
Adjunctive Effect of Green Tea Mouthwash Prepared at Different Steeping Temperatures on Gingivitis: A Triple-Blind Randomized Controlled Clinical Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
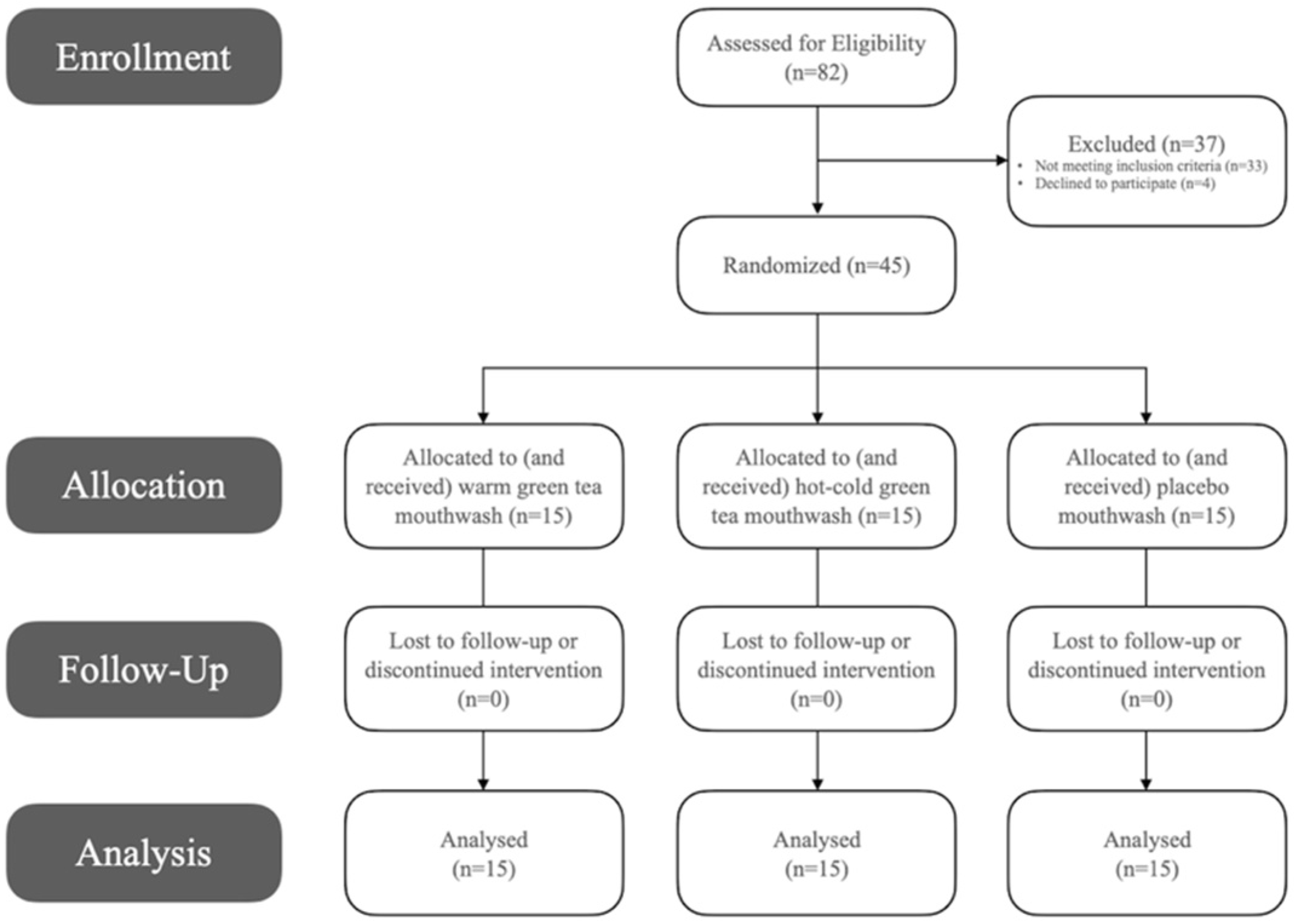
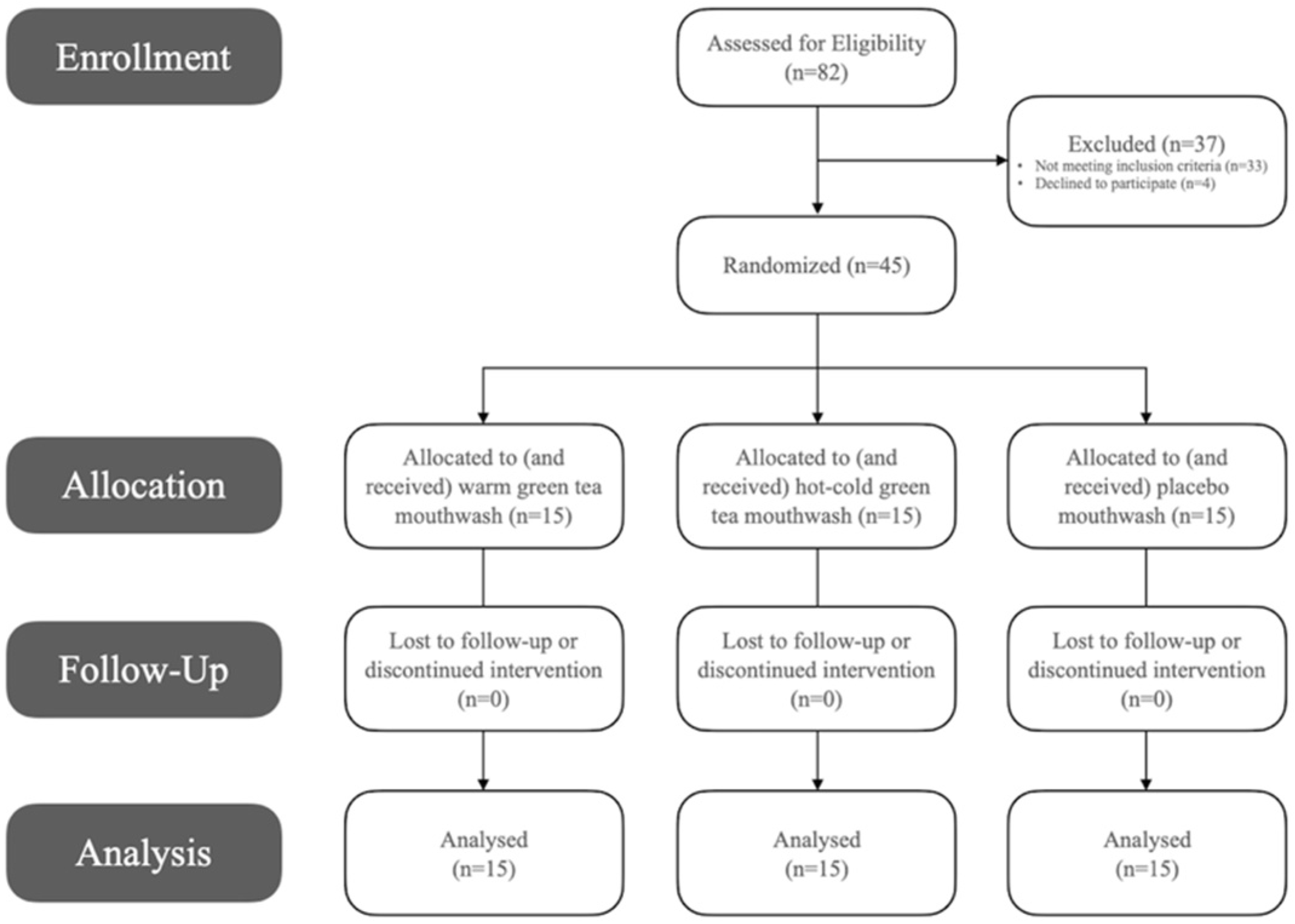
2.1. Study Design and Sample
2.2. Solution Preparation
2.3. Study Outline
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
4. Discussion
Limitations
5. Conclusions
Practical Significance
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramesh, A.; Varghese, S.; Doraiswamy, J.; Malaiappan, S. Herbs as an antioxidant arsenal for periodontal diseases. J. Intercult. Ethnopharmacol. 2016, 5, 92. [Google Scholar] [CrossRef]
- Venkateswara, B.; Sirisha, K.; Chava, V.K. Green tea extract for periodontal health. J. Indian Soc. Periodontol. 2011, 15, 18. [Google Scholar] [CrossRef]
- Emmadi, P.; Krishna, P.; Namasi, A.; Nugala, B. Role of green tea as an antioxidant in periodontal disease: The Asian paradox. J. Indian Soc. Periodontol. 2012, 16, 313–316. [Google Scholar]
- Wong, L.B.; Yap, A.U.; Allen, P.F. Periodontal disease and quality of life: Umbrella review of systematic reviews. J. Periodontal. Res. 2021, 56, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Tinanoff, N.; Baez, R.J.; Diaz Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Pitts, N.B.; Seow, W.K.; Sharkov, N.; et al. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int. J. Paediatr. Dent. 2019, 29, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Chapple, I.L.C.; Van Der Weijden, F.; Doerfer, C.; Herrera, D.; Shapira, L.; Polak, D.; Madianos, P.; Louropoulou, A.; Machtei, E.; Donos, N.; et al. Primary prevention of periodontitis: Managing gingivitis. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S71–S76. [Google Scholar] [CrossRef] [Green Version]
- Idrees, M.M.; Azzeghaiby, S.N.; Hammad, M.M.; Kujan, O.B. Prevalence and severity of plaque-induced gingivitis in a Saudi adult population. Saudi. Med. J. 2014, 35, 1373. [Google Scholar]
- Behfarnia, P.; Aslani, A.; Jamshidian, F.; Noohi, S.; Author, C. The efficacy of green tea chewing gum on gingival inflammation. J. Dent. Shiraz. Univ. Med. Sci. 2016, 17, 149–154. [Google Scholar]
- Rassameemasmaung, S.; Phusudsawang, P.; Sangalungkarn, V. Effect of green tea mouthwash on oral malodor. ISRN Prev. Med. 2013, 2013, 97514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priya, B.M.; Anitha, V.; Shanmugam, M.; Ashwath, B.; Sylva, S.D.; Vigneshwari, S.K. Efficacy of chlorhexidine and green tea mouthwashes in the management of dental plaque-induced gingivitis: A comparative clinical study. Contemp. Clin. Dent. 2015, 6, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Laleman, I.; Teughels, W. Novel natural product-based oral topical rinses and toothpastes to prevent periodontal diseases. Periodontology 2000, 84, 102–123. [Google Scholar] [CrossRef]
- Kim, M.A.; Kim, J.H.; Nam, O.H. Tea extracts differentially inhibit Streptococcus mutans and Streptococcus sobrinus biofilm colonization depending on the steeping temperature. Biofouling 2020, 36, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Steiger-Ronay, V.; Steingruber, A.; Becker, K.; Aykut-Yetkiner, A.; Wiedemeier, D.B.; Attin, T. Temperature-dependent erosivity of drinks in a model simulating oral fluid dynamics. J. Dent. 2018, 70, 118–123. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 10, 28–55. [Google Scholar]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S68–S77. [Google Scholar] [CrossRef]
- Neturi, R.S.; Srinivas, R.; Vikram Simha, B.; Sree, S.; Chandra Shekar, T.; Siva Kumar, P. Effects of green tea on streptococcus mutans counts-a randomised control trail. J. Clin. Diagn. Res. 2014, 8, ZC128. [Google Scholar] [CrossRef]
- Lantano, C.; Rinaldi, M.; Cavazza, A.; Barbanti, D.; Corradini, C. Effects of alternative steeping methods on composition, antioxidant property and colour of green, black and oolong tea infusions. J. Food Sci. Technol. 2015, 52, 8276–8283. [Google Scholar] [CrossRef] [Green Version]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Bessa Rebelo, M.A.; de Queiroz, A.C. Gingival indices: State of art. In Gingival Diseases—Their Aetiology, Prevention and Treatment; Panagakos, F., Ed.; West Virginia University: Morgantown, WV, USA, 2011. [Google Scholar]
- Sarin, S.; Marya, C.; Nagpal, R.; Oberoi, S.S.; Rekhi, A. Preliminary clinical evidence of the antiplaque, antigingivitis efficacy of a mouthwash containing 2% green tea—A randomised clinical trial. Oral. Health Prev. Dent. 2015, 13, 197–203. [Google Scholar] [PubMed]
- Kaur, H.; Jain, S.; Kaur, A. Comparative evaluation of the antiplaque effectiveness of green tea catechin mouthwash with chlorhexidine gluconate. J. Indian Soc. Periodontol. 2014, 18, 178–182. [Google Scholar] [CrossRef]
- Chacko, S.M.; Thambi, P.T.; Kuttan, R.; Nishigaki, I. Beneficial effects of green tea: A literature review. Chin. Med. 2010, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirasawa, M.; Takada, K.; Makimura, M.; Otake, S. Improvement of periodontal status by green tea catechin using a local delivery system: A clinical pilot study. J. Periodontal. Res. 2002, 37, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Seminario-Amez, M.; López-López, J.; Estrugo-Devesa, A.; Ayuso-Montero, R.; Jané-Salas, E. Probiotics and oral health: A systematic review. Med. Oral. Patol. Oral. Cir. Bucal. 2017, 22, e282–e288. [Google Scholar] [CrossRef] [Green Version]
- Pujia, A.M.; Costacurta, M.; Fortunato, L.; Merra, G.; Cascapera, S.; Calvani, M. The probiotics in dentistry: A narrative review. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 1405–1412. [Google Scholar] [PubMed]
- Prasad, M.; Patthi, B.; Singla, A.; Gupta, R.; Jankiram, C.; Kumar, J.K.; Vashishtha, V.; Malhi, R. The clinical effectiveness of post-brushing rinsing in reducing plaque and gingivitis: A systematic review. J. Clin. Diagn. Res. 2016, 10, ZE01. [Google Scholar] [CrossRef]
- Otomo-Corgel, J. Dental management of the female patient. Periodontol. 2000 2013, 61, 219–231. [Google Scholar] [CrossRef]
- Van Der Velden, U.; Abbas, F.; Hart, A.A.M. Experimental gingivitis in relation to susceptibility to periodontal disease: (I.) Clinical observations. J. Clin. Periodontol. 1985, 12, 61–68. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | All Participants (N = 45) | Group A: Green Tea (Warm MW) (n = 15) | Group B: Green Tea (Hot-Ice MW) (n = 15) | Group C: Placebo (n = 15) | ||||
|---|---|---|---|---|---|---|---|---|
| Median | Mean ± SD | Median | Mean ± SD | Median | Mean ± SD | Median | Mean ± SD | |
| Age | 20 | 20 ± 2 | 20 | 20 ± 2 | 21 | 21 ± 2 | 20 | 20 ± 1 |
| Plaque Control Record—PCR | 80 | 77 ± 17 | 82 | 78 ± 17 | 86 | 82 ± 19 | 76 | 70 ± 13 |
| Gingival Bleeding Index—GBI | 82 | 82 ± 7 | 80 | 80 ± 7 | 85 | 86 ± 7 | 81 | 82 ± 6 |
| Variable | Group A: Green Tea (Warm MW) (n = 15) | Group B: Green Tea (Hot-Ice MW) (n = 15) | Group C: Placebo (n = 15) | p-Value |
|---|---|---|---|---|
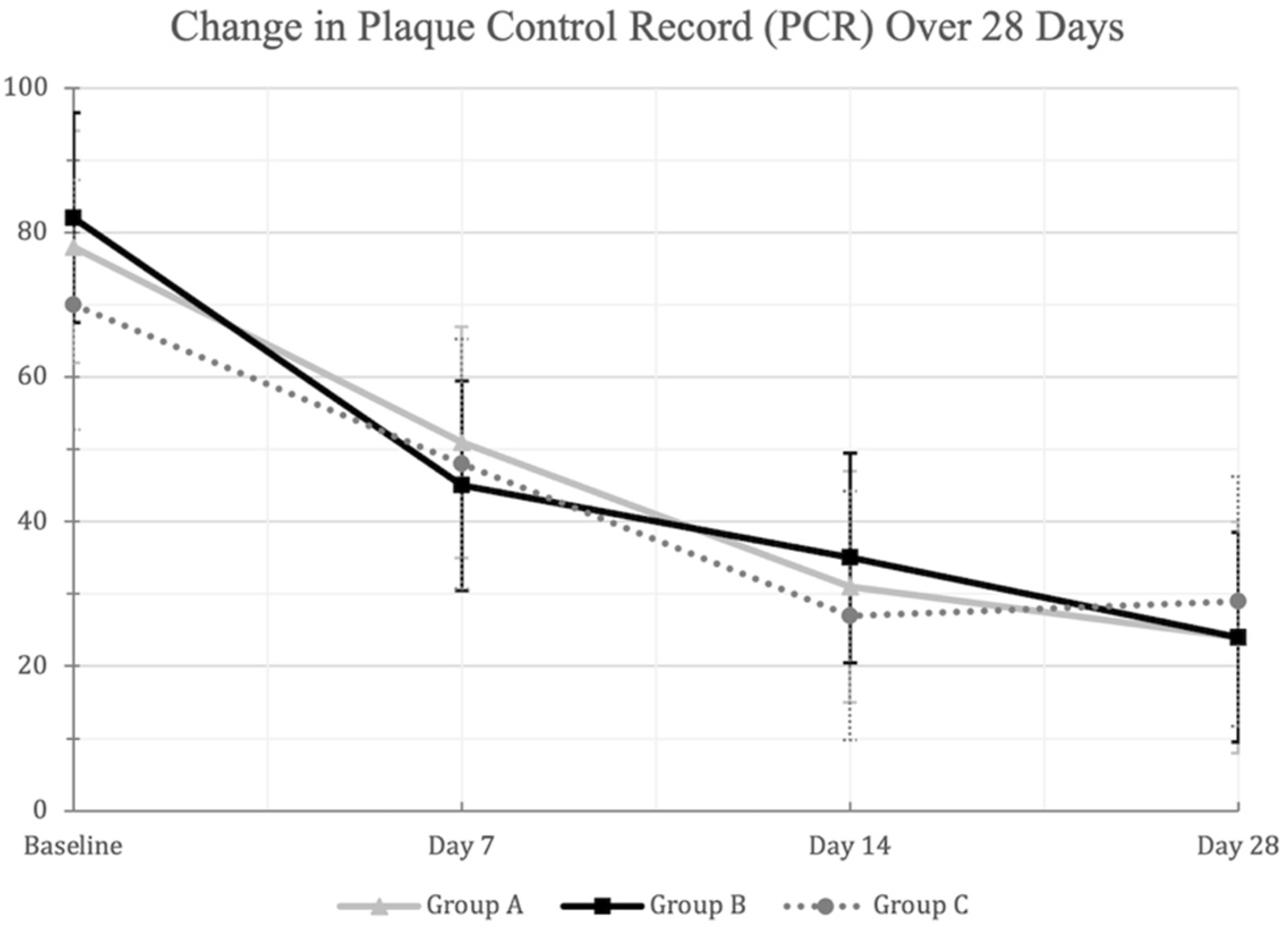
| PCR (mean ± SD) | ||||
| Baseline Examination (Day 0) | 78 ± 17 | 82 ± 19 | 70 ± 13 | 0.113 |
| 1st Examination (Day 7) | 51 ± 22 | 45 ± 21 | 48 ± 23 | 0.767 |
| 2nd Examination (Day 14) | 31 ± 9 | 35 ± 18 | 27 ± 7 | 0.236 |
| 3rd Examination (Day 28) | 24 ± 10 | 24 ± 11 | 29 ± 21 | 0.633 |
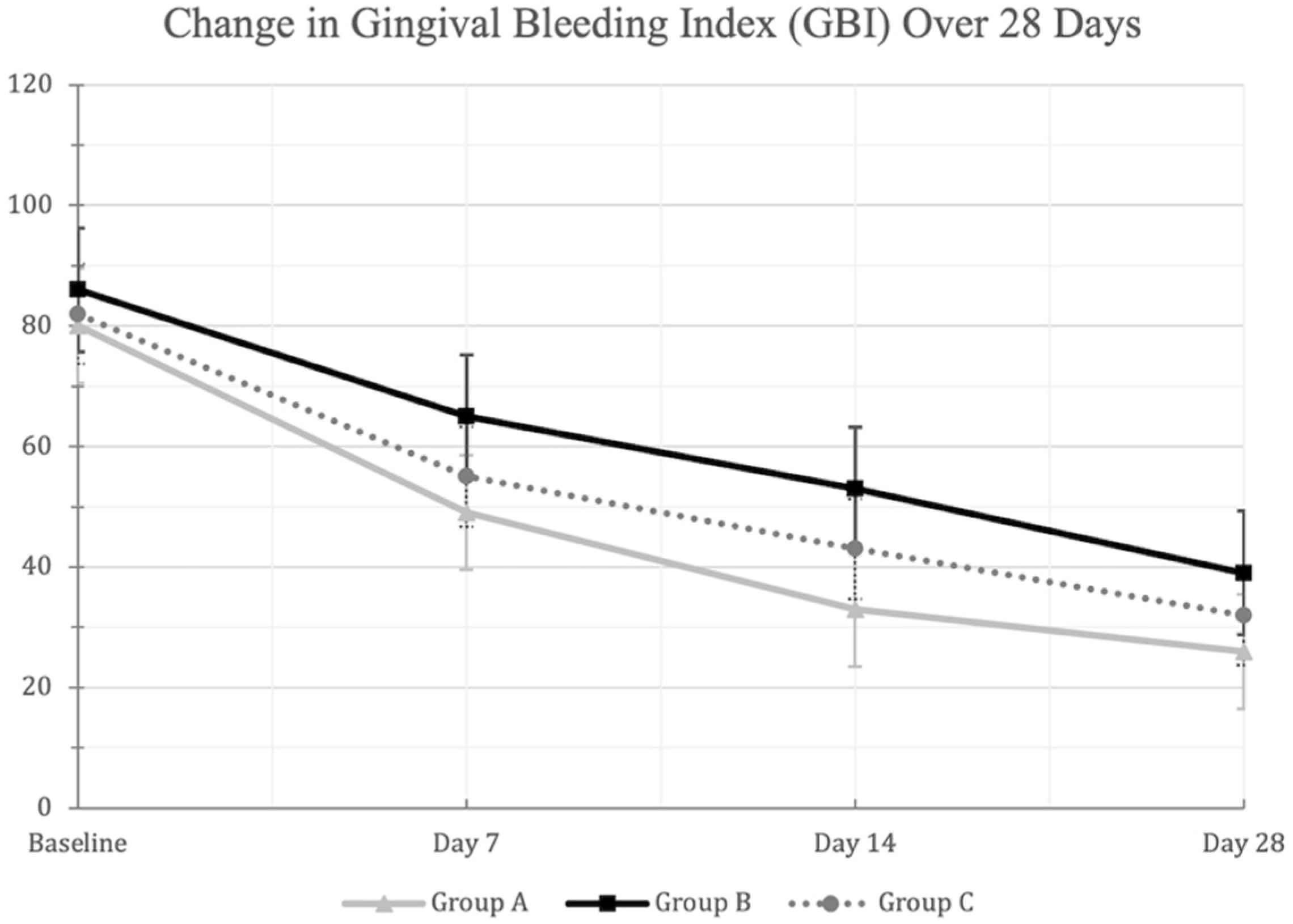
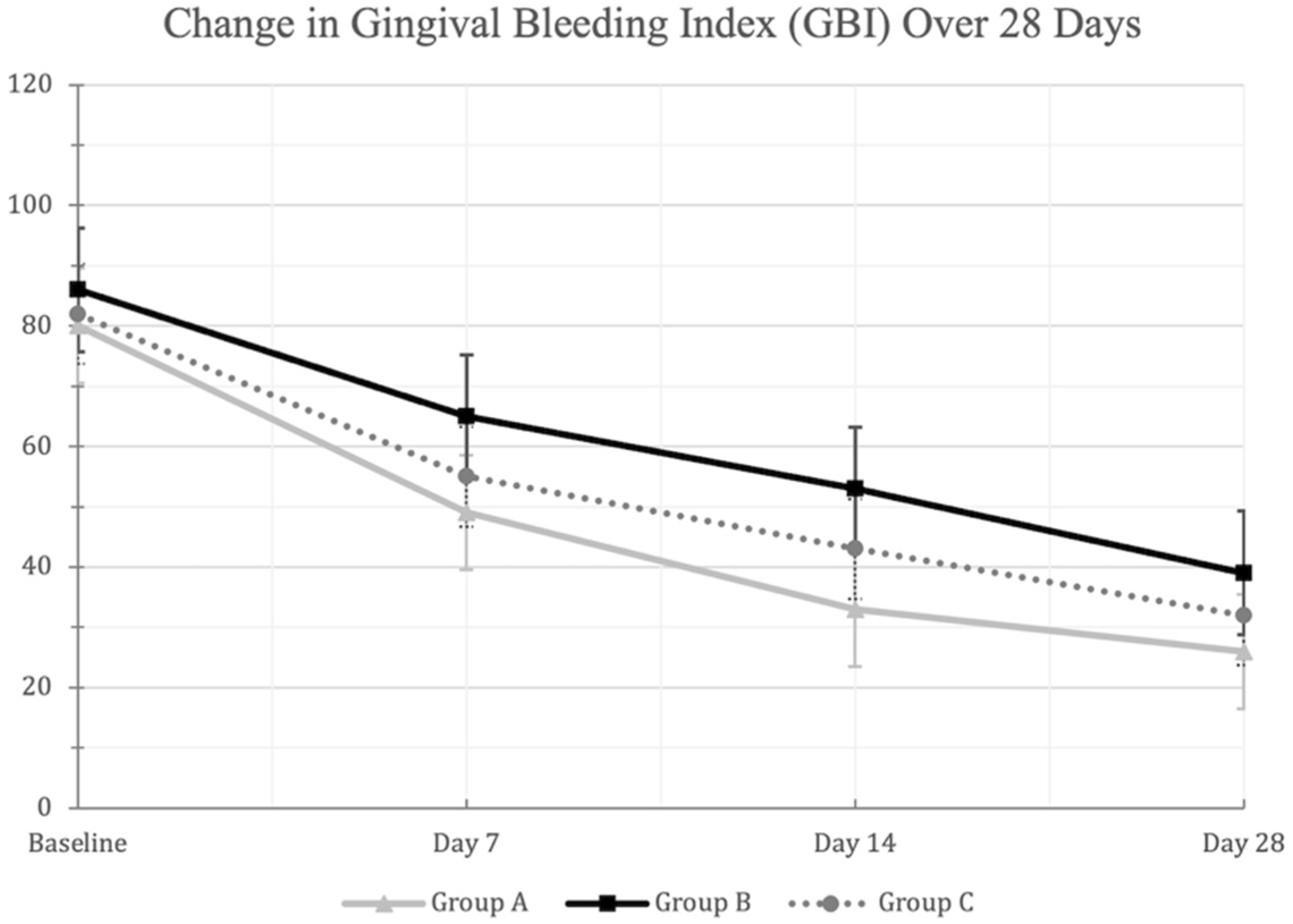
| GBI (mean ± SD) | ||||
| Baseline Examination (Day 0) | 80 ± 7 | 86 ± 7 | 82 ± 6 | 0.053 |
| 1st Examination (Day 7) | 49 ± 14 | 65 ± 10 | 55 ± 10 | 0.001 |
| 2nd Examination (Day 14) | 33 ± 9 | 53 ± 8 | 43 ± 8 | <0.001 |
| 3rd Examination (Day 28) | 26 ± 11 | 39 ± 8 | 32 ± 14 | 0.013 |
| Variable | Group A: Green Tea (Warm MW) | Group B: Green Tea (Hot-Ice MW) | Group C: Placebo |
|---|---|---|---|
| Baseline Examination (Day 0) | |||
| Group A: Green Tea (Warm MW) | - | 0.018 | 0.445 |
| Group B: Green Tea (Hot-Ice MW) | 0.018 | - | 0.099 |
| Group C: Placebo | 0.445 | 0.099 | - |
| 1st Examination (Day 7) | |||
| Group A: Green Tea (Warm MW) | - | <0.001 | 0.125 |
| Group B: Green Tea (Hot-Ice MW) | <0.001 | - | 0.025 |
| Group C: Placebo | 0.125 | 0.025 | - |
| 2nd Examination (Day 14) | |||
| Group A: Green Tea (Warm MW) | - | <0.001 | 0.004 |
| Group B: Green Tea (Hot-Ice MW) | <0.001 | - | 0.001 |
| Group C: Placebo | 0.004 | 0.001 | - |
| 3rd Examination (Day 28) | |||
| Group A: Green Tea (Warm MW) | - | 0.003 | 0.182 |
| Group B: Green Tea (Hot-Ice MW) | 0.003 | - | 0.088 |
| Group C: Placebo | 0.182 | 0.088 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fadel, H.T.; AlRehaili, A.M.; AlShanqiti, M.M.; Alraddadi, A.A.; Albolowi, A.M. Adjunctive Effect of Green Tea Mouthwash Prepared at Different Steeping Temperatures on Gingivitis: A Triple-Blind Randomized Controlled Clinical Trial. Dent. J. 2021, 9, 139. https://doi.org/10.3390/dj9120139
Fadel HT, AlRehaili AM, AlShanqiti MM, Alraddadi AA, Albolowi AM. Adjunctive Effect of Green Tea Mouthwash Prepared at Different Steeping Temperatures on Gingivitis: A Triple-Blind Randomized Controlled Clinical Trial. Dentistry Journal. 2021; 9(12):139. https://doi.org/10.3390/dj9120139
Chicago/Turabian StyleFadel, Hani T., Alhanouf M. AlRehaili, Mona M. AlShanqiti, Afnan A. Alraddadi, and Alhanouf M. Albolowi. 2021. "Adjunctive Effect of Green Tea Mouthwash Prepared at Different Steeping Temperatures on Gingivitis: A Triple-Blind Randomized Controlled Clinical Trial" Dentistry Journal 9, no. 12: 139. https://doi.org/10.3390/dj9120139
APA StyleFadel, H. T., AlRehaili, A. M., AlShanqiti, M. M., Alraddadi, A. A., & Albolowi, A. M. (2021). Adjunctive Effect of Green Tea Mouthwash Prepared at Different Steeping Temperatures on Gingivitis: A Triple-Blind Randomized Controlled Clinical Trial. Dentistry Journal, 9(12), 139. https://doi.org/10.3390/dj9120139