL = 503 mg/kg bw/d (Rats) [76] NOAEL: 44.1 mg/kg bw/d (Rabbits) [78] | LOAEL = 800 ppm (Rats) [69] |
| Dermal | - | LOAEL: 94 mg/kg/d (Rats) 100 mg/kg/d (Rabbits) [76] | - |
| Analyte | Biological Matrix | Advantages | Limits |
|---|---|---|---|
| Total NMF | Urine |
|
|
| AMCC | Urine |
|
|
| MCVal | Blood |
|
|
| DMF | Urine |
|
|
| Formamide | Urine | None |
|
| Agency | Reference Value for Airborne DMF (Key Studies and Critical Effect) | Biomarker | Approach/ Endpoint | Key Study | Internal TRV and Sampling Time |
|---|---|---|---|---|---|
| SCOEL, 2006 [20] | 8h-TWA = 5 ppm (Liver damage in rats and mice, exposed by inhalation, whole body) [68] | tNMF in urine | Correlation based on the OEL of 5 ppm | Studies in workers [32,48,55,79,80,81,89,90] | BLV = 15 mg·L−1 Post-shift |
| ACGIH, 2017 [16] | TLV-TWA = 5 ppm Liver damage in rats and mice and irritation in humans (eyes and upper respiratory tract) [49,68,91,92] | tNMF in urine | Relation between BME levels and effects on liver | Studies in workers [27,45,48,55] | BEI = 30 mg·L−1 End of shift |
| AMCC in urine | Relation between BME levels and effects on liver | Studies in workers [45,55] | BEI = 30 mg·L−1 End of shift and end of workweek | ||
| DFG, 2019 [19] | MAK value = 5 ppm (Liver damage in rats and mice, exposed by inhalation, whole body) [68] | tNMF in urine | Correlation based on the MAK value of 5 ppm | Studies in workers [82] | BAT = 20 mg·L−1 End of exposure or end of shift |
| AMCC in urine | BAT = 25 mg·g−1·cr End of exposure or end of shift; Long-term exposure indicator: sampling at the end of a shift after several previous shifts |
| Urinary tNMF | Urinary AMCC | |
|---|---|---|
| Regarding the nature and quality of the toxicological data | The database on DMF is based on a large number of both human and animal studies, and data on tNMF are robust and consistent. LoC: High | The database on DMF is based on a large number of both human and animal studies, but available studies reporting results for AMCC are limited. LoC: Medium |
| Regarding the critical endpoint and mode of action | The confidence in the evidence of effects on the liver function is high. The effects on the liver after DMF exposure are well-studied in humans (workplace) and animals. LoC: High | The confidence in the evidence of effects on the liver function is high. The effects on the liver after DMF exposure are well-studied (in humans and animals). LoC: High |
| Regarding the selected key studies for identification of the POD and their results | The database gives several robust occupational studies with many subjects and consistent results for tNMF. The approach consists of the selection of a pool of studies (from 1980 to 2017) carried out on Asians and Caucasian people (to consider the genetic variability due to ethnicity). LoC: High | The HBM-GVWorker is based on a the same four studies used for the derivation of tNMF HBM-GVWorker. However, the results of these studies indicate a large interval of NOAEL values together with a large margin between NOAEL and LOAEL values. LoC: Low |
| Global LoC | High | Low-medium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamkarkach, F.; Meslin, M.; Kolossa-Gehring, M.; Apel, P.; Garnier, R. Human Biomonitoring Initiative (HBM4EU): Human Biomonitoring Guidance Values Derived for Dimethylformamide. Toxics 2022, 10, 298. https://doi.org/10.3390/toxics10060298
Lamkarkach F, Meslin M, Kolossa-Gehring M, Apel P, Garnier R. Human Biomonitoring Initiative (HBM4EU): Human Biomonitoring Guidance Values Derived for Dimethylformamide. Toxics. 2022; 10(6):298. https://doi.org/10.3390/toxics10060298
Chicago/Turabian StyleLamkarkach, Farida, Matthieu Meslin, Marike Kolossa-Gehring, Petra Apel, and Robert Garnier. 2022. "Human Biomonitoring Initiative (HBM4EU): Human Biomonitoring Guidance Values Derived for Dimethylformamide" Toxics 10, no. 6: 298. https://doi.org/10.3390/toxics10060298
APA StyleLamkarkach, F., Meslin, M., Kolossa-Gehring, M., Apel, P., & Garnier, R. (2022). Human Biomonitoring Initiative (HBM4EU): Human Biomonitoring Guidance Values Derived for Dimethylformamide. Toxics, 10(6), 298. https://doi.org/10.3390/toxics10060298