
Towards Reference Values for Malondialdehyde on Exhaled Breath Condensate: A Systematic Literature Review and Meta-Analysis

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Research
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Heterogeneity
4.1.1. Heterogeneity Related to the Collection of EBC
4.1.2. Heterogeneity Related to the Analytical Method
4.1.3. Heterogeneity Related to Data Collection and Reporting
5. Study Strengths and Limitations
6. Recommendations
- (a)
- Collection and reporting of demographics and health status, namely gender, age, smoking status, BMI, diet, living area, sports, and respiratory functions to insure that the study sample does really correspond to the reference sample, and that it is representative of the general healthy population and all its subgroups.
- (b)
- Collection and reporting of the time of EBC collection and volume of collected EBC as this is one ERS/ATS recommendation that has not yet been fulfilled. We strongly recommend avoiding the use of non-validated EBC collection devices since it has been shown that the inner surface of the collection equipment can interfere with the determination of biomarkers [67], presumably, also with MDA determination. Therefore, EBC collections need to be standardized. A greater number of studies respecting the current guidelines would help to get closer to establishing a standardized EBC collection method.
- (c)
- Reporting of analytical methods that may affect MDA quantification and other factors influencing or supposed to influence the results, related to the analysis itself or collection device and material.
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borrill, Z.L.; Roy, K.; Singh, D. Exhaled breath condensate biomarkers in COPD. Eur. Respir. J. 2008, 32, 472–486. [Google Scholar] [CrossRef] [PubMed]
- Repetto, M.; Semprine, J.; Boveris, A. Lipid Peroxidation: Chemical Mechanism, Biological Implications and Analytical Determination. In Lipid Peroxidation; Catala, A., Ed.; InTech: London, UK, 2012; Available online: http://www.intechopen.com/books/lipid-peroxidation/lipid-peroxidation-chemical-mechanism-biological-implications-and-analytical-determination (accessed on 19 October 2021).
- Ito, F.; Sono, Y.; Ito, T. Measurement and Clinical Significance of Lipid Peroxidation as a Biomarker of Oxidative Stress: Oxidative Stress in Diabetes, Atherosclerosis, and Chronic Inflammation. Antioxidants 2019, 8, 72. [Google Scholar] [CrossRef] [PubMed]
- Cherubini, A.; Ruggiero, C.; Polidori, M.C.; Mecocci, P. Potential markers of oxidative stress in stroke. Free. Radic. Biol. Med. 2005, 39, 841–852. [Google Scholar] [CrossRef]
- Cvetković, T.; Mitić, B.; Lazarević, G.; Vlahović, P.; Antić, S.; Stefanović, V. Oxidative stress parameters as possible urine markers in patients with diabetic nephropathy. J. Diabetes Its Complicat. 2009, 23, 337–342. [Google Scholar] [CrossRef]
- Jové, M.; Mota-Martorell, N.; Pradas, I.; Martín-Gari, M.; Ayala, V.; Pamplona, R. The Advanced Lipoxidation End-Product Malondialdehyde-Lysine in Aging and Longevity. Antioxidants 2020, 9, 1132. [Google Scholar] [CrossRef] [PubMed]
- Del Rio, D.; Stewart, A.J.; Pellegrini, N. A review of recent studies on malondialdehyde as toxic molecule and biological marker of oxidative stress. Nutr. Metab. Cardiovasc. Dis. 2005, 15, 316–328. [Google Scholar] [CrossRef]
- Kostikas, K.; Minas, M.; Nikolaou, E.; Papaioannou, A.I.; Liakos, P.; Gougoura, S.; Gourgoulianis, K.I.; Dinas, P.C.; Metsios, G.S.; Jamurtas, A.Z.; et al. Secondhand smoke exposure induces acutely airway acidification and oxidative stress. Respir. Med. 2013, 107, 172–179. [Google Scholar] [CrossRef]
- Denise, G.; Santa, M.L.; Juliana, V.; Clóvis, P.; Cristina, S.G.G.S.; Pomblum; Juarez, V.; Rocha, J.B.T.; Marcelo, F. Importance of the lipid peroxidation biomarkers and methodological aspects FOR malondialdehyde quantification. Quim. Nova 2009, 32, 169–174. [Google Scholar]
- Sauvain, J.J.; Edmé, J.L.; Wild, P.; Suarez, G.; Bezerra, O.M.P.A.; Talvani, A.; Algranti, E.; Carneiro, A.P.S.; Chérot-Kornobis, N.; Sobaszek, A.; et al. Does exposure to inflammatory particles modify the pattern of anion in exhaled breath condensate? J. Breath Res. 2020, 14, 026005. [Google Scholar] [CrossRef]
- Gaggini, M.; Sabatino, L.; Vassalle, C. Conventional and innovative methods to assess oxidative stress biomarkers in the clinical cardiovascular setting. Biotechniques 2020, 68, 223–231. [Google Scholar] [CrossRef]
- Hunt, J. Exhaled breath condensate: An evolving tool for noninvasive evaluation of lung disease. J. Allergy Clin. Immunol. 2002, 110, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.D.; Montpetit, A.; Hunt, J. Exhaled Breath Condensate: An overview. Immunol. Allergy Clin. N. Am. 2012, 32, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Horváth, I.; Barnes, P.J.; Loukides, S.; Sterk, P.J.; Högman, M.; Olin, A.C.; Amann, A.; Antus, B.; Baraldi, E.; Bikov, A. A European Respiratory Society technical standard: Exhaled biomarkers in lung disease. Eur. Respir. J. 2017, 49, 1600965. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.D.; Montpetit, A.J. Exhaled Breath Condensate: An update. Immunol. Allergy Clin. N. Am. 2018, 38, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Latzin, P.; Beck, J.; Bartenstein, A.; Griese, M. Comparison of exhaled breath condensate from nasal and oral collection. Eur. J. Med Res. 2003, 8, 505–510. [Google Scholar] [PubMed]
- Horváth, I.; Hunt, J.; Barnes, P.J. Exhaled breath condensate: Methodological recommendations and unresolved questions. Eur. Respir. J. 2005, 26, 523–548. [Google Scholar] [CrossRef] [PubMed]
- Forman, H.J.; Augusto, O.; Brigelius-Flohe, R.; Dennery, P.A.; Kalyanaraman, B.; Ischiropoulos, H.; Mann, G.E.; Radi, R.; Roberts, L.J.; Vina, J. Even free radicals should follow some rules: A Guide to free radical research terminology and methodology. Free. Radic. Biol. Med. 2015, 78, 233–235. [Google Scholar] [CrossRef]
- Hemmendinger, M.; Wild, P.; Shoman, Y.; Graille, M.; Bergamaschi, E.; Hopf, N.; Guseva Canu, I. Reference ranges of oxidative stress biomarkers selected for non-invasive biological surveillance of nanotechnology workers: Study protocol and meta-analysis results for 8-OHdG in exhaled breath condensate. Toxicol. Lett. 2020, 327, 41–47. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Shoman, Y.; Wild, P.; Hemmendinger, M.; Graille, M.; Sauvain, J.J.; Hopf, N.B.; Guseva Canu, I. Reference Ranges of 8-Isoprostane Concentrations in Exhaled Breath Condensate (EBC): A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2020, 21, 3822. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst Rev. Déc 2016, 5, 210. [Google Scholar]
- Aksu, K.; Kurt, H.; Gündüz, E.; Değirmenci, I.; Kurt, E. Inflammatory markers in exhaled breath condensate in patients with asthma and rhinitis. Tuberk Toraks 2012, 60, 321–326. [Google Scholar]
- Andreoli, R.; Manini, P.; Corradi, M.; Mutti, A.; Niessen, W.M.A. Determination of patterns of biologically relevant aldehydes in exhaled breath condensate of healthy subjects by liquid chromatography/atmospheric chemical ionization tandem mass spectrometry. Rapid Commun. Mass Spectrom. 2003, 17, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Antus, B.; Drozdovszky, O.; Barta, I.; Kelemen, K. Comparison of Airway and Systemic Malondialdehyde Levels for Assessment of Oxidative Stress in Cystic Fibrosis. Lung 2015, 193, 597–604. [Google Scholar] [CrossRef]
- Antus, B.; Harnasi, G.; Drozdovszky, O.; Barta, I. Monitoring oxidative stress during chronic obstructive pulmonary disease exacerbations using malondialdehyde: MDA and COPD exacerbations. Respirology 2014, 19, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Antczak, A.; Nowak, D.; Shariati, B.; Król, M.; Piasecka, G.; Kurmanowska, Z. Increased hydrogen peroxide and thiobarbituric acid-reactive products in expired breath condensate of asthmatic patients. Eur. Respir. J. 1997, 10, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Araneda, O.F.; García, C.; Lagos, N.; Quiroga, G.B.; Cajigal, J.Y.; Salazar, M.P.; Behn, C. Lung oxidative stress as related to exercise and altitude. Lipid peroxidation evidence in exhaled breath condensate: A possible predictor of acute mountain sickness. Eur. J. Appl. Physiol. 2005, 95, 383–390. [Google Scholar] [CrossRef]
- Araneda, O.; Guevara, A.; Contreras, C.; Lagos, N.; Berral, F. Exhaled Breath Condensate Analysis after Long Distance Races. Int. J. Sports Med. 2012, 33, 955–961. [Google Scholar] [CrossRef]
- Araneda, O.F.; Urbina-Stagno, R.; Tuesta, M.; Haichelis, D.; Alvear, M.; Salazar, M.P.; García, C. Increase of pro-oxidants with no evidence of lipid peroxidation in exhaled breath condensate after a 10-km race in non-athletes. J. Physiol. Biochem. 2014, 70, 107–115. [Google Scholar] [CrossRef]
- Barregard, L.; Sällsten, G.; Andersson, L.; Almstrand, A.C.; Gustafson, P.; Andersson, M.; Olin, A.C. Experimental exposure to wood smoke: Effects on airway inflammation and oxidative stress. Occup. Environ. Med. 2008, 65, 319–324. [Google Scholar] [CrossRef]
- Bartoli, M.L.; Novelli, F.; Costa, F.; Malagrinò, L.; Melosini, L.; Bacci, E.; Cianchetti, S.; Dente, F.L.; Di Franco, A.; Vagaggini, B.; et al. Malondialdehyde in Exhaled Breath Condensate as a Marker of Oxidative Stress in Different Pulmonary Diseases. Mediat. Inflamm. 2011, 2011, 891752. [Google Scholar] [CrossRef]
- Brand, P.; Bischof, K.; Siry, L.; Bertram, J.; Schettgen, T.; Reisgen, U.; Kraus, T.; Gube, M. Exposure of healthy subjects with emissions from a gas metal arc welding process: Part 3—biological effect markers and lung function. Int. Arch. Occup. Environ. Health 2013, 86, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Caglieri, A.; Goldoni, M.; Acampa, O.; Andreoli, R.; Vettori, M.V.; Corradi, M.; Apostoli, P.; Mutti, A. The Effect of Inhaled Chromium on Different Exhaled Breath Condensate Biomarkers among Chrome-Plating Workers. Environ. Health Perspect. 2006, 114, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Casimirri, E.; Stendardo, M.; Bonci, M.; Andreoli, R.; Bottazzi, B.; Leone, R.; Schito, M.; Vaccari, A.; Papi, A.; Contoli, M.; et al. Biomarkers of oxidative-stress and inflammation in exhaled breath condensate from hospital cleaners. Biomarkers 2016, 21, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Corradi, M.; Rubinstein, I.; Andreoli, R.; Manini, P.; Caglieri, A.; Poli, D.; Alinovi, R.; Mutti, A. Aldehydes in Exhaled Breath Condensate of Patients with Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2003, 167, 1380–1386. [Google Scholar] [CrossRef]
- Corradi, M.; Alinovi, R.; Goldoni, M.; Vettori, M.; Folesani, G.; Mozzoni, P.; Cavazzini, S.; Bergamaschi, E.; Rossi, L.; Mutti, A. Biomarkers of oxidative stress after controlled human exposure to ozone. Toxicol. Lett. 2002, 134, 219–225. [Google Scholar] [CrossRef]
- Corradi, M. Comparison between exhaled and sputum oxidative stress biomarkers in chronic airway inflammation. Eur. Respir. J. 2004, 24, 1011–1017. [Google Scholar] [CrossRef]
- Doruk, S.; Ozyurt, H.; Inonu, H.; Erkorkmaz, U.; Saylan, O.; Seyfikli, Z. Oxidative status in the lungs associated with tobacco smoke exposure. Clin. Chem. Lab. Med. 2011, 49, 2007–2012. Available online: https://www.degruyter.com/document/doi/10.1515/CCLM.2011.698/html (accessed on 30 March 2022). [CrossRef]
- Goldoni, M.; Catalani, S.; De Palma, G.; Manini, P.; Acampa, O.; Corradi, M.; Bergonzi, R.; Apostoli, P.; Mutti, A. Breath Condensate as a Suitable Matrix to Assess Lung Dose and Effects in Workers Exposed to Cobalt and Tungsten. Environ. Health Perspect. 2004, 112, 1293–1298. [Google Scholar] [CrossRef]
- Goldoni, M.; Corradi, M.; Mozzoni, P.; Folesani, G.; Alinovi, R.; Pinelli, S.; Andreoli, R.; Pigini, D.; Tillo, R.; Filetti, A.; et al. Concentration of exhaled breath condensate biomarkers after fractionated collection based on exhaled CO2 signal. J. Breath Res. 2013, 7, 017101. [Google Scholar] [CrossRef]
- Goldoni, M.; Caglieri, A.; Andreoli, R.; Poli, D.; Manini, P.; Vettori, M.V.; Corradi, M.; Mutti, A. Influence of condensation temperature on selected exhaled breath parameters. BMC Pulm. Med. 2005, 5, 10. [Google Scholar] [CrossRef]
- Gong, J.; Zhu, T.; Kipen, H.; Wang, G.; Hu, M.; Ohman-Strickland, P.; Lu, S.E.; Zhang, L.; Wang, Y.; Zhu, P.; et al. Malondialdehyde in exhaled breath condensate and urine as a biomarker of air pollution induced oxidative stress. J. Expo. Sci. Environ. Epidemiol. 2013, 23, 322–327. [Google Scholar] [CrossRef]
- Graczyk, H.; Lewinski, N.; Zhao, J.; Sauvain, J.J.; Suarez, G.; Wild, P.; Danuser, B.; Riediker, M. Increase in oxidative stress levels following welding fume inhalation: A controlled human exposure study. Part. Fibre Toxicol. 2015, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Gube, M.; Ebel, J.; Brand, P.; Göen, T.; Holzinger, K.; Reisgen, U.; Kraus, T. Biological effect markers in exhaled breath condensate and biomonitoring in welders: Impact of smoking and protection equipment. Int. Arch. Occup. Environ. Health 2010, 83, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Inonu, H.; Doruk, S.; Sahin, S.; Erkorkmaz, U.; Celik, D.; Celikel, S.; Seyfikli, Z. Oxidative Stress Levels in Exhaled Breath Condensate Associated With COPD and Smoking. Respir. Care 2012, 57, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Lärstad, M.; Ljungkvist, G.; Olin, A.-C.; Torén, K. Determination of malondialdehyde in breath condensate by high-performance liquid chromatography with fluorescence detection. J. Chromatogr. B 2002, 766, 107–114. [Google Scholar] [CrossRef]
- Laumbach, R.J.; Kipen, H.M.; Ko, S.; Kelly-McNeil, K.; Cepeda, C.; Pettit, A.; Ohman-Strickland, P.; Zhang, L.; Zhang, J.; Gong, J.; et al. A controlled trial of acute effects of human exposure to traffic particles on pulmonary oxidative stress and heart rate variability. Part. Fibre Toxicol. 2014, 11, 45. [Google Scholar] [CrossRef]
- Lee, J.S.; Choi, Y.C.; Shin, J.H.; Lee, J.H.; Lee, Y.; Park, S.Y.; Baek, J.E.; Park, J.D.; Ahn, K.; Yu, I.J. Health surveillance study of workers who manufacture multi-walled carbon nanotubes. Nanotoxicology 2015, 9, 802–811. [Google Scholar] [CrossRef]
- Majewska, E.; Kasielski, M.; Luczynski, R.; Bartosz, G.; Bialasiewicz, P.; Nowak, D. Elevated exhalation of hydrogen peroxide and thiobarbituric acid reactive substances in patients with community acquired pneumonia. Respir. Med. 2004, 98, 669–676. [Google Scholar] [CrossRef][Green Version]
- Nowak, D.; Kałucka, S.; Białasiewicz, P.; Król, M. Exhalation of H2O2 and thiobarbituric acid reactive substances (TBARs) by healthy subjects. Free Radic. Biol. Med. 2001, 30, 178–186. [Google Scholar] [CrossRef]
- Pelclova, D.; Zdimal, V.; Schwarz, J.; Dvorackova, S.; Komarc, M.; Ondracek, J.; Kostejn, M.; Kacer, P.; Vlckova, S.; Fenclova, Z.; et al. Markers of Oxidative Stress in the Exhaled Breath Condensate of Workers Handling Nanocomposites. Nanomaterials 2018, 8, 611. [Google Scholar] [CrossRef]
- Pelclová, D.; Fenclová, Z.; Vlčková, S.; Klusáčková, P.; Lebedová, J.; Syslová, K.; Běláček, J.; Kuzma, M.; Navrátil, T.; Zakharov, S. Occupational asthma follow-up—which markers are elevated in exhaled breath condensate and plasma? Int. J. Occup. Med. Environ. Health 2014, 27, 206–215. Available online: http://ijomeh.eu/Occupational-asthma-follow-up-Which-markers-are-elevated-in-exhaled-breath-condensate-and-plasma-,2044,0,2.html (accessed on 30 March 2022). [CrossRef] [PubMed]
- Pelclova, D.; Zdimal, V.; Kacer, P.; Fenclova, Z.; Vlckova, S.; Syslova, K.; Navratil, T.; Schwarz, J.; Zikova, N.; Barosova, H. Oxidative stress markers are elevated in exhaled breath condensate of workers exposed to nanoparticles during iron oxide pigment production. J. Breath Res. 2016, 10, 016004. [Google Scholar] [CrossRef]
- Riccelli, M.G.; Goldoni, M.; Andreoli, R.; Mozzoni, P.; Pinelli, S.; Alinovi, R.; Selis, L.; Mutti, A.; Corradi, M. Biomarkers of exposure to stainless steel tungsten inert gas welding fumes and the effect of exposure on exhaled breath condensate. Toxicol. Lett. 2018, 292, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Rundell, K.W.; Slee, J.B.; Caviston, R.; Hollenbach, A.M. Decreased Lung Function After Inhalation of Ultrafine and Fine Particulate Matter During Exercise is Related to Decreased Total Nitrate in Exhaled Breath Condensate. Inhal. Toxicol. 2008, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sakhvidi, M.J.; Biabani Ardekani, J.; Firoozichahak, A.; Zavarreza, J.; Hajaghazade, M.; Mostaghaci, M.; Mehrparvar, A.; Barkhordari, A. Exhaled breath malondialdehyde, spirometric results and dust exposure assessment in ceramics production workers. Int. J. Occup. Med. Environ. Health 2015, 28, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Sauvain, J.-J.; Hohl, M.S.S.; Wild, P.; Pralong, J.A.; Riediker, M. Exhaled Breath Condensate as a Matrix for Combustion-Based Nanoparticle Exposure and Health Effect Evaluation. J. Aerosol Med. Pulm. Drug Deliv. 2014, 27, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Stockfelt, L.; Sallsten, G.; Olin, A.C.; Almerud, P.; Samuelsson, L.; Johannesson, S.; Molnar, P.; Strandberg, B.; Almstrand, A.C.; Bergemalm-Rynell, K. Effects on airways of short-term exposure to two kinds of wood smoke in a chamber study of healthy humans. Inhal. Toxicol. 2012, 24, 47–59. [Google Scholar] [CrossRef]
- Syslová, K.; Kacer, P.; Kuzma, M.; Najmanová, V.; Fenclová, Z.; Vlcková, S.; Lebedová, J.; Pelclová, D. Rapid and easy method for monitoring oxidative stress markers in body fluids of patients with asbestos or silica-induced lung diseases. J. Chromatogr. B 2009, 877, 2477–2486. [Google Scholar] [CrossRef]
- Szkudlarek, U.; Maria, L.; Kasielski, M.; Kaucka, S.; Nowak, D. Exhaled hydrogen peroxide correlates with the release of reactive oxygen species by blood phagocytes in healthy subjects. Respir. Med. 2003, 97, 718–725. [Google Scholar] [CrossRef][Green Version]
- Tanger, S.R.O. (Ed.) Proceedings of the 10th Anniversary International Conference on Nanomaterials—Research and Application (NANOCON 2018), Brno, Czech Republic, 17–19 October 2018; Curran Associates: Red Hook, NY, USA, 2019; p. 741.
- Pinchuk, I.; Weber, D.; Kochlik, B.; Stuetz, W.; Toussaint, O.; Debacq-Chainiaux, F.; Dollé, M.E.T.; Jansen, E.H.J.M.; Gonos, E.S.; Sikora, E. Gender- and age-dependencies of oxidative stress, as detected based on the steady state concentrations of different biomarkers in the MARK-AGE study. Redox Biol. 2019, 24, 101204. [Google Scholar] [CrossRef]
- Caliri, A.W.; Tommasi, S.; Besaratinia, A. Relationships among smoking, oxidative stress, inflammation, macromolecular damage, and cancer. Mutat. Res./Rev. Mutat. Res. 2021, 787, 108365. [Google Scholar] [CrossRef] [PubMed]
- Lykkesfeldt, J. Malondialdehyde as biomarker of oxidative damage to lipids caused by smoking. Clin. Chim. Acta 2007, 380, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Carraro, E.; Schilirò, T.; Biorci, F.; Romanazzi, V.; Degan, R.; Buonocore, D.; Verri, M.; Dossena, M.; Bonetta, S.; Gilli, G. Physical Activity, Lifestyle Factors and Oxidative Stress in Middle Age Healthy Subjects. Int. J. Environ. Res. Public Health 2018, 15, 1152. [Google Scholar] [CrossRef]
- Rosias, P. Methodological aspects of exhaled breath condensate collection and analysis. J. Breath Res. 2012, 6, 027102. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Study Objectives | Population Studied and Number of Participants | Control Population | Method of EBC Collection and Analysis | Main Findings | Quality Score |
|---|---|---|---|---|---|---|
| Aksu, 2012, Turkey [23] | To investigate lower airway inflammation using malondialdehyde and total protein measurement in exhaled breath condensate | 12 Mild asthma, 53 persistent rhinitis, and 16 concomitant asthma and rhinitis | 13 Control subjects (5 males and 8 females) | EBC was collected with a homemade apparatus for max 15 min at 10.00 am, no nose clip, immediately stored at −80 °C | MDA and total protein levels in EBC did not differ among the groups | 14 Moderate |
| Andreoli, 2003, Italy [24] | Method development | None | 2 Non-smoking and 13 asymptomatic smoking control subjects | EBC collected on EcoScreen, 15 min with nose clip, and then quickly stored at −80 °C | MDA concentrations were consistent with those determined in EBC using an independent HPLC-FLD method, mass spectrometry to EBC analysis could play a fundamental role in the validation of EBC as a new accessible biological matrix and in the definition of standardized EBC collection | 12 Moderate |
| Antus, 2015, Hungary [25] | To investigate oxidative stress in cystic fibrosis (CF) patients | 40 Patients with CF | 25 Control subjects (13 males and 12 females) | EBC collection with an EcoScreen condenser using MDA reagent kit, MDA concentrations in EBC were measured with an isocratic HPLC system | 19 High | |
| Antus, 2013, Hungary [26] | To investigate MDA levels in patients with acute COPD exacerbation | 55 Patients with COPD | 20 Healthy controls, ex-smokers (10 females and 10 males) | EBC collected for 10 min EcoScreen condenser, samples were stored frozen at −80 °C before analysis, isocratic HPLC system using MDA reagent kit | 12 Moderate | |
| Antczak, 1997, Poland [27] | To determine whether asthmatic patients exhale more H2O2 and TBARS than healthy subjects | 21 Asthmatic patients | 10 Healthy subjects (6 males and 4 females) | EBC collected in a tube installed in a polystyrene foam container filled with ice and salt, for 20 min, and aliquotes were transferred in Eppendorf tubes stored at −80 °C for no longer than 7 days until measurement, TBAR species in expired breath condensate was determined according to the method of YAGI | H2O2 was 26 times higher in asthmatic EBC as compared with TBARS, these findings were statistically significant | 15 Moderate |
| Araneda, 2005, Chile [28] | To investigate lung oxidative stress in subjects exercising in moderate and high altitude | None | 6 Healthy males | EBC collected with self-constructed device for 20 min, condensated at −5 °C, and stored in liquid nitrogen, MDA was determined with HPLC according to Larstad | Lung OS may constitute a pathogenic factor in acute mountain sickness | 11 Moderate |
| Araneda, 2012, Chile [29] | To investigate the impact of an endurance race on pulmonary pro-oxidative formation and lipoperoxidation | 41 Healthy recreational runners divided into 3 groups according to the races they decided to run (10, 21.1, and 41.2 km) non-smokers | Two groups (10 and 42.2 km) with MDA in EBC, pre-race data was available just for these subjects | EBC collected with self-constructed device for 10 to 20 min, with nose clip, condensated at −5 °C, and stored in liquid nitrogen, MDA was determined with HPLC according to Larstad | Intense prolonged exercise favors an increase in pulmonary pro-oxidative levels, with no modifications on lipoperoxidation; Running time relates to the magnitude of acute post exercise pro-oxidative formation | 12 Moderate |
| Araneda, 2013, Chile [30] | To investigate pro-oxidative, lipid peroxidation, and inflammation in EBC, in subjects running 10 km | None | 10 Physically active healthy subjects (9 males and 1 female), EBC measured 20 min before the race | EBC collected with self-constructed device for 10 to 15 min, with nose clip, condensated at −5 °C, and stored in liquid nitrogen, MDA was determined with HPLC according to Larstad | Unlike the previous results obtained in amateur runners, in physically active subjects, 10 km produces an increase in oxygen- and nitrogen-derived pro-oxidative species, without early peroxidation | 7 Low |
| Barregard, 2007, Sweden [31] | To examine whether short-term exposure to wood smoke in healthy subjects affects markers of pulmonary inflammation and oxidative stress | 13 Healty subjects (6 males and 7 females), EBC measured prior to exposure | EBC was collected with an Rtube, with nose clip, until 80 L were collected, samples were frozen at −20 °C, MDA was determined with HPLC according to Larstad | Wood smoke exposure affects the respiratory tract, especially the lower airways | 10 Moderate | |
| Bartoli, 2011, Italy [32] | To assess the usefulness of MDA in EBC in different groups of pulmonary diseases | 64 Subjects with asthma, 19 with bronchiectasies, 73 with COPD, 38 with idiopathic pulmonary fibrosis | 14 Healthy non-smoking subjects | EBC was collected on an EcoScreen device, during 15 min, samples were immediately stored at −80 °C and analyzed within 6 months, with HPLC according to Larstad | Subjects with chronic airway disorders have increased levels of MDA in EBC, MDA concentrations in EBC are related to FEV1 and neutrophilic inflammation, particularly in COPD patients. | 15 Moderate |
| Brand, 2013, Germany [33] | To investigate if short-term exposure to welding fumes results in changes in lung function and early stages of inflammatory reactions | 12 Healthy non-smoking males | EBC was collecte on an ECOSCREEN device wearing a nose clip, for 20 min, samples stored at −80 °C until analysis, MDA was derivatized with DNPH, and then separated by HPLC and determined by mass spectrometry | In healthy, young subjects, neither changes in spirometry nor changes in inflammatory markers measured in exhaled breath condensate could be detected after short-term exposure | 12 Moderate | |
| Caglieri, 2006, Italy [34] | To investigate chromium levels in EBC of workers exposed to Cr(VI) and to assess their relationship with biochemical changes in the airways by analyzing EBC biomarkers of oxidative stress | 24 Chrome-plating workers | 25 Control subjects (13 males and 12 females, 5 ex-smokers and 20 non-smokers) | EBC was collected on TURBO DECCS, condensation temperature of −5 °C, during 15 min; MDA-EBC was measured by tandem liquid chromatography–mass spectrometry | Cr-EBC levels correlated with those of H2O2-EBC and MDA-EBC, as well as with urinary Cr levels. | 14 Moderate |
| Casimirri, 2015, Italy [35] | Casimirri, 2015, Italy | Casimirri, 2015, Italy | Casimirri, 2015, Italy | Casimirri, 2015, Italy | Professional exposure to chlorinated agents increases EBC biomarkers of oxidativestress and inflammation | 15 Moderate |
| Corradi, 2003, Italy [36] | To evaluate if aldehydes could be measured in EBC, to assess the influence of sampling procedures, to compare levels of different pulmonary disease groups with those of a control group | 20 Patients with stable COPD (18 males and 2 females) | 12 Smoking (9 males and 3 females) and 20 non-smoking (17 males and 3 females) control subjects | EBC was collected on a Tygon Tube immersed in thawing ice, and then frozen to −80 °C, no nose clip, MDA measured with LC-MS tandem | Aldehydes were identified in EBC, all, but were lower in control groups | 16 Moderate |
| Corradi, 2002, Italy [37] | To investigate if short-term exposure to ozone (O3) induces changes in biomarkers of lung inflammation and oxidative stress in EBC | 22 Non-smoking healthy control subjects (12 males and females) | EBC was collected on an ECO SCREEN device, during 15 min, frozen at −80 °C, MDA was measured as TBARS according to Nowak | A single 2-hour exposure to 0.1 ppm of O3 induces changes in biomarkers of inflammation and oxidative stress in those susceptible | 11 Moderate | |
| Corradi, 2004, Italy [38] | To compare aldehyde levels resulting from lipid peroxidation in EBC and induced sputum (IS) supernatant of subjects with asthma and chronic obstructive pulmonary disease | 21 Subjects with COPD, 10 asthmatics | 9 Healthy non-smoking control subjects (8 females and 1 male) | EBC was collected on a two glass chamber device from Incofar, no nose clip for 20 min, samples were stored at −80 °C, and MDA measured according to Larstad | Aldehydes can be detected in both exhaled breath condensate and supernatant of induced sputum, but their relative concentrations are different and not correlated with each other | 12 Moderate |
| Doruk, 2011, Turkey [39] | To investigate oxidative stress in the lungs associated with tobacco smoke and to evaluate the effect of this stress with pulmonary function tests | 69 Healthy subjects divided into 3 groups according to their exposure to tobacco smoke: 26 current smokers (23 males and 3 females), 21 subjects (15 males and 6 females) who did not smoke within the last year but had second-hand smoking and 22 (100 males and 12 females) with no tobacco smoke exposure | EBC was collected on an ECOSCREEN device for 15 min, wearing a nose clip, samples stored at −70 °C, MDA measured as TBARS | The levels of MDA, 8-OHdG, SOD, and GSH-Px were higher in smokers; NO levels gradually increased from Group I to Group III; MDA levels were lower in Group III than Group II | 14 Moderate | |
| Goldoni, 2004, Italy [40] | To investigate whether EBC can be used as a suitable matrix to assess target tissue dose and effects of inhaled cobalt and tungsten, using EBC malondialdehyde (MDA) as a biomarker of pulmonary oxidative stress | 33 Workers exposed to Co and W in workshops producing either diamond tools or hard-metal mechanical parts | 16 Control subjects (11 males and 5 females) | EBC was collected on a homemade apparatus, during 10 min, samples were transported in ice to the lab, and then stored at −80 °C, MDA was measured by liquid chromatography–tandem mass spectrometry (LC-MS/MS) | MDA levels were increased depending on cobalt concentration and were enhanced by coexposure to tungsten. | 11 Moderate |
| Goldoni, 2013, Italy [41] | To compare the concentration of several biomarkers in whole (W-EBC) and fractionated EBC (A-EBC) | 45 Healthy control subjects (10 males and 35 females, 6 smokers and 39 non-smokers) | EBC was collected on a homemade apparatus for the fractioned EBC and a TURBODECCS for the whole EBC for 15 min without a nose clip, EBC was centrifuged, and then stored at −80 °C, MDA was measured by liquid chromatography–tandem mass spectrometry | H2O2, 8-isoprostane, malondialdehyde, and 4-hydroxy-2-nonhenal were all higher in W-EBC, suggesting a contribution from the upper airways to oxidative stress biomarkers in apparently healthy subjects | 10 Moderate | |
| Goldoni, 2005, Italy [42] | To test the effect of condensation temperature on the parameters of exhaled breath condensate and the levels of selected biomarkers | 24 Healthy control subjects (13 males and 11 females, 3 ex-smokers and 21 non-smokers) | EBC was collected on a TURBODECCS, during 10 min, at different temperatures, samples were centrifuged, and then stored at −80 °C, MDA was measured by liquid chromatography–tandem mass spectrometry (LC-MS/MS) within 2 weeks | Cooling temperature of exhaled breath condensate collection influenced selected biomarkers | 13 Moderate | |
| Gong, 2014, USA/China [43] | To compare ultrafine particles (UFPs) and fine particles (PM2.5) with respect to their associations with biomarkers reflecting multiple pathophysiological pathways linking exposure and cardiorespiratory events | 125 Healthy non-smoking individuals (initially 64 males and 64 females) working on a campus near Peking’s University Health Sciences Centre | EBC was collected on an ECOSCREEN device, collected for 20 min, with nose clip, aliquotes stored at −70 °C, MDA was measured as MDA-TBA in HPLC | Associations of certain biomarkers with UFPs had different lag patterns as compared with those with PM2.5, suggesting that the ultrafine size fraction and the fine size fraction of PM2.5 are likely to affect PM-induced pathophysiological pathways independently | 15 Moderate | |
| Graczyk, 2016, Switzerland [44] | To investigate time course changes of particle-associated oxidative stress in exposed tungsten inert gas welders | 20 Non-smoking healthy volunteers, with less than 1 year of apprentice in welding | EBC was collected on an Rtube, during 10 min, while wearing a nose clip, EBC samples were stored at −70 °C, MDA was measured by HPLC separation and fluorescence detection TBARS | A 60-minute exposure to TIG welding fume in a controlled, well-ventilated setting induced acute oxidative stress at 3 h post exposure in healthy, non-smoking apprentice welders not chronically exposed to welding fumes | 10 Moderate | |
| Gube, 2010, Germany [45] | To investigate the effect of welding as well as the impact of smoking and protection measures on biological markers in EBC | 45 Male welders | 24 Healthy males, non-exposed | EBC was collected on an ECOSCREEN device, wearing a nose clip, as long as 200 L of exhaled breath was collected, then stored at −80 °C, MDA was measued with a previously described but slightly changed method, i.e., MDA derivatized with DNPH and separated by HPLC, and then tandem mass spectrometry | Welders showed significantly increased concentrations of all these parameters at baseline as compared with non-exposed controls | 14 Moderate |
| Inonu, 2012, Turkey [46] | To evaluate the differences in the burden of oxidative stress in patients with COPD, smokers, and non-smokers by measuring hydrogen peroxide (H2O2), malondialdehyde (MDA), and 8-isoprostane levels in EBC | 25 Male COPD smokers | 26 Smokers and 29 non-smokers, males, healthy | EBC collected on an EcoScreen device, 15 min with nose clip, and then quickly stored at −70 °C for 6 months, MDA was measured using a commercial kit in a fluorescence detector in HPLC | Even if respiratory function tests were within normal limits, oxidant burden in the lungs of smokers was equivalent to that in COPD patients, 8-isoprostane could be useful in assessing symptom severity and health status of COPD patients | 16 Moderate |
| Larstad, 2001, Sweden [47] | To develop a method of MDA quantification | 29 Patients with asthma, 7 of which with wheezing | 15 control subjects without asthma | EBC was collected on an ECOSCREEN d evice, during 4 min, with a nose clip, stored at −20 °C until analysis, MDA was measured using TBS at 95 °C, and then separated by HPLC and MDA-TBA measured by fluorescence | No statistically significant difference between patients with asthma and patients without asthma; however, among females, subjects with asthma had higher MDA levels as compared with females without asthma; the use of the method when studying airway inflammation has to be further evaluated | 12 Moderate |
| Laumbach, 2014, USA [48] | To determine if exposure to traffic-related pollutant particles (TRAPs) during commuting causes acute oxidative stress in the respiratory tract or changes in heart rate variability | 21 Young volunteers (15 males and 6 females) | EBC was collected with an ECOSCREEN device, for 20 min, samples were frozen to −80 °C, MDA analysiswas performed by using a mixture of EBC, phosphoric acid, and thiobarbituric acid, which was heated and injected into an HPLC fluorescence system | Increases in markers of oxidative stress in EBC may represent early biological responses to widespread exposures to TRAPs particles that affect passengers in vehicles on heavily trafficked roadways | 9 Low | |
| Lee, 2015, Korea [49] | To investigate the actual health effects of multi wall carbon nanotubes in manufacturing workers | 9 Male carbon nanotube manufacturing workers, 5 smokers | 4 Office workers (3 males and 1 female), 2 smokers | EBC was collected on an Rtube, during 10 min, with a noseclip, stored in dry ice for 2 weeks. MDA was measured using fluorescence HPLC | Analyzed biomarkers in the MWCNT manufacturing workers were significantly higher than those in the office workers; MDA, n-hexanal, and molybdenum could be useful biomarkers of MWCNT exposure | 10 Moderate |
| Majewska, 2004, Poland [50] | To determine whether concentrations of H2O2 and TBARs in EBC are elevated and correlate with systemic response to pneumonia during 10 days of hospital treatment | 43 Inpatients with community acquired pneumonia (12 females and 31 males) | 20 Healthy non-smoking control subjects (6 females and 14 males) | EBC was collected on a device from Jaeger, cooled with ethanol at −9 °C, during 20 min, wearing a nose clip, stored on ice until measurement was performed, MDA was measured as TBARS | Pneumonia is accompanied by oxidative stress in airways that moderately correlates with intensity of systemic inflammatory response, determination of H2O2 in EBC may be helpful for noninvasive monitoring of oxidant production during lower respiratory tract infection | 13 Moderate |
| Nowak, 2001, Poland [51] | To investigate the concentration of H2O2 and TBARs in EBC and influencing factors | 58 Healthy volunteers (18 smokers and 40 non-smokers, 31 males and 27 females) | EBC was collected on a device from Jaeger Toennies, during 20 min, wearing a noseclip, MDA was measured as TBARS spectrofotometrically | Neither moderate exercise nor one puff of salbutamol nor ipratropium significantly influenced the concentration of H2O2 and TBARs in EBC, only 4 of 120 EBC specimens from non-smoker subjects revealed detectable levels of TBARs, cigarette smokers exhaled more TBARs | 11 Moderate | |
| Pelclova, 2018, Czech Republic [52] | To investigate lung oxidative stress in workers handling nanocomposites | 19 Nanocomposite-synthesizing and processing researchers (14 males and 5 females), all non-smokers | 19 Control subjects (13 males and 6 females, all non-smokers) | EBC was collected on an ECOSCREEN device, until a minimum of 120 L of exhaled breath, wearing a nose clip, immediately stored at −80 °C, MDA was measured | Significant associations were found between working in nanocomposite synthesis and EBC biomarkers; more research is needed to understand the contribution of nanoparticles from nanocomposite processing in inducing oxidative stress, relative to other co-exposures generated during welding, smelting, and secondary oxidation processes | 12 Moderate |
| Pelclova, 2014, Czech Republic [53] | To search for optimal markers in the exhaled breath condensate (EBC), plasma, and urine that would reflect the activity/severity of occupational asthma (OA) after withdrawal from the exposure to the allergen | 43 Subjects with previously diagnosed immunological OA (18 males and 25 females) | 20 Control subjects, working as office or healthcare employees and having no symptoms of asthma (10 males and 10 females) | EBC was collected for 15–20 min with EcoScreen, wearing a nose clip, samples were stored at −80 °C for a maximum of 2 months, MDA was measured with LC-ESI-MS/MS | Improvement in OA is very slow and objective impairments persist years after removal from the exposure; cysteinyl LTs and 8-ISO in EBC and 8-ISO in plasma might enrich the spectrum of useful objective tests for the follow-up of OA | 12 Moderate |
| Pelclova, 2016, Czech Republic [54] | To investigate the utility of oxidative stress biomarkers in EBC in iron oxide pigment production workers | 14 male workers, 43 ± 7 years, 43% smokers | 14 Males, 39 ± 4 years, 50% smokers, non-exposed | EBC was collected for 15 min with an EcoScreen device, wearing a nose clip, samples were stored at −80 °C, MDA was measured with LC-ESI-MS/MS | Almost all markers of lipid, nucleic acid, and protein oxidation were elevated in the EBC of workers as compared with control subjects; markers in urine were not elevated | 10 Moderate |
| Ricelli, 2018, Italy [55] | To investigate the cromium and nickel content of EBC of stainless steel (SS) tungsten inert gas (TIG) welders, and relate their concentrations with oxidative stress and inflammatory biomarkers | 100 SS welding workers, aged 18–65 years, smokers/non-smokers/ex-smokers 33/36/31, values were considered pre-shift | EBC was collected on an ECOSCREEN device, during 15 min, and stored at −80 °C, MDA was determined by tandem LC-MS/MS | Given the weak relationship between the biomarkers and effects of exposure, we speculate that other substances generated during SS TIG welding also play a role in generating lung oxidative stress | 11 Moderate | |
| Rundell, 2008, USA [56] | To investigate PM1 inhalation during exercise on lung function, exhaled nitric oxide (eNO), total nitrate (NO3), S-nitrosoglutathione (GSNO), and malondialdehyde (MDA) in EBC | Twelve physically fit, non-asthmatic, non-smoking males | EBC was collected on an ECOSCREEN device, during 15 min, wearing a nose clip and stored at −80 °C, MDA was measured after derivatization with TBA by HPLC fluorescence | MDA increased 40% after low PM exercise, high PM1 inhalation during exercise caused a reduced alveolar contribution to eNO, NO3 and eNO variables were decreased and were related to impaired lung function | 9 Low | |
| Sakhvidi, 2015, Iran [57] | To measure exhaled breath malondialdehyde (EBC-MDA) in workers exposed to dust containing silica as compared with that of a non-exposed control group | 25 Male workers in a ceramic factory | 25 Male control subjects from administrative departments of the same factory | EBC was collected with a homemade apparatus, during 5 min, wearing a nose clip, samples were stored in a freezer at −20 °C until examination, MDA was analyzed using an HPLC equipped with a fluorescent detector | Significant correlation between respirable dust exposure intensity and the level of EBC-MDA of the exposed subjects, but no significant correlation with lung functions | 13 Moderate |
| Sauvain, 2014, Switzerland [58] | To evaluate the feasibility of using exhaled breath condensate (EBC) from healthy volunteers for (1) assessing the lung deposited dose of combustion nanoparticles and (2) determining the resulting oxidative stress | 15 Healthy non-smoking control subjects | EBC collected on a Rtube, during 10 min, wearing a nose clip, a aliquote was stored at −78 °C, MDA was derivatized with TBA, and then measured with HPLC fluorescence | The results suggest two phases of oxidation markers in EBC: first, the initial deposition of particles and gases in the lung lining liquid, and later the start of oxidative stress with associated cell membrane damage | 11 Moderate | |
| Stockfelt, 2012, Sweden [59] | To examine airway effects of two kinds of wood smoke in a chamber study | 16 Healthy non-smoking control subjects (8 males and 8 females), 3 excluded for respiratory problems before the experiment | EBC collected according to Barregard, MDA measured always according to Barregard | Relatively low levels of wood smoke exposure induce effects on airways | 8 Low | |
| Syslova, 2009, Czech Republic [60] | To develop a sensitive method for a parallel, rapid and precise determination of the most prominent oxidative stress biomarkers for patients with silica or asbestos disease | 20 Subjects with previous exposure to silica or asbestos and related disease | 10 Control subjects | EBC was collected on an ECOSCREEN device, for 5−10 min, wearing a nose clip, frozen at −80 °C, and stored for a maximum of 1 month, MDA was measured with optimized LC–ESI-MS/MS | The differences in concentration levels of biomarkers between the two groups was perceptible in all the body fluids (the difference observed in an exhaled breath condensatewas statistically most significant) | 12 Moderate |
| Szkudlarek, 2003, Poland [61] | To test whether exhalation of H2O2 and TBARs by healthy subjects depends on reactive oxygen species generation from blood phagocytes | 41 Healthy, non-smoking control subjects, mean age 20.770.8 years (18 males and 23 females) | EBC was collected on a homemade mouth piece connected to a glass tube cooler, wearing a nose clip, during 20 min, MDA was measured as TBARS according to Nowak | No association between exhaled TBARs and blood phagocytes activity was found | 10 Moderate | |
| Pelclova, 2020, Czech Republic [62] | To analyze biomarkers in EBC of nanocomposite workers and understand the health effects | 20 Researchers handling nanocomposites (15 males and 5 females), 19 non-smokers, mean age of 41.8 years | 21 Control subjects (15 males and 6 females), office emplyees, 19 non-smokers, mean age of 42.7 years | EBC was collected on ECOSCREEN and stored at −80 °C, MDA was measured with LC-ESI- MS/MS | among inflammation markers, LT4 and tumor necrosis factor were the most useful | 10 moderate |
| Parameters | β Coefficient | [95% Conf. Interval] | P > |t| |
|---|---|---|---|
| Analytical method | |||
| HPLCfluo/TBA (n = 9) | reference | ||
| Spectro/TBA (n = 2) | 0.30 | [−0.902; 1.49] | 0.59 |
| MS/DNPH (n = 9) | −1.03 | [−2.02; 0.032] | 0.04 |
| HPLCfluo/NA (n = 2) | 1.26 | [−0.079; 2.6] | 0.06 |
| Factor-specific Wald test | 0.04 | ||
| Use of nose clip | |||
| Yes (n = 9) | reference | ||
| No (n = 8) | 0.64 | [−0.52; 1.81] | 0.25 |
| NA/other (n = 5) | 1.14 | [0.32; 1.96] | 0.01 |
| Factor-specific Wald test | 0.04 | ||
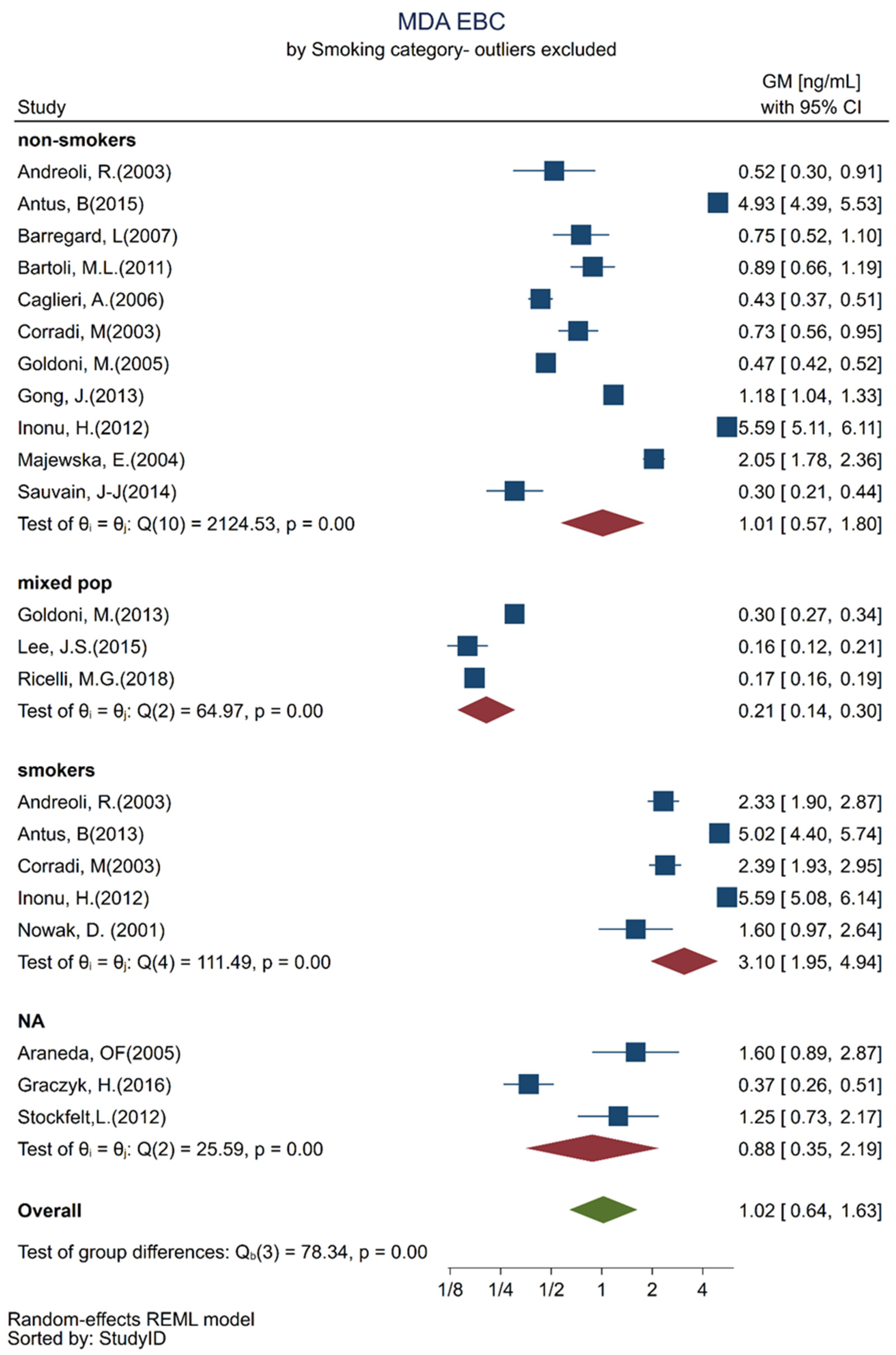
| Smoking habit | |||
| Non-smokers (n = 11) | reference | ||
| Mixed population (n = 3) | −0.71 | [−1.70; 0.28] | 0.14 |
| Smokers (n = 5) | 0.8 | [0.08; 1.51] | 0.03 |
| NA (n = 3) | 0.37 | [−0.57; 1.31] | 0.4 |
| Factor-specific Wald test | 0.04 | ||
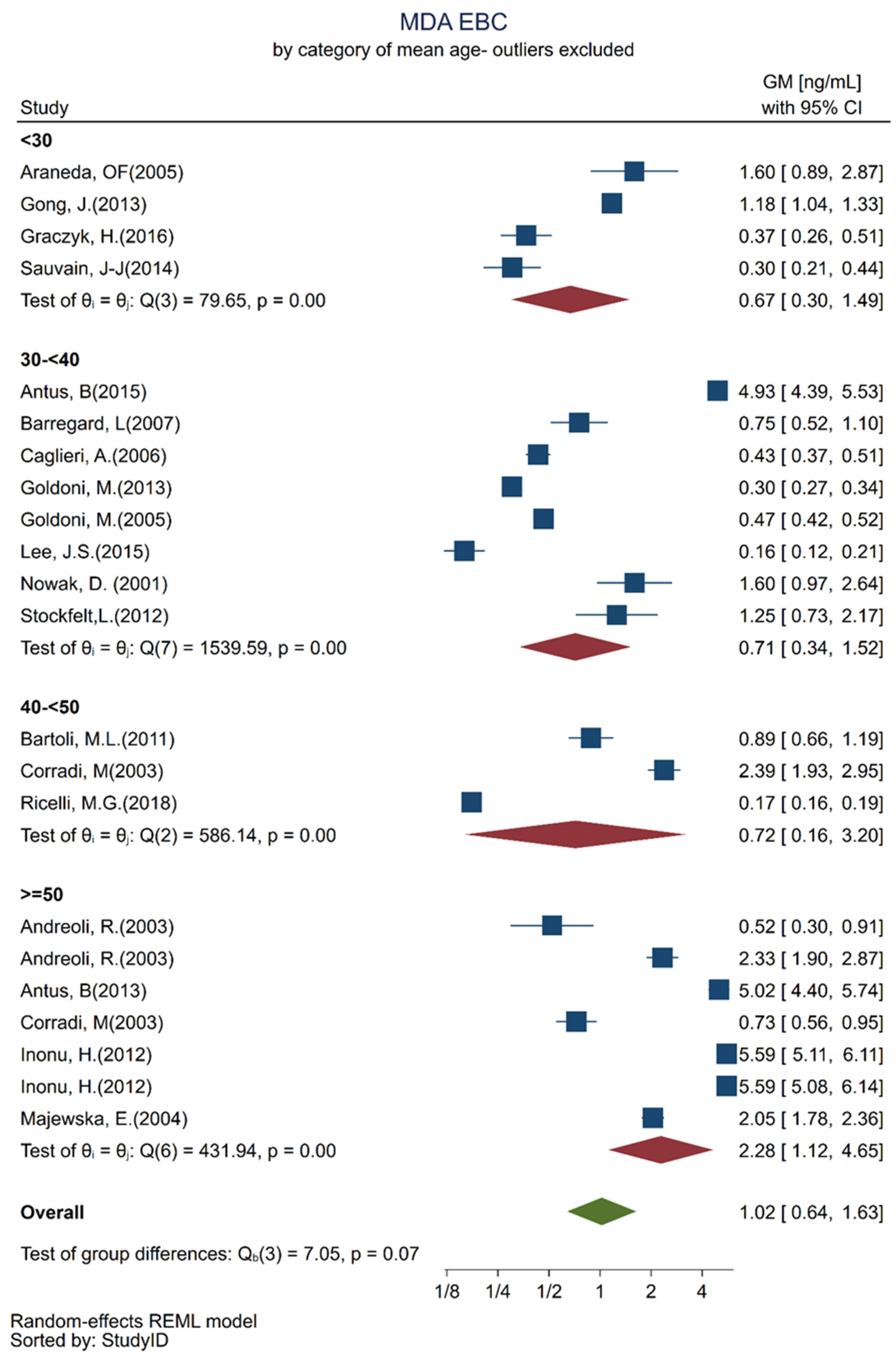
| Mean age (years) | |||
| <30 (n = 4) | reference | ||
| 30–<40 (n = 8) | 0.88 | [−0.014; 1.77] | 0.05 |
| 40–<50 (n = 3) | 0.82 | [−0.51; 2.16] | 0.2 |
| ≥50 (n = 7) | 1.21 | [0.09; 2.33] | 0.04 |
| Factor-specific Wald test | 0.15 | ||
| Intercept | −1.15 | [−2.07; −0.22] | 0.02 |
| Parameters | GM | 95% Confidence Interval |
|---|---|---|
| Analytical method | ||
| HPLCfluo/TBA (n = 9) | 1.8 | [0.795; 2.814] |
| Spectro/TBA (n = 2) | 2.43 | [0.142; 4.710] |
| MS/DNPH (n = 9) | 0.65 | [0.279; 1.015] |
| HPLCfluo/NA (n = 2) | 6.35 | [−0.252; 12.954] |
| Use of nose Clip | ||
| NA/other (n = 5) | 3.72 | [1.150; 6.292] |
| No (n = 8) | 2.27 | [0.141; 4.403] |
| Yes (n = 9) | 1.19 | [0.656; 1.727] |
| Smoking habits | ||
| Non-smokers (n = 11) | 1.2 | [0.751; 1.665] |
| Mixed population (n = 3) | 0.6 | [0.074; 1.111] |
| Smokers (n = 5) | 2.69 | [1.297; 4.065] |
| NA (n = 3) | 1.75 | [0.294; 3.207] |
| Mean Age (years) | ||
| <30 (n = 4) | 0.68 | [0.186; 1.178] |
| 30–<40 (n = 8) | 1.64 | [0.767; 2.520] |
| 40–<50 (n = 3) | 1.56 | [0.238; 2.875] |
| ≥50 (n = 7) | 2.28 | [1.150; 3.425] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turcu, V.; Wild, P.; Hemmendinger, M.; Sauvain, J.-J.; Bergamaschi, E.; Hopf, N.B.; Canu, I.G. Towards Reference Values for Malondialdehyde on Exhaled Breath Condensate: A Systematic Literature Review and Meta-Analysis. Toxics 2022, 10, 258. https://doi.org/10.3390/toxics10050258
Turcu V, Wild P, Hemmendinger M, Sauvain J-J, Bergamaschi E, Hopf NB, Canu IG. Towards Reference Values for Malondialdehyde on Exhaled Breath Condensate: A Systematic Literature Review and Meta-Analysis. Toxics. 2022; 10(5):258. https://doi.org/10.3390/toxics10050258
Chicago/Turabian StyleTurcu, Veronica, Pascal Wild, Maud Hemmendinger, Jean-Jacques Sauvain, Enrico Bergamaschi, Nancy B. Hopf, and Irina Guseva Canu. 2022. "Towards Reference Values for Malondialdehyde on Exhaled Breath Condensate: A Systematic Literature Review and Meta-Analysis" Toxics 10, no. 5: 258. https://doi.org/10.3390/toxics10050258
APA StyleTurcu, V., Wild, P., Hemmendinger, M., Sauvain, J.-J., Bergamaschi, E., Hopf, N. B., & Canu, I. G. (2022). Towards Reference Values for Malondialdehyde on Exhaled Breath Condensate: A Systematic Literature Review and Meta-Analysis. Toxics, 10(5), 258. https://doi.org/10.3390/toxics10050258