
Toxicological Aspects of Methotrexate Intoxication: Concentrations in Postmortem Biological Samples and Autopsy Findings


Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Instrumentation
2.3. Blank Samples
2.4. Sample Preparation
2.5. Working Solutions, Calibration Curve, Quality Control Samples
2.6. Method Validation
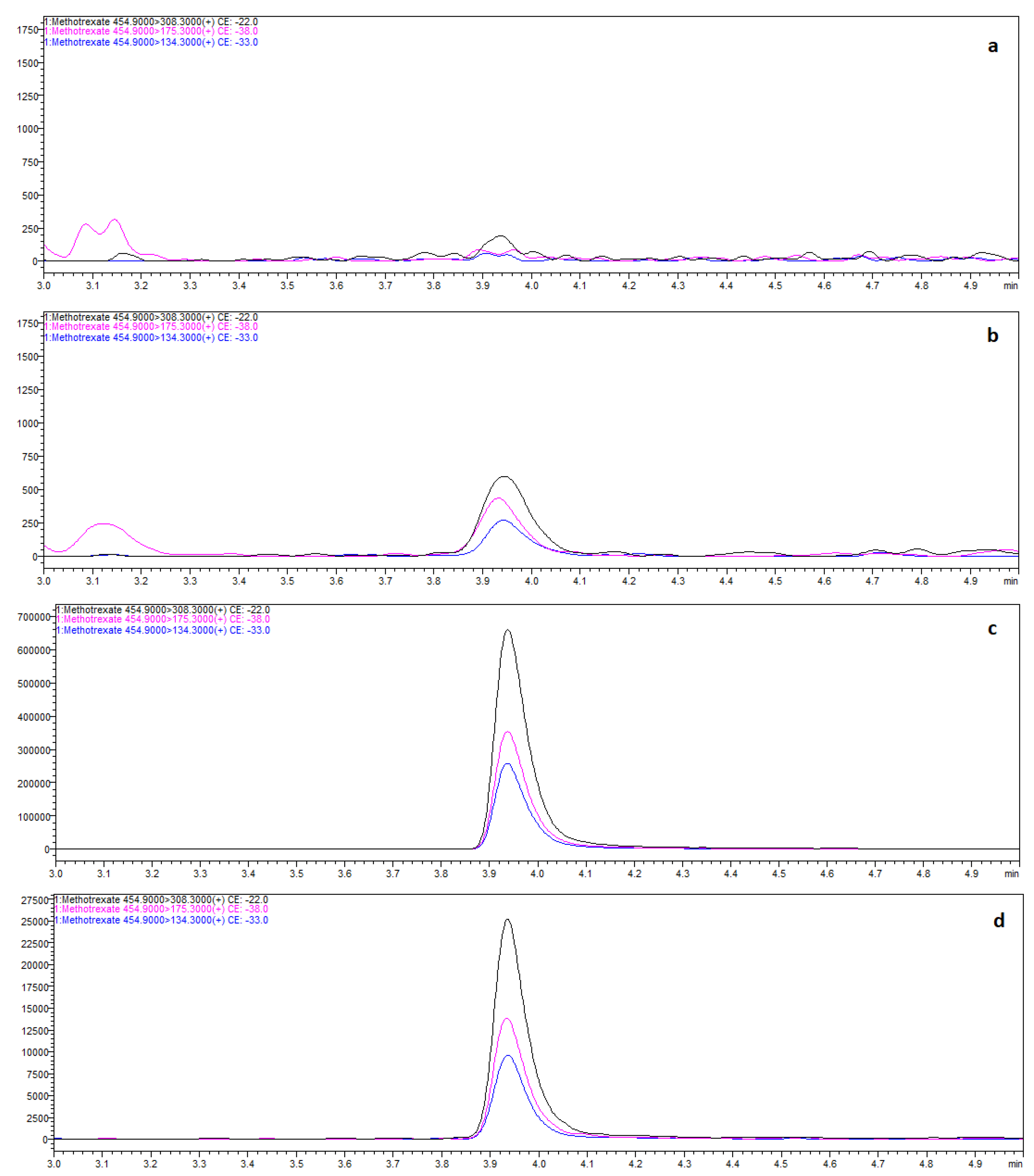
2.6.1. Selectivity
2.6.2. Linearity
2.6.3. Precision and Accuracy
2.6.4. Lower Limits of Quantification (LLOQ)
2.6.5. Recovery and Matrix Effect
2.7. Case Histories
2.7.1. Case 1
2.7.2. Case 2
2.7.3. Case 3
3. Results and Discussion
3.1. Method Development
3.2. Case Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Borgatta, L.; Burnhill, M.S.; Tyson, J.; Leonhardt, K.K.; Hausknecht, R.U.; Haskell, S. Early medical abortion with methotrexate and misoprostol. Obstet. Gynecol. 2001, 97, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Schaff, E.A.; Penmetsa, U.; Eisinger, S.H.; Franks, P. Methotrexate. A single agent for early abortion. J. Reprod. Med. 1997, 42, 56–60. [Google Scholar] [PubMed]
- Cairns, R.; Brown, J.A.; Lynch, A.M.; Robinson, J.; Wylie, C.; Buckley, N.A. A decade of Australian methotrexate dosing errors. Med. J. Aust. 2016, 204, 384. [Google Scholar] [CrossRef] [PubMed]
- Vial, T.; Patat, A.M.; Boels, D.; Castellan, D.; Villa, A.; Theophile, H.; Torrents, R.; Kassai, B. Adverse consequences of low-dose methotrexate medication errors: Data from French poison control and pharmacovigilance centers. Jt. Bone Spine 2019, 86, 351–355. [Google Scholar] [CrossRef]
- Hays, H.; Beuhler, M.C.; Spiller, H.A.; Weber, J.; Mowry, J.B.; Ryan, M.L.; Spiller, N.E.; Webb, A. Evaluation of toxicity after acute accidental methotrexate ingestions in children under 6 years old: A 16-year multi-center review. Clin. Toxicol. 2018, 56, 120–125. [Google Scholar] [CrossRef]
- Badurdeen, S.; Kang, S.L.; Saravanan, M. Accidental methotrexate ingestion in a 19-month-old child. BMJ Case Rep. 2011, 2011, bcr1120103477. [Google Scholar] [CrossRef]
- Gibbon, B.N.; Manthey, D.E. Pediatric case of accidental oral overdose of methotrexate. Ann. Emerg. Med. 1999, 34, 98–100. [Google Scholar] [CrossRef]
- Perregaard, H.; Aronson, J.K.; Dalhoff, K.; Hellebek, A. Medication errors detected in non-traditional databases: Types of errors in methotrexate dosing as listed in four different Danish registers. Eur. J. Clin. Pharmacol. 2015, 71, 1375–1379. [Google Scholar] [CrossRef]
- Salgueiro-Vázquez, M.E.; Sáinz Gil, M.; Fernández Peña, S.; Martín Arias, L.H. Medication errors associated with oral administration of methotrexate. Data from spontaneous reporting and medical literature review. Med. Clin. 2017, 148, 330–332. [Google Scholar] [CrossRef]
- Moore, T.J.; Walsh, C.S.; Cohen, M.R. Reported medication errors associated with methotrexate. Am. J. Health Syst. Pharm. 2004, 61, 1380–1384. [Google Scholar] [CrossRef]
- Sinicina, I.; Mayr, B.; Mall, G.; Keil, W. Deaths following methotrexate overdoses by medical staff. J. Rheumatol. 2005, 32, 2009–2011. [Google Scholar] [PubMed]
- Singh, A.; Handa, A.C. Medication Error—A Case Report of Misadventure with Methotrexate. JNMA 2018, 56, 711–715. [Google Scholar] [CrossRef]
- Baselt, R.C. Disposition of Toxic Drugs and Chemical in Man, 11th ed.; Biomedical Publications: Seal Beach, CA, USA, 2017; pp. 1343–1345. [Google Scholar]
- Chan, B.S.; Dawson, A.H.; Buckley, N.A. What can clinicians learn from therapeutic studies about the treatment of acute oral methotrexate poisoning? Clin. Toxicol. 2017, 55, 88–96. [Google Scholar] [CrossRef]
- Moisa, A.; Fritz, P.; Benz, D.; Wehner, H.D. Iatrogenically-related, fatal methotrexate intoxication: A series of four cases. Forensic Sci. Int. 2006, 156, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, M.; Matsumoto, T.; Matsumoto, T.; Jimi, S.; Takamatsu, Y.; Tamura, K.; Hara, S. Simple and sensitive HPLC method for the fluorometric determination of methotrexate and its major metabolites in human plasma by post-column photochemical reaction. Biomed. Chromatogr. 2012, 26, 76–80. [Google Scholar] [CrossRef]
- Li, H.; Luo, W.; Zeng, Q.; Lin, Z.; Luo, H.; Zhang, Y. Method for the determination of blood methotrexate by high performance liquid chromatography with online post-column electrochemical oxidation and fluorescence detection. J. Chromatogr. B Anal. Technol. Biomed Life Sci. 2007, 845, 164–168. [Google Scholar] [CrossRef]
- Rodríguez Flores, J.; Peñalvo, G.C.; Mansilla, A.E.; Gómez, M.J. Capillary electrophoretic determination of methotrexate, leucovorin and folic acid in human urine. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2005, 819, 141–147. [Google Scholar] [CrossRef]
- Kuo, C.Y.; Wu, H.L.; Kou, H.S.; Chiou, S.S.; Wu, D.C.; Wu, S. Simultaneous determination of methotrexate and its eight metabolites in human whole blood by capillary zone electrophoresis. J. Chromatogr. A 2003, 1014, 93–101. [Google Scholar] [CrossRef]
- Rule, G.; Chapple, M.; Henion, J. A 384-well solid-phase extraction for LC/MS/MS determination of methotrexate and its 7-hydroxy metabolite in human urine and plasma. Anal. Chem. 2001, 73, 439–443. [Google Scholar] [CrossRef]
- Guo, P.; Wang, X.; Liu, L.; Belinsky, M.G.; Kruh, G.D.; Gallo, J.M. Determination of methotrexate and its major metabolite 7-hydroxymethotrexate in mouse plasma and brain tissue by liquid chromatography-tandem mass spectrometry. J. Pharm. Biomed. Anal. 2007, 43, 1789–1795. [Google Scholar] [CrossRef]
- Steinborner, S.; Henion, J. Liquid-liquid extraction in the 96-well plate format with SRM LC/MS quantitative determination of methotrexate and its major metabolite in human plasma. Anal. Chem. 1999, 71, 2340–2345. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghobashy, M.A.; Hassan, S.A.; Abdelaziz, D.H.; Elhosseiny, N.M.; Sabry, N.A.; Attia, A.S.; El-Sayed, M.H. Development and validation of LC-MS/MS assay for the simultaneous determination of methotrexate, 6-mercaptopurine and its active metabolite 6-thioguanine in plasma of children with acute lymphoblastic leukemia: Correlation with genetic polymorphism. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2016, 1038, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Rodin, I.; Braun, A.; Stavrianidi, A.; Shpigun, O. A validated LC-MS/MS method for rapid determination of methotrexate in human saliva and its application to an excretion evaluation study. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2013, 937, 1–6. [Google Scholar] [CrossRef]
- Wu, D.; Wang, Y.; Sun, Y.; Ouyang, N.; Qian, J. A simple, rapid and reliable liquid chromatography-mass spectrometry method for determination of methotrexate in human plasma and its application to therapeutic drug monitoring. Biomed. Chromatogr. 2015, 29, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Thappali, S.R.; Varanasi, K.V.; Veeraraghavan, S.; Vakkalanka, S.K.; Khagga, M. Simultaneous determination of methotrexate, dasatinib and its active metabolite N-deshydroxyethyl dasatinib in rat plasma by LC-MS/MS: Method validation and application to pharmacokinetic study. Arzneimittelforschung 2012, 62, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.S.; Selvo, N.S.; Roberts, J.K.; Daryani, V.M.; Owens, T.S.; Harstead, K.E.; Gajjar, A.; Stewart, C.F. Determination of Methotrexate, 7-Hydroxymethotrexate, and 2,4-Diamino-N10-methylpteroic Acid by LC-MS/MS in Plasma and Cerebrospinal Fluid and Application in a Pharmacokinetic Analysis of High-Dose Methotrexate. J. Liq. Chromatogr. Relat. Technol. 2016, 39, 745–751. [Google Scholar] [CrossRef]
- Bouquié, R.; Deslandes, G.; Bernáldez, B.N.; Renaud, C.; Daillyad, E.; Jolliet, P. A fast LC-MS/MS assay for methotrexate monitoring in plasma: Validation, comparison to FPIA and application in the setting of carboxypeptidase therapy. Anal. Methods 2014, 6, 178–186. [Google Scholar] [CrossRef]
- den Boer, E.; Heil, S.G.; van Zelst, B.D.; Meesters, R.J.; Koch, B.C.; Te Winkel, M.L.; van den Heuvel-Eibrink, M.M.; Luider, T.M.; de Jonge, R. A U-HPLC-ESI-MS/MS-based stable isotope dilution method for the detection and quantitation of methotrexate in plasma. Ther. Drug Monit. 2012, 34, 432–439. [Google Scholar] [CrossRef]
- Sharma, K.; Giri, K.; Dhiman, V.; Dixit, A.; Zainuddin, M.; Mullangi, R. A validated LC-MS/MS assay for simultaneous quantification of methotrexate and tofacitinib in rat plasma: Application to a pharmacokinetic study. Biomed. Chromatogr. 2015, 29, 722–732. [Google Scholar] [CrossRef]
- Schofield, R.C.; Ramanathan, L.V.; Murata, K.; Grace, M.; Fleisher, M.; Pessin, M.S.; Carlow, D.C. Development and validation of a turbulent flow chromatography and tandem mass spectrometry method for the quantitation of methotrexate and its metabolites 7-hydroxy methotrexate and DAMPA in serum. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2015, 1002, 169–175. [Google Scholar] [CrossRef]
- Mo, X.; Wen, Y.; Ren, B.; Chen, J.; Xu, C.; Wang, X.; Huang, M.; Chen, X. Determination of erythrocyte methotrexate polyglutamates by liquid chromatography/tandem mass spectrometry after low-dose methotrexate therapy in Chinese patients with rheumatoid arthritis. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2012, 907, 41–48. [Google Scholar] [CrossRef]
- Bluett, J.; Riba-Garcia, I.; Hollywood, K.; Verstappen, S.M.; Barton, A.; Unwin, R.D. A HPLC-SRM-MS based method for the detection and quantification of methotrexate in urine at doses used in clinical practice for patients with rheumatological disease: A potential measure of adherence. Analyst 2015, 140, 1981–1987. [Google Scholar] [CrossRef]
- Canal-Raffin, M.; Khennoufa, K.; Martinez, B.; Goujon, Y.; Folch, C.; Ducint, D.; Titier, K.; Brochard, P.; Verdun-Esquer, C.; Molimard, M. Highly sensitive LC-MS/MS methods for urinary biological monitoring of occupational exposure to cyclophosphamide, ifosfamide, and methotrexate antineoplastic drugs and routine application. J. Chromatogr. B Anal. Technol. Biomed Life Sci. 2016, 1038, 109–117. [Google Scholar] [CrossRef]
- Upadhyay, V.; Rajput, M.; Sen, A.; Suvarna, S.; Dhanse, S. A sensitive, high throughput estimation of methotrexate in human plasma by high performance liquid chromatography tandem mass spectrometry. Int. J. Pharm. Sci. Res. 2017, 8, 3371–3378. [Google Scholar] [CrossRef]
- Chambers, E.; Wagrowski-Diehl, D.M.; Lu, Z.; Mazzeo, J.R. Systematic and comprehensive strategy for reducing matrix effects in LC/MS/MS analyses. J. Chromatogr. B Analyt. Technol. Biomed Life Sci. 2007, 852, 22–34. [Google Scholar] [CrossRef]
- Iskierka, M.; Zawadzki, M.; Szpot, P.; Jurek, T. Detection of Drugs in Postmortem Specimens of Blood, Vitreous Humor and Bone Marrow Aspirate. J. Anal. Toxicol. 2021, 45, 348–355. [Google Scholar] [CrossRef]
- Anderson, L.L.; Collins, G.J.; Ojima, Y.; Sullivan, R.D. A study of the distribution of methotrexate in human tissues and tumors. Cancer Res. 1970, 30, 1344–1348. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Compounds | Retention Time a | Precursor Ions b | Product Ions b | Dwell Time c | Q1 Pre Bias d | CE d | Q3 Pre Bias d |
|---|---|---|---|---|---|---|---|
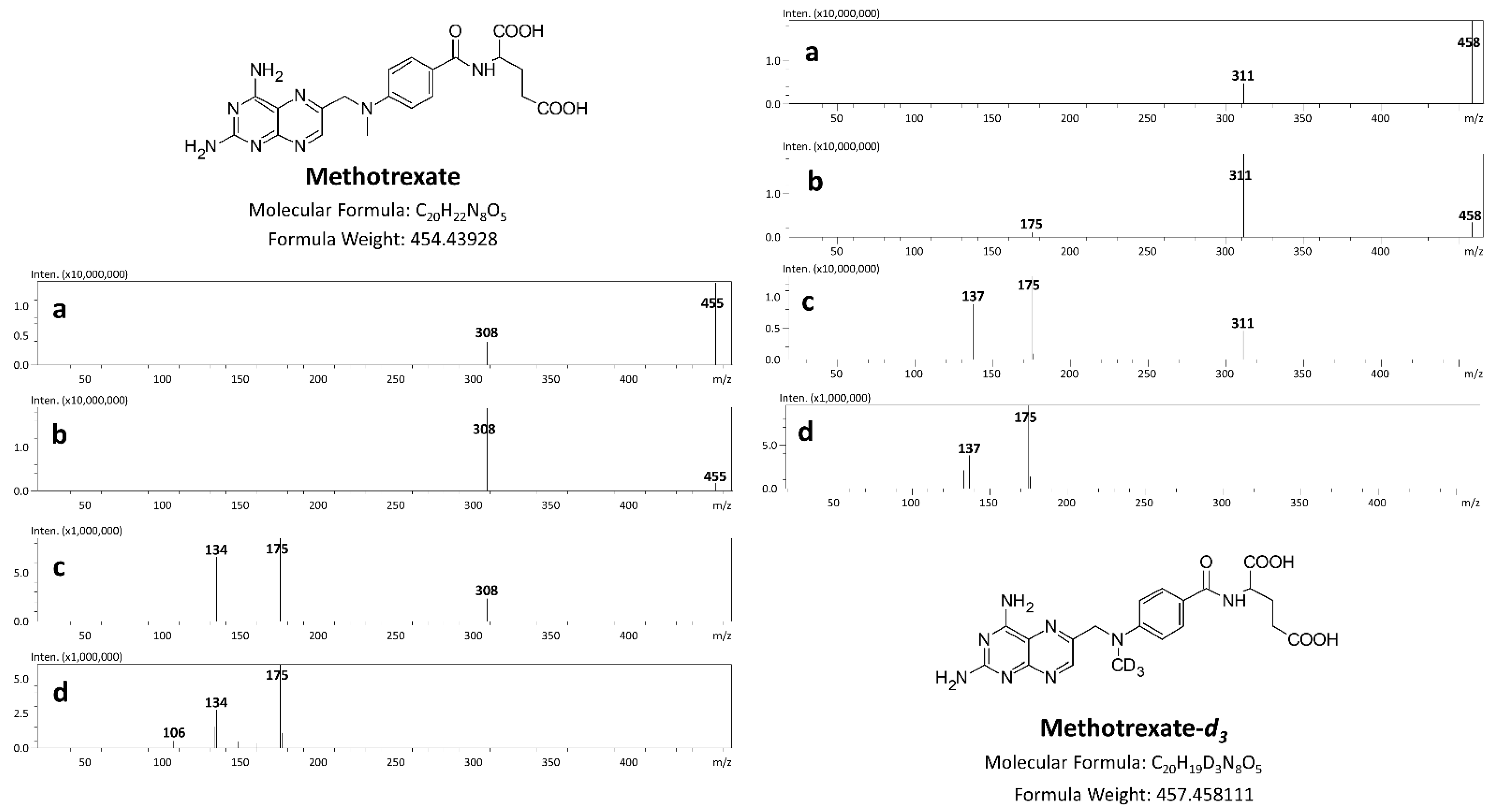
| MTX | 3.94 | 454.9 | 308.3 * 175.3 134.3 | 22 | −13 −13 −13 | −22 −38 −33 | −21 −11 −24 |
| MTX-d3 | 3.96 | 457.9 | 311.3 * 175.2 137.3 | 22 | −13 −13 −13 | −21 −45 −33 | −22 −11 −19 |
| Biological Matrix | Validation Parameters | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| The Linear Concentration Range [ng/mL] or [ng/g] | The Coefficient of Determination (R2) | LLOQ [ng/mL] or [ng/g] | Concentration Level [ng/mL] or [ng/g] | Intraday | Interday | Recovery [%] * | Matrix Effect [%] * | |||
| Precision [%] * | Accuracy [%] * | Precision [%] * | Accuracy [%] * | |||||||
| Postmortem blood | 0.1–1000 | >0.998 | 0.1 | 1 100 1000 | 7.7 5.5 4.5 | 14.3 5.5 5.1 | 10.8 14.0 10.3 | 4.9 11.6 8.6 | 104.7 101.8 89.0 | 4.7 1.8 −11.0 |
| Vitreous humor | 0.5–1000 | >0.996 | 0.5 | 1 100 1000 | 2.0 7.2 17.4 | 9.1 11.5 11.0 | 13.4 8.4 5.7 | 9.3 5.1 14.8 | 113.6 105.0 101.2 | 13.6 1.2 1.2 |
| Kidney | 0.1–1000 | >0.999 | 0.1 | 1 100 1000 | 5.2 6.4 4.6 | 7.8 0.3 3.8 | 0.8 4.3 2.4 | −0.4 −0.9 −0.5 | 106.7 97.7 100.3 | 6.7 −2.3 0.3 |
| Liver | 1.0–1000 | >0.999 | 1.0 | 1 100 1000 | 0.5 1.5 2.6 | 0.5 1.5 8.3 | 6.4 4.0 12.7 | 7.0 4.1 5.9 | 99.4 92.2 100.4 | −0.6 −7.8 0.4 |
| Type of Biological Sample (Volume) | Sample Preparation Technique | Detector (Mode) | Recovery (%)/IS | LOQ/Unit | References |
|---|---|---|---|---|---|
| Plasma (500 μL) | SPE | ESI/triple quadrupole (MRM) | 94.28–102.22/thiouracil | 6.25 ng/mL | [23] |
| Saliva (1400 μL) | SPE | ESI/Qtrap (MRM) | 89–94/ aminopterin | 2 ng/mL a | [24] |
| Plasma and urine (30 μL) | SPE | Z-Spray/triple quadrupole (MRM) | ≥95/ methotrexate-d3 | 1000 ng/mL | [20] |
| Plasma (10 μL) | Protein precipitation with methanol | ESI/triple quadrupole (MRM) | 66.2/ aminopterin | 3.7 ng/mL | [21] |
| Plasma (200 μL) | LLE with chloroform | ESI/triple quadrupole (MRM) | 61.0/ methotrexate-d3 | 0.5 ng/mL | [22] |
| Plasma (10 μL) | Dilution with water– acetonitrile, 70:30 (v/v) | ESI/Qtrap (MRM) | 97.8–112.0/ p-amino-acetophenone | 0.05 μmol/L | [25] |
| Plasma (50 μL) | LLE with tert-methyl-butyl ether | HESI/triple quadrupole (MRM) | 79.4–87.2/tolbutamide | 1 ng/mL | [26] |
| Plasma and cerebrospinal fluid (100 μL) | SPE | ESI/Qtrap (MRM) | 86.5–90.4 (plasma) 98.7–103.8 (CSF)/methotrexate-d3 | 0.0022 μM | [27] |
| Plasma (50 μL) | Protein precipitation with methanol and 0.2 M ZnSO4 (80:20, v/v) | ESI/triple quadrupole (MRM) | 24.0/ 13C2H3-methotrexate | 0.025 μmol/L | [28] |
| Plasma (50 μL) | Protein precipitation with cold 16% perchloric acid | ESI/triple quadrupole (MRM) | 96.0–102.0/methotrexate-d3 | 5 nM | [29] |
| Plasma (50 μL) | SPE | ESI/Qtrap (MRM) | 84.8–90.7/phenacetin | 0.49 ng/mL | [30] |
| Plasma (200 μL) | SPE | ESI/triple quadrupole (MRM) | 92.0/ methotrexate-d3 | 0.5 ng/mL | [35] |
| Serum (100 μL) | Protein precipitation with methanol containing formic acid | HESI/triple quadrupole (MRM) | 94.6–104.3/methotrexate-d3 | 10 nmol/L | [31] |
| Whole blood (400 μL) | Protein precipitation with trifluoroacetic acid solution and LLE with ethyl acetoacetate | ESI/triple quadrupole (MRM) | 29.3–37.8/doxofylline | 1 ng/mL | [32] |
| Urine (50 μL) | Protein precipitation with ACN | ESI/triple quadrupole (MRM) | 104.0–126.0/methotrexate-d3 | 2.5 nM | [33] |
| Urine (5000 μL) | SPE | ESI/triple quadrupole (MRM) | 75.3–81.7/methotrexate-d3 | 20 pg/mL | [34] |
| Postmortem samples (100 μL or 100 mg) | Protein precipitation with methanol | ESI/triple quadrupole (MRM) | 89.0–113.6/methotrexate-d3 | 0.1–1.0 ng/mL or ng/g | Presented method |
| Blood | Vitreous Humor | Liver | Kidney | Bone Marrow | Lumbar Vertebra | |
|---|---|---|---|---|---|---|
| MTX concentrations [ng/mL] or [ng/g] * | 7.2 | 0.8 | 43.7 * | 20.6 * | 29.9 * | 20.0 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szpot, P.; Wachełko, O.; Zawadzki, M. Toxicological Aspects of Methotrexate Intoxication: Concentrations in Postmortem Biological Samples and Autopsy Findings. Toxics 2022, 10, 572. https://doi.org/10.3390/toxics10100572
Szpot P, Wachełko O, Zawadzki M. Toxicological Aspects of Methotrexate Intoxication: Concentrations in Postmortem Biological Samples and Autopsy Findings. Toxics. 2022; 10(10):572. https://doi.org/10.3390/toxics10100572
Chicago/Turabian StyleSzpot, Paweł, Olga Wachełko, and Marcin Zawadzki. 2022. "Toxicological Aspects of Methotrexate Intoxication: Concentrations in Postmortem Biological Samples and Autopsy Findings" Toxics 10, no. 10: 572. https://doi.org/10.3390/toxics10100572
APA StyleSzpot, P., Wachełko, O., & Zawadzki, M. (2022). Toxicological Aspects of Methotrexate Intoxication: Concentrations in Postmortem Biological Samples and Autopsy Findings. Toxics, 10(10), 572. https://doi.org/10.3390/toxics10100572